
Type of Physical Training and Selected Aspects of Psychological Functioning of Women with Obesity: A Randomised Trial

 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
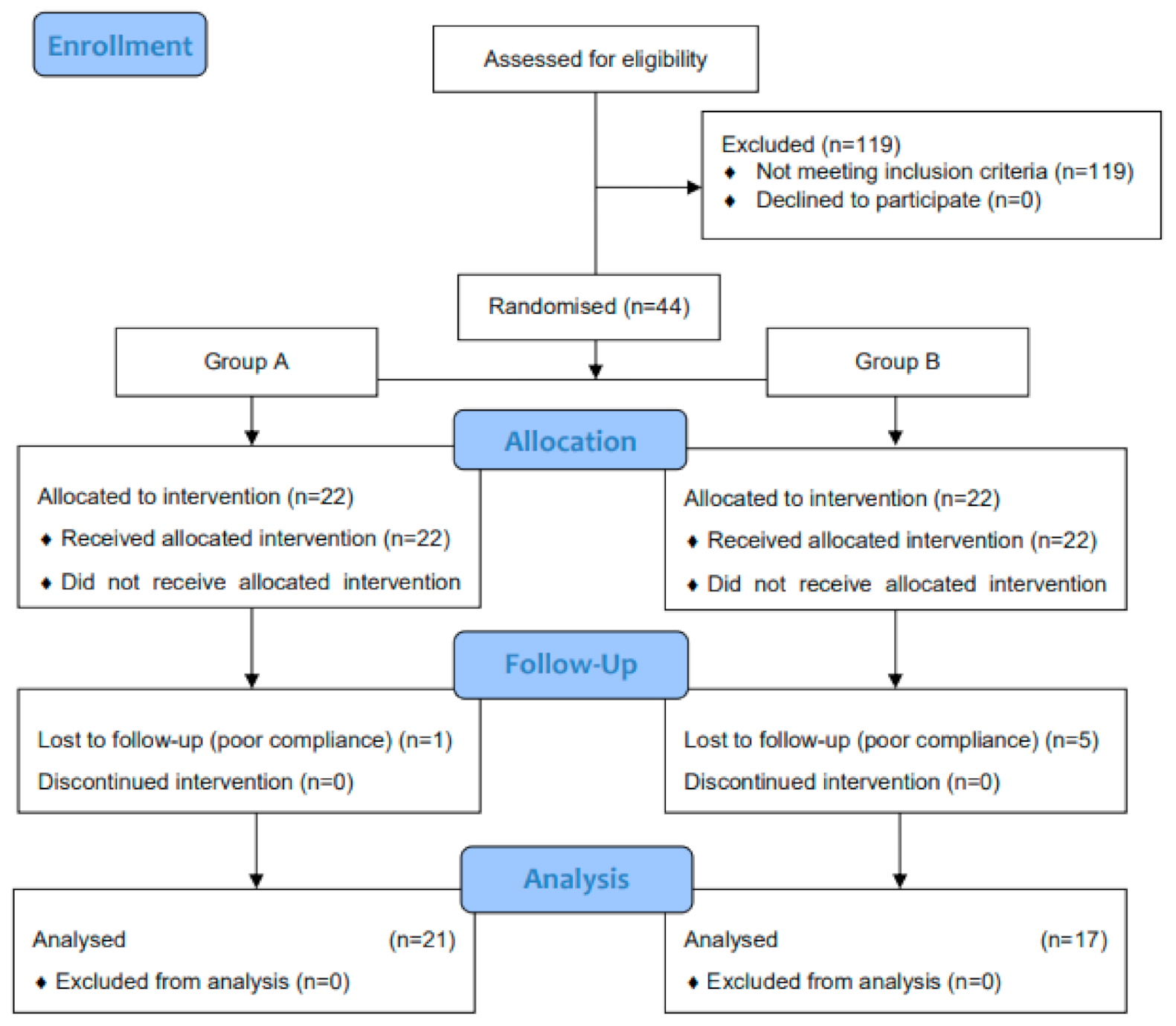
2.1. Trial Information
2.2. Participants
2.3. Study Design
2.4. Intervention
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. Strengths of the Study
4.2. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Umpierre, D.; Ribeiro, P.A.B.; Kramer, C.K.; Leitão, C.B.; Zucatti, A.T.N.; Azevedo, M.J.; Gross, J.L.; Ribeiro, J.P.; Schaan, B.D. Physical activity advice only or structured exercise training and association with HbA1c levels in type 2 diabetes: A systematic review and meta-analysis. JAMA J. Am. Med. Assoc. 2011, 305, 1790–1799. [Google Scholar] [CrossRef] [Green Version]
- Pinckard, K.; Baskin, K.K.; Stanford, K.I. Effects of Exercise to Improve Cardiovascular Health. Front. Cardiovasc. Med. 2019, 6, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marc-Hernández, A.; Ruiz-Tovar, J.; Aracil, A.; Guillén, S.; Moya-Ramón, M. Impact of Exercise on Body Composition and Cardiometabolic Risk Factors in Patients Awaiting Bariatric Surgery. Obes. Surg. 2019, 29, 3891–3900. [Google Scholar] [CrossRef] [PubMed]
- Abd El-Kader, S.M.; Al-Jiffri, O.H. Impact of weight reduction on insulin resistance, adhesive molecules and adipokines dysregulation among obese type 2 diabetic patients. Afr. Health Sci. 2018, 18, 873–883. [Google Scholar] [CrossRef]
- Hayashino, Y.; Jackson, J.L.; Hirata, T.; Fukumori, N.; Nakamura, F.; Fukuhara, S.; Tsujii, S.; Ishii, H. Effects of exercise on C-reactive protein, inflammatory cytokine and adipokine in patients with type 2 diabetes: A meta-analysis of randomized controlled trials. Metabolism 2014, 63, 431–440. [Google Scholar] [CrossRef] [PubMed]
- Lugo, D.; Pulido, A.L.; Mihos, C.G.; Issa, O.; Cusnir, M.; Horvath, S.A.; Lin, J.; Santana, O. The effects of physical activity on cancer prevention, treatment and prognosis: A review of the literature. Complement. Ther. Med. 2019, 44, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Ramos, R.M.; Coelho-Júnior, H.J.; Asano, R.Y.; Prado, R.C.R.; Silveira, R.; Urtado, C.B.; de Lima, L.C.R.; Aguiar, S.d.S.; Prestes, J.; Medeiros, A.I.A.; et al. Impact of Moderate Aerobic Training on Physical Capacities of Hypertensive Obese Elderly. Gerontol. Geriatr. Med. 2019, 5, 233372141985969. [Google Scholar] [CrossRef] [Green Version]
- Castro, E.A.; Peinado, A.B.; Benito, P.J.; Galindo, M.; González-Gross, M.; Cupeiro, R. What is the most effective exercise protocol to improve cardiovascular fitness in overweight and obese subjects? J. Sport Health Sci. 2017, 6, 454–461. [Google Scholar] [CrossRef] [Green Version]
- Shin, Y.-A. How Does Obesity and Physical Activity Affect Aging? Focused on Telomere as a Biomarker of Aging. J. Obes. Metab. Syndr. 2019, 28, 92–104. [Google Scholar] [CrossRef]
- Bauman, A.E.; Grunseit, A.C.; Rangul, V.; Heitmann, B.L. Physical activity, obesity and mortality: Does pattern of physical activity have stronger epidemiological associations? BMC Public Health 2017, 17, 788. [Google Scholar] [CrossRef]
- Sattelmair, J.; Pertman, J.; Ding, E.L.; Kohl, H.W.; Haskell, W.; Lee, I.M. Dose response between physical activity and risk of coronary heart disease: A meta-analysis. Circulation 2011, 124, 789–795. [Google Scholar] [CrossRef] [Green Version]
- Saris, W.H.M.; Blair, S.N.; Van Baak, M.A.; Eaton, S.B.; Davies, P.S.W.; Di Pietro, L.; Fogelholm, M.; Rissanen, A.; Schoeller, D.; Swinburn, B.; et al. How much physical activity is enough to prevent unhealthy weight gain? Outcome of the IASO 1st stock conference and consensus statement. Obes. Rev. 2003, 4, 101–114. [Google Scholar] [CrossRef]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sports Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef] [PubMed]
- Swift, D.L.; McGee, J.E.; Earnest, C.P.; Carlisle, E.; Nygard, M.; Johannsen, N.M. The Effects of Exercise and Physical Activity on Weight Loss and Maintenance. Prog. Cardiovasc. Dis. 2018, 61, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Wiklund, P.; Alen, M.; Munukka, E.; Cheng, S.M.; Yu, B.; Pekkala, S.; Cheng, S. Metabolic response to 6-week aerobic exercise training and dieting in previously sedentary overweight and obese pre-menopausal women: A randomized trial. J. Sport Health Sci. 2014, 3, 217–224. [Google Scholar] [CrossRef] [Green Version]
- Hamasaki, H.; Kawashima, Y.; Tamada, Y.; Furuta, M.; Katsuyama, H.; Sako, A.; Yanai, H. Associations of low-intensity resistance training with body composition and lipid profile in obese patients with type 2 diabetes. PLoS ONE 2015, 10, e0132959. [Google Scholar] [CrossRef]
- Skrypnik, D.; Bogdański, P.; Mądry, E.; Karolkiewicz, J.; Ratajczak, M.; Kryściak, J.; Pupek-Musialik, D.; Walkowiak, J. Effects of Endurance and Endurance Strength Training on Body Composition and Physical Capacity in Women with Abdominal Obesity. Obes. Facts 2015, 8, 175–187. [Google Scholar] [CrossRef] [PubMed]
- Skrypnik, D.; Ratajczak, M.; Karolkiewicz, J.; Madry, E.; Pupek-Musialik, D.; Hansdorfer-Korzon, R.; Walkowiak, J.; Jakubowski, H.; Bogdański, P. Effects of endurance and endurance-strength exercise on biochemical parameters of liver function in women with abdominal obesity. Biomed. Pharmacother. 2016, 80, 1–7. [Google Scholar] [CrossRef]
- Szulińska, M.; Skrypnik, D.; Ratajczak, M.; Karolkiewicz, J.; Madry, E.; Musialik, K.; Walkowiak, J.; Jakubowski, H.; Bogdański, P. Effects of Endurance and Endurance-strength Exercise on Renal Function in Abdominally Obese Women with Renal Hyperfiltration: A Prospective Randomized Trial. Biomed. Environ. Sci. 2016, 29, 706–712. [Google Scholar] [CrossRef] [PubMed]
- Skrypnik, D.; Bogdański, P.; Skrypnik, K.; Mądry, E.; Karolkiewicz, J.; Szulińska, M.; Suliburska, J.; Walkowiak, J. Influence of endurance and endurance-strength training on mineral status in women with abdominal obesity: A randomized trial. Medicine 2019, 98, e14909. [Google Scholar] [CrossRef] [PubMed]
- Maciaszek, J.; Skrypnik, D.; Ratajczak, M.; Stemplewski, R.; Osinski, W.; Bogdanski, P.; Madry, E.; Walkowiak, J.; Karolkiewicz, J. Two aerobic exercise programs in management of back pain among middle-aged obese women: A randomized controlled study. Hum. Mov. 2016, 17, 72–79. [Google Scholar] [CrossRef] [Green Version]
- Bernard, P.; Doré, I.; Romain, A.J.; Hains-Monfette, G.; Kingsbury, C.; Sabiston, C. Dose response association of objective physical activity with mental health in a representative national sample of adults: A cross-sectional study. PLoS ONE 2018, 13, e0204682. [Google Scholar] [CrossRef]
- Romain, A.J.; Marleau, J.; Baillot, A. Association between physical multimorbidity, body mass index and mental health/disorders in a representative sample of people with obesity. J. Epidemiol. Community Health 2019, 73, 874–880. [Google Scholar] [CrossRef] [PubMed]
- Brechan, I.; Kvalem, I.L. Relationship between body dissatisfaction and disordered eating: Mediating role of self-esteem and depression. Eat. Behav. 2015, 17, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Yazdani, N.; Hosseini, S.V.; Amini, M.; Sobhani, Z.; Sharif, F.; Khazraei, H. Relationship between Body Image and Psychological Well-being in Patients with Morbid Obesity. IJBNM 2018, 6, 175–184. [Google Scholar]
- Unlu, S.; Aykut, M.; Borlu, A.; Kaner, G. Are low self-esteem and body image dissatisfaction related with body mass index? Prog. Nutr. 2019, 21, 94–103. [Google Scholar] [CrossRef]
- Osama, A.J.; Shehab, A.E.K. Psychological wellbeing and biochemical modulation in response to weight loss in obese type 2 diabetes patients. Afr. Health Sci. 2015, 15, 503–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vancini, R.L.; Rayes, A.B.R.; de Lira, C.A.B.; Sarro, K.J.; Andrade, M.S. Pilates and aerobic training improve levels of depression, anxiety and quality of life in overweight and obese individuals. Arq. Neuropsiquiatr. 2017, 75, 850–857. [Google Scholar] [CrossRef] [Green Version]
- Tiwari, S.; Dutt, K.; Kumar, R.; Dhananjai, S. Sadashiv Reducing psychological distress and obesity through Yoga practice. Int. J. Yoga 2013, 6, 66. [Google Scholar] [CrossRef] [PubMed]
- Ten Hoor, G.A.; Kok, G.; Peters, G.J.Y.; Frissen, T.; Schols, A.M.W.J.; Plasqui, G. The Psychological Effects of Strength Exercises in People who are Overweight or Obese: A Systematic Review. Sports Med. 2017, 47, 2069–2081. [Google Scholar]
- Ghroubi, S.; Elleuch, H.; Chikh, T.; Kaffel, N.; Abid, M.; Elleuch, M. Physical training combined with dietary measures in the treatment of adult obesity. A comparison of two protocols. Ann. Phys. Rehabil. Med. 2009, 52, 394–413. [Google Scholar] [CrossRef] [Green Version]
- Ghroubi, S.; Kossemtini, W.; Mahersi, S.; Elleuch, W.; Chaabene, M.; Elleuch, M.H. Contribution of isokinetic muscle strengthening in the rehabilitation of obese subjects. Ann. Phys. Rehabil. Med. 2016, 59, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Juczyński, Z.; Ogińska-Bulik, N. NPSR Tools for Measuring Stress and for Coping with Stress; Pracownia Testów Psychologicznych: Warszawa, Poland, 2009. [Google Scholar]
- Laguna, M.; Lachowicz-Tabaczek, K.; Dzwonkowska, I. The Rosenberg Self-Esteem Scale: Polish adaptation of the scale. Psychol. Społeczna 2007, 4, 164–176. [Google Scholar]
- Cooper, P.; Taylor, M.; Cooper, Z.; Fairburn, C. The development and validation of the Body Satisfaction Questionnaire. Int. J. Eat. Disord. 1987, 6, 485–494. [Google Scholar] [CrossRef]
- Stunkard, A.J.; Sorensen, T.; Schulsinger, F. Use of the Danish Adoption Register for the study of obesity and thinness. Res. Publ. Assoc. Res. Nerv. Ment. Dis. 1983, 60, 115–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brytek-Matera, A.; Rogoza, R.; Czepczor-Bernat, K. The Three-Factor Eating Questionnaire-R18 Polish version: Factor structure analysis among normal weight and obese adult women. Arch. Psychiatry Psychother. 2017, 3, 81–90. [Google Scholar] [CrossRef]
- Singh, D.; Singh, D. Shape and Significance of Feminine Beauty: An Evolutionary Perspective. Sex Roles 2011, 64, 723–731. [Google Scholar] [CrossRef]
- Furnham, A.; Swami, V.; Shah, K. Body weight, waist-to-hip ratio and breast size correlates of ratings of attractiveness and health. Pers. Individ. Dif. 2006, 41, 443–454. [Google Scholar] [CrossRef]
- Platek, S.M.; Singh, D. Optimal waist-to-hip ratios in women activate neural reward centers in men. PLoS ONE 2010, 5, e9042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holliday, I.E.; Longe, O.A.; Thai, N.J.; Hancock, P.J.B.; Tovée, M.J. Bmi not WHR modulates BOLD fMRI responses in a sub-cortical reward network when participants judge the attractiveness of human female bodies. PLoS ONE 2011, 6, e27255. [Google Scholar] [CrossRef]
- Aquino, M.T.; Orense, C.L.; Tanchoco, C.C.; Amarra, S.V.; Tajan, M.G.; Dela Cruz, E.O. Correlates of body image satisfaction among economically depressed Urban Filipino women. Philipp. J. Sci. 2009, 138, 67–74. [Google Scholar]
- Chao, H.L. Body image change in obese and overweight persons enrolled in weight loss intervention programs: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0124036. [Google Scholar] [CrossRef] [Green Version]
- Lasikiewicz, N.; Myrissa, K.; Hoyland, A.; Lawton, C.L. Psychological benefits of weight loss following behavioural and/or dietary weight loss interventions. A systematic research review. Appetite 2014, 72, 123–137. [Google Scholar] [CrossRef] [Green Version]
- Weinberger, N.A.; Kersting, A.; Riedel-Heller, S.G.; Luck-Sikorski, C. Body Dissatisfaction in Individuals with Obesity Compared to Normal-Weight Individuals: A Systematic Review and Meta-Analysis. Obes. Facts 2017, 9, 424–441. [Google Scholar] [CrossRef] [PubMed]
- Amissah, C.M.; Student, M.; Nyarko, K.; Gyasi-Gyamerah, A.A.; Anto-Winne, M.N. Relationships among Body Image, Eating Behavior, and Psychological Health of University of Ghana Students. Int. J. Hum. Soc. Sci. 2015, 5, 192–203. [Google Scholar]
- Rodrigues, S.; Paiva, J.S.; Dias, D.; Aleixo, M.; Filipe, R.M.; Cunha, J.P.S. Cognitive Impact and Psychophysiological Effects of Stress Using a Biomonitoring Platform. Int. J. Environ. Res. Public Health 2018, 15, 1080. [Google Scholar] [CrossRef] [Green Version]
- Levoy, E.; Lazaridou, A.; Brewer, J.; Fulwiler, C. An exploratory study of Mindfulness Based Stress Reduction for emotional eating. Appetite 2017, 109, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Manna, P.; Jain, S.K. Obesity, Oxidative Stress, Adipose Tissue Dysfunction, and the Associated Health Risks: Causes and Therapeutic Strategies. Metab. Syndr. Relat. Disord. 2015, 13, 423–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomiyama, A.J. Stress and Obesity. Annu. Rev. Psychol. 2019, 70, 703–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morici, G.; Gruttad’Auria, C.I.; Baiamonte, P.; Mazzuca, E.; Castrogiovanni, A.; Bonsignore, M.R. Endurance training: Is it bad for you? Breathe 2016, 12, 140–147. [Google Scholar] [CrossRef]
- Westcott, W.L. Resistance Training is Medicine. Curr. Sports Med. Rep. 2012, 11, 209–216. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Group A before Intervention (n = 21) | Group B before Intervention (n = 17) | p | g | Group A after Intervention (n = 21) | Group B after Intervention (n = 17) | p | g | |
|---|---|---|---|---|---|---|---|---|---|
| Body mass [kg] | 91.7 ± 11.8 | 94.5 ± 13.4 | 0.325 | 0.2234 | 89.5 ± 11.8 | 91.8 ± 13.7 | 0.628 | 0.1814 | |
| BMI [kg/m2] | 35.2 ± 3.9 | 34.9 ± 3.8 | 0.747 | 0.0778 | 34.3 ± 3.9 | 33.9 ± 4.1 | 0.725 | 0.1002 | |
| Waist circumference [cm] | 110.8 ± 10.2 | 111.6 ± 11.3 | 0.883 | 0.0747 | 105.5 ± 11.1 | 104.0 ± 10.5 | 0.538 | 0.1384 | |
| Hip circumference [cm] | 115.0 ± 8.0 | 115.8 ± 9.4 | 0.577 | 0.0924 | 111.7 ±8.5 | 112.4 ±9.7 | 0.837 | 0.0773 | |
| WHR | 0.96 ± 0.06 | 0.96 ± 0.07 | 0.770 | 0.00 | 0.94 ± 0.07 | 0.92 ± 0.07 | 0.445 | 0.2857 | |
| PSS-10 | 18.00 ± 7.3 | 18.8 ± 7.4 | 0.714 | 0.1089 | 17.1 ± 7.2 | 17.2 ± 7.3 | 0.973 | 0.0138 | |
| SES | 29.1 ± 4.6 | 27.2 ± 4.1 | 0.183 * | 0.4333 | 29.4 ± 4.09 | 28.3 ± 4.3 | 0.414 | 0.2629 | |
| BSQ-34 | 97.4 ± 23.07 | 99.2 ± 30.2 | 0.836 | 0.0680 | 82.5 ± 24.4 | 80.9 ± 25.8 | 0.814 | 0.0639 | |
| FRS | CS | 6.62 ± 0.92 | 6.70 ± 1.16 | 0.978 * | 0.0774 | 5.71 ±0.78 | 6.29 ±1.31 | 0.230 * | 0.5528 |
| IS | 4.04 ± 0.59 | 4.12 ± 0.60 | 0.726 * | 0.1346 | 4.00 ± 0.63 | 4.00 ± 0.71 | 0.987 * | 0.00 | |
| TFEQ-18 | CR | 14.5 ±3.1 | 13.8 ± 2.8 | 0.483 * | 0.2357 | 14.7 ± 2.5 | 15.5 ± 2.6 | 0.371 | 0.3144 |
| UE | 20.4 ±3.8 | 20.5 ± 4.6 | 0.948 | 0.0239 | 19.3 ±3.7 | 19.2 ± 4.4 | 0.906 | 0.0248 | |
| EE | 6.8 ± 2.5 | 8.4 ± 2.09 | 0.0835 * | 06877 | 6.4 ± 1.4 | 7.6 ± 2.001 | 0.037 | 0.7087 | |
| Variables | Group A before Intervention (n = 21) | Group A after Intervention (n = 21) | p | d | Group B before Intervention (n = 17) | Group B after Intervention (n = 17) | p | d | |
|---|---|---|---|---|---|---|---|---|---|
| Body mass [kg] | 91.7 ± 11.8 | 89.5 ± 11.8 | <0.001 | 0.181 | 94.5 ± 13.4 | 91.8 ± 13.7 | 0.003 | 0.193 | |
| BMI [kg/m2] | 35.2 ± 3.9 | 34.3 ± 3.9 | <0.001 | 0.225 | 34.9 ± 3.8 | 33.9 ± 4.1 | <0.001 | 0.245 | |
| Waist circumference [cm] | 110.8 ± 10.2 | 105.5 ± 11.1 | <0.001 | 0.485 | 111.6 ± 11.3 | 104.0 ± 10.5 | <0.001 | 0.675 | |
| Hip circumference [cm] | 115.0 ± 8.0 | 111.7 ± 8.5 | <0.001 | 0.390 | 115.8 ± 9.4 | 112.4 ±9.7 | 0.001 | 0.345 | |
| WHR | 0.96 ± 0.06 | 0.94 ± 0.07 | 0.010 | 0.299 | 0.96 ± 0.07 | 0.92 ± 0.07 | 0.005 | 0.554 | |
| PSS-10 | 18.00 ± 7.3 | 17.1 ± 7.2 | 0.471 | 0.121 | 18.8 ± 7.4 | 17.2 ± 7.3 | 0.151 | 0.211 | |
| SES | 29.1 ± 4.6 | 29.4 ± 4.09 | 0.298 | 0.067 | 27.2 ± 4.1 | 28.3 ± 4.3 | 0.106 * | 0.254 | |
| BSQ-34 | 97.4 ± 23.07 | 82.5 ± 24.4 | <0.001 | 0.612 | 99.2 ± 30.2 | 80.9 ± 25.8 | 0.008 | 0.632 | |
| FRS | CS | 6.62 ± 0.92 | 5.71 ±0.78 | 0.001 * | 1.041 | 6.70 ± 1.16 | 6.29 ±1.31 | 0.017 | 0.321 |
| IS | 4.04 ± 0.59 | 4.00 ± 0.63 | 0.767 * | 0.063 | 4.12 ± 0.60 | 4.00 ± 0.71 | 0.361 * | 0.177 | |
| TFEQ-18 | CR | 14.5 ±3.1 | 14.7 ± 2.5 | 0.802 * | 0.069 | 13.8 ± 2.8 | 15.5 ± 2.6 | 0.004 | 0.610 |
| UE | 20.4 ±3.8 | 19.3 ±3.7 | 0.233 | 0.286 | 20.5 ± 4.6 | 19.2 ± 4.4 | 0.135 | 0.280 | |
| EE | 6.8 ± 2.5 | 6.4 ± 1.4 | 0.394 * | 0.192 | 8.4 ± 2.09 | 7.6 ± 2.001 | 0.017 | 0.379 | |
| Variables | Group A (n = 21) | Group B (n = 17) | p | g | |
|---|---|---|---|---|---|
| δ Body mass [kg] | −2.20 ± 2.12 | −2.71 ± 2.25 | 0.371 | 0.234 | |
| δ BMI [kg/m2] | −0.84 ± 0.80 | −0.99 ± 0.80 | 0.348 | 0.187 | |
| δ Waist circumference [cm] | −5.26 ± 4.45 | −7.65 ± 4.56 | 0.142 * | 0.531 | |
| δ Hip circumference [cm] | −3.33 ± 2.83 | −3.41 ± 3.58 | 0.547 | 0.025 | |
| δ WHR | −0.02 ± 0.03 | −0.04 ± 0.05 | 0.207 | 0.498 | |
| δ PSS-10 | −0.90 ± 5.64 | −1.71 ± 4.66 | 0.642 | 0.154 | |
| δ SES | 0.33 ± 2.43 | 1.12 ± 2.61 | 0.447 * | 0.314 | |
| δ BSQ–34 | −14.90 ± 13.5 | −18.64 ± 25.4 | 0.565 | 0.189 | |
| δ FRS | CS | −0.90 ± 0.83 | −0.41 ± 0.50 | 0.035 * | 0.697 |
| IS | −0.05 ± 0.67 | −0.12 ± 0.48 | 0.766 * | 0.118 | |
| δ TFEQ–18 | CR | 0.24 ± 2.96 | 1.65 ± 2.06 | 0.106 | 0.542 |
| UE | −1.05 ± 3.90 | −1.29 ± 3.38 | 0.538 * | 0.065 | |
| EE | −0.43 ± 2.09 | −0.82 ± 1.28 | 0.941 * | 0.219 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bąk-Sosnowska, M.; Gruszczyńska, M.; Skrypnik, D.; Grzegorczyn, S.; Karolkiewicz, J.; Ratajczak, M.; Mądry, E.; Walkowiak, J.; Bogdański, P. Type of Physical Training and Selected Aspects of Psychological Functioning of Women with Obesity: A Randomised Trial. Nutrients 2021, 13, 2555. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082555
Bąk-Sosnowska M, Gruszczyńska M, Skrypnik D, Grzegorczyn S, Karolkiewicz J, Ratajczak M, Mądry E, Walkowiak J, Bogdański P. Type of Physical Training and Selected Aspects of Psychological Functioning of Women with Obesity: A Randomised Trial. Nutrients. 2021; 13(8):2555. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082555
Chicago/Turabian StyleBąk-Sosnowska, Monika, Magdalena Gruszczyńska, Damian Skrypnik, Sławomir Grzegorczyn, Joanna Karolkiewicz, Marzena Ratajczak, Edyta Mądry, Jarosław Walkowiak, and Paweł Bogdański. 2021. "Type of Physical Training and Selected Aspects of Psychological Functioning of Women with Obesity: A Randomised Trial" Nutrients 13, no. 8: 2555. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13082555