
Association of Estimated Salt and Miso Intake with the Prevalence of Obesity in People with Type 2 Diabetes: A Cross-Sectional Study

 , , , , , ,
, , , , , , 
Abstract
:1. Introduction
2. Method
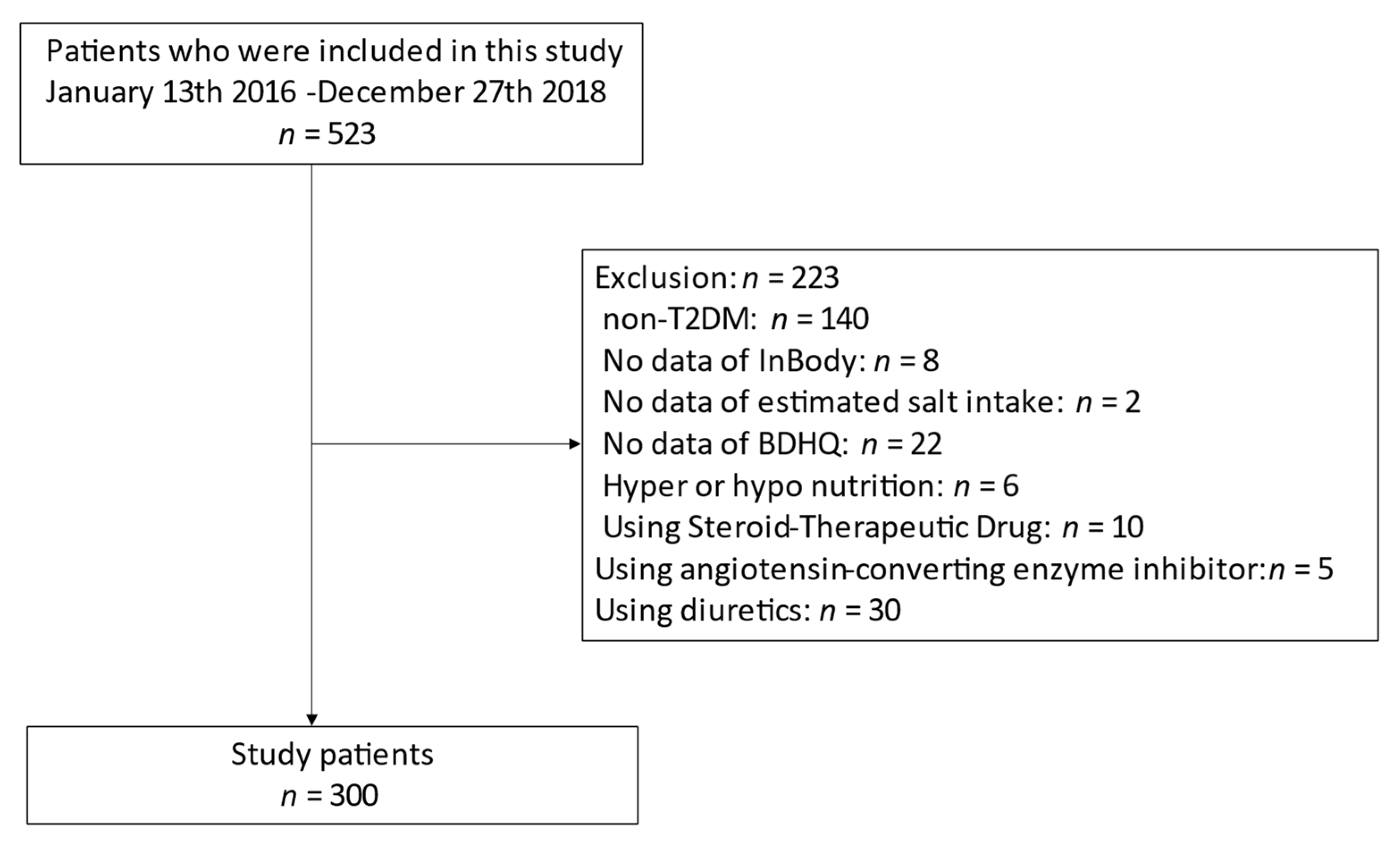
2.1. Study Participants
2.2. Data Collection
2.3. Definition of Obesity
2.4. Data on Habitual Dietary Intake, including Habitual Miso Consumption
2.5. Definition of Estimated Salt Intake
2.6. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- He, F.J.; Li, J.; Macgregor, G.A. Effect of longer term modest salt reduction on blood pressure: Cochrane systematic review and meta-analysis of randomised trials. BMJ 2013, 346, f1325. [Google Scholar] [CrossRef] [Green Version]
- Strazzullo, P.; D’Elia, L.; Kandala, N.B.; Cappuccio, F.P. Salt intake, stroke, and cardiovascular disease: Meta-analysis of prospective studies. BMJ 2009, 339, b4567. [Google Scholar] [CrossRef] [Green Version]
- Feldstein, C.A. Salt intake, hypertension and diabetes mellitus. J. Hum. Hypertens. 2002, 16 (Suppl. 1), S48–S51. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. 5. Facilitating Behavior Change and Well-being to Improve Health Outcomes: Standards of Medical Care in Diabetes-2020. Diabetes Care 2020, 43 (Suppl. 1), S48–S65. [Google Scholar] [CrossRef] [Green Version]
- Strom, B.L.; Anderson, C.A.; Ix, J.H. Sodium reduction in populations: Insights from the Institute of Medicine committee. JAMA 2013, 310, 31–32. [Google Scholar] [CrossRef] [PubMed]
- Horikawa, C.; Yoshimura, Y.; Kamada, C.; Tanaka, S.; Tanaka, S.; Hanyu, O.; Araki, A.; Ito, H.; Tanaka, A.; Ohashi, Y.; et al. Dietary sodium intake and incidence of diabetes complications in Japanese patients with type 2 diabetes: Analysis of the Japan Diabetes Complications Study (JDCS). J. Clin. Endocrinol. Metab. 2014, 99, 3635–3643. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.S.; Oh, S.W. Sodium density and obesity; the Korea National Health and Nutrition Examination Survey 2007–2010. Eur. J. Clin. Nutr. 2013, 67, 141–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lanaspa, M.A.; Kuwabara, M.; Andres-Hernando, A.; Li, N.; Cicerchi, C.; Jensen, T.; Orlicky, D.J.; Roncal-Jimenez, C.A.; Ishimoto, T.; Nakagawa, T.; et al. High salt intake causes leptin resistance and obesity in mice by stimulating endogenous fructose production and metabolism. Proc. Natl. Acad. Sci. USA 2018, 115, 3138–3143. [Google Scholar] [CrossRef] [Green Version]
- Zhou, L.; Stamler, J.; Chan, Q.; Van Horn, L.; Daviglus, M.L.; Dyer, A.R.; Miura, K.; Okuda, N.; Wu, Y.; Ueshima, H.; et al. Salt intake and prevalence of overweight/obesity in Japan, China, the United Kingdom, and the United States: The INTERMAP Study. Am. J. Clin. Nutr. 2019, 110, 34–40. [Google Scholar] [CrossRef]
- Larsen, S.C.; Ängquist, L.; Sørensen, T.I.; Heitmann, B.L. 24h urinary sodium excretion and subsequent change in weight, waist circumference and body composition. PLoS ONE 2013, 8, e69689. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, Y.; Kosaki, K.; Sugasawa, T.; Matsui, M.; Yoshioka, M.; Aoki, K.; Kuji, T.; Mizuno, R.; Kuro-O, M.; Yamagata, K.; et al. High Salt Diet Impacts the Risk of Sarcopenia Associated with Reduction of Skeletal Muscle Performance in the Japanese Population. Nutrients 2020, 12, 3474. [Google Scholar] [CrossRef] [PubMed]
- Ota, Y.; Kitamura, M.; Tsuji, K.; Torigoe, K.; Yamashita, A.; Abe, S.; Muta, K.; Uramatsu, T.; Obata, Y.; Furutani, J.; et al. Risk Reduction for End-Stage Renal Disease by Dietary Guidance Using the Gustatory Threshold Test for Salty Taste. Nutrients 2020, 12, 2703. [Google Scholar] [CrossRef] [PubMed]
- Koo, H.S.; Kim, Y.C.; Ahn, S.Y.; Oh, S.W.; Kim, S.; Chin, H.J.; Park, J.H. Estimating 24-hour urine sodium level with spot urine sodium and creatinine. J. Korean Med. Sci. 2014, 29 (Suppl. 2), S97–S102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, T.; Okamura, T.; Miura, K.; Kadowaki, T.; Ueshima, H.; Nakagawa, H.; Hashimoto, T. A simple method to estimate populational 24-h urinary sodium and potassium excretion using a casual urine specimen. J. Hum. Hypertens. 2002, 16, 97–103. [Google Scholar] [CrossRef] [Green Version]
- Umemura, S.; Arima, H.; Arima, S.; Asayama, K.; Dohi, Y.; Hirooka, Y.; Horio, T.; Hoshide, S.; Ikeda, S.; Ishimitsu, T.; et al. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2019). Hypertens. Res. 2019, 42, 1235–1481. [Google Scholar] [CrossRef] [PubMed]
- Du, D.D.; Yoshinaga, M.; Sonoda, M.; Kawakubo, K.; Uehara, Y. Blood pressure reduction by Japanese traditional Miso is associated with increased diuresis and natriuresis through dopamine system in Dahl salt-sensitive rats. Clin. Exp. Hypertens. 2014, 36, 359–366. [Google Scholar] [CrossRef]
- Lim, P.O.; MacFadyen, R.J.; Struthers, A.D. Is there a role for renin profiling in selecting chronic heart failure patients for ACE inhibitor treatment? Heart 2000, 83, 257–261. [Google Scholar] [CrossRef] [Green Version]
- Filipowicz, E.; Staszków, M. Leki moczopedne [Diuretics]. Wiad. Lek. 2013, 66, 319–323. [Google Scholar]
- Kanda, A.; Hoshiyama, Y.; Kawaguchi, T. Association of lifestyle parameters with the prevention of hypertension in elderly Japanese men and women: A four-year follow-up of normotensive subjects. Asia Pac. J. Public Health 1999, 11, 77–81. [Google Scholar] [CrossRef]
- Manzoni, M.S.; Rossi, E.A.; Carlos, I.Z.; Vendramini, R.C.; Duarte, A.C.; Dâmaso, A.R. Fermented soy product supplemented with isoflavones affected fat depots in juvenile rats. Nutrition 2005, 21, 1018–1024. [Google Scholar] [CrossRef]
- Okouchi, R.; Sakanoi, Y.; Tsuduki, T. Miso (Fermented Soybean Paste) Suppresses Visceral Fat Accumulation in Mice, Especially in Combination with Exercise. Nutrients 2019, 11, 560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, F.; Hashimoto, Y.; Kaji, A.; Sakai, R.; Kawate, Y.; Okamura, T.; Kitagawa, N.; Okada, H.; Nakanishi, N.; Majima, S.; et al. Habitual Miso (Fermented Soybean Paste) Consumption Is Associated with a Low Prevalence of Sarcopenia in Patients with Type 2 Diabetes: A Cross-Sectional Study. Nutrients 2020, 13, 72. [Google Scholar] [CrossRef]
- Sakai, R.; Hashimoto, Y.; Ushigome, E.; Miki, A.; Okamura, T.; Matsugasumi, M.; Fukuda, T.; Majima, S.; Matsumoto, S.; Senmaru, T.; et al. Late-night-dinner is associated with poor glycemic control in people with type 2 diabetes: The KAMOGAWA-DM cohort study. Endocr. J. 2018, 65, 395–402. [Google Scholar] [CrossRef] [Green Version]
- Murakami, K.; Sasaki, S.; Takahashi, Y.; Okubo, H.; Hosoi, Y.; Horiguchi, H.; Oguma, E.; Kayama, F. Dietary glycemic index and load in relation to metabolic risk factors in Japanese female farmers with traditional dietary habits. Am. J. Clin. Nutr. 2006, 83, 1161–1169. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.J.; Pramyothin, P.; Karastergiou, K.; Fried, S.K. Deconstructing the roles of glucocorticoids in adipose tissue biology and the development of central obesity. Biochim. Biophys. Acta 2014, 1842, 473–481. [Google Scholar] [CrossRef] [Green Version]
- Carretero, O.A.; Oparil, S. Essential hypertension. Part I: Definition and etiology. Circulation 2000, 101, 329–335. [Google Scholar] [CrossRef]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A.; et al. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef]
- Antunes, M.V.; Wagner, S.C.; Camargo, J.L.; Linden, R. Standardization of method for determining glycosylated hemoglobin (Hb A1c) by cation exchange high performance liquid chromatography. Braz. J. Pharm. Sci. 2009, 45, 651–657. [Google Scholar] [CrossRef]
- Kaji, A.; Hashimoto, Y.; Kobayashi, Y.; Sakai, R.; Okamura, T.; Miki, A.; Hamaguchi, M.; Kuwahata, M.; Yamazaki, M.; Fukui, M. Sarcopenia is associated with tongue pressure in older patients with type 2 diabetes: A cross-sectional study of the KAMOGAWA-DM cohort study. Geriatr. Gerontol. Int. 2019, 19, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Lemmens, H.J.; Brodsky, J.B.; Bernstein, D.P. Estimating ideal body weight--A new formula. Obes. Surg. 2005, 15, 1082–1083. [Google Scholar] [CrossRef]
- Yoshimura, Y.; Wakabayashi, H.; Nagano, F.; Bise, T.; Shimazu, S.; Kudo, M.; Shiraishi, A. Sarcopenic Obesity Is Associated with Activities of Daily Living and Home Discharge in Post-Acute Rehabilitation. J. Am. Med. Dir. Assoc. 2020, 21, 1475–1480. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Murakami, K.; Sasaki, S.; Okubo, H.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Comparison of relative validity of food group intakes estimated by comprehensive and brief-type self-administered diet history questionnaires against 16 d dietary records in Japanese adults. Public Health Nutr. 2011, 14, 1200–1211. [Google Scholar] [CrossRef] [PubMed]
- Kaji, A.; Hashimoto, Y.; Sakai, R.; Okada, H.; Hamaguchi, M.; Ushigome, E.; Majima, S.; Yamazaki, M.; Fukui, M. Frequent Usage of Convenience Stores is Associated with Low Diet Quality. Nutrients 2019, 11, 1212. [Google Scholar] [CrossRef] [Green Version]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [Green Version]
- Fonseca-Alaniz, M.H.; Brito, L.C.; Borges-Silva, C.N.; Takada, J.; Andreotti, S.; Lima, F.B. High dietary sodium intake increases white adipose tissue mass and plasma leptin in rats. Obesity 2007, 15, 2200–2208. [Google Scholar] [CrossRef] [PubMed]
- Fonseca-Alaniz, M.H.; Takada, J.; Andreotti, S.; de Campos, T.B.; Campaña, A.B.; Borges-Silva, C.N.; Lima, F.B. High sodium intake enhances insulin-stimulated glucose uptake in rat epididymal adipose tissue. Obesity 2008, 16, 1186–1192. [Google Scholar] [CrossRef] [PubMed]
- Gruzdeva, O.; Borodkina, D.; Uchasova, E.; Dyleva, Y.; Barbarash, O. Leptin resistance: Underlying mechanisms and diagnosis. Diabetes Metab. Syndr. Obes. 2019, 12, 191–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogihara, T.; Asano, T.; Ando, K.; Chiba, Y.; Sekine, N.; Sakoda, H.; Anai, M.; Onishi, Y.; Fujishiro, M.; Ono, H.; et al. Insulin resistance with enhanced insulin signaling in high-salt diet-fed rats. Diabetes 2001, 50, 573–583. [Google Scholar] [CrossRef] [Green Version]
- Jin, G.; Xu, M.; Zou, M.; Duan, S. The Processing, Gene Regulation, Biological Functions, and Clinical Relevance of N4-Acetylcytidine on RNA: A Systematic Review. Mol. Ther. Nucleic Acids. 2020, 20, 13–24. [Google Scholar] [CrossRef]
- Zheng, S.; Zhao, T.; Yuan, S.; Yang, L.; Ding, J.; Cui, L.; Xu, M. Immunodeficiency Promotes Adaptive Alterations of Host Gut Microbiome: An Observational Metagenomic Study in Mice. Front. Microbiol. 2019, 10, 2415. [Google Scholar] [CrossRef]
- Tanaka, M.; Itoh, H. Hypertension as a Metabolic Disorder and the Novel Role of the Gut. Curr. Hypertens. Rep. 2019, 21, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashimoto, Y.; Hamaguchi, M.; Kaji, A.; Sakai, R.; Osaka, T.; Inoue, R.; Kashiwagi, S.; Mizushima, K.; Uchiyama, K.; Takagi, T.; et al. Intake of sucrose affects gut dysbiosis in patients with type 2 diabetes. J. Diabetes Investig. 2020, 11, 1623–1634. [Google Scholar] [CrossRef]
- Messerli, F.H.; Hofstetter, L.; Syrogiannouli, L.; Rexhaj, E.; Siontis, G.; Seiler, C.; Bangalore, S. Sodium intake, life expectancy, and all-cause mortality. Eur. Heart J. 2020, 21, 2103–2112. [Google Scholar]
- Takenaka, T.; Murayama, T.; Furusho, T.; Takenaka, Y. Antihypertensive effects of nicotianamine from soybean broth in spontaneously hypertensive rats. Food Sci. Technol. Res. 2009, 15, 541–546. [Google Scholar] [CrossRef]
- Tomari, H.S.; Uchikawa, M.; Yamazaki, A.; Hirabayashi, S.; Yamakawa, S.; Kitagawa, M.; Yamada, M.; Itou, S.; Yamamoto, T.; Uehara, Y. Newly manufactured Marukome MK-34-1 miso with angiotensin-converting enzyme inhibitory activity and its antihypertensive effects in genetic hypertensive rat models. Hypertens. Res. 2019, 42, 790–800. [Google Scholar] [CrossRef] [Green Version]
- Dougher, C.E.; Rifkin, D.E.; Anderson, C.A.; Smits, G.; Persky, M.S.; Block, G.A.; Ix, J.H. Spot urine sodium measurements do not accurately estimate dietary sodium intake in chronic kidney disease. Am. J. Clin. Nutr. 2016, 104, 298–305. [Google Scholar] [CrossRef] [Green Version]
- Kelly, C.; Geaney, F.; Fitzgerald, A.P.; Browne, G.M.; Perry, I.J. Validation of diet and urinary excretion derived estimates of sodium excretion against 24-h urine excretion in a worksite sample. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 771–779. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Cooper, R.; McKeever, J.; McKeever, P.; Byington, R.; Soltero, I.; Stamler, R.; Gosch, F.; Stevens, E.; Stamler, J. Assessment of the association between habitual salt intake and high blood pressure: Methodological problems. Am. J. Epidemiol. 1979, 110, 219–226. [Google Scholar] [CrossRef]
- Wang, X.; Fang, X.; Zheng, W.; Zhou, J.; Song, Z.; Xu, M.; Min, J.; Wang, F. Genetic support of a causal relationship between iron status and type 2 diabetes: A Mendelian randomization study. J. Clin. Endocrinol. Metab. 2021, dgab454. [Google Scholar] [CrossRef]
- Zhang, F.; Baranova, A.; Zhou, C.; Cao, H.; Chen, J.; Zhang, X.; Xu, M. Causal influences of neuroticism on mental health and cardiovascular disease. Hum. Genet. 2021, 140, 1267–1281. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Rao, S.; Cao, H.; Zhang, X.; Wang, Q.; Xu, Y.; Sun, J.; Wang, C.; Chen, J.; Xu, X.; et al. Genetic evidence suggests posttraumatic stress disorder as a subtype of major depressive disorder. J. Clin. Investig. 2021, 145942. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | All n = 300 |
|---|---|
| Sex (men/women) | 163/137 |
| Age (years) | 65.7 (10.7) |
| Duration of diabetes (years) | 13.7 (10.0) |
| Family history of diabetes (−/+) | 160/140 |
| Height (cm) | 161.1 (9.4) |
| Body weight (kg) | 63.5 (12.9) |
| BMI (kg/m2) | 24.5 (4.4) |
| SBP (mmHg) | 133.8 (18.8) |
| DBP (mmHg) | 79.1 (11.1) |
| Antihypertensive drugs (−/+) | 156/144 |
| Presence of hypertension (−/+) | 112/188 |
| Insulin (−/+) | 230/70 |
| Habit of smoking (−/+) | 255/45 |
| Habit of exercise (−/+) | 154/146 |
| HbA1c (%) | 7.4 (1.3) |
| HbA1c (mmol/mol) | 57.3 (13.9) |
| Plasma glucose (mmol/L) | 8.3 (2.8) |
| Triglycerides (mmol/L) | 1.5 (0.9) |
| HDL cholesterol (mmol/L) | 1.6 (0.4) |
| Creatinine (µmol/L) | 70.0 (28.2) |
| eGFR (mL/min/1.73 m2) | 72.0 (18.3) |
| Na (mmol/L) | 139.6 (2.2) |
| K (mmol/L) | 4.4 (0.4) |
| Cl (mmol/L) | 103.2 (2.4) |
| Urinary Creatinine (µmol/L) | 88.9 (56.9) |
| Urinary Na (mmol/L) | 102.4 (47.6) |
| Urinary K (mmol/L) | 46.6 (24.6) |
| Urinary Na/K (mmol/mmol) | 2.7 (1.5) |
| Estimated salt intake (g/day) | 9.4 (2.4) |
| High estimated salt intake (−/+) | 150/150 |
| Body fat mass (kg) | 19.2 (8.6) |
| Percent body fat mass (%) | 29.6 (9.1) |
| Presence of obesity (−/+) | 192/108 |
| Energy intake (kcal/IBW kg/day) | 30.8 (9.8) |
| Protein intake (g/IBW kg/day) | 1.3 (0.5) |
| Fat intake (g/IBW kg/day) | 1.0 (0.4) |
| Carbohydrate intake (g/IBW kg/day) | 3.9 (1.4) |
| Habitual miso consumption (−/+) | 41/259 |
| Alcohol consumption (g/day) | 8.3 (20.7) |
| Habit of drinking alcohol (−/+) | 262/38 |
| High Estimated Salt Intake/Habitual Miso Consumption | (−/−) | (+/−) | (−/+) | (+/+) | p |
|---|---|---|---|---|---|
| n = 23 | n = 18 | n = 127 | n = 132 | ||
| Sex (men/women) | 13/10 | 8/10 | 71/56 | 71/61 | 0.826 |
| Age (years) | 66.9 (14.7) | 65.7 (9.9) | 66.7 (10.4) | 64.5 (10.3) | 0.391 |
| Duration of diabetes (years) | 20.4 (12.1) | 15.1 (8.1) | 13.4 (9.8) | 12.7 (9.6) | 0.006 |
| Family history of diabetes (−/+) | 13/10 | 9/9 | 63/64 | 75/57 | 0.676 |
| Height (cm) | 158.1 (9.7) | 159.4 (8.8) | 161.2 (9.9) | 161.7 (8.8) | 0.336 |
| Body weight (kg) | 62.5 (12.1) | 67.3 (12.8) | 61.1 (12.6) | 65.5 (13.0) ‡ | 0.026 |
| BMI (kg/m2) | 25.0 (4.6) | 26.5 (4.8) | 23.4 (3.8) † | 25.1 (4.6) ‡ | 0.003 |
| SBP (mmHg) | 129.5 (16.3) | 138.6 (21.4) | 133.8 (19.4) | 133.8 (18.4) | 0.503 |
| DBP (mmHg) | 75.0 (10.5) | 77.3 (9.1) | 78.9 (11.2) | 80.3 (11.2) | 0.161 |
| Antihypertensive drugs (−/+) | 9/14 | 6/12 | 71/56 | 70/62 | 0.181 |
| Presence of hypertension (−/+) | 7/16 | 4/14 | 54/73 | 47/85 | 0.278 |
| Insulin (−/+) | 17/6 | 13/5 | 100/27 | 100/32 | 0.882 |
| smoking (−/+) | 19/4 | 16/2 | 107/20 | 113/19 | 0.938 |
| exercise (−/+) | 15/8 | 8/10 | 64/63 | 67/65 | 0.536 |
| HbA1c (%) | 7.8 (1.6) | 7.9 (2.0) | 7.3 (1.2) | 7.3 (1.1) | 0.111 |
| HbA1c (mmol/mol) | 61.5 (17.3) | 63.2 (21.5) | 56.7 (13.4) | 56.4 (12.2) | 0.111 |
| Plasma glucose (mmol/L) | 8.9 (2.9) | 8.8 (4.5) | 8.5 (3.0) | 8.0 (2.2) | 0.243 |
| Triglycerides (mmol/L) | 1.4 (0.8) | 1.5 (0.7) | 1.4 (0.9) | 1.6 (1.0) | 0.468 |
| HDL cholesterol (mmol/L) | 1.5 (0.5) | 1.5 (0.3) | 1.6 (0.4) | 1.5 (0.5) | 0.639 |
| Creatinine (µmol/L) | 73.1 (19.8) | 66.9 (23.2) | 73.6 (37.0) | 66.3 (18.3) | 0.183 |
| eGFR (mL/min/1.73 m2) | 67.7 (18.6) | 74.3 (21.6) | 69.3 (17.1) | 75.0 (18.7) | 0.048 |
| Na (mmol/L) | 139.5 (2.4) | 139.7 (2.7) | 139.4 (2.2) | 139.8 (2.0) | 0.434 |
| K (mmol/L) | 4.4 (0.4) | 4.6 (0.5) | 4.4 (0.4) | 4.4 (0.4) | 0.136 |
| Cl (mmol/L) | 103.0 (2.5) | 102.7 (2.7) | 102.9 (2.5) | 103.5 (2.3) | 0.148 |
| Urinary Creatinine (µmol/L) | 123.6 (52.6) | 50.8 (31.5) * | 117.6 (63.2) † | 60.5 (30.7) *‡ | <0.001 |
| Urinary Na (mmol/L) | 83.9 (37.5) | 97.2 (45.5) | 87.9 (39.6) | 120.3 (50.6) *‡ | <0.001 |
| Urinary K (mmol/L) | 58.8 (33.1) | 30.3 (17.4) * | 54.8 (25.7) † | 38.8 (18.4) *‡ | <0.001 |
| Urinary Na/K (mmol/mmol) | 1.7 (1.0) | 3.6 (1.3) * | 1.9 (1.0) † | 3.5 (1.5) *‡ | <0.001 |
| Estimated salt intake (g/day) | 7.0 (1.5) | 11.3 (2.3) * | 7.5 (1.4) † | 11.3 (1.5) *‡ | <0.001 |
| Body fat mass (kg) | 20.2 (8.6) | 24.4 (9.6) | 16.9 (7.1) † | 20.5 (9.1) ‡ | <0.001 |
| Percent body fat mass (%) | 31.8 (9.5) | 35.6 (8.3) | 27.2 (8.4) † | 30.6 (9.1) ‡ | <0.001 |
| Presence of obesity (−/+) | 15/8 | 4/14 | 94/33 † | 79/53 † | <0.001 |
| Energy intake (kcal/IBW kg/day) | 25.4 (6.7) | 27.9 (12.0) | 31.6 (10.0) * | 31.3 (9.5) * | 0.019 |
| Protein intake (g/IBW kg/day) | 1.1 (0.3) | 1.1 (0.4) | 1.3 (0.5) | 1.3 (0.5) | 0.037 |
| Fat intake (g/IBW kg/day) | 0.9 (0.3) | 1.0 (0.4) | 1.0 (0.4) | 1.0 (0.3) | 0.467 |
| Carbohydrate intake (g/IBW kg/day) | 3.2 (0.9) | 3.5 (2.1) | 3.9 (1.3) | 4.0 (1.4) * | 0.038 |
| Alcohol consumption (g/day) | 1.7 (4.7) | 3.5 (12.8) | 9.8 (20.5) | 8.5 (23.1) | 0.260 |
| Habit of drinking alcohol (−/+) | 23/0 | 17/1 | 108/19 | 114/18 | 0.181 |
| High Estimated Salt Intake/ Habitual Miso Consumption | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| (−/−) | 0.15 (0.04–0.62) | 0.009 | 0.14 (0.03–0.64) | 0.011 | 0.16 (0.03–0.76) | 0.022 |
| (+/−) | ref | - | ref | - | ref | - |
| (−/+) | 0.10 (0.03–0.33) | <0.001 | 0.09 (0.03–0.32) | <0.001 | 0.07 (0.02–0.26) | <0.001 |
| (+/+) | 0.19 (0.06–0.61) | 0.005 | 0.17 (0.05–0.59) | 0.005 | 0.14 (0.04–0.51) | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takahashi, F.; Hashimoto, Y.; Kaji, A.; Sakai, R.; Miki, A.; Kawate, Y.; Okamura, T.; Kitagawa, N.; Okada, H.; Nakanishi, N.; et al. Association of Estimated Salt and Miso Intake with the Prevalence of Obesity in People with Type 2 Diabetes: A Cross-Sectional Study. Nutrients 2021, 13, 3014. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13093014
Takahashi F, Hashimoto Y, Kaji A, Sakai R, Miki A, Kawate Y, Okamura T, Kitagawa N, Okada H, Nakanishi N, et al. Association of Estimated Salt and Miso Intake with the Prevalence of Obesity in People with Type 2 Diabetes: A Cross-Sectional Study. Nutrients. 2021; 13(9):3014. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13093014
Chicago/Turabian StyleTakahashi, Fuyuko, Yoshitaka Hashimoto, Ayumi Kaji, Ryosuke Sakai, Akane Miki, Yuka Kawate, Takuro Okamura, Noriyuki Kitagawa, Hiroshi Okada, Naoko Nakanishi, and et al. 2021. "Association of Estimated Salt and Miso Intake with the Prevalence of Obesity in People with Type 2 Diabetes: A Cross-Sectional Study" Nutrients 13, no. 9: 3014. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13093014