
Effects of 6 Months of Soy-Enriched High Protein Compared to Eucaloric Low Protein Snack Replacement on Appetite, Dietary Intake, and Body Composition in Normal-Weight Obese Women: A Randomized Controlled Trial




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Protocol
2.3. Randomization and Blinding
2.4. Dietary Intake and Physical Activity Assessment
2.5. Body Composition Assessment
2.6. Appetite Assessment
2.7. Statistical Analyses
3. Results
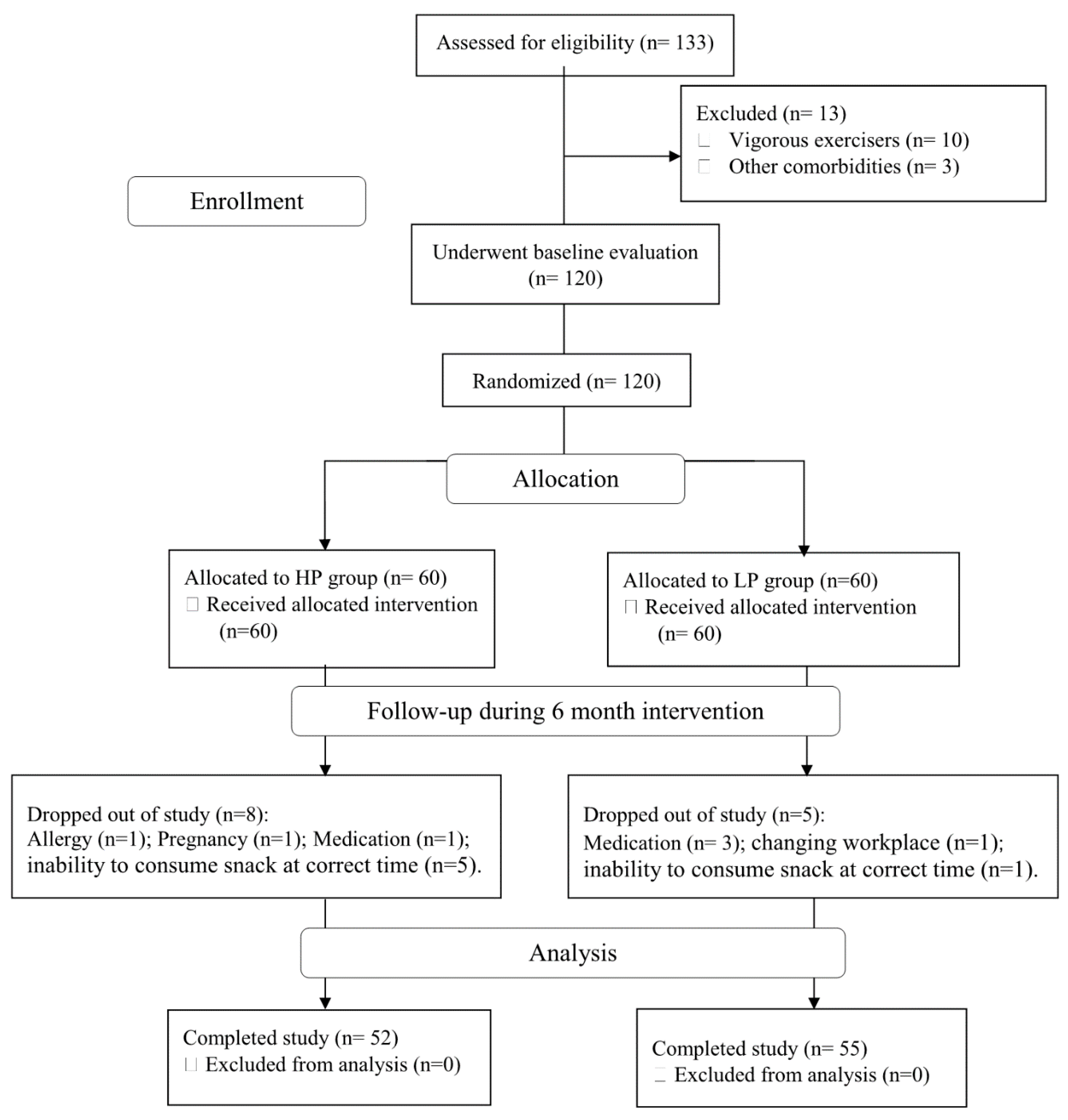
3.1. Study Population and Compliance
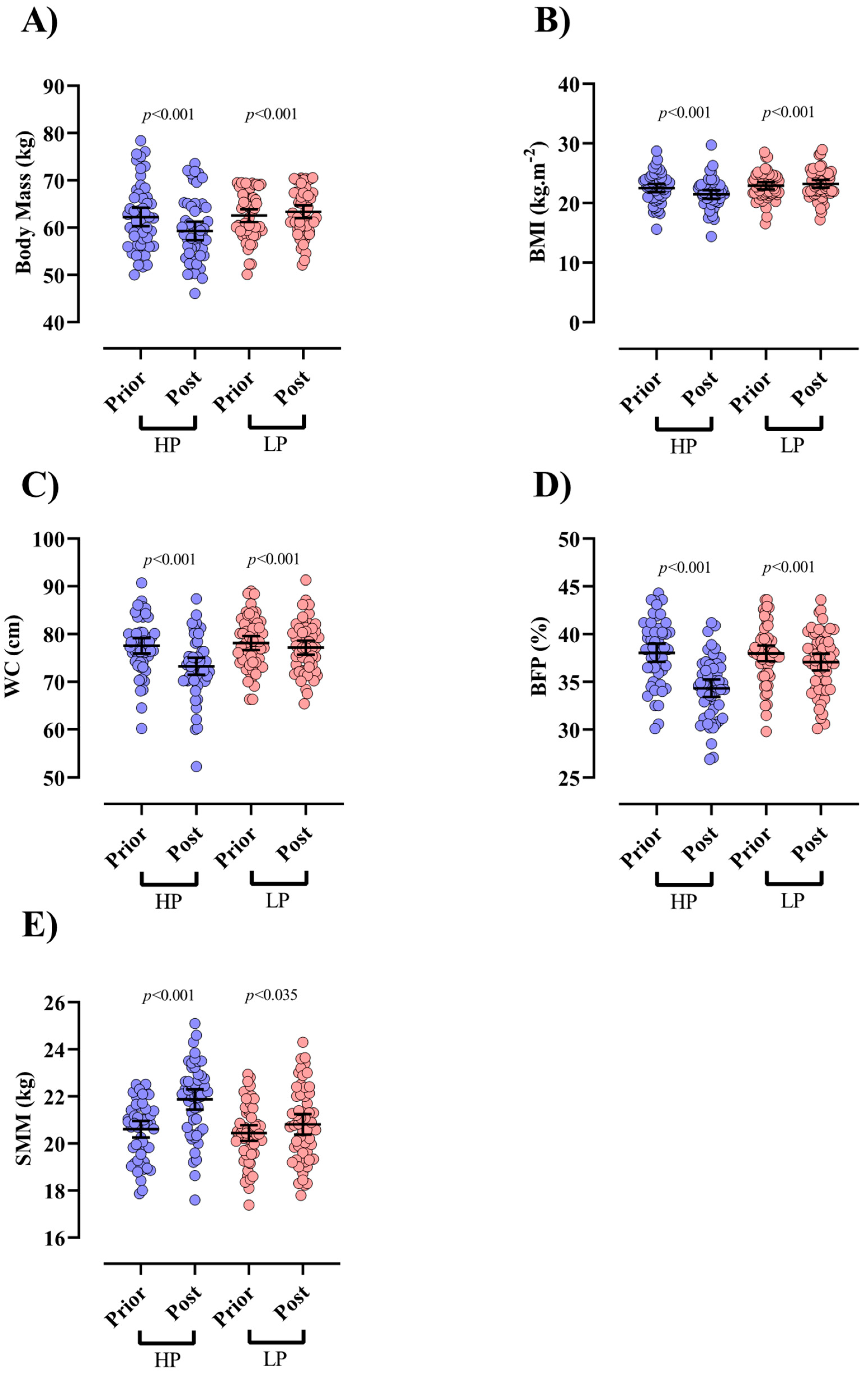
3.2. Body Composition
3.3. Appetite and Physical Activity
3.4. Dietary Intake
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hosseini, S.A.; Aghamohammadi, V.; Ashtary-Larky, D.; Alipour, M.; Ghanavati, M.; Lamuchi-Deli, N. Are young Iranian women with metabolically healthy obesity at increased risk of CVD incidence? J. Vasc. Bras. 2020, 19. [Google Scholar] [CrossRef]
- Olafsdottir, A.S.; Torfadottir, J.E.; Arngrimsson, S.A. Health Behavior and Metabolic Risk Factors Associated with Normal Weight Obesity in Adolescents. PLoS ONE 2016, 11, e0161451. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, N.; Furler, J.; Paul, T.V.; Thomas, N.; Oldenburg, B. Normal Weight Obesity: An Underrecognized Problem in Individuals of South Asian Descent. Clin. Ther. 2019, 41, 1638–1642. [Google Scholar] [CrossRef]
- Tayefi, M.; Tayefi, B.; Darroudi, S.; Mohammadi-Bajgiran, M.; Mouhebati, M.; Heidari-Bakavoli, A.; Ebrahimi, M.; Ferns, G.A.; Esmaily, H.; Dabaghian, M.; et al. There is an association between body fat percentage and metabolic abnormality in normal weight subjects: Iranian large population. Transl. Metab. Syndr. Res. 2019, 2, 11–16. [Google Scholar] [CrossRef]
- Marques-Vidal, P.; Pécoud, A.; Hayoz, D.; Paccaud, F.; Mooser, V.; Waeber, G.; Vollenweider, P. Prevalence of normal weight obesity in Switzerland: Effect of various definitions. Eur. J. Nutr. 2008, 47, 251–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellisle, F. Meals and snacking, diet quality and energy balance. Physiol. Behav. 2014, 134, 38–43. [Google Scholar] [CrossRef]
- Giesen, J.C.A.H.; Havermans, R.; Douven, A.; Tekelenburg, M.; Jansen, A. Will Work for Snack Food: The Association of BMI and Snack Reinforcement. Obesity 2010, 18, 966–970. [Google Scholar] [CrossRef]
- Keast, D.R.; Nicklas, T.A.; O’Neil, C.E. Snacking is associated with reduced risk of overweight and reduced abdominal obesity in adolescents: National Health and Nutrition Examination Survey (NHANES) 1999–2004. Am. J. Clin. Nutr. 2010, 92, 428–435. [Google Scholar] [CrossRef] [Green Version]
- Forslund, H.B.; Torgerson, J.; Sjöström, L.; Lindroos, A. Snacking frequency in relation to energy intake and food choices in obese men and women compared to a reference population. Int. J. Obesity 2005, 29, 711–719. [Google Scholar] [CrossRef] [Green Version]
- Franco, L.P.; Morais, C.C.; Cominetti, C. Normal-weight obesity syndrome: Diagnosis, prevalence, and clinical implications. Nutr. Rev. 2016, 74, 558–570. [Google Scholar] [CrossRef]
- Veldhorst, M.; Smeets, A.; Soenen, S.; Hochstenbach-Waelen, A.; Hursel, R.; Diepvens, K.; Lejeune, M.; Luscombe-Marsh, N.; Westerterp-Plantenga, M. Protein-induced satiety: Effects and mechanisms of different proteins. Physiol. Behav. 2008, 94, 300–307. [Google Scholar] [CrossRef]
- Pasiakos, S.M.; Cao, J.J.; Margolis, L.M.; Sauter, E.R.; Whigham, L.D.; McClung, J.P.; Rood, J.C.; Carbone, J.W.; Combs, G.F.; Young, A.J. Effects of high-protein diets on fat-free mass and muscle protein synthesis following weight loss: A randomized controlled trial. FASEB J. 2013, 27, 3837–3847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Astbury, N.M.; Taylor, M.A.; French, S.J.; Macdonald, I.A. Snacks containing whey protein and polydextrose induce a sustained reduction in daily energy intake over 2 wk under free-living conditions. Am. J. Clin. Nutr. 2014, 99, 1131–1140. [Google Scholar] [CrossRef] [Green Version]
- Bagheri, R.; Moghadam, B.H.; Ashtary-Larky, D.; Forbes, S.C.; Candow, D.G.; Galpin, A.J.; Eskandari, M.; Kreider, R.B.; Wong, A. Whole Egg Vs. Egg White Ingestion During 12 weeks of Resistance Training in Trained Young Males: A Randomized Controlled Trial. J. Strength Cond. Res. 2021, 35, 411–419. [Google Scholar] [CrossRef]
- Bagheri, R.; Moghadam, B.H.; Jo, E.; Tinsley, G.M.; Stratton, M.T.; Ashtary-Larky, D.; Eskandari, M.; Wong, A. Comparison of whole egg v. egg white ingestion during 12 weeks of resistance training on skeletal muscle regulatory markers in resistance-trained men. Br. J. Nutr. 2020, 124, 1–9. [Google Scholar] [CrossRef]
- Morales, F.E.; Tinsley, G.M.; Gordon, P.M. Acute and Long-Term Impact of High-Protein Diets on Endocrine and Metabolic Function, Body Composition, and Exercise-Induced Adaptations. J. Am. Coll. Nutr. 2017, 36, 295–305. [Google Scholar] [CrossRef]
- Piatti, P.; Monti, L.; Magni, F.; Fermo, I.; Baruffaldi, L.; Nasser, R.; Santambrogio, G.; Librenti, M.; Galli-Kienle, M.; Pontiroli, A.; et al. Hypocaloric high-protein diet improves glucose oxidation and spares lean body mass: Comparison to hypocaloric high-carbohydrate diet. Metabolism 1994, 43, 1481–1487. [Google Scholar] [CrossRef]
- Lonnie, M.; Hooker, E.; Brunstrom, J.M.; Corfe, B.M.; Green, M.A.; Watson, A.W.; Williams, E.A.; Stevenson, E.J.; Penson, S.; Johnstone, A.M. Protein for Life: Review of Optimal Protein Intake, Sustainable Dietary Sources and the Effect on Appetite in Ageing Adults. Nutrients 2018, 10, 360. [Google Scholar] [CrossRef] [Green Version]
- Ortinau, L.C.; Culp, J.M.; Hoertel, H.A.; Douglas, S.M.; Leidy, H.J. The effects of increased dietary protein yogurt snack in the afternoon on appetite control and eating initiation in healthy women. Nutr. J. 2013, 12, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poppitt, S.D.; Proctor, J.; McGill, A.-T.; Wiessing, K.R.; Falk, S.; Xin, L.; Budgett, S.C.; Darragh, A.; Hall, R.S. Low-dose whey protein-enriched water beverages alter satiety in a study of overweight women. Appetite 2011, 56, 456–464. [Google Scholar] [CrossRef]
- Rizzo, G.; Baroni, L. Soy, Soy Foods and Their Role in Vegetarian Diets. Nutrients 2018, 10, 43. [Google Scholar] [CrossRef] [Green Version]
- Romero-Corral, A.; Somers, V.K.; Sierra-Johnson, J.; Korenfeld, Y.; Boarin, S.; Korinek, J.; Jensen, M.D.; Parati, G.; Lopez-Jimenez, F. Normal weight obesity: A risk factor for cardiometabolic dysregulation and cardiovascular mortality. Eur. Heart J. 2009, 31, 737–746. [Google Scholar] [CrossRef]
- Shirali, S.; Daneghian, S.; Hosseini, S.A.; Ashtary-Larky, D.; Daneghian, M.; Mirlohi, M.-S. Effect of Caffeine Co-Ingested with Carnitine on Weight, Body-Fat Percent, Serum Leptin and Lipid Profile Changes in Male Teen Soccer Players: A Randomized Clinical Trial. Int. J. Pediatr. 2016, 4, 3685–3698. [Google Scholar]
- Bodner-Montville, J.; Ahuja, J.K.; Ingwersen, L.A.; Haggerty, E.S.; Enns, C.W.; Perloff, B.P. USDA Food and Nutrient Database for Dietary Studies: Released on the web. J. Food Compos. Anal. 2006, 19, S100–S107. [Google Scholar] [CrossRef]
- Wheeler, M.L.; Daly, A.; Evert, A.; Franz, M.J.; Geil, P.; Holzmeister, L.A.; Kulkarni, K.; Loghmani, E.; Ross, T.A.; Woolf, P. Choose Your Foods: Exchange Lists for Diabetes, Sixth Edition, 2008: Description and Guidelines for Use. J. Am. Diet. Assoc. 2008, 108, 883–888. [Google Scholar] [CrossRef]
- Mohammadifard, N.; Omidvar, N.; Houshyarrad, A.; Neyestani, T.R.; Naderi, G.-A.; Soleymani, B. Validity and reproducibility of a food frequency questionnaire for assessment of fruit and vegetable intake in Iranian adults*. J. Res. Med Sci. 2011, 16, 1286–1297. [Google Scholar]
- Bagheri, R.; Rashidlamir, A.; Ashtary-Larky, D.; Wong, A.; Grubbs, B.; Motevalli, M.S.; Baker, J.S.; Laher, I.; Zouhal, H. Effects of green tea extract supplementation and endurance training on irisin, pro-inflammatory cytokines, and adiponectin concentrations in overweight middle-aged men. Eur. J. Appl. Physiol. 2020, 120, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Thompson, E.F.; Byers, T. Dietary assessment resource manual. J. Nutr. 1994, 124, 2245s–2317s. [Google Scholar]
- Beer-Borst, S.; Amado, R. Validation of a self-administered 24-hour recall questionnaire used in a large-scale dietary survey. Z. Ernährungswissenschaft 1995, 34, 183–189. [Google Scholar] [CrossRef]
- Greger, J.; Etnyre, G.M. Validity of 24-hour dietary recalls by adolescent females. Am. J. Public Health 1978, 68, 70–72. [Google Scholar] [CrossRef]
- Karvetti, R.; Knuts, L.R. Validity of the 24-hour dietary recall. J. Am. Diet. Assoc. 1985, 85, 1437–1442. [Google Scholar]
- Maddison, R.; Mhurchu, C.N.; Jiang, Y.; Vander Hoorn, S.; Rodgers, A.; Lawes, C.M.; Rush, E. International physical activity questionnaire (IPAQ) and New Zealand physical activity questionnaire (NZPAQ): A doubly labelled water validation. Int. J. Behav. Nutr. Phys. Activity 2007, 4, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Bagheri, R.; Ashtary-Larky, D.; Elliott, B.T.; Willoughby, D.S.; Kargarfard, M.; Alipour, M.; Lamuchi-Deli, N.; Kooti, W.; Asbaghi, O.; Wong, A. The effects of gradual vs. rapid weight loss on serum concentrations of myokines and body composition in overweight and obese females. Arch. Physiol. Biochem. 2021, 2021, 1–8. [Google Scholar] [CrossRef]
- American College of Sports Medicine. ACSM’s Resource Manual for Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012. [Google Scholar]
- Schoenfeld, B.J.; Nickerson, B.S.; Wilborn, C.D.; Urbina, S.L.; Hayward, S.B.; Krieger, J.; Aragon, A.A.; Tinsley, G. Comparison of Multifrequency Bioelectrical Impedance vs. Dual-Energy X-ray Absorptiometry for Assessing Body Composition Changes After Participation in a 10-Week Resistance Training Program. J. Strength Cond. Res. 2020, 34, 678–688. [Google Scholar] [CrossRef]
- Ling, C.H.; de Craen, A.J.; Slagboom, P.E.; Gunn, D.A.; Stokkel, M.P.; Westendorp, R.G.; Maier, A.B. Accuracy of direct segmental multi-frequency bioimpedance analysis in the assessment of total body and segmental body composition in middle-aged adult population. Clin. Nutr. 2011, 30, 610–615. [Google Scholar] [CrossRef] [Green Version]
- Jackson, A.S.; Pollock, M.L.; Graves, J.E.; Mahar, M.T. Reliability and validity of bioelectrical impedance in determining body composition. J. Appl. Physiol. 1988, 64, 529–534. [Google Scholar] [CrossRef]
- Ashtary-Larky, D.; Ghanavati, M.; Lamuchi-Deli, N.; Payami, S.A.; Alavi-Rad, S.; Boustaninejad, M.; Afrisham, R.; Abbasnezhad, A.; Alipour, M. Rapid Weight Loss vs. Slow Weight Loss: Which is More Effective on Body Composition and Metabolic Risk Factors? Int. J. Endocrinol. Metab. 2017, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rondanelli, M.; Klersy, C.; Iadarola, P.; Monteferrario, F.; Opizzi, A. Satiety and amino-acid profile in overweight women after a new treatment using a natural plant extract sublingual spray formulation. Int. J. Obes. 2009, 33, 1174–1182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tahavorgar, A.; Vafa, M.; Shidfar, F.; Gohari, M.; Heydari, I. Whey protein preloads are more beneficial than soy protein preloads in regulating appetite, calorie intake, anthropometry, and body composition of overweight and obese men. Nutr. Res. 2014, 34, 856–861. [Google Scholar] [CrossRef] [PubMed]
- Flint, A.; Raben, A.; Blundell, J.; Astrup, A. Reproducibility, power and validity of visual analogue scales in assessment of appetite sensations in single test meal studies. Int. J. Obes. 2000, 24, 38–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Haghighat, N.; Ashtary-Larky, D.; Bagheri, R.; Mahmoodi, M.; Rajaei, M.; Alipour, M.; Kooti, W.; Aghamohammdi, V.; Wong, A. The effect of 12 weeks of equicaloric high protein diet in regulating appetite and body composition of women with Normal Weight Obesity: A randomized controlled trial. Br. J. Nutr. 2020, 124, 1044–1051. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.I.; Atherton, P.; Reeds, D.N.; Mohammed, B.S.; Jaffery, H.; Rankin, D.; Rennie, M.J.; Mittendorfer, B. No major sex differences in muscle protein synthesis rates in the postabsorptive state and during hyperinsulinemia-hyperaminoacidemia in middle-aged adults. J. Appl. Physiol. 2009, 107, 1308–1315. [Google Scholar] [CrossRef] [PubMed]
- Cheraghpour, M.; Hosseini, S.A.; Ashtary-Larky, D.; Shirali, S.; Ghanavati, M.; Alipour, M. Effects of High-Protein, Low-Energy Diet on Body Composition in Overweight and Obese Adults: A Clinical Trial. Int. J. Nutr. Food Eng. 2017, 11, 77–80. [Google Scholar]
- Weigle, D.S.; Breen, P.A.; Matthys, C.C.; Callahan, H.S.; Meeuws, K.E.; Burden, V.R.; Purnell, J.Q. A high-protein diet induces sustained reductions in appetite, ad libitum caloric intake, and body weight despite compensatory changes in diurnal plasma leptin and ghrelin concentrations. Am. J. Clin. Nutr. 2005, 82, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Heymsfield, S.B.; Gonzalez, M.C.C.; Shen, W.; Redman, L.; Thomas, D. Weight loss composition is one-fourth fat-free mass: A critical review and critique of this widely cited rule. Obes. Rev. 2014, 15, 310–321. [Google Scholar] [CrossRef] [PubMed]
- Krieger, J.W.; Sitren, H.S.; Daniels, M.J.; Langkamp-Henken, B. Effects of variation in protein and carbohydrate intake on body mass and composition during energy restriction: A meta-regression. Am. J. Clin. Nutr. 2006, 83, 260–274. [Google Scholar] [CrossRef]
- Wycherley, T.P.; Moran, L.J.; Clifton, P.; Noakes, M.; Brinkworth, G. Effects of energy-restricted high-protein, low-fat compared with standard-protein, low-fat diets: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2012, 96, 1281–1298. [Google Scholar] [CrossRef] [Green Version]
- Treyzon, L.; Chen, S.; Hong, K.; Yan, E.; Carpenter, C.L.; Thames, G.; Bowerman, S.; Wang, H.-J.; Elashoff, R.; Li, Z. A controlled trial of protein enrichment of meal replacements for weight reduction with retention of lean body mass. Nutr. J. 2008, 7, 23. [Google Scholar] [CrossRef] [Green Version]
- Gwin, J.A.; Church, D.D.; Wolfe, R.R.; Ferrando, A.A.; Pasiakos, S.M. Muscle protein synthesis and whole-body protein turnover responses to ingesting essential amino acids, intact protein, and protein-containing mixed meals with considerations for energy deficit. Nutrients 2020, 12, 2457. [Google Scholar] [CrossRef]
- Ciuris, C.; Lynch, H.M.; Wharton, C.; Johnston, C.S. A Comparison of Dietary Protein Digestibility, Based on DIAAS Scoring, in Vegetarian and Non-Vegetarian Athletes. Nutrients 2019, 11, 3016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ertl, P.; Knaus, W.; Zollitsch, W. An approach to including protein quality when assessing the net contribution of livestock to human food supply. Animals 2016, 10, 1883–1889. [Google Scholar] [CrossRef] [Green Version]
- Khairuddin, K.; Umar, U.; Gustiawan, W. The Effect of Supplement Soybean Milk and Whey Protein in Load Exercisestoward the Increasing Hypertrophy of Thigh Muscles. In Proceedings of the 1st Yogyakarya International Seminar on Health, Physical Education, and Sports Science: Evidence-based Practice of Sports Scinece in Education Performance, and Health, Yogyakarta, India, 14 October 2017. [Google Scholar]
- Burd, N.A.; McKenna, C.F.; Salvador, A.F.; Paulussen, K.J.; Moore, D. Dietary Protein Quantity, Quality, and Exercise Are Key to Healthy Living: A Muscle-Centric Perspective Across the Lifespan. Front. Nutr. 2019, 6, 83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jäger, R.; Kerksick, C.M.; Campbell, B.I.; Cribb, P.J.; Wells, S.D.; Skwiat, T.M.; Purpura, M.; Ziegenfuss, T.N.; Ferrando, A.A.; Arent, S.M.; et al. International Society of Sports Nutrition Position Stand: Protein and exercise. J. Int. Soc. Sports Nutr. 2017, 14, 20. [Google Scholar] [CrossRef] [Green Version]
- Chapelot, D.; Payen, F. Comparison of the effects of a liquid yogurt and chocolate bars on satiety: A multidimensional approach. Br. J. Nutr. 2009, 103, 760–767. [Google Scholar] [CrossRef] [Green Version]
- Azadbakht, L.; Izadi, V.; Surkan, P.J.; Esmaillzadeh, A. Effect of a High Protein Weight Loss Diet on Weight, High-Sensitivity C-Reactive Protein, and Cardiovascular Risk among Overweight and Obese Women: A Parallel Clinical Trial. Int. J. Endocrinol. 2013, 2013, 1–8. [Google Scholar] [CrossRef]
- Allison, D.; Gadbury, G.; Schwartz, L.G.; Murugesan, R.; Kraker, J.L.; Heshka, S.; Fontaine, K.R.; Heymsfield, S.B. A novel soy-based meal replacement formula for weight loss among obese individuals: A randomized controlled clinical trial. Eur. J. Clin. Nutr. 2003, 57, 514–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deibert, P.; König, D.; Schmidt-Trucksaess, A.; Zaenker, K.S.; Frey, I.; Landmann, U.; Berg, A. Weight loss without losing muscle mass in pre-obese and obese subjects induced by a high-soy-protein diet. Int. J. Obes. 2004, 28, 1349–1352. [Google Scholar] [CrossRef] [Green Version]
- Ørgaard, A.; Jensen, L. The Effects of Soy Isoflavones on Obesity. Exp. Biol. Med. 2008, 233, 1066–1080. [Google Scholar] [CrossRef] [Green Version]
- Tchernof, A.; Calles-Escandon, J.; Sites, C.K.; Poehlman, E.T. Menopause, central body fatness, and insulin resistance: Effects of hormone-replacement therapy. Coron. Artery Dis. 1998, 9, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Solon-Biet, S.; McMahon, A.C.; Ballard, J.W.O.; Ruohonen, K.; Wu, L.E.; Cogger, V.C.; Warren, A.; Huang, X.; Pichaud, N.; Melvin, R.G.; et al. The Ratio of Macronutrients, Not Caloric Intake, Dictates Cardiometabolic Health, Aging, and Longevity in Ad Libitum-Fed Mice. Cell Metab. 2014, 19, 418–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solon-Biet, S.M.; Mitchell, S.J.; Coogan, S.C.; Cogger, V.C.; Gokarn, R.; McMahon, A.C.; Raubenheimer, D.; de Cabo, R.; Simpson, S.J.; Le Couteur, D.G. Dietary Protein to Carbohydrate Ratio and Caloric Restriction: Comparing Metabolic Outcomes in Mice. Cell Rep. 2015, 11, 1529–1534. [Google Scholar] [CrossRef] [Green Version]
- Dhillon, J.; Craig, B.A.; Leidy, H.J.; Amankwaah, A.F.; Anguah, K.; Jacobs, A.; Jones, B.L.; Jones, J.B.; Keeler, C.L.; Keller, C.E.; et al. The Effects of Increased Protein Intake on Fullness: A Meta-Analysis and Its Limitations. J. Acad. Nutr. Diet. 2016, 116, 968–983. [Google Scholar] [CrossRef]
- Hochstenbach-Waelen, A.; Ab Veldhorst, M.; Nieuwenhuizen, A.; Westerterp-Plantenga, M.S.; Westerterp, K.R.; Veldhorst, M.A. Comparison of 2 diets with either 25% or 10% of energy as casein on energy expenditure, substrate balance, and appetite profile. Am. J. Clin. Nutr. 2009, 89, 831–838. [Google Scholar] [CrossRef]
- Hall, W.L.; Millward, D.J.; Long, S.J.; Morgan, L.M. Casein and whey exert different effects on plasma amino acid profiles, gastrointestinal hormone secretion and appetite. Br. J. Nutr. 2003, 89, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Leidy, H.J.; Todd, C.B.; Zino, A.Z.; Immel, J.E.; Mukherjea, R.; Shafer, R.S.; Ortinau, L.C.; Braun, M. Consuming High-Protein Soy Snacks Affects Appetite Control, Satiety, and Diet Quality in Young People and Influences Select Aspects of Mood and Cognition. J. Nutr. 2015, 145, 1614–1622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pesta, D.H.; Samuel, V.T. A high-protein diet for reducing body fat: Mechanisms and possible caveats. Nutr. Metab. 2014, 11, 53. [Google Scholar] [CrossRef] [Green Version]
- Blundell, J.; De Graaf, C.; Hulshof, T.; Jebb, S.; Livingstone, B.; Lluch, A.; Mela, D.; Salah, S.; Schuring, E.; Van Der Knaap, H.; et al. Appetite control: Methodological aspects of the evaluation of foods. Obes. Rev. 2010, 11, 251–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stubbs, R.J.; Hughes, D.A.; Johnstone, A.M.; Rowley, E.; Reid, C.; Elia, M.; Stratton, R.; Delargy, H.; King, N.; Blundell, J.E. The use of visual analogue scales to assess motivation to eat in human subjects: A review of their reliability and validity with an evaluation of new hand-held computerized systems for temporal tracking of appetite ratings. Br. J. Nutr. 2000, 84, 405–415. [Google Scholar] [CrossRef] [Green Version]
- Papakonstantinou, E.; Orfanakos, N.; Farajian, P.; Kapetanakou, A.E.; Makariti, I.P.; Grivokostopoulos, N.; Ha, M.-A.; Skandamis, P.N. Short-term effects of a low glycemic index carob-containing snack on energy intake, satiety, and glycemic response in normal-weight, healthy adults: Results from two randomized trials. Nutrients 2017, 42, 12–19. [Google Scholar] [CrossRef] [Green Version]
- Pol, K.; De Graaf, C.; Meyer, D.; Mars, M. The efficacy of daily snack replacement with oligofructose-enriched granola bars in overweight and obese adults: A 12-week randomised controlled trial. Br. J. Nutr. 2018, 119, 1076–1086. [Google Scholar] [CrossRef]
- Douglas, S.M.; Ortinau, L.C.; Hoertel, H.A.; Leidy, H.J. Low, moderate, or high protein yogurt snacks on appetite control and subsequent eating in healthy women. Appetite 2013, 60, 117–122. [Google Scholar] [CrossRef]
- Drapeau, V.; King, N.; Hetherington, M.; Doucet, E.; Blundell, J.; Tremblay, A. Appetite sensations and satiety quotient: Predictors of energy intake and weight loss. Appetite 2007, 48, 159–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ince, B.A.; Anderson, E.J.; Neer, R.M. Lowering Dietary Protein to U.S. Recommended Dietary Allowance Levels Reduces Urinary Calcium Excretion and Bone Resorption in Young Women. J. Clin. Endocrinol. Metab. 2004, 89, 3801–3807. [Google Scholar] [CrossRef] [Green Version]
- Granic, A.; Mendonça, N.; Sayer, A.A.; Hill, T.R.; Davies, K.; Adamson, A.; Siervo, M.; Mathers, J.C.; Jagger, C. Low protein intake, muscle strength and physical performance in the very old: The Newcastle 85+ Study. Clin. Nutr. 2018, 37, 2260–2270. [Google Scholar] [CrossRef] [Green Version]
- Intention to Treat Analysis and Per Protocol Analysis: Complementary Information. Available online: https://pubmed.ncbi.nlm.nih.gov/23373104/ (accessed on 29 June 2021).
- Ward, L.C. Bioelectrical impedance analysis for body composition assessment: Reflections on accuracy, clinical utility, and standardisation. Eur. J. Clin. Nutr. 2019, 73, 194–199. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| HP Snack (50 g Soybeans) | LP Snack (3.5 Servings Fruit) | |
|---|---|---|
| Energy (g) | 210 | ≈210 |
| Protein (g) | 18.2 | <2 |
| Carbohydrate (g) | 15 | ≈50 |
| Fat (g) | 10 | <1 |
| Fiber (g) | 4.6 | 4–6 |
| Variables | Contrast | β (SE) | 95% CI | p-Value |
|---|---|---|---|---|
| Body Mass (kg) | HP vs. LP | −3.7 (0.34) | −4.46 to −3.11 | <0.001 |
| BMI (kg.m−2) | HP vs. LP | −1.38 (0.13) | −1.63 to −1.13 | <0.001 |
| WC (cm) # | HP vs. LP | −3.46 (0.76) | −4.98 to −1.95 | <0.001 |
| BFP (%) | HP vs. LP | −2.80 (0.27) | −3.33 to −2.26 | <0.001 |
| SMM (kg) | HP vs. LP | 0.91 (0.21) | 0.5 to 1.3 | <0.001 |
| Appetite (mm) # | HP vs. LP | −11.44 (0.65) | −12.73 to −10.16 | <0.001 |
| Protein (g/day) | HP vs. LP | 19.46 (1.23) | 17.03 to 21.89 | <0.001 |
| Fat (g/day) # | HP vs. LP | −6.31 (1.67) | −9.62 to −2.99 | <0.001 |
| Fiber (g/day) | HP vs. LP | −0.59 (0.43) | −1.45 to 0.28 | 0.180 |
| Carb (g/day) # | HP vs. LP | −62.43 (6.53) | −75.38 to −49.49 | <0.001 |
| Energy (kcal/day) # | HP vs. LP | −238.37 (30.93) | −299.70 to −177.03 | <0.001 |
| Relative protein (g/kg/day) | HP vs. LP | 0.38 (0.03) | 0.32 to 0.44 | <0.001 |
| Nutrient | Group | Pre | Post | Post-Pre | p-Value of Paired t-Test |
|---|---|---|---|---|---|
| Protein (g/day) | HP | 51.37 ± 7.36 | 74.94 ± 6.40 * | 23.58 ± 8.35 * | <0.001 |
| LP | 48.80 ± 7.21 | 55.02 ± 6.30 | 6.22 ± 8.84 | <0.001 | |
| Fat (g/day) | HP | 48.87 ± 5.42 | 45.88 ± 8.37 * | −2.98 ± 9.94 * | 0.035 |
| LP | 46.36 ± 7.97 | 50.91 ± 9.56 | 4.55 ± 7.87 | <0.001 | |
| Fiber (g/day) | HP | 11.65 ± 2.82 * | 12.77 ± 2.29 * | 1.12 ± 2.30 | 0.001 |
| LP | 13.02 ± 3.70 | 14.02 ± 3.03 | 1.00 ± 3.12 | 0.021 | |
| Carbohydrate (g/day) | HP | 253.48 ± 39.24 | 195.04 ± 33.47 * | −58.44 ± 44.96 * | <0.001 |
| LP | 247.05 ± 57.55 | 253.45 ± 55.55 | 6.40 ± 32.29 | 0.147 | |
| Energy (kcal/day) | HP | 1659.17 ± 172.29 | 1492.88 ± 175.82 * | −166.29 ± 205.64 * | <0.001 |
| LP | 1600.69 ± 239.62 | 1692.07 ± 239.19 | 91.38 ± 132.04 | <0.001 | |
| Relative protein (g/kg/day) | HP | 0.84 ± 0.15 | 1.28 ± 0.20 * | 0.45 ± 0.16 * | <0.001 |
| LP | 0.79 ± 0.14 | 0.87 ± 0.12 | 0.09 ± 0.14 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haghighat, N.; Ashtary-Larky, D.; Bagheri, R.; Wong, A.; Cheraghloo, N.; Moradpour, G.; Nordvall, M.; Asbaghi, O.; Moeinvaziri, N.; Amini, M.; et al. Effects of 6 Months of Soy-Enriched High Protein Compared to Eucaloric Low Protein Snack Replacement on Appetite, Dietary Intake, and Body Composition in Normal-Weight Obese Women: A Randomized Controlled Trial. Nutrients 2021, 13, 2266. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072266
Haghighat N, Ashtary-Larky D, Bagheri R, Wong A, Cheraghloo N, Moradpour G, Nordvall M, Asbaghi O, Moeinvaziri N, Amini M, et al. Effects of 6 Months of Soy-Enriched High Protein Compared to Eucaloric Low Protein Snack Replacement on Appetite, Dietary Intake, and Body Composition in Normal-Weight Obese Women: A Randomized Controlled Trial. Nutrients. 2021; 13(7):2266. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072266
Chicago/Turabian StyleHaghighat, Neda, Damoon Ashtary-Larky, Reza Bagheri, Alexei Wong, Neda Cheraghloo, Gholamreza Moradpour, Michael Nordvall, Omid Asbaghi, Nader Moeinvaziri, Masoud Amini, and et al. 2021. "Effects of 6 Months of Soy-Enriched High Protein Compared to Eucaloric Low Protein Snack Replacement on Appetite, Dietary Intake, and Body Composition in Normal-Weight Obese Women: A Randomized Controlled Trial" Nutrients 13, no. 7: 2266. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13072266