Nutrition Behaviors in Polish Adults before and during COVID-19 Lockdown

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey Questionnaires
2.2. Statistical Analysis
3. Results
3.1. Study Group Baseline Characteristics
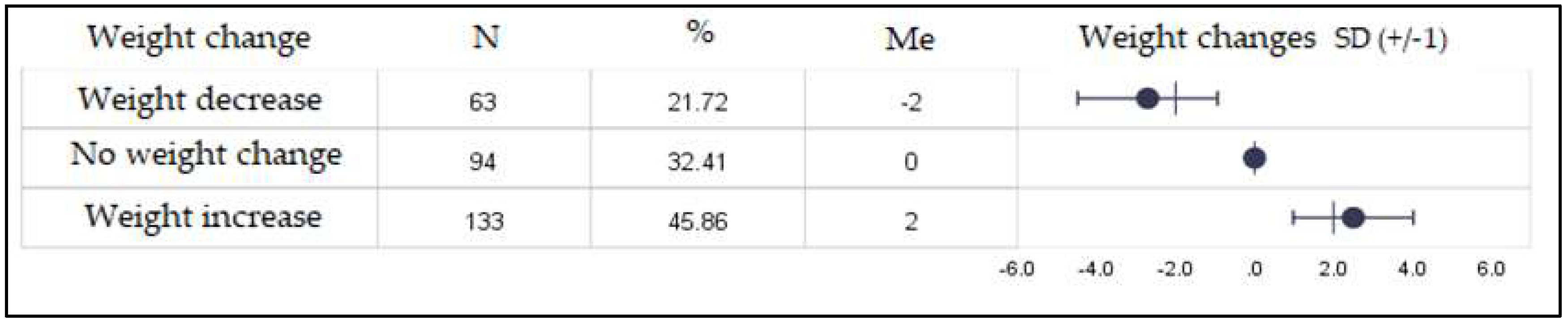
3.2. The Nutritional Status of the Study Group before and during Confinement
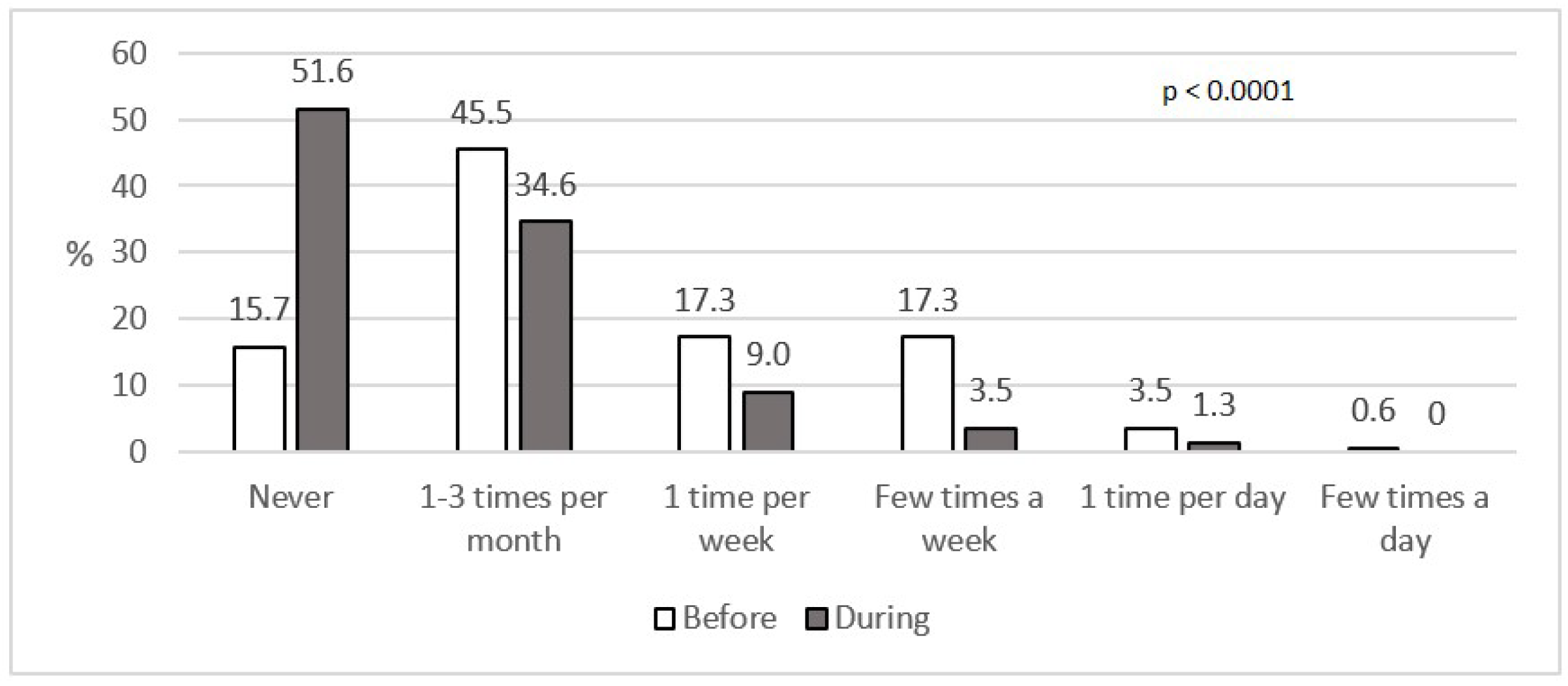
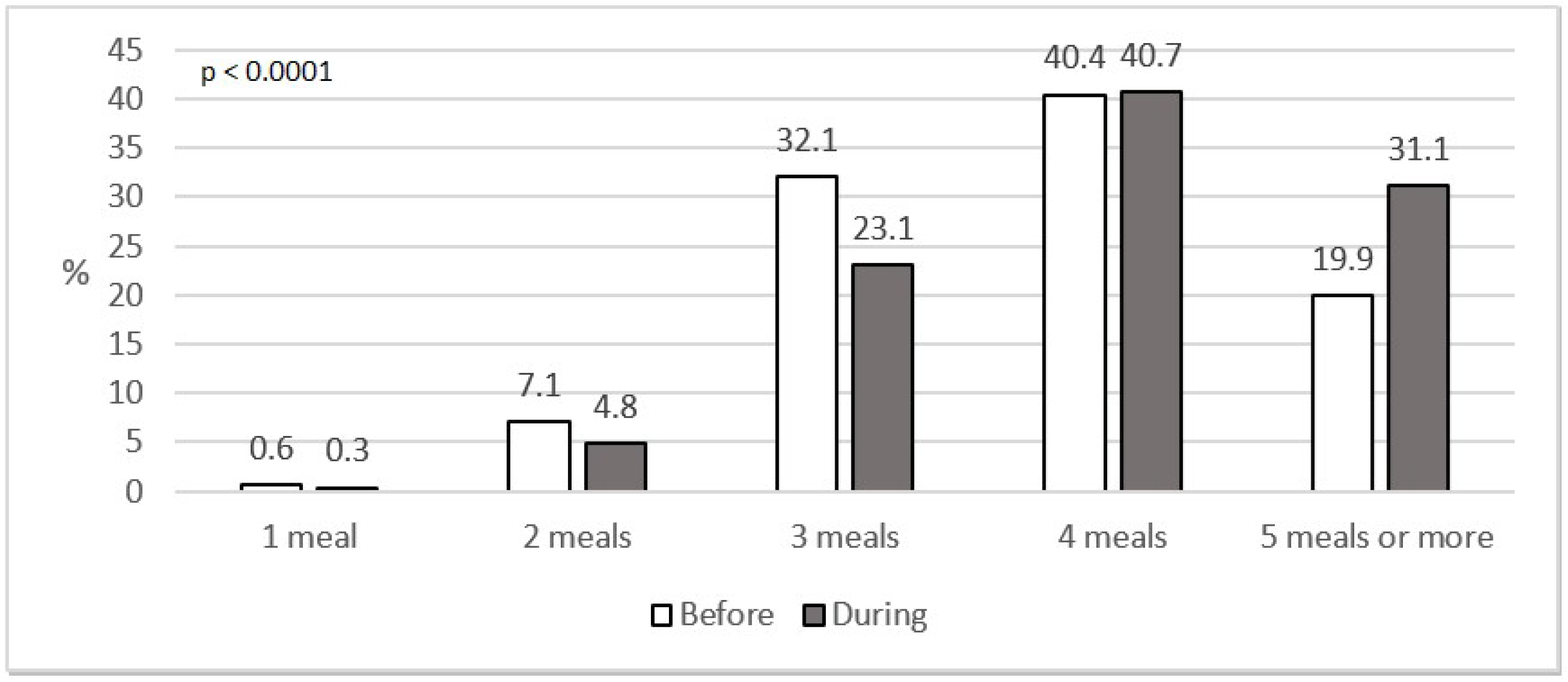
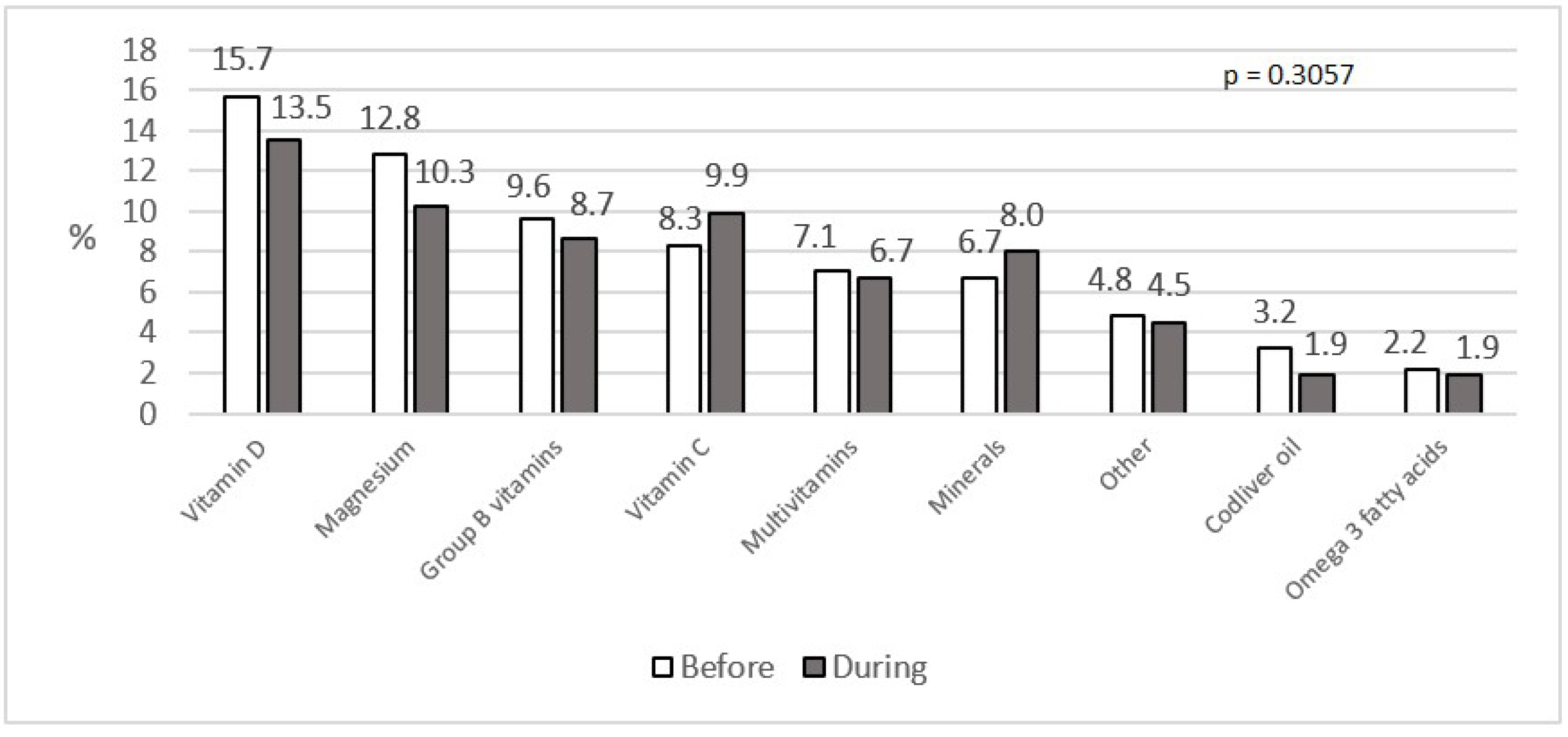
3.3. Eating Habits of the Study Group before and during Confinement
3.4. Limitations
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kowalska-Bobko, I.; Sowada, C.; Furman, M.; Gałązka-Sobotka, M. Policy Responses for Poland. Available online: https://www.covid19healthsystem.org/countries/poland/livinghit.aspx?Section=6.%20Measures%20in%20other%20sectors&Type=Chapter (accessed on 16 June 2020).
- Pinkas, J.; Jankowski, M.; Szumowski, Ł.; Lusawa, A.; Zgliczyński, W.S.; Raciborski, F.; Wierzba, W.; Gujski, M. Public Health Interventions to Mitigate Early Spread of SARS-CoV-2 in Poland. Med. Sci. Monit. 2020, 26, e924730. [Google Scholar] [CrossRef] [PubMed]
- Zabdyr-Jamróz, M.; Kowalska-Bobko, I. Poland’s Response to the Coronavirus «Economics» Cambridge Core Blog. Available online: https://0-www-cambridge-org.brum.beds.ac.uk/core/blog/2020/05/19/polands-response-to-the-coronavirus-pandemic/?fbclid=IwAR1dEeJofRlVuPW2hwjlNdQdILmXMDDXr1Opt1Z6xzhPwSkJTDDlbluE9-Y (accessed on 16 June 2020).
- Johns Hopkins Coronavirus Resource Center COVID-19 Map. Available online: https://0-coronavirus-jhu-edu.brum.beds.ac.uk/map.html (accessed on 22 September 2020).
- Połowa Polaków w Czasie Pandemii Koronawirusa Pracuje bez Zmian. 8 Proc. Straciło już Pracę. Available online: https://www.wirtualnemedia.pl/artykul/jak-polacy-pracuja-w-czasie-epidemii-koronawirusa-badanie-polowa-pracuje-bez-zmain-8-proc-bez-pracy (accessed on 16 June 2020).
- Cox, C.E. Role of Physical Activity for Weight Loss and Weight Maintenance. Diabetes Spectr. 2017, 30, 157–160. [Google Scholar] [CrossRef] [Green Version]
- Chen, P.; Mao, L.; Nassis, G.P.; Harmer, P.; Ainsworth, B.E.; Li, F. Coronavirus disease (COVID-19): The need to maintain regular physical activity while taking precautions. J. Sport Health Sci. 2020, 9, 103–104. [Google Scholar] [CrossRef]
- Butler, M.J.; Barrientos, R.M. The impact of nutrition on COVID-19 susceptibility and long-term consequences. Brain Behav. Immun. 2020. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus: No Evidence That Food Is a Source or Transmission Route. Available online: http://www.efsa.europa.eu/en/news/coronavirus-no-evidence-food-source-or-transmission-route (accessed on 19 June 2020).
- Bezpieczeństwo Żywności w Dobie Epidemii Koronawirusa Narodowe Centrum Edukacji Żywieniowej. Available online: https://ncez.pl/abc-zywienia-/zasady-zdrowego-zywienia/bezpieczenstwo-zywnosci-w-dobie-epidemii-koronawirusa (accessed on 19 June 2020).
- Q&A Dotyczące Żywności i Koronawirusa—Aktualizacja 11/05/2020. Available online: https://gis.gov.pl/zywnosc-i-woda/zywnosc-zywnosc-i-woda/qa-dotyczace-zywnosci-i-koronawirusa-aktualizacja-28-04-2020/ (accessed on 19 June 2020).
- Prawo Żywnościowe—Blog—O Prawie Żywnościowym Prawie Wszystko. Available online: https://www.prawo-zywnosciowe.pl/ (accessed on 19 June 2020).
- Pallus, P. Branża Handlowa: Nie ma Obaw o Brak Żywności w Kraju. Available online: //businessinsider.com.pl/finanse/handel/koronawirus-w-polsce-dostawy-do-sklepow-sa-zapewnione/03dm6jj (accessed on 19 June 2020).
- Departament Handlu i Usług. Dynamika Sprzedaży Detalicznej w Kwietniu 22.05.2020 r. Available online: https://stat.gov.pl/obszary-tematyczne/ceny-handel/handel/dynamika-sprzedazy-detalicznej-w-kwietniu-2020-roku,14,64.html (accessed on 22 September 2020).
- Zabetakis, I.; Lordan, R.; Norton, C.; Tsoupras, A. COVID-19: The Inflammation Link and the Role of Nutrition in Potential Mitigation. Nutrients 2020, 12, 1466. [Google Scholar] [CrossRef] [PubMed]
- Naja, F.; Hamadeh, R. Nutrition amid the COVID-19 pandemic: A multi-level framework for action. Eur. J. Clin. Nutr. 2020, 74, 1117–1121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Górnicka, M.; Drywień, M.E.; Zielinska, M.A.; Hamułka, J. Dietary and Lifestyle Changes During COVID-19 and the Subsequent Lockdowns among Polish Adults: A Cross-Sectional Online Survey PLifeCOVID-19 Study. Nutrients 2020, 12, 2324. [Google Scholar] [CrossRef] [PubMed]
- Sidor, A.; Rzymski, P. Dietary Choices and Habits during COVID-19 Lockdown: Experience from Poland. Nutrients 2020, 12, 1657. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Food and Nutrition Tips during Self-Quarantine. Available online: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/technical-guidance/food-and-nutrition-tips-during-self-quarantine (accessed on 22 September 2020).
- Jeżewska-Zychowicz, M.; Gawęcki, J.; Wądołowska, L.; Czarnocińska, J.; Galiński, G.; Kollajtis-Dolowy, A.; Roszkowski, W.; Wawrzyniak, A.; Przybyłowicz, K.; Krusinska, B.; et al. Dietary Habits and Nutrition Beliefs Questionnaire for People 15–65 Years Old, Version 1.1.—Interviewer Administered Questionnaire. Chapter 1. In Dietary Habits and Nutrition Beliefs Questionnaire and the Manual for Developing of Nutritional Data; The Committee of Human Nutrition, Polish Academy of Sciences: Olsztyn, Poland, 2018. [Google Scholar]
- Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 4 July 2020).
- Rozporządzenie Ministra Edukacji Narodowej z dnia 28 maja 2020 r. Zmieniające Rozporządzenie w Sprawie Czasowego Ograniczenia Funkcjonowania Jednostek Systemu Oświaty w Związku z Zapobieganiem, Przeciwdziałaniem i Zwalczaniem COVID-19 2020. Available online: https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20200000953 (accessed on 19 June 2020).
- Rozporządzenie Ministra Kultury i Dziedzictwa Narodowego z dnia 23 Marca 2020 r. w Sprawie Czasowego Ograniczenia Funkcjonowania Uczelni Artystycznych w Związku z Zapobieganiem, Przeciwdziałaniem i Zwalczaniem COVID-19 2020. Available online: http://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20200000516 (accessed on 19 June 2020).
- Rozporządzenie Ministra Nauki i Szkolnictwa Wyższego z dnia 11 Marca 2020 r. w Sprawie Czasowego Ograniczenia Funkcjonowania Niektórych Podmiotów Systemu Szkolnictwa Wyższego i Nauki w Związku z Zapobieganiem, Przeciwdziałaniem i Zwalczaniem COVID-19 2020. Available online: https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20200000405 (accessed on 19 June 2020).
- Frontczak, J. Raport PMR: Wpływ COVID-19 na Zmiany Zachowań Konsumentów. Available online: https://retailmarketexperts.com/ (accessed on 19 June 2020).
- Eating Habit Changes during Lockdown in Great Britain. 2020. Available online: https://0-www-statista-com.brum.beds.ac.uk/statistics/1114594/eating-habit-changes-during-lockdown-in-great-britain/ (accessed on 19 June 2020).
- Todd, J.E.; Mancino, L.; Lin, B.-H. The Impact of Food away from Home on Adult Diet Quality. SSRN J. 2010. [Google Scholar] [CrossRef] [Green Version]
- WHO EMRO | Nutrition Advice for Adults during the COVID-19 Outbreak | Nutrition-Infocus | Nutrition. Available online: http://www.emro.who.int/nutrition/nutrition-infocus/nutrition-advice-for-adults-during-the-covid-19-outbreak.html (accessed on 19 June 2020).
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef] [PubMed]
- Schoenfeld, B.J.; Aragon, A.A.; Krieger, W.J. Effects of meal frequency on weight loss and body composition: A meta-analysis. Nutr. Rev. 2015, 73, 69–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghosh, A.; Arora, B.; Gupta, R.; Anoop, S.; Misra, A. Effects of nationwide lockdown during COVID-19 epidemic on lifestyle and other medical issues of patients with type 2 diabetes in north India. Diabetes Metab. Syndr. 2020. [Google Scholar] [CrossRef] [PubMed]
- Pietrobelli, A.; Pecoraro, L.; Ferruzzi, A.; Heo, M.; Faith, M.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; Fearnbach, S.N.; Heymsfield, S.B. Effects of COVID-19 Lockdown on Lifestyle Behaviors in Children with Obesity Living in Verona, Italy: A Longitudinal Study. Obesity 2020. [Google Scholar] [CrossRef] [PubMed]
- Piramida Zdrowego Żywienia i Aktywności Fizycznej dla Osób Dorosłych Narodowe Centrum Edukacji Żywieniowej. Available online: https://ncez.pl/abc-zywienia-/zasady-zdrowego-zywienia/piramida-zdrowego-zywienia-i-aktywnosci-fizycznej-dla-osob-doroslych (accessed on 19 June 2020).
- Jribi, S.; Ben Ismail, H.; Doggui, D.; Debbabi, H. COVID-19 virus outbreak lockdown: What impacts on household food wastage? Environ. Dev. Sustain. 2020, 22, 3939–3955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. J. Trans. Med. 2020, 18, 229. [Google Scholar] [CrossRef] [PubMed]
- Guelinckx, I.; Ferreira-Pêgo, C.; Moreno, L.A.; Kavouras, S.A.; Gandy, J.; Martinez, H.; Bardosono, S.; Abdollahi, M.; Nasseri, E.; Jarosz, A.; et al. Intake of water and different beverages in adults across 13 countries. Eur. J. Nutr. 2015, 54, 45–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GUS. In Mały Rocznik Statystyczny Polski; 2019. Available online: https://stat.gov.pl/obszary-tematyczne/roczniki-statystyczne/roczniki-statystyczne/maly-rocznik-statystyczny-polski-2019,1,21.html (accessed on 22 September 2020).
- Rusińska, A.; Płudowski, P.; Walczak, M.; Borszewska-Kornacka, M.K. Vitamin D supplementation guidelines for Poland—A 2018 update. Medicine 2018, 2018, 1–24. [Google Scholar] [CrossRef]
- Dziedziński, M.; Goryńska-Goldman, E.; Kobus-Cisowska, J.; Szczepaniak, O.; Marciniak, G. Problem nadkonsumpcji suplementów diety przez Polaków. Intercathedra 2019, 3, 235–242. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N | % |
|---|---|---|
| Age (years) | ||
| ≤24 | 27 | 8.7 |
| 25–65 | 263 | 84.2 |
| ≥66 | 22 | 7.1 |
| Gender | ||
| Female | 200 | 64.1 |
| Male | 112 | 35.9 |
| Place of living | ||
| Village | 69 | 22.3 |
| Town <20,000 citizens | 30 | 9.7 |
| Town >20,000–100,000 citizens | 48 | 15.5 |
| City >100,000 citizens | 162 | 52.5 |
| Occupation | ||
| Unemployed | 11 | 3.6 |
| Student | 25 | 8.1 |
| Employed | 243 | 78.6 |
| Retired | 30 | 9.7 |
| Level of education | ||
| Primary | 3 | 1 |
| Vocational | 7 | 2.3 |
| Secondary | 65 | 21.2 |
| Higher | 232 | 75.5 |
| Nutritional Status | Before Confinement | During Confinement | p-Value |
|---|---|---|---|
| Underweight, n (%) | 6 (2.1) | 7 (2.3) | |
| Normal weight, n (%) | 154 (53.3) | 153 (50.8) | 0.7213 |
| Overweight, n (%) | 94 (32.5) | 101 (33.6) | |
| Obese, n (%) | 35 (12.1) | 40 (13.3) |
| Answers to the Question: In Your Opinion, Has Your Diet Changed Due to the Social Isolation? | N | % |
|---|---|---|
| No, I was eating the same kind and quantity of food. | 101 | 32.4 |
| Yes, I was eating the same products, but in greater quantities. | 57 | 18.3 |
| Yes, I was eating the same products, but in smaller quantities. | 30 | 9.6 |
| Yes, I have changed my product range without changing the quantity. | 48 | 15.4 |
| Yes, I have changed my product range and I eat less. | 31 | 9.9 |
| Yes, I have changed my product range and I eat more. | 45 | 14.4 |
| Food Product | Time | Never | 1–3 Times a Month | Once a Week | Few Times a Week | Once a Day | Few Times a Day | p-Value |
|---|---|---|---|---|---|---|---|---|
| White bread | B D | 6.7 6.1 | 9.6 8.7 | 11.9 16.3 | 29.5 30.1 | 21.8 18.3 | 20.5 20.5 | 0.3737 |
| Wholemeal bread | B D | 16.3 20.5 | 22.1 13.1 | 11.2 16.0 | 25.6 28.8 | 16.7 14.7 | 8.0 6.7 | 0.5118 |
| White rice, white pasta | B D | 5.4 6.1 | 15.7 16.7 | 29.2 26.0 | 42.3 45.2 | 6.4 5.8 | 1.0 0.3 | 0.7314 |
| Buckwheat, oats | B D | 9.6 11.2 | 23.1 17.0 | 21.5 24.7 | 36.5 36.9 | 7.4 7.7 | 1.9 2.6 | 0.2765 |
| Butter | B D | 12.8 10.3 | 9.0 6.7 | 8.0 11.2 | 23.4 27.2 | 21.2 22.4 | 25.6 22.1 | 0.7000 |
| Lard | B D | 73.7 76.0 | 16.7 10.6 | 3.8 6.4 | 3.8 4.2 | 1.6 2.6 | 0.3 0.3 | 0.2404 |
| Oils or margarines | B D | 20.2 18.3 | 15.7 14.1 | 16.0 14.4 | 31.7 38.1 | 11.9 11.9 | 4.5 3.2 | 0.1060 |
| Milk | B D | 16.0 16.7 | 15.4 13.1 | 7.1 7.4 | 19.9 21.2 | 25.0 25.3 | 16.8 16.3 | 0.8312 |
| Fermented milk | B D | 9.9 11.2 | 19.6 17.0 | 12.8 18.3 | 38.1 33.0 | 16.3 17.9 | 3.2 2.6 | 0.4454 |
| Fresh cheeses | B D | 11.5 11.9 | 20.2 16.7 | 21.2 22.1 | 37.5 41.0 | 8.3 8.0 | 1.3 0.3 | 0.6004 |
| Cheeses | B D | 5.1 6.7 | 13.8 12.2 | 20.8 17.6 | 45.2 44.9 | 11.5 14.1 | 3.5 4.5 | 0.2293 |
| Cold meats | B D | 10.3 9.0 | 9.9 10.6 | 20.5 20.5 | 41.7 42.0 | 10.6 12.5 | 7.1 5.4 | 0.9189 |
| Red meats | B D | 12.8 17.9 | 30.4 23.4 | 28.8 34.3 | 26.3 22.8 | 1.6 1.3 | 0.0 0.3 | 0.1745 |
| White meats | B D | 7.1 6.1 | 10.9 12.2 | 26.3 27.2 | 53.8 51.9 | 1.6 1.9 | 0.3 0.6 | 0.9940 |
| Fishes | B D | 8.7 11.5 | 40.7 38.5 | 41.7 33.7 | 8.7 14.7 | 0.0 1.3 | 0.3 0.3 | 0.1531 |
| Eggs | B D | 2.6 1.6 | 9.6 7.4 | 26.3 24.0 | 54.2 55.8 | 5.4 9.6 | 1.9 1.6 | 0.0022 |
| Pulses | B D | 19.2 25.3 | 50.0 40.7 | 17.0 18.9 | 11.9 13.5 | 1.9 1.3 | 0.0 0.3 | 0.7694 |
| Potatoes | B D | 4.8 5.1 | 18.6 10.3 | 26.9 26.6 | 44.2 51.6 | 4.5 6.1 | 1.0 0.3 | 0.0004 |
| Fruits | B D | 0.6 1.6 | 5.8 7.1 | 11.9 10.3 | 34.9 33.7 | 31.1 30.1 | 15.7 17.3 | 0.6880 |
| Vegetables | B D | 0.6 1.0 | 2.6 3.8 | 9.0 7.4 | 32.1 33.3 | 28.5 27.6 | 27.2 26.9 | 0.4241 |
| Fast foods | B D | 25.6 41.7 | 57.4 42.0 | 10.6 11.5 | 6.1 4.2 | 0.0 0.6 | 0.3 0.0 | 0.0001 |
| Fried foods | B D | 6.7 9.3 | 28.5 23.1 | 29.2 29.2 | 33.3 36.5 | 1.6 0.0 | 0.6 1.9 | 0.5751 |
| Sweets | B D | 5.4 7.4 | 19.9 16.0 | 16.7 15.4 | 38.1 34.0 | 13.8 16.0 | 6.1 11.2 | 0.0241 |
| Instant soups | B D | 74.7 78.2 | 16.0 15.1 | 5.1 3.8 | 2.6 2.6 | 1.3 0.3 | 0.3 0.0 | 0.0247 |
| Tinned meats | B D | 73.1 68.3 | 20.2 19.2 | 5.1 9.3 | 1.0 2.6 | 0.3 0.6 | 0.3 0.0 | 0.0004 |
| Tinned vegetables | B D | 23.7 27.9 | 27.6 20.8 | 23.1 22.1 | 23.1 23.4 | 2.2 4.2 | 0.3 1.6 | 0.2190 |
| Beverage | Time | Never | 1–3 Times a Month | Once a Week | Few Times a Week | Once a Day | Few Times a Day | p-Value |
| Fruit juices | B | 25.0 | 27.9 | 16.0 | 20.5 | 7.7 | 2.9 | 0.5520 |
| D | 33.7 | 19.6 | 15.7 | 18.3 | 7.4 | 5.4 | ||
| Vegetable juices | B | 45.8 | 30.1 | 9.3 | 10.9 | 2.9 | 1.0 | 0.4047 |
| D | 55.4 | 19.2 | 9.6 | 10.3 | 3.5 | 1.9 | ||
| Hot beverages | B | 1.9 | 3.2 | 1.3 | 5.1 | 16.0 | 72.4 | 0.1500 |
| D | 1.3 | 3.5 | 1.6 | 7.1 | 16.3 | 70.2 | ||
| Sweetened beverages | B | 44.6 | 29.2 | 11.9 | 10.3 | 2.9 | 1.3 | 0.7253 |
| D | 49.0 | 24.4 | 11.2 | 11.2 | 2.2 | 1.9 | ||
| Energy drinks | B | 78.5 | 14.7 | 1.6 | 4.2 | 0.3 | 0.6 | 0.0150 |
| D | 85.3 | 8.3 | 3.2 | 1.9 | 0.6 | 0.6 | ||
| Mineral water | B | 0.0 | 4.8 | 2.6 | 10.3 | 13.1 | 66.0 | 0.6431 |
| D | 5.4 | 3.2 | 2.2 | 8.0 | 11.5 | 69.6 | ||
| Alcohols | B | 21.8 | 37.8 | 19.6 | 16.0 | 3.8 | 1.0 | 0.0031 |
| D | 25.6 | 26.0 | 19.9 | 22.2 | 5.4 | 1.0 |
| Food Product | Time | 0 Serving | 0.5 Serving | 1 Serving | 2 Servings | 3 Servings | 4 Servings | 5 Servings | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| White bread | B | 7.4 | 28.8 | 23.4 | 17.6 | 1.9 | 10.9 | 9.9 | 0.0400 |
| D | 6.4 | 34.9 | 23.4 | 13.8 | 4.2 | 7.1 | 10.3 | ||
| Wholemeal bread | B | 16.7 | 41.7 | 20.8 | 12.2 | 1.9 | 2.6 | 4.2 | 0.1155 |
| D | 20.8 | 38.5 | 21.5 | 11.9 | 1.0 | 4.2 | 2.2 | ||
| White rice, white pasta | B | 5.4 | 71.8 | 19.9 | 1.9 | 0.0 | 1.0 | 0.0 | 0.3913 |
| D | 6.4 | 69.9 | 19.2 | 2.9 | 1.0 | 0.6 | 0.0 | ||
| Buckwheat, oats | B | 9.6 | 68.3 | 16.0 | 3.2 | 1.0 | 1.3 | 0.6 | 0.7467 |
| D | 11.5 | 64.7 | 16.7 | 5.1 | 0.0 | 1.0 | 1.0 | ||
| Butter | B | 13.1 | 31.7 | 19.9 | 16.0 | 1.6 | 8.3 | 9.3 | 0.1506 |
| D | 10.6 | 34.3 | 22.1 | 17.0 | 2.2 | 6.1 | 7.7 | ||
| Lard | B | 74.0 | 22.8 | 2.2 | 0.6 | 0.0 | 0.3 | 0.0 | 0.5520 |
| D | 76.6 | 18.6 | 3.5 | 0.6 | 0.3 | 0.0 | 0.3 | ||
| Oils or margarines | B | 20.8 | 47.8 | 18.9 | 7.1 | 2.2 | 1.3 | 1.9 | 0.5037 |
| D | 18.6 | 46.5 | 22.8 | 7.7 | 2.2 | 1.6 | 0.6 | ||
| Milk | B | 16.7 | 40.4 | 26.3 | 10.3 | 0.3 | 3.5 | 2.6 | 0.6404 |
| D | 16.7 | 39.1 | 27.9 | 9.0 | 0.3 | 3.2 | 3.8 | ||
| Fermented milk | B | 10.3 | 62.2 | 19.6 | 5.8 | 0.6 | 1.3 | 0.3 | 0.4484 |
| D | 11.2 | 62.2 | 19.9 | 4.5 | 1.0 | 1.0 | 0.3 | ||
| Fresh cheeses | B | 11.9 | 59.3 | 20.5 | 6.1 | 1.0 | 1.0 | 0.3 | 0.0960 |
| D | 11.9 | 60.9 | 22.4 | 3.8 | 0.3 | 0.6 | 0.0 | ||
| Cheeses | B | 5.4 | 53.2 | 28.2 | 7.4 | 2.2 | 1.6 | 1.9 | 0.7206 |
| D | 6.7 | 51.3 | 28.5 | 8.0 | 1.3 | 1.9 | 2.2 | ||
| Cold meats | B | 10.3 | 49.0 | 25.0 | 9.0 | 1.0 | 3.8 | 1.9 | 0.8761 |
| D | 9.3 | 49.7 | 25.3 | 9.0 | 2.2 | 3.2 | 1.3 | ||
| Red meats | B | 13.1 | 74.0 | 11.5 | 0.6 | 0.3 | 0.3 | 0.0 | 0.0199 |
| D | 18.6 | 68.9 | 11.5 | 1.0 | 0.0 | 0.0 | 0.0 | ||
| White meats | B | 7.1 | 66.3 | 22.8 | 2.9 | 0.6 | 0.0 | 0.3 | 0.4011 |
| D | 6.4 | 68.6 | 22.8 | 1.3 | 0.6 | 0.0 | 0.3 | ||
| Fishes | B | 8.7 | 87.5 | 2.9 | 1.0 | 0.0 | 0.0 | 0.0 | 0.7827 |
| D | 11.9 | 79.8 | 7.7 | 0.6 | 0.0 | 0.0 | 0.0 | ||
| Eggs | B | 2.9 | 55.1 | 31.4 | 7.4 | 1.3 | 1.3 | 0.6 | 0.2399 |
| D | 1.9 | 47.4 | 40.7 | 8.0 | 1.0 | 0.0 | 1.0 | ||
| Pulses | B | 19.2 | 74.0 | 5.4 | 1.3 | 0.0 | 0.0 | 0.0 | 0.2129 |
| D | 25.3 | 67.0 | 5.4 | 2.2 | 0.0 | 0.0 | 0.0 | ||
| Potatoes | B | 4.8 | 63.1 | 25.6 | 4.8 | 0.3 | 0.3 | 1.0 | 0.3020 |
| D | 5.1 | 58.3 | 30.4 | 4.8 | 1.0 | 0.3 | 5.1 | ||
| Fruits | B | 0.6 | 36.9 | 29.5 | 19.2 | 4.2 | 4.5 | 5.1 | 0.6376 |
| D | 1.6 | 33.0 | 35.6 | 17.0 | 2.2 | 5.1 | 5.4 | ||
| Vegetables | B | 0.6 | 31.1 | 27.6 | 18.6 | 3.8 | 7.4 | 10.9 | 0.4464 |
| D | 1.0 | 34.0 | 26.6 | 16.3 | 4.2 | 8.3 | 9.6 | ||
| Fast foods | B | 26.0 | 67.6 | 6.1 | 0.3 | 0.0 | 0.0 | 0.0 | <0.0001 |
| D | 41.7 | 54.8 | 2.9 | 0.3 | 0.3 | 0.0 | 0.0 | ||
| Fried foods | B | 7.1 | 75.6 | 14.4 | 1.9 | 0.6 | 0.3 | 0.0 | 0.2618 |
| D | 9.3 | 73.7 | 15.1 | 1.0 | 1.0 | 0.0 | 0.0 | ||
| Sweets | B | 5.8 | 66.0 | 19.2 | 4.5 | 1.0 | 1.6 | 1.9 | 0.0029 |
| D | 7.4 | 58.0 | 18.9 | 7.7 | 1.0 | 3.5 | 3.5 | ||
| Instant soups | B | 74.7 | 23.4 | 1.0 | 0.6 | 0.3 | 0.0 | 0.0 | 0.0283 |
| D | 78.2 | 20.8 | 1.0 | 0.0 | 0.0 | 0.0 | 0.0 | ||
| Tinned meats | B | 73.1 | 25.6 | 1.3 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0390 |
| D | 68.6 | 30.8 | 0.3 | 0.0 | 0.3 | 0.0 | 0.0 | ||
| Tinned vegetables | BD | 23.727.9 | 66.759.6 | 7.79.6 | 1.91.9 | 0.00.0 | 0.00.0 | 0.01.0 | 0.8251 |
| Beverage | Time | 0 Serving | 0.5 Serving | 1 Serving | 2 Servings | 3 Servings | 4 Servings | 5 Servings | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| Fruit juices | B | 25.6 | 55.8 | 13.5 | 2.2 | 0.6 | 1.3 | 1.0 | 0.4344 |
| D | 34.0 | 46.8 | 13.5 | 2.2 | 0.0 | 1.0 | 2.6 | ||
| Vegetable juices | B | 46.5 | 45.8 | 5.8 | 0.6 | 0.3 | 0.6 | 0.3 | 0.0749 |
| D | 55.8 | 34.3 | 7.4 | 1.3 | 0.3 | 0.6 | 0.3 | ||
| Hot beverages | B | 1.9 | 7.4 | 10.6 | 29.5 | 1.6 | 10.9 | 38.1 | 0.1237 |
| D | 1.3 | 8.0 | 12.2 | 30.1 | 1.3 | 13.1 | 34.0 | ||
| Sweetened beverages | B | 44.6 | 44.9 | 6.1 | 3.2 | 0.3 | 0.3 | 0.6 | 0.0254 |
| D | 49.4 | 42.0 | 5.8 | 1.3 | 0.0 | 1.6 | 0.0 | ||
| Energy drinks | B | 78.5 | 18.3 | 2.2 | 0.3 | 0.0 | 0.0 | 0.6 | 0.0008 |
| D | 85.3 | 13.5 | 0.3 | 0.0 | 0.0 | 0.6 | 0.3 | ||
| Mineral water | B | 3.2 | 11.2 | 16.7 | 19.9 | 1.0 | 11.5 | 36.5 | 0.6482 |
| D | 5.8 | 10.9 | 12.2 | 21.2 | 0.6 | 12.2 | 37.2 | ||
| Alcohol | B | 22.1 | 59.9 | 13.8 | 2.9 | 0.3 | 0.6 | 0.3 | 0.1859 |
| D | 25.6 | 51.9 | 16.7 | 3.5 | 1.3 | 0.3 | 0.6 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Błaszczyk-Bębenek, E.; Jagielski, P.; Bolesławska, I.; Jagielska, A.; Nitsch-Osuch, A.; Kawalec, P. Nutrition Behaviors in Polish Adults before and during COVID-19 Lockdown. Nutrients 2020, 12, 3084. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12103084
Błaszczyk-Bębenek E, Jagielski P, Bolesławska I, Jagielska A, Nitsch-Osuch A, Kawalec P. Nutrition Behaviors in Polish Adults before and during COVID-19 Lockdown. Nutrients. 2020; 12(10):3084. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12103084
Chicago/Turabian StyleBłaszczyk-Bębenek, Ewa, Paweł Jagielski, Izabela Bolesławska, Anna Jagielska, Aneta Nitsch-Osuch, and Paweł Kawalec. 2020. "Nutrition Behaviors in Polish Adults before and during COVID-19 Lockdown" Nutrients 12, no. 10: 3084. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12103084