
Neuropsychological Learning Deficits as Predictors of Treatment Outcome in Patients with Eating Disorders

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.2.1. Decision-Making Assessment
2.2.2. Treatment
2.3. Data Analysis
3. Results
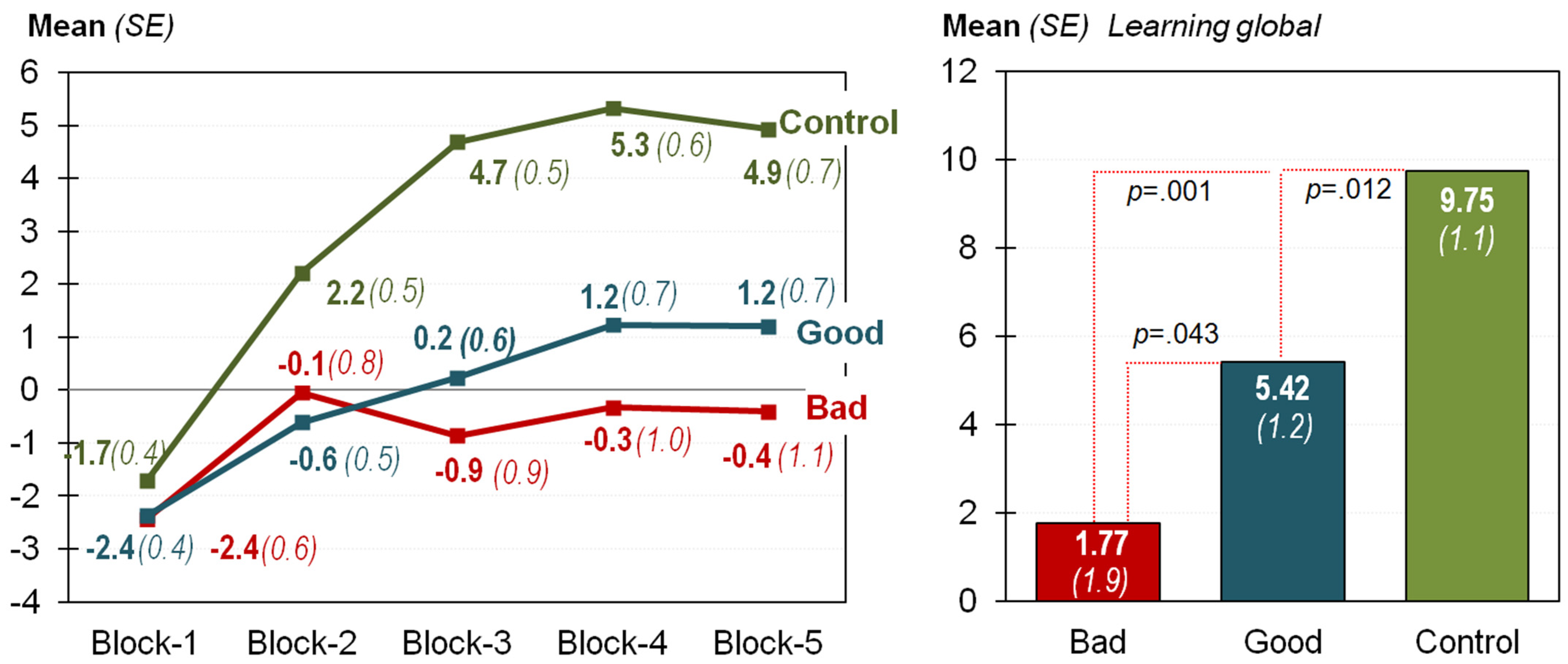
3.1. Comparison of the IGT Measures between the Groups
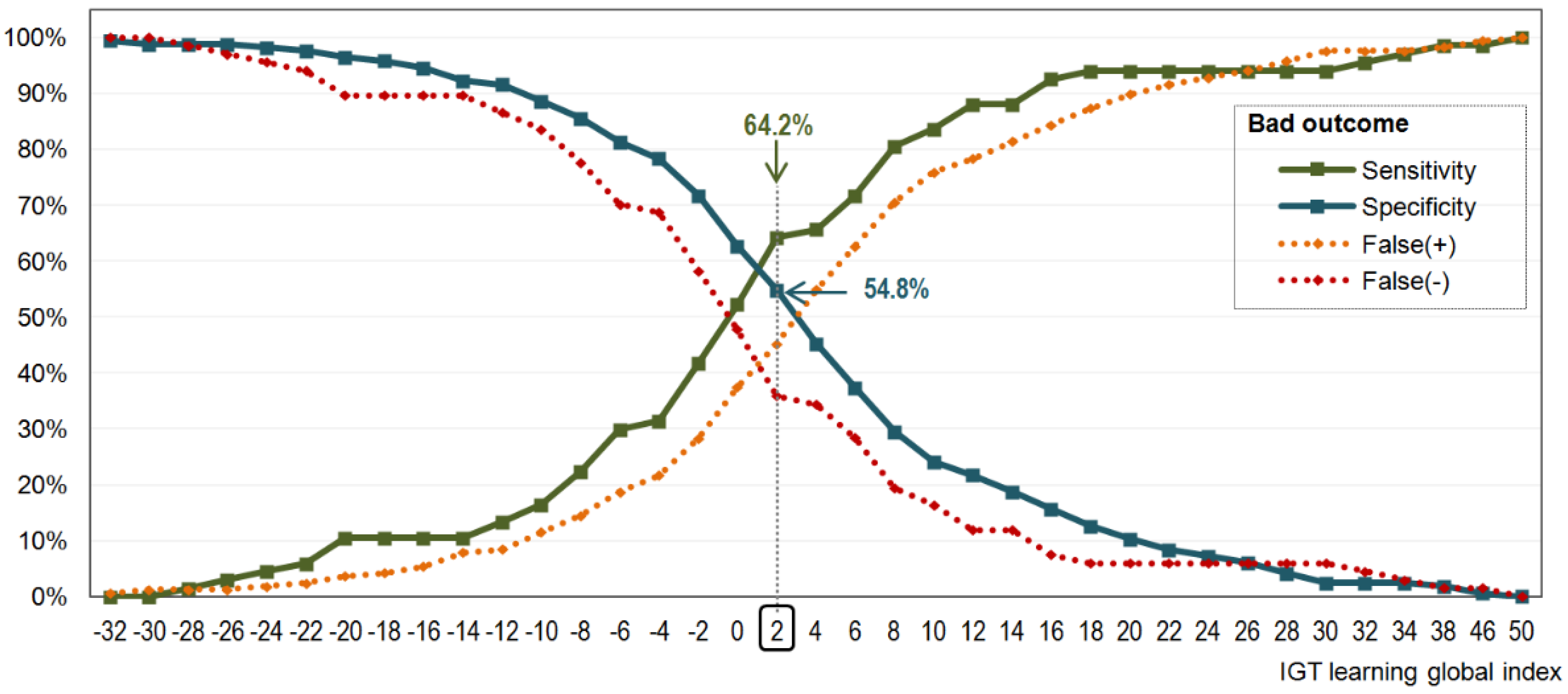
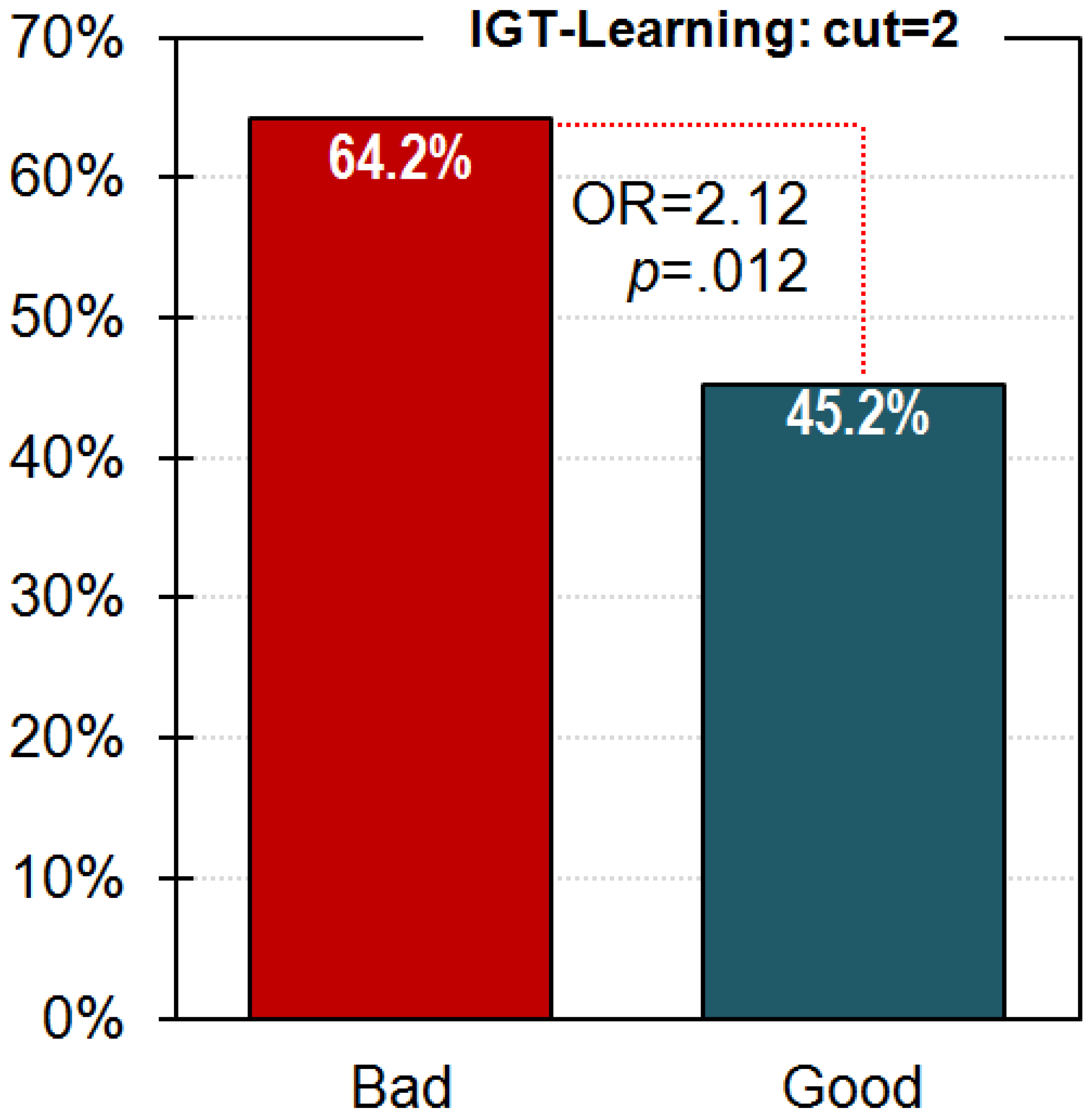
3.2. Discriminative Capacity of the IGT-Learning Score
3.3. Variables Associated with the CBT Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kerr-Gaffney, J.; Harrison, A.; Tchanturia, K. Social anxiety in the eating disorders: A systematic review and meta-analysis. Psychol. Med. 2018, 48, 2477–2491. [Google Scholar] [CrossRef]
- Chesney, E.; Goodwin, G.M.; Fazel, S. Risks of all-cause and suicide mortality in mental disorders: A meta-review. World Psychiatry 2014, 13, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Foulon, C.; Guelfi, J.D.; Kipman, A.; Adès, J.; Romo, L.; Houdeyer, K.; Marquez, S.; Mouren, M.C.; Rouillon, F.; Gorwood, P. Switching to the bingeing/purging subtype of anorexia nervosa is frequently associated with suicidal attempts. Eur. Psychiatry 2007, 22, 513–519. [Google Scholar] [CrossRef]
- Preti, A.; Rocchi, M.B.L.; Sisti, D.; Camboni, M.V.; Miotto, P. A comprehensive meta-analysis of the risk of suicide in eating disorders. Acta Psychiatr. Scand. 2011, 124, 6–17. [Google Scholar] [CrossRef]
- Mandelli, L.; Arminio, A.; Atti, A.-R.; De Ronchi, D. Suicide attempts in eating disorder subtypes: A meta-analysis of the literature employing DSM-IV, DSM-5, or ICD-10 diagnostic criteria. Psychol. Med. 2019, 49, 1237–1249. [Google Scholar] [CrossRef]
- Galmiche, M.; Déchelotte, P.; Lambert, G.; Tavolacci, M.P. Prevalence of eating disorders over the 2000-2018 period: A systematic literature review. Am. J. Clin. Nutr. 2019, 109, 1402–1413. [Google Scholar] [CrossRef] [PubMed]
- Linardon, J.; Wade, T.D.; de la Piedad Garcia, X.; Brennan, L. The efficacy of cognitive-behavioral therapy for eating disorders: A systematic review and meta-analysis. J. Consult. Clin. Psychol. 2017, 85, 1080–1094. [Google Scholar] [CrossRef]
- Vaidya, V. Cognitive behavior therapy in patients with binge eating disorder. Eur. Psychiatry 2011, 26, 739. [Google Scholar] [CrossRef]
- Agüera, Z.; Sánchez, I.; Granero, R.; Riesco, N.; Steward, T.; Martín-Romera, V.; Jiménez-Murcia, S.; Romero, X.; Caroleo, M.; Segura-García, C.; et al. Short-Term Treatment Outcomes and Dropout Risk in Men and Women with Eating Disorders. Eur. Eat. Disord. Rev. 2017, 25, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Keel, P.K.; Brown, T.A. Update on course and outcome in eating disorders. Int. J. Eat. Disord. 2010, 43, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Radunz, M.; Keegan, E.; Osenk, I.; Wade, T.D. Relationship between eating disorder duration and treatment outcome: Systematic review and meta-analysis. Int. J. Eat. Disord. 2020, 53, 1761–1773. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, P.E. Treatment of anorexia nervosa: Is it lacking power? Psychol. Med. 2019, 49, 1055–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nazar, B.P.; Gregor, L.K.; Albano, G.; Marchica, A.; Coco, G.L.; Cardi, V.; Treasure, J. Early Response to treatment in Eating Disorders: A Systematic Review and a Diagnostic Test Accuracy Meta-Analysis. Eur. Eat. Disord. Rev. 2017, 25, 67–79. [Google Scholar] [CrossRef] [PubMed]
- Cavedini, P.; Zorzi, C.; Bassi, T.; Gorini, A.; Baraldi, C.; Ubbiali, A.; Bellodi, L. Decision-making functioning as a predictor of treatment outcome in anorexia nervosa. Psychiatry Res. 2006, 145, 179–187. [Google Scholar] [CrossRef]
- Graves, T.A.; Tabri, N.; Thompson-Brenner, H.; Franko, D.L.; Eddy, K.T.; Bourion-Bedes, S.; Brown, A.; Constantino, M.J.; Flückiger, C.; Forsberg, S.; et al. A meta-analysis of the relation between therapeutic alliance and treatment outcome in eating disorders. Int. J. Eat. Disord. 2017, 50, 323–340. [Google Scholar] [CrossRef]
- Juarascio, A.S.; Manasse, S.M.; Espel, H.M.; Kerrigan, S.G.; Forman, E.M. Could training executive function improve treatment outcomes for eating disorders? Appetite 2015, 90, 187–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Preyde, M.; Watson, J.; Remers, S.; Stuart, R. Emotional dysregulation, interoceptive deficits, and treatment outcomes in patients with eating disorders. Soc. Work Ment. Health 2016, 14, 227–244. [Google Scholar] [CrossRef]
- Stewart, C.S.; McEwen, F.S.; Konstantellou, A.; Eisler, I.; Simic, M. Impact of ASD Traits on Treatment Outcomes of Eating Disorders in Girls. Eur. Eat. Disord. Rev. 2017, 25, 123–128. [Google Scholar] [CrossRef]
- Testa, G.; Baenas, I.; Vintró-Alcaraz, C.; Granero, R.; Agüera, Z.; Sánchez, I.; Riesco, N.; Jiménez-Murcia, S.; Fernández-Aranda, F. Does ADHD Symptomatology Influence Treatment Outcome and Dropout Risk in Eating Disorders? A longitudinal Study. J. Clin. Med. 2020, 9, 2305. [Google Scholar] [CrossRef]
- Fernández-Aranda, F.; Casas, M.; Claes, L.; Bryan, D.C.; Favaro, A.; Granero, R.; Gudiol, C.; Jiménez-Murcia, S.; Karwautz, A.; Le Grange, D.; et al. COVID-19 and implications for eating disorders. Eur. Eat. Disord. Rev. 2020, 28, 239–245. [Google Scholar] [CrossRef]
- Kan, C.; Cardi, V.; Stahl, D.; Treasure, J. Precision psychiatry—What it means for eating disorders? Eur. Eat. Disord. Rev. 2019, 27, 3–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, S.B.; Quintana, D.S.; Loeb, K.L.; Griffiths, S.; Le Grange, D. Treatment outcomes for anorexia nervosa: A systematic review and meta-analysis of randomized controlled trials. Psychol. Med. 2019, 49, 535–544. [Google Scholar] [CrossRef]
- Boeka, A.G.; Lokken, K.L. The Iowa gambling task as a measure of decision making in women with bulimia nervosa. J. Int. Neuropsychol. Soc. 2006, 12, 741–745. [Google Scholar] [CrossRef] [PubMed]
- Fagundo, A.B.; de la Torre, R.; Jiménez-Murcia, S.; Agüera, Z.; Granero, R.; Tárrega, S.; Botella, C.; Baños, R.; Fernández-Real, J.M.; Rodríguez, R.; et al. Executive functions profile in extreme eating/weight conditions: From Anorexia Nervosa to Obesity. PLoS ONE 2012, 7, e43382. [Google Scholar] [CrossRef] [Green Version]
- Guillaume, S.; Sang, C.N.T.; Jaussent, I.; Raingeard, I.; Bringer, J.; Jollant, F.; Courtet, P. Is Decision Making Really Impaired in Eating Disorders? Neuropsychology 2010, 24, 808–812. [Google Scholar] [CrossRef] [Green Version]
- Liao, P.C.; Uher, R.; Lawrence, N.; Treasure, J.; Schmidt, U.; Campbell, I.C.; Collier, D.A.; Tchanturia, K. An examination of decision making in bulimia nervosa. J. Clin. Exp. Neuropsychol. 2009, 31, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Perpiñá, C.; Segura, M.; Sánchez-Reales, S. Cognitive flexibility and decision-making in eating disorders and obesity. Eat. Weight Disord. 2017, 22, 435–444. [Google Scholar] [CrossRef]
- Tchanturia, K.; Lounes, N.; Holttum, S. Cognitive remediation in anorexia nervosa and related conditions: A systematic review. Eur. Eat. Disord. Rev. 2014, 22, 454–462. [Google Scholar] [CrossRef]
- Diamond, A. Executive functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [Green Version]
- Gleichgerrcht, E.; Ibáñez, A.; Roca, M.; Torralva, T.; Manes, F. Decision-making cognition in neurodegenerative diseases. Nat. Rev. Neurol. 2010, 6, 611–623. [Google Scholar] [CrossRef]
- Del Missier, F.; Mäntylä, T.; de Bruin, W.B. Executive functions in decision making: An individual differences approach. Think. Reason. 2010, 16, 69–97. [Google Scholar] [CrossRef]
- Yuan, P.; Raz, N. Prefrontal cortex and executive functions in healthy adults: A meta-analysis of structural neuroimaging studies. Neurosci. Biobehav. Rev. 2014, 42, 180–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnstren, A.; Li, B. Neurobiology of executive functions: Catecholamine influences on prefrontal cortical functions. Biol. Psychiatry 2005, 57, 1377–1384. [Google Scholar] [CrossRef] [PubMed]
- Vinogradov, S.; Fisher, M.; De Villers-Sidani, E. Cognitive training for impaired neural systems in neuropsychiatric illness. Neuropsychopharmacology 2012, 37, 43–76. [Google Scholar] [CrossRef] [PubMed]
- Friederich, H.C.; Wu, M.; Simon, J.J.; Herzog, W. Neurocircuit function in eating disorders. Int. J. Eat. Disord. 2013, 46, 425–432. [Google Scholar] [CrossRef]
- Brogan, A.; Hevey, D.; Pignatti, R. Anorexia, bulimia, and obesity: Shared decision making deficits on the Iowa Gambling Task (IGT). J. Int. Neuropsychol. Soc. 2010, 16, 711–715. [Google Scholar] [CrossRef] [Green Version]
- Francesconi, M.; Flouri, E.; Harrison, A. Change in decision-making skills and risk for eating disorders in adolescence: A population-based study. Eur. Psychiatry 2020, 63, e93. [Google Scholar] [CrossRef] [PubMed]
- Garrido, I.; Subirá, S. Decision-making and impulsivity in eating disorder patients. Psychiatry Res. 2013, 207, 107–112. [Google Scholar] [CrossRef]
- Steward, T.; Mestre-Bach, G.; Vintró-Alcaraz, C.; Lozano-Madrid, M.; Agüera, Z.; Fernández-Formoso, J.A.; Granero, R.; Jiménez-Murcia, S.; Vilarrasa, N.; García-Ruiz-de-Gordejuela, A.; et al. Food addiction and impaired executive functions in women with obesity. Eur. Eat. Disord. Rev. 2018, 26, 574–584. [Google Scholar] [CrossRef]
- Steward, T.; Mestre-Bach, G.; Agüera, Z.; Granero, R.; Martín-Romera, V.; Sánchez, I.; Riesco, N.; Tolosa-Sola, I.; Fernández-Formoso, J.A.; Fernández-García, J.C.; et al. Enduring Changes in Decision Making in Patients with Full Remission from Anorexia Nervosa. Eur. Eat. Disord. Rev. 2016, 24, 523–527. [Google Scholar] [CrossRef]
- Danner, U.N.; Ouwehand, C.; Van Haastert, N.L.; Hornsveld, H.; De Ridder, D.T.D. Decision-making impairments in women with binge eating disorder in comparison with obese and normal weight women. Eur. Eat. Disord. Rev. 2012, 20, e56–e62. [Google Scholar] [CrossRef] [PubMed]
- Giannunzio, V.; Degortes, D.; Tenconi, E.; Collantoni, E.; Solmi, M.; Santonastaso, P.; Favaro, A. Decision-making impairment in anorexia nervosa: New insights into the role of age and decision-making style. Eur. Eat. Disord. Rev. 2018, 26, 302–314. [Google Scholar] [CrossRef] [PubMed]
- Galimberti, E.; Fadda, E.; Cavallini, M.C.; Martoni, R.M.; Erzegovesi, S.; Bellodi, L. Executive functioning in anorexia nervosa patients and their unaffected relatives. Psychiatry Res. 2013, 208, 238–244. [Google Scholar] [CrossRef] [PubMed]
- Oldershaw, A.; Lavender, T.; Schmidt, U. Are socio-emotional and neurocognitive functioning predictors of therapeutic outcomes for adults with anorexia nervosa? Eur. Eat. Disord. Rev. 2018, 26, 346–359. [Google Scholar] [CrossRef]
- Hemmingsen, S.D.; Wesselhoeft, R.; Lichtenstein, M.B.; Sjögren, J.M.; Støving, R.K. Cognitive improvement following weight gain in patients with anorexia nervosa: A systematic review. Eur. Eat. Disord. Rev. 2020, 29, 402–426. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Philadelphia, PA, USA, 2013; ISBN 0-89042-555-8. [Google Scholar]
- Bechara, A.; Damasio, A.R.; Damasio, H.; Anderson, S.W. Insensitivity to future consequences following damage to human prefrontal cortex. Cognition 1994, 50, 7–15. [Google Scholar] [CrossRef]
- Derogatis, L.R.; Savitz, K.L. The SCL-90-R, Brief Symptom Inventory, and Matching Clinical Rating Scales. In The Use of Psychological Testing for Treatment Planning and Outcomes Assessment, 2nd ed.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 1999; pp. 679–724. ISBN 0-8058-2761-7. (Hardcover). [Google Scholar]
- Garner, D. Manual del EDI-2 Inventario de Trastorno de la Conducta Alimentaria; TEA: Madrid, Spain, 1998. [Google Scholar]
- Eisinger, A.; Magi, A.; Gyurkovics, M.; Szabo, E.; Demetrovics, Z.; Kokonyei, G. Iowa Gambling Task: Illustration of a behavioral measurement. Neuropsychopharmacol. Hung. 2016, 18, 45–55. [Google Scholar]
- Brand, M.; Labudda, K.; Markowitsch, H.J. Neuropsychological correlates of decision-making in ambiguous and risky situations. Neural Netw. 2006, 19, 1266–1276. [Google Scholar] [CrossRef]
- Riesco, N.; Agüera, Z.; Granero, R.; Jiménez-Murcia, S.; Menchón, J.M.; Fernández-Aranda, F. Other Specified Feeding or Eating Disorders (OSFED): Clinical heterogeneity and cognitive-behavioral therapy outcome. Eur. Psychiatry 2018, 54, 109–116. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Aranda, F.; Treasure, J.; Paslakis, G.; Agüera, Z.; Giménez, M.; Granero, R.; Sánchez, I.; Serrano-Troncoso, E.; Gorwood, P.; Herpertz-Dahlmann, B.; et al. The Impact of Duration of Illness on Treatment Non-response and Drop-out: Exploring the Relevance of Enduring Eating Disorder (E-ED) Concept. Eur. Eat. Disord. Rev. 2021, 29, 499–513. [Google Scholar] [CrossRef]
- Finner, H.; Roters, M. On the false discovery rate and expected type I errors. Biom. J. 2001, 43, 985–1005. [Google Scholar] [CrossRef]
- Zhou, X.-H.; Obuchowski, N.A.; McClish, D.K. Statistical Methods in Diagnostic Medicine; Wiley Series in Probability and Statistics; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2011; ISBN 9780470906514. [Google Scholar]
- Levine, T.R.; Hullett, C.R. Eta Squared, Partial Eta Squared, and Misreporting of Effect Size in Communication Research. Hum. Commun. Res. 2002, 28, 612–625. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: New York, NY, USA, 1988; ISBN 9780203771587. [Google Scholar]
- Hiroto, D.S.; Seligman, M.E. Generality of learned helplessness in man. J. Pers. Soc. Psychol. 1975, 31, 311–327. [Google Scholar] [CrossRef]
- Harrison, A.; Treasure, J.; Smillie, L.D. Approach and avoidance motivation in eating disorders. Psychiatry Res. 2011, 188, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Harrison, A.; O’Brien, N.; Lopez, C.; Treasure, J. Sensitivity to reward and punishment in eating disorders. Psychiatry Res. 2010, 177, 1–11. [Google Scholar] [CrossRef]
- Miller, W.R.; Seligman, M.E. Depression and learned helplessness in man. J. Abnorm. Psychol. 1975, 84, 228–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dingemans, A.E.; van Son, G.E.; Vanhaelen, C.B.; van Furth, E.F. Depressive symptoms rather than executive functioning predict group cognitive behavioural therapy outcome in binge eating disorder. Eur. Eat. Disorders Rev. 2020, 28, 620–632. [Google Scholar] [CrossRef] [PubMed]
- Fortgang, R.G.; Srihari, V.; Cannon, T.D. Cognitive effort and amotivation in first-episode psychosis. J. Abnorm. Psychol. 2020, 129, 422–431. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| IGT Raw Scores | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Block 1 | Block 2 | Block 3 | Block 4 | Block 5 | ||||||||
| Group (outcome) | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||
| Bad (n = 67) | −2.45 | 3.85 | −0.05 | 4.28 | −0.87 | 5.82 | −0.32 | 7.78 | −0.41 | 7.64 | ||
| Good (n = 166) | −2.38 | 4.66 | −0.61 | 5.53 | 0.24 | 5.87 | 1.23 | 7.42 | 1.21 | 8.45 | ||
| Control (n = 191) | −1.72 | 5.92 | 2.22 | 7.06 | 4.68 | 8.35 | 5.32 | 9.03 | 4.93 | 9.90 | ||
| Multivariate tests | F | df | p | η2 | ||||||||
| Int. BxG | 4.09 | 8; 419 | 0.001 * | 0.019 | ||||||||
| Block | 0.80 | 4; 419 | 0.401 | 0.002 | ||||||||
| Group | 22.34 | 2; 419 | 0.001 * | 0.096 | ||||||||
| Factor Block Within Group | F | p | η2 | |||||||||
| Bad | 1.63 | 0.166 | 0.015 | |||||||||
| Good | 6.51 | 0.001 * | 0.059 | |||||||||
| Control | 30.89 | 0.001 * | 0.229 | |||||||||
| Polynomial contrast for Block | Linear (order 1) | Quadratic (order 2) | Cubic (order 3) | Quartic (order 4) | ||||||||
| F | p | η2 | F | p | η2 | F | p | η2 | F | p | η2 | |
| Group: bad | 1.14 | 0.289 | 0.017 | 3.94 | 0.051 | 0.056 | 1.20 | 0.277 | 0.018 | 1.73 | 0.193 | 0.026 |
| Group: good | 23.32 | 0.001 * | 0.124 | 6.49 | 0.012 * | 0.038 | 0.15 | 0.701 | 0.001 | 1.02 | 0.314 | 0.006 |
| Group: control | 79.71 | 0.001 * | 0.296 | 27.99 | 0.001 * | 0.128 | 0.55 | 0.457 | 0.003 | 0.53 | 0.468 | 0.003 |
| Bad Outcome | Good Outcome | Control | ||||
|---|---|---|---|---|---|---|
| Descriptives | Mean | SD | Mean | SD | Mean | SD |
| 1.77 | 14.04 | 5.42 | 13.15 | 9.75 | 16.67 | |
| Factor group | F | df | p | η2 | ||
| 7.14 | 2; 423 | 0.001 * | 0.033 | |||
| Pairwise comparisons | F | p | η2 | |||
| Bad vs. good | 4.84 | 0.043 * | 0.014 | |||
| Bad vs. control | 12.93 | 0.001 * | 0.030 | |||
| Good vs. control | 6.44 | 0.012 * | 0.015 | |||
| Bad Outcome (n = 67) | Good Outcome (n = 166) | ||||||
|---|---|---|---|---|---|---|---|
| Sex | n | % | n | % | p | V | |
| Women | 59 | 88.1% | 131 | 78.9% | 0.103 | 0.202 | |
| Men | 8 | 11.9% | 35 | 21.1% | |||
| Mean | SD | Mean | SD | p | η2 | ||
| Chronological age (years-old) | 28.99 | 9.50 | 31.13 | 11.39 | 0.174 | 0.008 | |
| Duration of disorder (years) | 9.57 | 8.36 | 7.79 | 8.65 | 0.152 | 0.009 | |
| EDI-2: Drive for thinness | 11.78 | 7.14 | 11.71 | 6.45 | 0.946 | 0.001 | |
| EDI-2: Body dissatisfaction | 15.22 | 8.17 | 14.74 | 8.84 | 0.700 | 0.001 | |
| EDI-2: Interoceptive awareness | 10.39 | 6.59 | 9.73 | 6.89 | 0.504 | 0.002 | |
| EDI-2: Bulimia | 6.28 | 5.85 | 5.41 | 5.34 | 0.273 | 0.005 | |
| EDI-2: Interpersonal distrust | 5.39 | 4.61 | 5.74 | 5.23 | 0.630 | 0.001 | |
| EDI-2: Ineffectiveness | 10.84 | 7.08 | 9.40 | 7.24 | 0.169 | 0.008 | |
| EDI-2: Maturity fears | 8.37 | 6.09 | 7.48 | 5.19 | 0.257 | 0.006 | |
| EDI-2: Perfectionism | 6.07 | 4.89 | 5.05 | 4.08 | 0.103 | 0.011 | |
| EDI-2: Impulse regulation | 5.43 | 5.30 | 5.36 | 5.81 | 0.925 | 0.001 | |
| EDI-2: Ascetic | 6.70 | 4.24 | 6.05 | 4.25 | 0.289 | 0.005 | |
| EDI-2: Social insecurity | 7.00 | 4.66 | 6.90 | 5.57 | 0.901 | 0.001 | |
| EDI-2: Total score | 93.48 | 46.79 | 87.56 | 45.95 | 0.377 | 0.003 | |
| SCL-90R: Somatization | 1.78 | 1.02 | 1.60 | 0.90 | 0.198 | 0.007 | |
| SCL-90R: Obsessive/compulsive | 1.78 | 0.97 | 1.73 | 0.92 | 0.734 | 0.001 | |
| SCL-90R: Interpersonal sensitivity | 1.90 | 0.99 | 1.88 | 1.00 | 0.848 | 0.001 | |
| SCL-90R: Depressive | 2.25 | 0.98 | 2.06 | 0.99 | 0.196 | 0.007 | |
| SCL-90R: Anxiety | 1.63 | 0.91 | 1.46 | 0.91 | 0.194 | 0.007 | |
| SCL-90R: Hostility | 1.17 | 0.88 | 1.19 | 0.90 | 0.898 | 0.001 | |
| SCL-90R: Phobic anxiety | 0.84 | 0.86 | 0.88 | 0.91 | 0.736 | 0.001 | |
| SCL-90R: Paranoid Ideation | 1.43 | 0.89 | 1.28 | 0.84 | 0.253 | 0.006 | |
| SCL-90R: Psychotic | 1.36 | 0.82 | 1.17 | 0.72 | 0.081 | 0.013 | |
| SCL-90R: GSI score | 1.69 | 0.78 | 1.58 | 0.78 | 0.300 | 0.005 | |
| SCL-90R: PST score | 61.43 | 19.63 | 60.36 | 18.86 | 0.697 | 0.001 | |
| SCL-90R: PSDI score | 2.35 | 0.59 | 2.22 | 0.61 | 0.127 | 0.010 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lucas, I.; Miranda-Olivos, R.; Testa, G.; Granero, R.; Sánchez, I.; Sánchez-González, J.; Jiménez-Murcia, S.; Fernández-Aranda, F. Neuropsychological Learning Deficits as Predictors of Treatment Outcome in Patients with Eating Disorders. Nutrients 2021, 13, 2145. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072145
Lucas I, Miranda-Olivos R, Testa G, Granero R, Sánchez I, Sánchez-González J, Jiménez-Murcia S, Fernández-Aranda F. Neuropsychological Learning Deficits as Predictors of Treatment Outcome in Patients with Eating Disorders. Nutrients. 2021; 13(7):2145. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072145
Chicago/Turabian StyleLucas, Ignacio, Romina Miranda-Olivos, Giulia Testa, Roser Granero, Isabel Sánchez, Jessica Sánchez-González, Susana Jiménez-Murcia, and Fernando Fernández-Aranda. 2021. "Neuropsychological Learning Deficits as Predictors of Treatment Outcome in Patients with Eating Disorders" Nutrients 13, no. 7: 2145. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072145