
Causal Effects of Homocysteine, Folate, and Cobalamin on Kidney Function: A Mendelian Randomization Study

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Approval
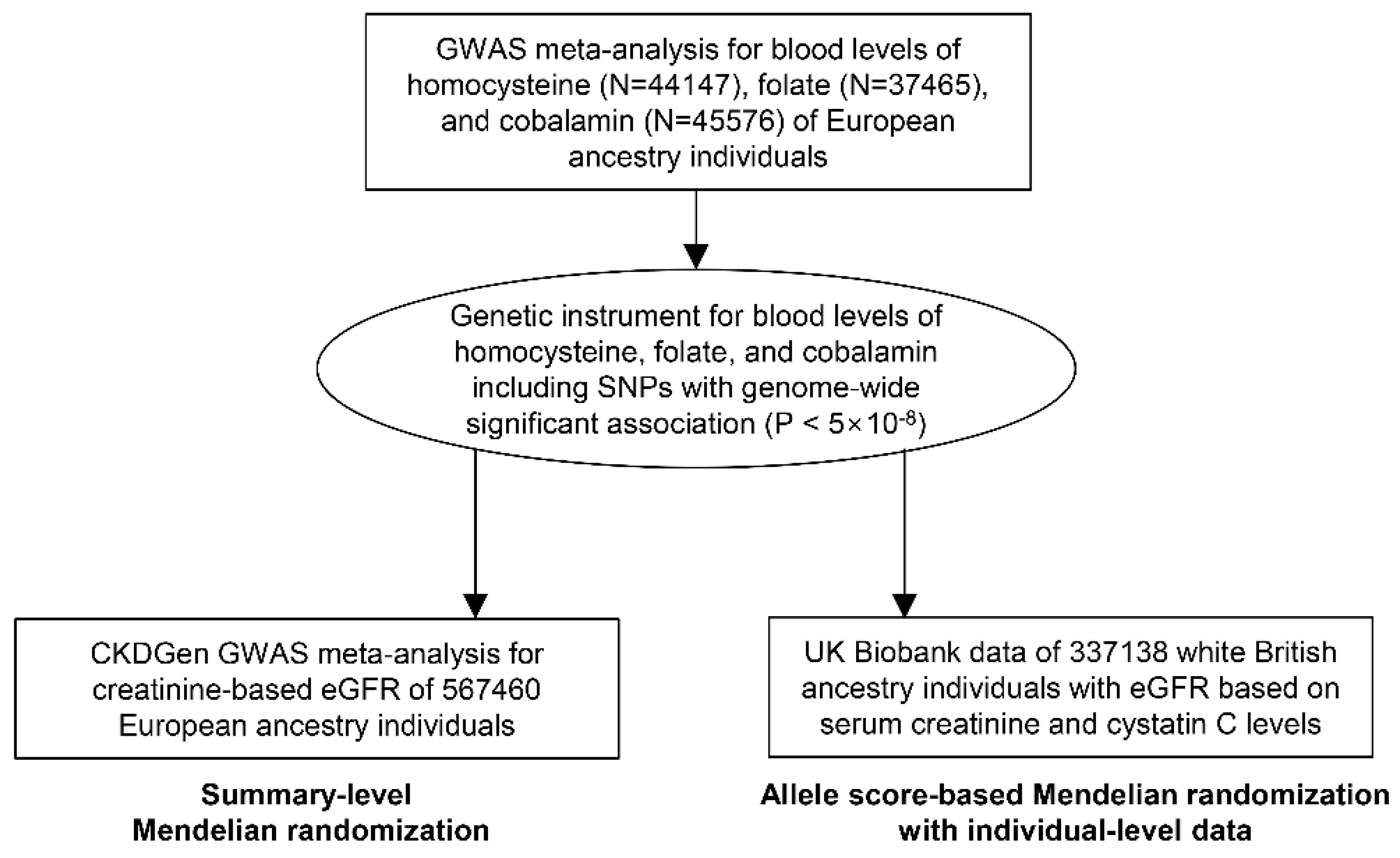
2.2. Study Setting
2.3. Genetic Instrument
2.4. Considerations for Key Assumption of MR
2.5. Summary-Level MR with the CKDGen Data
2.6. Allele-Score-Based MR with Individual-Level Data in the U.K. Biobank
3. Results
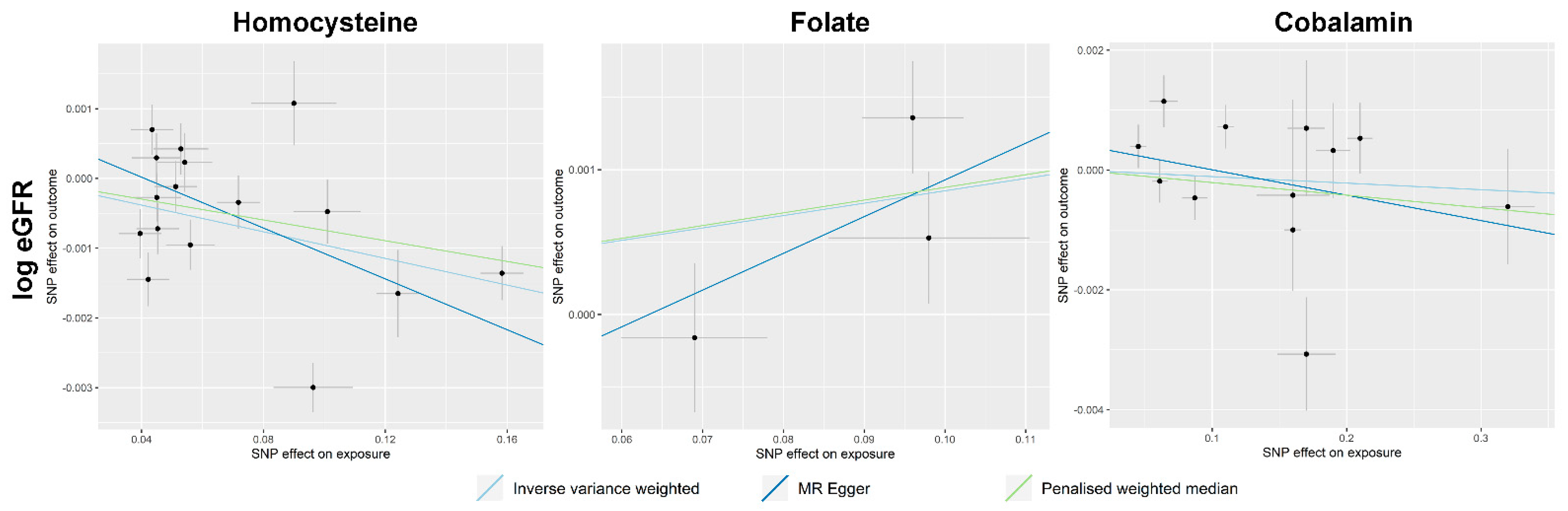
3.1. Summary-Level MR Results
3.2. Allele-Score-Based MR Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bikbov, B.; Purcell, C.A.; Levey, A.S.; Smith, M.; Abdoli, A.; Abebe, M.; Adebayo, O.M.; Afarideh, M.; Agarwal, S.K.; Agudelo-Botero, M.; et al. Global, regional, and national burden of chronic kidney disease, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [Green Version]
- Soinio, M.; Marniemi, J.; Laakso, M.; Lehto, S.; Rönnemaa, T. Elevated plasma homocysteine level is an independent predictor of coronary heart disease events in patients with type 2 diabetes mellitus. Ann. Intern. Med. 2004, 140, 94–100. [Google Scholar] [CrossRef] [Green Version]
- Nygård, O.; Nordrehaug, J.E.; Refsum, H.; Ueland, P.M.; Farstad, M.; Vollset, S.E. Plasma Homocysteine Levels and Mortality in Patients with Coronary Artery Disease. N. Engl. J. Med. 1997, 337, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Heinz, J.; Kropf, S.; Luley, C.; Dierkes, J. Homocysteine as a Risk Factor for Cardiovascular Disease in Patients Treated by Dialysis: A Meta–analysis. Am. J. Kidney Dis. 2009, 54, 478–489. [Google Scholar] [CrossRef] [PubMed]
- Moustapha, A.; Naso, A.; Nahlawi, M.; Gupta, A.; Arheart, K.L.; Jacobsen, D.W.; Robinson, K.; Dennis, V.W. Prospective study of hy-perhomocysteinemia as an adverse cardiovascular risk factor in end-stage renal disease. Circulation 1998, 97, 138–141. [Google Scholar] [CrossRef] [PubMed]
- Bostom, A.G.; Lathrop, L. Hyperhomocysteinemia in end-stage renal disease: Prevalence, etiology, and potential relationship to arteriosclerotic outcomes. Kidney Int. 1997, 52, 10–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, A.N.; Hunsicker, L.G.; Selhub, J.; Bostom, A.G. Total Plasma Homocysteine and Arteriosclerotic Outcomes in Type 2 Diabetes with Nephropathy. J. Am. Soc. Nephrol. 2005, 16, 3397–3402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menon, V.; Sarnak, M.J.; Greene, T.; Wang, X.; Pereira, A.A.; Beck, G.J.; Kusek, J.W.; Selhub, J.; Collins, A.J.; Levey, A.S.; et al. Relationship Between Homocysteine and Mortality in Chronic Kidney Disease. Circulation 2006, 113, 1572–1577. [Google Scholar] [CrossRef]
- Huo, Y.; Li, J.; Qin, X.; Huang, Y.; Wang, X.; Gottesman, R.F.; Tang, G.; Wang, B.; Chen, D.; He, M.; et al. Efficacy of folic acid therapy in primary prevention of stroke among adults with hypertension in China: The CSPPT randomized clinical trial. JAMA 2015, 313, 1325–1335. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Qin, X.; Li, Y.; Sun, D.; Wang, J.; Liang, M.; Wang, B.; Huo, Y.; Hou, F.F. Efficacy of Folic Acid Therapy on the Progression of Chronic Kidney Disease: The Renal Substudy of the China Stroke Primary Prevention Trial. JAMA Intern. Med. 2016, 176, 1443–1450. [Google Scholar] [CrossRef]
- Martí-Carvajal, A.J.; Solà, I.; Lathyris, D.; Dayer, M. Homocysteine-lowering interventions for preventing cardiovascular events. Cochrane Database Syst. Rev. 2017, 8, Cd006612. [Google Scholar] [CrossRef] [PubMed]
- House, A.A.; Eliasziw, M.; Cattran, D.C.; Churchill, D.N.; Oliver, M.J.; Fine, A.; Dresser, G.K.; Spence, J.D. Effect of B-vitamin therapy on progression of diabetic nephropathy: A randomized controlled trial. JAMA 2010, 303, 1603–1609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, N.M.; Holmes, M.V.; Smith, G.D. Reading Mendelian randomisation studies: A guide, glossary, and checklist for clinicians. BMJ 2018, 362, k601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsson, S.C.; Traylor, M.; Markus, H.S. Homocysteine and small vessel stroke: A mendelian randomization analysis. Ann. Neurol. 2019, 85, 495–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.; Lee, S.; Kim, Y.; Lee, Y.; Kang, M.W.; Kim, K.; Kim, Y.C.; Han, S.S.; Lee, H.; Lee, J.P.; et al. Short or Long Sleep Duration and CKD: A Mendelian Randomization Study. J. Am. Soc. Nephrol. 2020, 31, 2937–2947. [Google Scholar] [CrossRef] [PubMed]
- van Meurs, J.B.; Pare, G.; Schwartz, S.M.; Hazra, A.; Tanaka, T.; Vermeulen, S.H.; Cotlarciuc, I.; Yuan, X.; Mälarstig, A.; Bandinelli, S.; et al. Common genetic loci influencing plasma homocysteine concentrations and their effect on risk of coronary artery disease. Am. J. Clin. Nutr. 2013, 98, 668–676. [Google Scholar] [CrossRef] [PubMed]
- Grarup, N.; Sulem, P.; Sandholt, C.H.; Thorleifsson, G.; Ahluwalia, T.S.; Steinthorsdottir, V.; Bjarnason, H.; Gudbjartsson, D.F.; Magnusson, O.T.; Sparsø, T.; et al. Genetic Architecture of Vitamin B12 and Folate Levels Uncovered Applying Deeply Sequenced Large Datasets. PLoS Genet. 2013, 9, e1003530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wuttke, M.; Li, Y.; Li, M.; Sieber, K.B.; Feitosa, M.F.; Gorski, M.; Tin, A.; Wang, L.; Chu, A.Y.; Hoppmann, A.; et al. A catalog of genetic loci associated with kidney function from analyses of a million individuals. Nat. Genet. 2019, 51, 957–972. [Google Scholar] [CrossRef] [Green Version]
- Bowden, J.K.; Smith, G.D.; Burgess, S. Mendelian randomization with invalid instruments: Effect estimation and bias detection through Egger regression. Int. J. Epidemiol. 2015, 44, 512–525. [Google Scholar] [CrossRef] [Green Version]
- Bowden, J.; Smith, G.D.; Haycock, P.C.; Burgess, S. Consistent Estimation in Mendelian Randomization with Some Invalid Instruments Using a Weighted Median Estimator. Genet. Epidemiol. 2016, 40, 304–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartwig, F.P.; Davies, N.M.; Hemani, G.; Smith, G.D. Two-sample Mendelian randomization: Avoiding the downsides of a powerful, widely applicable but potentially fallible technique. Int. J. Epidemiol. 2016, 45, 1717–1726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemani, G.; Tilling, K.; Davey Smith, G. Orienting the causal relationship between imprecisely measured traits using GWAS summary data. PLoS Genet. 2017, 13, e1007081. [Google Scholar]
- Burgess, S.; Foley, C.N.; Allara, E.; Staley, J.R.; Howson, J.M.M. A robust and efficient method for Mendelian randomization with hundreds of genetic variants. Nat. Commun. 2020, 11, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, H.; Cheng, H.; Chen, W.; Sheng, X.; Levy, M.A.; Brown, M.J.; Tian, J. An evidence-based approach to globally assess the covari-ate-dependent effect of the MTHFR single nucleotide polymorphism rs1801133 on blood homocysteine: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2018, 107, 817–825. [Google Scholar] [CrossRef] [Green Version]
- Hemani, G.; Zheng, J.; Elsworth, B.; Wade, K.H.; Haberland, V.; Baird, D.; Laurin, C.; Burgess, S.; Bowden, J.; Langdon, R.; et al. The MR-Base platform supports systematic causal inference across the human phenome. eLife 2018, 7. [Google Scholar] [CrossRef]
- Bycroft, C.; Freeman, C.; Petkova, D.; Band, G.; Elliott, L.T.; Sharp, K.; Motyer, A.; Vukcevic, D.; Delaneau, O.; O’Connell, J.; et al. The UK Biobank resource with deep phenotyping and genomic data. Nat. Cell Biol. 2018, 562, 203–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sudlow, C.; Gallacher, J.; Allen, N.; Beral, V.; Burton, P.; Danesh, J.; Downey, P.; Elliott, P.; Green, J.; Landray, M.; et al. UK Biobank: An Open Access Resource for Identifying the Causes of a Wide Range of Complex Diseases of Middle and Old Age. PLoS Med. 2015, 12, e1001779. [Google Scholar] [CrossRef] [Green Version]
- Fry, A.; Littlejohns, T.J.; Sudlow, C.; Doherty, N.; Adamska, L.; Sprosen, T.; Collins, R.; E Allen, N. Comparison of Sociodemographic and Health-Related Characteristics of UK Biobank Participants with Those of the General Population. Am. J. Epidemiol. 2017, 186, 1026–1034. [Google Scholar] [CrossRef] [Green Version]
- Chang, C.C.; Chow, C.C.; Tellier, L.C.A.M.; Vattikuti, S.; Purcell, S.M.; Lee, J.J. Second-generation PLINK: Rising to the challenge of larger and richer datasets. GigaScience 2015, 4, 7. [Google Scholar] [CrossRef] [PubMed]
- Stamler, J.S.; Osborne, J.A.; Jaraki, O.; Rabbani, L.E.; Mullins, M.; Singel, D.; Loscalzo, J. Adverse vascular effects of homocysteine are modulated by endothelium-derived relaxing factor and related oxides of nitrogen. J. Clin. Investig. 1993, 91, 308–318. [Google Scholar] [CrossRef]
- Škovierová, H.; Vidomanová, E.; Mahmood, S.; Sopková, J.; Drgová, A.; Červeňová, T.; Halašová, E.; Lehotský, J. The Molecular and Cellular Effect of Homocysteine Metabolism Imbalance on Human Health. Int. J. Mol. Sci. 2016, 17, 1733. [Google Scholar] [CrossRef]
- Sen, U.; Mishra, P.K.; Tyagi, N.; Tyagi, S.C. Homocysteine to Hydrogen Sulfide or Hypertension. Cell Biophys. 2010, 57, 49–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Au-Yeung, K.K.; Woo, C.W.; Sung, F.L.; Yip, J.C.; Siow, Y.L.; O, K. Hyperhomocysteinemia activates nuclear factor-kappaB in endothelial cells via oxidative stress. Circ. Res. 2004, 94, 28–36. [Google Scholar] [CrossRef] [Green Version]
- Qin, X.; Huo, Y.; Langman, C.B.; Hou, F.; Chen, Y.; Matossian, D.; Xu, X.; Wang, X. Folic Acid Therapy and Cardiovascular Disease in ESRD or Advanced Chronic Kidney Disease: A Meta-Analysis. Clin. J. Am. Soc. Nephrol. 2010, 6, 482–488. [Google Scholar] [CrossRef] [PubMed]
- Bønaa, K.H.; Njølstad, I.; Ueland, P.M.; Schirmer, H.; Tverdal, A.; Steigen, T.; Wang, H.; Nordrehaug, J.E.; Arnesen, E.; Rasmussen, K. Homocysteine Lowering and Cardiovascular Events after Acute Myocardial Infarction. N. Engl. J. Med. 2006, 354, 1578–1588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burgess, S.; Butterworth, A.; Malarstig, A.; Thompson, S.G. Use of Mendelian randomisation to assess potential benefit of clinical intervention. BMJ 2012, 345, e7325. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Genetically Predicted Exposure | SNP | Effect Allele | Effect Allele Frequency | Beta | p Value |
|---|---|---|---|---|---|
| Homocysteine | rs1801133 | A | 0.34 | 0.1583 | 4.34E-104 |
| rs2275565 | T | 0.21 | −0.0542 | 1.96E-10 | |
| rs7422339 | A | 0.33 | 0.0864 | 4.58E-27 | |
| rs9369898 | A | 0.62 | 0.0449 | 2.17E-10 | |
| rs7130284 | T | 0.07 | −0.1242 | 1.88E-20 | |
| rs154657 | A | 0.47 | 0.0963 | 1.74E-43 | |
| rs234709 | T | 0.45 | −0.0718 | 3.90E-24 | |
| rs4660306 | T | 0.33 | 0.0435 | 2.33E-09 | |
| rs548987 | C | 0.13 | 0.0597 | 1.12E-08 | |
| rs42648 | A | 0.4 | −0.0395 | 1.97E-08 | |
| rs1801222 | A | 0.34 | 0.0453 | 8.43E-10 | |
| rs2251468 | A | 0.65 | −0.0512 | 1.28E-12 | |
| rs838133 | A | 0.45 | 0.0422 | 7.48E-09 | |
| rs12134663 | A | 0.8 | −0.101 | 2.54E-21 | |
| rs12780845 | A | 0.65 | 0.0529 | 7.80E-10 | |
| rs957140 | A | 0.45 | −0.045 | 2.43E-10 | |
| rs12921383 | T | 0.87 | −0.09 | 8.22E-11 | |
| rs2851391 | T | 0.47 | 0.056 | 1.70E-12 | |
| Folate | rs1801133 | G | 0.67 | 0.096 | 9.50E-53 |
| rs17421511 | G | 0.83 | 0.098 | 1.80E-15 | |
| rs652197 | C | 0.18 | 0.069 | 1.20E-14 | |
| Cobalamin | rs602662 | A | 0.6 | 0.16 | 2.40E-139 |
| rs34324219 | C | 0.88 | 0.21 | 1.10E-111 | |
| rs34528912 | T | 0.04 | 0.17 | 2.10E-15 | |
| rs117456053 | G | 0.98 | 0.16 | 1.90E-09 | |
| rs1801222 | G | 0.59 | 0.11 | 3.30E-75 | |
| rs56077122 | A | 0.33 | 0.087 | 4.80E-21 | |
| rs2336573 | T | 0.03 | 0.32 | 8.40E-59 | |
| rs1131603 | C | 0.055 | 0.19 | 4.90E-49 | |
| rs5753231 | C | 0.79 | 0.064 | 7.50E-10 | |
| rs41281112 | C | 0.95 | 0.17 | 8.90E-35 | |
| rs1141321 | C | 0.63 | 0.061 | 3.60E-26 | |
| rs3742801 | T | 0.29 | 0.045 | 1.70E-13 | |
| rs2270655 | G | 0.94 | 0.066 | 2.20E-13 | |
| rs12272669 | A | 0.0022 | 0.51 | 3.00E-09 |
| Genetically Predicted Exposure | MR Method | MR-Egger Intercept p Value | Beta of eGFR Change (%) and 95% CI | p Value for Causal Estimate |
|---|---|---|---|---|
| Homocysteine | Inverse variance weighted | 0.54 | −0.95 (−1.21, −0.69) | <0.001 |
| MR-Egger | −1.81 (−2.59, −1.02) | <0.001 | ||
| Penalized weighted median | −0.74 (−1.15, −0.33) | <0.001 | ||
| Contamination mixture | −0.60 (−1.09, −0.20) | <0.001 | ||
| Folate | Inverse variance weighted | 0.51 | 0.86 (0.30, 1.42) | 0.002 |
| MR-Egger | 2.57 (0.70, 4.47) | 0.001 | ||
| Penalized weighted median | 0.88 (0.20, 1.56) | 0.011 | ||
| Contamination mixture | 0.90 (0.10, 1.61) | <0.001 | ||
| Cobalamin | Inverse variance weighted | 0.33 | −0.11 (−0.33, 0.11) | 0.333 |
| MR-Egger | −0.42 (−0.84, 0.00) | 0.025 | ||
| Penalized weighted median | −0.21 (−0.59, 0.17) | 0.276 | ||
| Contamination mixture | −0.10 (−0.40, 0.20) | 0.092 |
| Outcome | Genetically Predicted Exposure | Main Analysis a | Clinical Covariates Adjusted b | ||
|---|---|---|---|---|---|
| Beta for eGFR (Continuous) and 95% CI | p | Beta for eGFR (Continuous) and 95% CI | p | ||
| eGFR (mL/min/1.73 m2) | Homocysteine | −0.108 (−0.148, −0.068) | 1.6 × 10−7 | −0.106 (−0.147, −0.066) | 2.3 × 10−7 |
| Folate | 0.067 (0.027, 0.108) | 0.001 | 0.061 (0.021, 0.101) | 0.003 | |
| Cobalamin | 0.005 (−0.035, 0.046) | 0.802 | 0.004 (−0.037, 0.044) | 0.855 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.; Lee, S.; Kim, Y.; Cho, S.; Kim, K.; Kim, Y.C.; Han, S.S.; Lee, H.; Lee, J.P.; Joo, K.W.; et al. Causal Effects of Homocysteine, Folate, and Cobalamin on Kidney Function: A Mendelian Randomization Study. Nutrients 2021, 13, 906. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13030906
Park S, Lee S, Kim Y, Cho S, Kim K, Kim YC, Han SS, Lee H, Lee JP, Joo KW, et al. Causal Effects of Homocysteine, Folate, and Cobalamin on Kidney Function: A Mendelian Randomization Study. Nutrients. 2021; 13(3):906. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13030906
Chicago/Turabian StylePark, Sehoon, Soojin Lee, Yaerim Kim, Semin Cho, Kwangsoo Kim, Yong Chul Kim, Seung Seok Han, Hajeong Lee, Jung Pyo Lee, Kwon Wook Joo, and et al. 2021. "Causal Effects of Homocysteine, Folate, and Cobalamin on Kidney Function: A Mendelian Randomization Study" Nutrients 13, no. 3: 906. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13030906