
Incorporating Post-Cessation Weight-Control Coaching into Smoking Cessation Therapy to Reduce Type 2 Diabetes Risk

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Sample Size Estimation
2.3. Anthropometric Indices and Laboratory Tests
2.4. Assignment, Prospective Follow-Up, and Analytic Design
2.5. The FIT2 Program and Post-Program Abstinence
2.6. Usual Care and Control
2.7. Outcome Measures
2.8. Covariates and Confounders
2.9. Statistical Analysis
3. Results
3.1. General Characteristics
3.2. HbA1c Changes
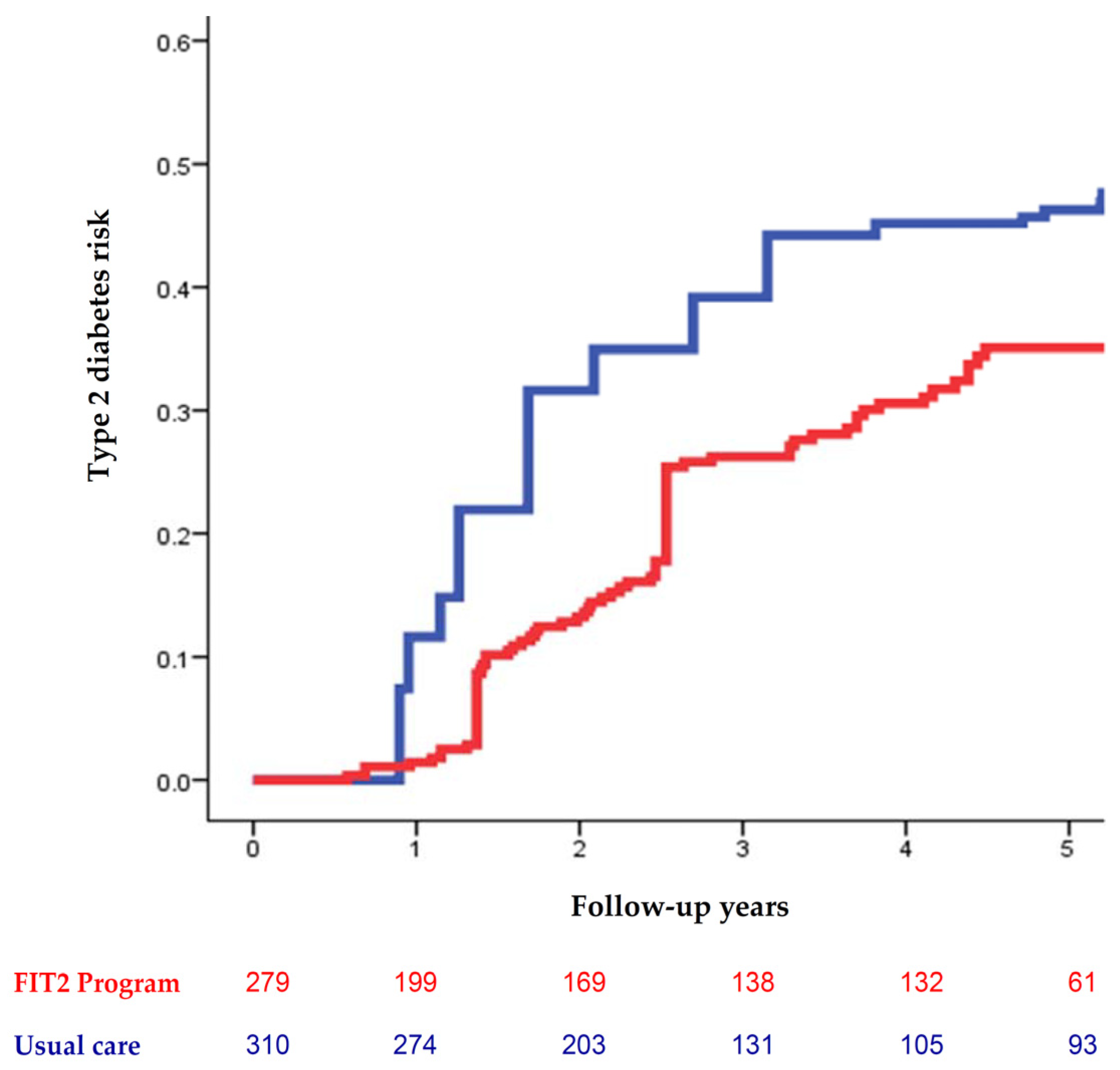
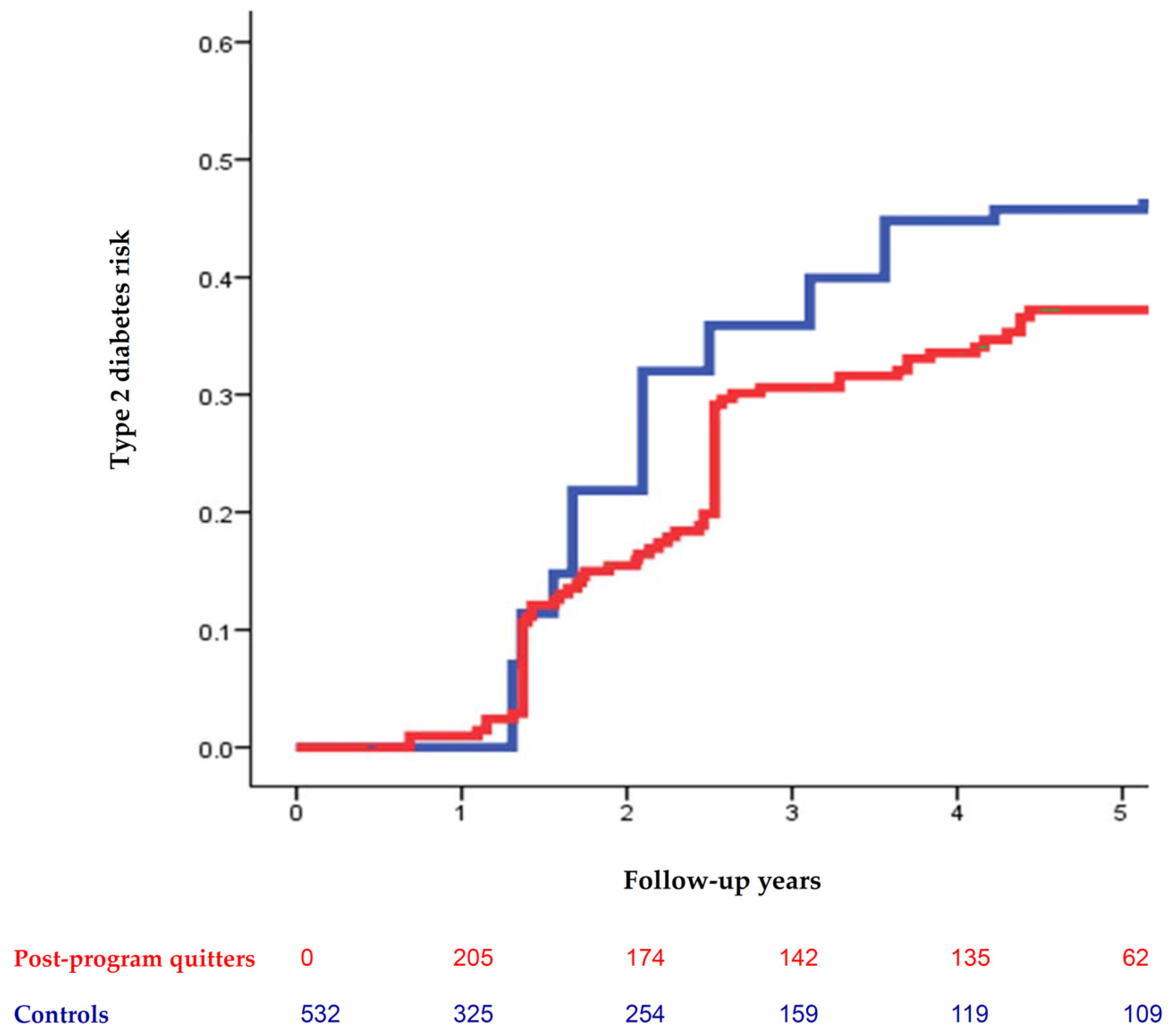
3.3. New-Onset T2D and Regression to Normoglycemia
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chiang, C.H.; Lee, L.T.; Hung, S.H.; Lin, W.Y.; Hung, H.F.; Yang, W.S.; Sung, P.K.; Huang, K.C. Opposite association between diabetes, dyslipidemia, and hepatocellular carcinoma mortality in the middle-aged and elderly. Hepatology 2014, 59, 2207–2215. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.H.; Lu, C.W.; Han, H.C.; Hung, S.H.; Lee, Y.H.; Yang, K.C.; Huang, K.C. The Relationship of Diabetes and Smoking Status to Hepatocellular Carcinoma Mortality. Medicine 2016, 95, e2699. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 10. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44, S125–S150. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 3. Prevention or Delay of Type 2 Diabetes: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44, S34–S39. [Google Scholar] [CrossRef]
- Cloostermans, L.; Wendel-Vos, W.; Doornbos, G.; Howard, B.; Craig, C.L.; Kivimäki, M.; Tabak, A.G.; Jefferis, B.J.; Ronkainen, K.; Brown, W.J.; et al. Independent and combined effects of physical activity and body mass index on the development of Type 2 Diabetes—A meta-analysis of 9 prospective cohort studies. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feldman, A.L.; Long, G.H.; Johansson, I.; Weinehall, L.; Fhärm, E.; Wennberg, P.; Norberg, M.; Griffin, S.J.; Rolandsson, O. Change in lifestyle behaviors and diabetes risk: Evidence from a population-based cohort study with 10 year follow-up. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergman, B.C.; Perreault, L.; Hunerdosse, D.; Kerege, A.; Playdon, M.; Samek, A.M.; Eckel, R.H. Novel and reversible mechanisms of smoking-induced insulin resistance in humans. Diabetes 2012, 61, 3156–3166. [Google Scholar] [CrossRef] [Green Version]
- Siahpush, M.; Singh, G.K.; Tibbits, M.; Pinard, C.A.; Shaikh, R.A.; Yaroch, A. It is better to be a fat ex-smoker than a thin smoker: Findings from the 1997–2004 National Health Interview Survey-National Death Index linkage study. Tob. Control. 2014, 23, 395–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, Y.; Zong, G.; Liu, G.; Wang, M.; Rosner, B.; Pan, A.; Willett, W.C.; Manson, J.E.; Hu, F.B.; Sun, Q. Smoking Cessation, Weight Change, Type 2 Diabetes, and Mortality. N. Engl. J. Med. 2018, 379, 623–632. [Google Scholar] [CrossRef]
- Morimoto, A.; Ohno, Y.; Tatsumi, Y.; Nishigaki, Y.; Maejima, F.; Mizuno, S.; Watanabe, S. Impact of smoking cessation on incidence of diabetes mellitus among overweight or normal-weight Japanese men. Diabetes Res. Clin. Pract. 2012, 96, 407–413. [Google Scholar] [CrossRef]
- Yeh, H.C.; Duncan, B.B.; Schmidt, M.I.; Wang, N.Y.; Brancati, F.L. Smoking, smoking cessation, and risk for type 2 diabetes mellitus: A cohort study. Ann. Intern. Med. 2010, 152, 10–17. [Google Scholar] [CrossRef]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef]
- Bush, T.; Lovejoy, J.C.; Deprey, M.; Carpenter, K.M. The effect of tobacco cessation on weight gain, obesity, and diabetes risk. Obesity 2016, 24, 1834–1841. [Google Scholar] [CrossRef]
- Campagna, D.; Alamo, A.; Di Pino, A.; Russo, C.; Calogero, A.E.; Purrello, F.; Polosa, R. Smoking and diabetes: Dangerous liaisons and confusing relationships. Diabetol. Metab. Syndr. 2019, 11, 85. [Google Scholar] [CrossRef]
- Adams, J.M. Smoking Cessation—Progress, Barriers, and New Opportunities: The Surgeon General’s Report on Smoking Cessation. JAMA 2020, 323, 2470–2471. [Google Scholar] [CrossRef]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44, S15–S33. [Google Scholar] [CrossRef]
- Ma, Y.C.; Zuo, L.; Chen, J.H.; Luo, Q.; Yu, X.Q.; Li, Y.; Xu, J.S.; Huang, S.M.; Wang, L.N.; Huang, W.; et al. Modified glomerular filtration rate estimating equation for Chinese patients with chronic kidney disease. J. Am. Soc. Nephrol. 2006, 17, 2937–2944. [Google Scholar] [CrossRef] [Green Version]
- Krist, A.H.; Davidson, K.W.; Mangione, C.M.; Barry, M.J.; Cabana, M.; Caughey, A.B.; Donahue, K.; Doubeni, C.A.; Epling, J.W., Jr.; Kubik, M.; et al. Interventions for Tobacco Smoking Cessation in Adults, Including Pregnant Persons: US Preventive Services Task Force Recommendation Statement. JAMA 2021, 325, 265–279. [Google Scholar] [CrossRef]
- Hills, A.P.; Emokhtar, N.; Byrne, N.M. Assessment of physical activity and energy expenditure: An overview of objective measures. Front. Nutr. 2014, 1, 5. [Google Scholar] [CrossRef]
- Shintani, A.K.; Girard, T.D.; Eden, S.K.; Arbogast, P.G.; Moons, K.G.; Ely, E.W. Immortal time bias in critical care research: Application of time-varying Cox regression for observational cohort studies. Crit. Care Med. 2009, 37, 2939–2945. [Google Scholar] [CrossRef] [Green Version]
- Farley, A.C.; Hajek, P.; Lycett, D.; Aveyard, P. Interventions for preventing weight gain after smoking cessation. Cochrane Database Syst. Rev. 2012, 1, CD006219. [Google Scholar] [CrossRef] [PubMed]
- Ponciano-Rodriguez, G.; Paez-Martinez, N.; Villa-Romero, A.; Gutierrez-Grobe, Y.; Mendez-Sanchez, N. Early changes in the components of the metabolic syndrome in a group of smokers after tobacco cessation. Metab. Syndr. Relat. Disord. 2014, 12, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Stadler, M.; Tomann, L.; Storka, A.; Wolzt, M.; Peric, S.; Bieglmayer, C.; Pacini, G.; Dickson, S.L.; Brath, H.; Bech, P.; et al. Effects of smoking cessation on beta-cell function, insulin sensitivity, body weight, and appetite. Eur. J. Endocrinol. 2014, 170, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Tian, J.; Venn, A.; Otahal, P.; Gall, S. The association between quitting smoking and weight gain: A systematic review and meta-analysis of prospective cohort studies. Obes. Rev. 2015, 16, 883–901. [Google Scholar] [CrossRef] [PubMed]
- Tong, X.; Chaudhry, Z.; Lee, C.C.; Bone, R.N.; Kanojia, S.; Maddatu, J.; Sohn, P.; Weaver, S.A.; Robertson, M.A.; Petrache, I.; et al. Cigarette smoke exposure impairs β-cell function through activation of oxidative stress and ceramide accumulation. Mol. Metab. 2020, 37, 100975. [Google Scholar] [CrossRef] [PubMed]
- Benowitz, N.L.; Pipe, A.; West, R.; Hays, J.T.; Tonstad, S.; McRae, T.; Lawrence, D.; St Aubin, L.; Anthenelli, R.M. Cardiovascular Safety of Varenicline, Bupropion, and Nicotine Patch in Smokers: A Randomized Clinical Trial. JAMA Intern. Med. 2018, 178, 622–631. [Google Scholar] [CrossRef] [Green Version]
- Aveyard, P.; Raw, M. Improving smoking cessation approaches at the individual level. Tob. Control. 2012, 21, 252–257. [Google Scholar] [CrossRef] [Green Version]
- Maddatu, J.; Anderson-Baucum, E.; Evans-Molina, C. Smoking and the risk of type 2 diabetes. Transl. Res. 2017, 184, 101–107. [Google Scholar] [CrossRef]
- Aubin, H.J.; Farley, A.; Lycett, D.; Lahmek, P.; Aveyard, P. Weight gain in smokers after quitting cigarettes: Meta-analysis. BMJ 2012, 345, e4439. [Google Scholar] [CrossRef] [Green Version]
- Peleg, O.; Cohen, A.; Haimov, I. Depressive symptoms mediate the relationship between sleep disturbances and type 2 diabetes mellitus. J. Diabetes 2020, 12, 305–314. [Google Scholar] [CrossRef]
- Stenvers, D.J.; Scheer, F.; Schrauwen, P.; la Fleur, S.E.; Kalsbeek, A. Circadian clocks and insulin resistance. Nat. Rev. Endocrinol. 2019, 15, 75–89. [Google Scholar] [CrossRef]
- Elwyn, G.; Frosch, D.L.; Kobrin, S. Implementing shared decision-making: Consider all the consequences. Implement. Sci. 2016, 11, 114. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| New-Onset Type 2 Diabetes (217 Cases) | ||
| Unadjusted Analysis | Adjusted Analysis a | |
| Body mass index (kg/m2) | 1.05 (1.02–1.09) ** | 1.10 (1.05–1.16) *** |
| Weight gain at 6 months (kg) | 1.17 (1.07–1.28) *** | 1.19 (1.04–1.35) ** |
| Physically active (vs. inactive) | 0.29 (0.19–0.43) *** | 0.31 (0.20–0.47) *** |
| Depression (vs. no) | 3.58 (2.57–4.98) *** | 2.34 (1.58–3.46) *** |
| FIT2 program (vs. usual care) | 0.64 (0.48–0.84) ** | 0.58 (0.40–0.84) ** |
| Regression to Normoglycemia (68 Cases) | ||
| Unadjusted Analysis | Adjusted Analysis a | |
| Body mass index (kg/m2) | 0.79 (0.73–0.86) *** | 0.88 (0.79–0.97) * |
| Weight gain at 6 months (kg) | 0.67 (0.58–0.77) *** | 0.72 (0.62–0.84) *** |
| Physically active (vs. inactive) | 1.76 (1.08–2.86) * | 0.73 (0.43–1.23) |
| Depression (vs. no) | 0.39 (0.12–1.26) | 0.68 (0.19–2.37) |
| FIT2 program (vs. usual care) | 1.85 (1.13–3.04) * | 1.91 (1.04–3.53) * |
| New-Onset Type 2 Diabetes (217 Cases) | ||
| Unadjusted Analysis | Adjusted Analysis a | |
| Body mass index (kg/m2) | 1.05 (1.02–1.08) ** | 1.10 (1.05–1.15) *** |
| Weight gain at 6 months (kg) | 1.20 (1.10–1.31) *** | 1.28 (1.13–1.45) *** |
| Physically active (vs. inactive) | 0.27 (0.18–0.42) *** | 0.25 (0.15–0.39) *** |
| Depression (vs. no) | 3.13 (2.25–4.36) *** | 1.77 (1.19–2.64) ** |
| Post-program quitters vs. controls | 0.74 (0.56–0.97) * | 0.63 (0.44–0.92) * |
| Regression to Normoglycemia (68 Cases) | ||
| Unadjusted Analysis | Adjusted Analysis a | |
| Body mass index (kg/m2) | 0.73 (0.65–0.82) *** | 0.88 (0.79–0.97) ** |
| Weight gain at 6 months (kg) | 0.64 (0.55–0.73) *** | 0.73 (0.63–0.84) *** |
| Physically active (vs. inactive) | 1.80 (1.09–2.95) * | 0.93 (0.53–1.63) |
| Depression (vs. no) | 0.41 (0.15–1.15) | 0.62 (0.20–1.93) |
| Post-program quitters vs. controls | 1.67 (1.03–2.72) * | 1.83 (1.01–3.30) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiang, C.-H.; Sheu, Y.-H.; Guo, F.-R.; Lin, W.-W.; Chen, G.-R.; Huang, K.-C. Incorporating Post-Cessation Weight-Control Coaching into Smoking Cessation Therapy to Reduce Type 2 Diabetes Risk. Nutrients 2021, 13, 3360. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13103360
Chiang C-H, Sheu Y-H, Guo F-R, Lin W-W, Chen G-R, Huang K-C. Incorporating Post-Cessation Weight-Control Coaching into Smoking Cessation Therapy to Reduce Type 2 Diabetes Risk. Nutrients. 2021; 13(10):3360. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13103360
Chicago/Turabian StyleChiang, Chien-Hsieh, Yi-Han Sheu, Fei-Ran Guo, Wan-Wan Lin, Guan-Ru Chen, and Kuo-Chin Huang. 2021. "Incorporating Post-Cessation Weight-Control Coaching into Smoking Cessation Therapy to Reduce Type 2 Diabetes Risk" Nutrients 13, no. 10: 3360. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13103360