
Ultra-Processed Foods and Nutritional Dietary Profile: A Meta-Analysis of Nationally Representative Samples

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
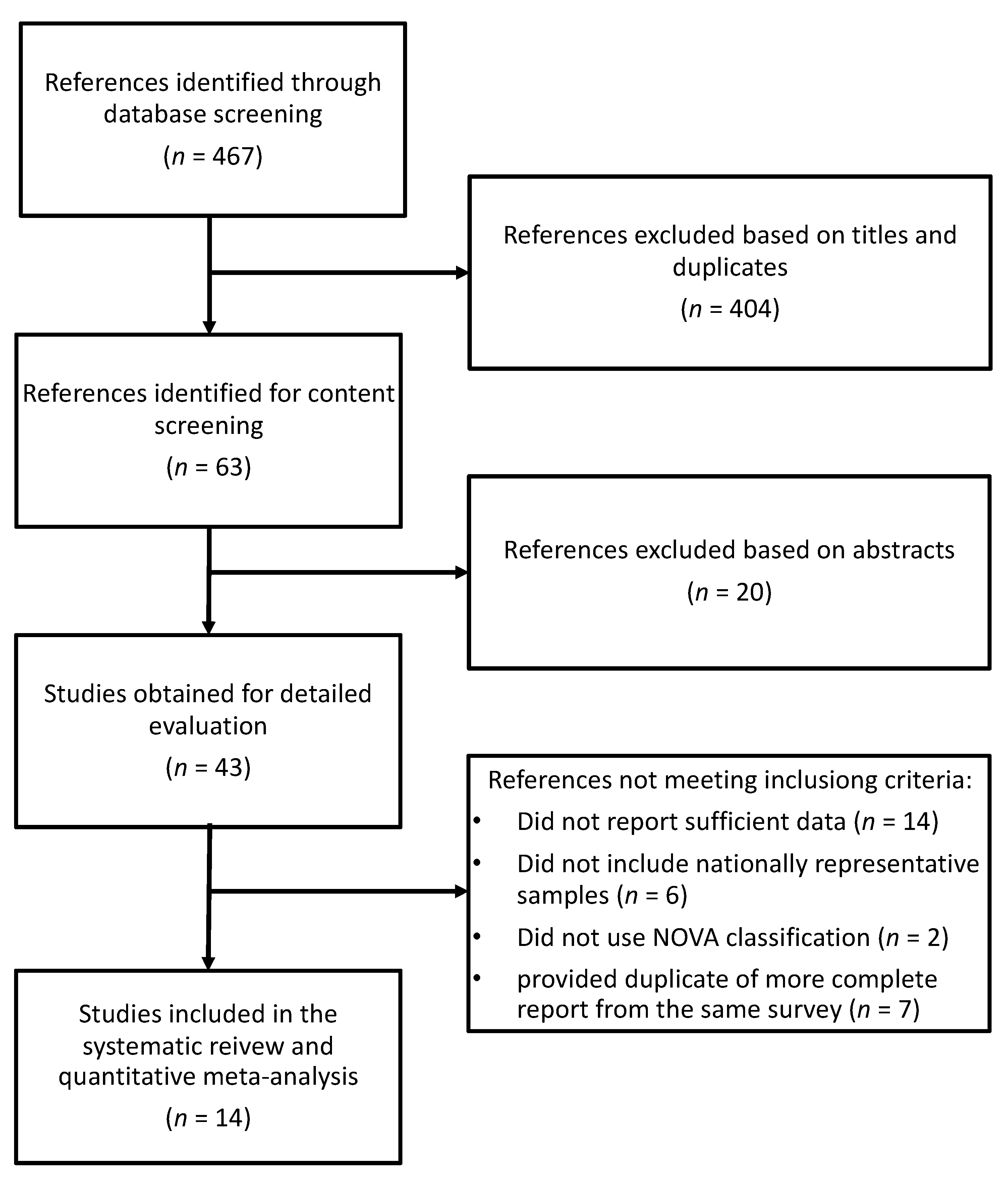
2.1. Study Selection
2.2. Data Extraction
2.3. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Study Characteristics and UPF Consumption
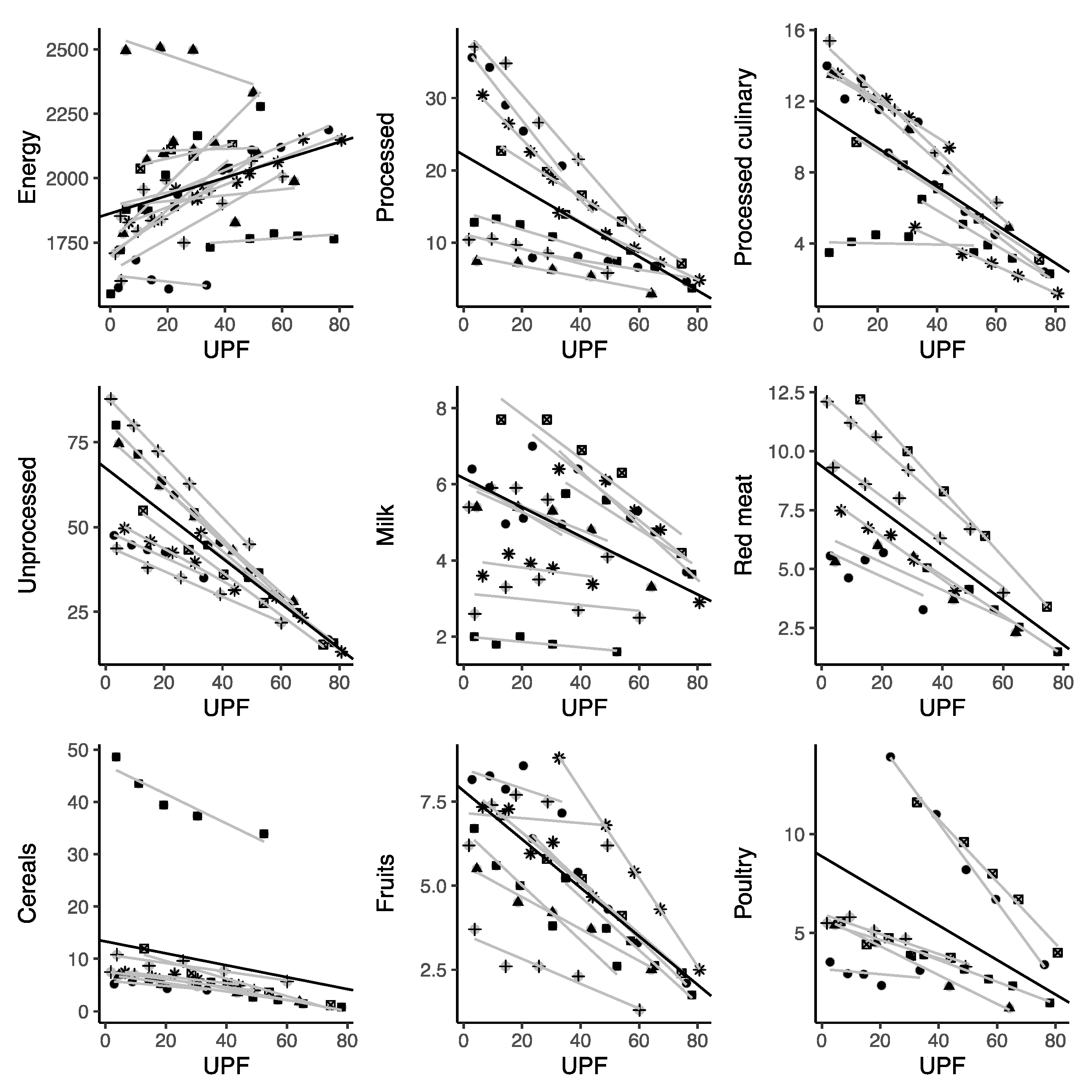
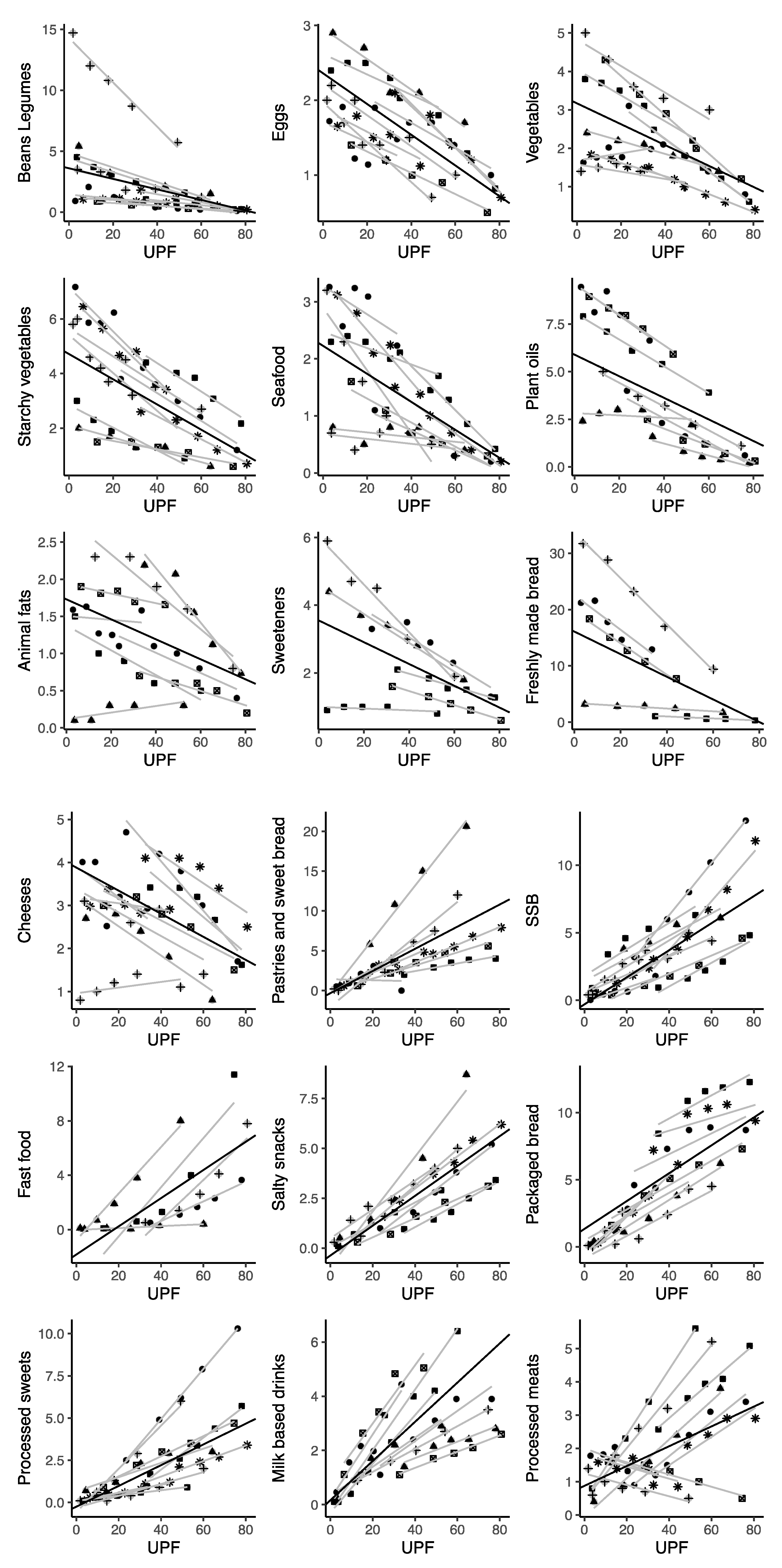
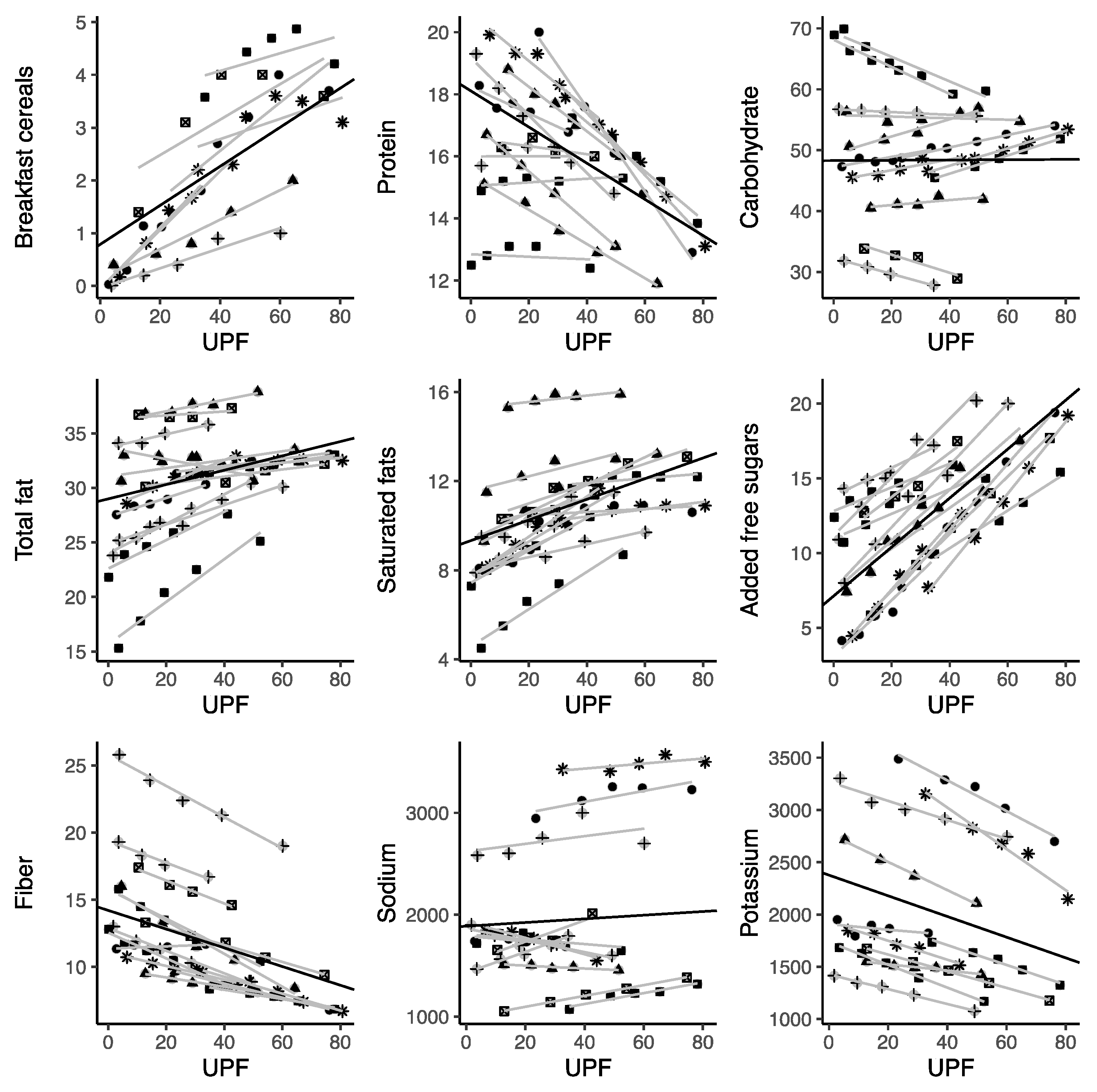
3.3. Correlation with Dietary and Nutritional Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- GBD 2017 Risk Factor Collaborators. Global, Regional, and National Comparative Risk Assessment of 84 Behavioural, Environmental and Occupational, and Metabolic Risks or Clusters of Risks for 195 Countries and Territories, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994. [Google Scholar] [CrossRef] [Green Version]
- GBD 2019 Risk Factors Collaborators. Global Burden of 87 Risk Factors in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Angelino, D.; Godos, J.; Ghelfi, F.; Tieri, M.; Titta, L.; Lafranconi, A.; Marventano, S.; Alonzo, E.; Gambera, A.; Sciacca, S.; et al. Fruit and Vegetable Consumption and Health Outcomes: An Umbrella Review of Observational Studies. Int. J. Food Sci. Nutr. 2019, 70, 652–667. [Google Scholar] [CrossRef]
- Veronese, N.; Solmi, M.; Caruso, M.G.; Giannelli, G.; Osella, A.R.; Evangelou, E.; Maggi, S.; Fontana, L.; Stubbs, B.; Tzoulaki, I. Dietary Fiber and Health Outcomes: An Umbrella Review of Systematic Reviews and Meta-Analyses. Am. J. Clin. Nutr. 2018, 107, 436–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tieri, M.; Ghelfi, F.; Vitale, M.; Vetrani, C.; Marventano, S.; Lafranconi, A.; Godos, J.; Titta, L.; Gambera, A.; Alonzo, E.; et al. Whole Grain Consumption and Human Health: An Umbrella Review of Observational Studies. Int. J. Food Sci. Nutr. 2020, 71, 668–677. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Hoffmann, G.; Missbach, B.; Stelmach-Mardas, M.; Boeing, H. An Umbrella Review of Nuts Intake and Risk of Cardiovascular Disease. Curr. Pharm. Des. 2017, 23, 1016–1027. [Google Scholar] [CrossRef] [PubMed]
- Martini, D.; Godos, J.; Marventano, S.; Tieri, M.; Ghelfi, F.; Titta, L.; Lafranconi, A.; Trigueiro, H.; Gambera, A.; Alonzo, E.; et al. Nut and Legume Consumption and Human Health: An Umbrella Review of Observational Studies. Int. J. Food Sci. Nutr. 2021, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Gibney, M.J.; Forde, C.G.; Mullally, D.; Gibney, E.R. Ultra-Processed Foods in Human Health: A Critical Appraisal. [Commentary]. Am. J. Clin. Nutr. 2017, 106, 717–724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moubarac, J.-C.; Parra, D.C.; Cannon, G.; Monteiro, C.A. Food Classification Systems Based on Food Processing: Significance and Implications for Policies and Actions: A Systematic Literature Review and Assessment. Curr. Obes. Rep. 2014, 3, 256–272. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A.; Cannon, G.; Levy, R.B.; Moubarac, J.-C.; Louzada, M.L.; Rauber, F.; Khandpur, N.; Cediel, G.; Neri, D.; Martinez-Steele, E.; et al. Ultra-Processed Foods: What They Are and How to Identify Them. Public Health Nutr. 2019, 22, 936–941. [Google Scholar] [CrossRef]
- Baker, P.; Machado, P.; Santos, T.; Sievert, K.; Backholer, K.; Hadjikakou, M.; Russell, C.; Huse, O.; Bell, C.; Scrinis, G.; et al. Ultra-Processed Foods and the Nutrition Transition: Global, Regional and National Trends, Food Systems Transformations and Political Economy Drivers. Obes. Rev. 2020, 21, e13126. [Google Scholar] [CrossRef]
- Kac, G.; Pérez-Escamilla, R. Nutrition Transition and Obesity Prevention through the Life-Course. Int. J. Obes. Suppl. 2013, 3, S6–S8. [Google Scholar] [CrossRef]
- Popkin, B.M. Relationship between Shifts in Food System Dynamics and Acceleration of the Global Nutrition Transition. Nutr. Rev. 2017, 75, 73–82. [Google Scholar] [CrossRef] [Green Version]
- Costa, C.S.; Del-Ponte, B.; Assunção, M.C.F.; Santos, I.S. Consumption of Ultra-Processed Foods and Body Fat during Childhood and Adolescence: A Systematic Review. Public Health Nutr. 2018, 21, 148–159. [Google Scholar] [CrossRef] [Green Version]
- Silva Meneguelli, T.; Viana Hinkelmann, J.; Hermsdorff, H.H.M.; Zulet, M.Á.; Martínez, J.A.; Bressan, J. Food Consumption by Degree of Processing and Cardiometabolic Risk: A Systematic Review. Int. J. Food Sci. Nutr. 2020, 71, 678–692. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Zhang, Z.; Yang, H.; Qiu, P.; Wang, H.; Wang, F.; Zhao, Q.; Fang, J.; Nie, J. Consumption of Ultra-Processed Foods and Health Outcomes: A Systematic Review of Epidemiological Studies. Nutr. J. 2020, 19, 86. [Google Scholar] [CrossRef] [PubMed]
- Lane, M.M.; Davis, J.A.; Beattie, S.; Gómez-Donoso, C.; Loughman, A.; O’Neil, A.; Jacka, F.; Berk, M.; Page, R.; Marx, W.; et al. Ultraprocessed Food and Chronic Noncommunicable Diseases: A Systematic Review and Meta-Analysis of 43 Observational Studies. Obes. Rev. 2021, 22, e13146. [Google Scholar] [CrossRef] [PubMed]
- Fardet, A. Characterization of the Degree of Food Processing in Relation with Its Health Potential and Effects. Adv. Food Nutr. Res. 2018, 85, 79–129. [Google Scholar] [CrossRef] [PubMed]
- Poti, J.M.; Braga, B.; Qin, B. Ultra-Processed Food Intake and Obesity: What Really Matters for Health-Processing or Nutrient Content? Curr. Obes. Rep. 2017, 6, 420–431. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Becker, B.J.; Wu, M.-J. The Synthesis of Regression Slopes in Meta-Analysis. Stat. Sci. 2007, 22, 414–429. [Google Scholar] [CrossRef]
- Costa Louzada, M.L.; Martins, A.P.B.; Canella, D.S.; Baraldi, L.G.; Levy, R.B.; Claro, R.M.; Moubarac, J.-C.; Cannon, G.; Monteiro, C.A. Ultra-Processed Foods and the Nutritional Dietary Profile in Brazil. Rev. Saude Publica 2015, 49, 38. [Google Scholar] [CrossRef] [PubMed]
- Louzada, M.L.D.C.; Martins, A.P.B.; Canella, D.S.; Baraldi, L.G.; Levy, R.B.; Claro, R.M.; Moubarac, J.-C.; Cannon, G.; Monteiro, C.A. Impact of Ultra-Processed Foods on Micronutrient Content in the Brazilian Diet. Rev. Saude Publica 2015, 49, 45. [Google Scholar] [CrossRef] [PubMed]
- Moubarac, J.-C.; Batal, M.; Louzada, M.L.; Martinez Steele, E.; Monteiro, C.A. Consumption of Ultra-Processed Foods Predicts Diet Quality in Canada. Appetite 2017, 108, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Martínez Steele, E.; Popkin, B.M.; Swinburn, B.; Monteiro, C.A. The Share of Ultra-Processed Foods and the Overall Nutritional Quality of Diets in the US: Evidence from a Nationally Representative Cross-Sectional Study. Popul. Health Metr. 2017, 15, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.-C.; Huang, Y.-C.; Lo, Y.-T.C.; Wu, H.-J.; Wahlqvist, M.L.; Lee, M.-S. Secular Trend towards Ultra-Processed Food Consumption and Expenditure Compromises Dietary Quality among Taiwanese Adolescents. Food Nutr. Res. 2018, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rauber, F.; da Costa Louzada, M.L.; Steele, E.M.; Millett, C.; Monteiro, C.A.; Levy, R.B. Ultra-Processed Food Consumption and Chronic Non-Communicable Diseases-Related Dietary Nutrient Profile in the UK (2008−2014). Nutrients 2018, 10, 587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cediel, G.; Reyes, M.; Corvalán, C.; Levy, R.B.; Uauy, R.; Monteiro, C.A. Ultra-Processed Foods Drive to Unhealthy Diets: Evidence from Chile. Public Health Nutr. 2021, 24, 1698–1707. [Google Scholar] [CrossRef] [PubMed]
- Machado, P.P.; Steele, E.M.; Levy, R.B.; Sui, Z.; Rangan, A.; Woods, J.; Gill, T.; Scrinis, G.; Monteiro, C.A. Ultra-Processed Foods and Recommended Intake Levels of Nutrients Linked to Non-Communicable Diseases in Australia: Evidence from a Nationally Representative Cross-Sectional Study. BMJ Open 2019, 9, e029544. [Google Scholar] [CrossRef] [Green Version]
- Marrón-Ponce, J.A.; Flores, M.; Cediel, G.; Monteiro, C.A.; Batis, C. Associations between Consumption of Ultra-Processed Foods and Intake of Nutrients Related to Chronic Non-Communicable Diseases in Mexico. J. Acad. Nutr. Diet. 2019, 119, 1852–1865. [Google Scholar] [CrossRef] [PubMed]
- Parra, D.C.; da Costa-Louzada, M.L.; Moubarac, J.-C.; Bertazzi-Levy, R.; Khandpur, N.; Cediel, G.; Monteiro, C.A. Association between Ultra-Processed Food Consumption and the Nutrient Profile of the Colombian Diet in 2005. Salud Publica Mex. 2019, 61, 147–154. [Google Scholar] [CrossRef] [Green Version]
- Costa de Miranda, R.; Rauber, F.; de Moraes, M.M.; Afonso, C.; Santos, C.; Rodrigues, S.; Levy, R.B. UPPER Group Consumption of Ultra-Processed Foods and Non-Communicable Disease-Related Nutrient Profile in Portuguese Adults and Elderly (2015-2016): The UPPER Project. Br. J. Nutr. 2021, 125, 1177–1187. [Google Scholar] [CrossRef]
- Calixto Andrade, G.; Julia, C.; Deschamps, V.; Srour, B.; Hercberg, S.; Kesse-Guyot, E.; Allès, B.; Chazelas, E.; Deschasaux, M.; Touvier, M.; et al. Consumption of Ultra-Processed Food and Its Association with Sociodemographic Characteristics and Diet Quality in a Representative Sample of French Adults. Nutrients 2021, 13, 682. [Google Scholar] [CrossRef]
- Shim, J.-S.; Shim, S.Y.; Cha, H.-J.; Kim, J.; Kim, H.C. Association between Ultra-Processed Food Consumption and Dietary Intake and Diet Quality in Korean Adults. J. Acad. Nutr. Diet. 2021. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, E.; Esposito, S.; Costanzo, S.; Di Castelnuovo, A.; Cerletti, C.; Donati, M.B.; de Gaetano, G.; Iacoviello, L.; Bonaccio, M. INHES Study Investigators Ultra-Processed Food Consumption and Its Correlates among Italian Children, Adolescents and Adults from the Italian Nutrition & Health Survey (INHES) Cohort Study. Public Health Nutr. 2021, 1–14. [Google Scholar] [CrossRef]
- Weaver, C.M.; Dwyer, J.; Fulgoni, V.L.; King, J.C.; Leveille, G.A.; MacDonald, R.S.; Ordovas, J.; Schnakenberg, D. Processed Foods: Contributions to Nutrition. Am. J. Clin. Nutr. 2014, 99, 1525–1542. [Google Scholar] [CrossRef] [PubMed]
- Medina-Reyes, E.I.; Rodríguez-Ibarra, C.; Déciga-Alcaraz, A.; Díaz-Urbina, D.; Chirino, Y.I.; Pedraza-Chaverri, J. Food Additives Containing Nanoparticles Induce Gastrotoxicity, Hepatotoxicity and Alterations in Animal Behavior: The Unknown Role of Oxidative Stress. Food Chem. Toxicol. 2020, 146, 111814. [Google Scholar] [CrossRef]
- Ronto, R.; Wu, J.H.; Singh, G.M. The Global Nutrition Transition: Trends, Disease Burdens and Policy Interventions. Public Health Nutr. 2018, 21, 2267–2270. [Google Scholar] [CrossRef] [Green Version]
- Imamura, F.; Micha, R.; Khatibzadeh, S.; Fahimi, S.; Shi, P.; Powles, J.; Mozaffarian, D. Global Burden of Diseases Nutrition and Chronic Diseases Expert Group (NutriCoDE) Dietary Quality among Men and Women in 187 Countries in 1990 and 2010: A Systematic Assessment. Lancet Glob. Health 2015, 3, e132–e142. [Google Scholar] [CrossRef] [Green Version]
- GBD 2017 Diet Collaborators. Health Effects of Dietary Risks in 195 Countries, 1990-2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- Martínez Steele, E.; Baraldi, L.G.; Louzada, M.L.D.C.; Moubarac, J.-C.; Mozaffarian, D.; Monteiro, C.A. Ultra-Processed Foods and Added Sugars in the US Diet: Evidence from a Nationally Representative Cross-Sectional Study. BMJ Open 2016, 6, e009892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rauber, F.; Louzada, M.L.D.C.; Martinez Steele, E.; de Rezende, L.F.M.; Millett, C.; Monteiro, C.A.; Levy, R.B. Ultra-Processed Foods and Excessive Free Sugar Intake in the UK: A Nationally Representative Cross-Sectional Study. BMJ Open 2019, 9, e027546. [Google Scholar] [CrossRef] [PubMed]
- Machado, P.P.; Steele, E.M.; Louzada, M.L.D.C.; Levy, R.B.; Rangan, A.; Woods, J.; Gill, T.; Scrinis, G.; Monteiro, C.A. Ultra-Processed Food Consumption Drives Excessive Free Sugar Intake among All Age Groups in Australia. Eur. J. Nutr. 2020, 59, 2783–2792. [Google Scholar] [CrossRef] [PubMed]
- Qin, P.; Li, Q.; Zhao, Y.; Chen, Q.; Sun, X.; Liu, Y.; Li, H.; Wang, T.; Chen, X.; Zhou, Q.; et al. Sugar and Artificially Sweetened Beverages and Risk of Obesity, Type 2 Diabetes Mellitus, Hypertension, and All-Cause Mortality: A Dose-Response Meta-Analysis of Prospective Cohort Studies. Eur. J. Epidemiol. 2020, 35, 655–671. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.M.; Micha, R.; Khatibzadeh, S.; Lim, S.; Ezzati, M.; Mozaffarian, D.; Global Burden of Diseases Nutrition and Chronic Diseases Expert Group (NutriCoDE). Estimated Global, Regional, and National Disease Burdens Related to Sugar-Sweetened Beverage Consumption in 2010. Circulation 2015, 132, 639–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popkin, B.M.; Barquera, S.; Corvalan, C.; Hofman, K.J.; Monteiro, C.; Ng, S.W.; Swart, E.C.; Taillie, L.S. Towards Unified and Impactful Policies to Reduce Ultra-Processed Food Consumption and Promote Healthier Eating. Lancet Diabetes Endocrinol. 2021. [Google Scholar] [CrossRef]
- Marino, M.; Puppo, F.; Del Bo’, C.; Vinelli, V.; Riso, P.; Porrini, M.; Martini, D. A Systematic Review of Worldwide Consumption of Ultra-Processed Foods: Findings and Criticisms. Nutrients 2021, 13, 2778. [Google Scholar] [CrossRef] [PubMed]
- Cattafesta, M.; Petarli, G.B.; Zandonade, E.; Bezerra, O.M.P.A.; Abreu, S.M.R.D.; Salaroli, L.B. Energy Contribution of NOVA Food Groups and the Nutritional Profile of the Brazilian Rural Workers’ Diets. PLoS ONE 2020, 15, e0240756. [Google Scholar] [CrossRef]
- Cornwell, B.; Villamor, E.; Mora-Plazas, M.; Marin, C.; Monteiro, C.A.; Baylin, A. Processed and Ultra-Processed Foods Are Associated with Lower-Quality Nutrient Profiles in Children from Colombia-CORRIGENDUM. Public Health Nutr. 2018, 21, 254. [Google Scholar] [CrossRef] [Green Version]
- Batal, M.; Johnson-Down, L.; Moubarac, J.-C.; Ing, A.; Fediuk, K.; Sadik, T.; Tikhonov, C.; Chan, L.; Willows, N. Quantifying Associations of the Dietary Share of Ultra-Processed Foods with Overall Diet Quality in First Nations Peoples in the Canadian Provinces of British Columbia, Alberta, Manitoba and Ontario. Public Health Nutr. 2018, 21, 103–113. [Google Scholar] [CrossRef] [Green Version]
- Batal, M.; Johnson-Down, L.; Moubarac, J.-C.; Ing, A.; Fediuk, K.; Sadik, T.; Chan, H.M.; Willows, N. Sociodemographic Associations of the Dietary Proportion of Ultra-Processed Foods in First Nations Peoples in the Canadian Provinces of British Columbia, Manitoba, Alberta and Ontario. Int. J. Food Sci. Nutr. 2018, 69, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Koiwai, K.; Takemi, Y.; Hayashi, F.; Ogata, H.; Matsumoto, S.; Ozawa, K.; Machado, P.P.; Monteiro, C.A. Consumption of Ultra-Processed Foods Decreases the Quality of the Overall Diet of Middle-Aged Japanese Adults. Public Health Nutr. 2019, 22, 2999–3008. [Google Scholar] [CrossRef]
- Bonaccio, M.; Di Castelnuovo, A.; Costanzo, S.; De Curtis, A.; Persichillo, M.; Sofi, F.; Cerletti, C.; Donati, M.B.; de Gaetano, G.; Iacoviello, L. Ultra-Processed Food Consumption Is Associated with Increased Risk of All-Cause and Cardiovascular Mortality in the Moli-Sani Study. Am. J. Clin. Nutr. 2021, 113, 446–455. [Google Scholar] [CrossRef] [PubMed]
- Rico-Campà, A.; Martínez-González, M.A.; Alvarez-Alvarez, I.; Mendonça, R.D.; de la Fuente-Arrillaga, C.; Gómez-Donoso, C.; Bes-Rastrollo, M. Association between Consumption of Ultra-Processed Foods and All Cause Mortality: SUN Prospective Cohort Study. BMJ 2019, 365, l1949. [Google Scholar] [CrossRef] [Green Version]
- Beslay, M.; Srour, B.; Méjean, C.; Allès, B.; Fiolet, T.; Debras, C.; Chazelas, E.; Deschasaux, M.; Wendeu-Foyet, M.G.; Hercberg, S.; et al. Ultra-Processed Food Intake in Association with BMI Change and Risk of Overweight and Obesity: A Prospective Analysis of the French NutriNet-Santé Cohort. PLoS Med. 2020, 17, e1003256. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Survey Name | Country | Years | Number; Sex | Age | Dietary Assessment | %E UPFs, (Mean) | Lowest Quintile%E UPFs (Mean) | Upper Quintile%E UPFs (Mean) |
|---|---|---|---|---|---|---|---|---|---|
| Shim, 2021 [34] | Korea National Health and Nutrition Examination Survey (KNHANES) | Korea | 2016–2018 | 16,657; 49.7% females | 19+ years old | 24-h dietary recall | 25.1 | 3.6 | 52.4 |
| Ruggiero, 2021 [35] | Italian Nutrition & HEalth Survey (INHES) | Italy | 2010–2013 | 9078 | 5–97 years old | 24-h dietary recall | 17.8 | 4.0 | 35.0 |
| Costa de Miranda, 2021 [32] | National Food, Nutrition and Physical Activity Survey (IAN-AF) | Portugal | 2015–2016 | 3852 (3102 adults, 750 elderly) | 18–64 or 65+ years old | two 24-h dietary recalls | 24.0 | 6.5 | 44.1 |
| Calixto Andrade, 2021 [33] | Étude Nationale Nutrition Santé Survey (ENNS) | France | 2006–2007 | 2642; 63.3% females | 18–74 years old | three 24-h dietary recalls | 31.1 | 12.8 | 51.5 |
| Parra, 2019 [31] | National Nutrition Survey and the Demographic and Health National Survey of Colombia (ENDS) | Colombia | 2004–2005 | 38,643; 51.9% females | 2–64 years | 24-h dietary recall | 15.9 | 0.2 | 41.1 |
| Marron-Ponce, 2019 [30] | Mexican National Health and Nutrition Survey | Mexico | 2012 | 10,087; 50.5% females | 1 year or older (50% adults aged 20 to 59 years) | 24-h dietary recall | 30.0 | 4.5 | 64.2 |
| Machado, 2019 [29] | National Nutrition and Physical Activity Survey (NNPAS) | Australia | 2011–2012 | 12,153 | 2+ years old | two 24-h dietary recalls | 42.0 | 12.8 | 74.5 |
| Cediel, 2021 [28] | National Dietary Survey in Chile (ENCA) | Chile | 2010 | 4920 | 2+ years old | 24-h dietary recall | 28.6 | 3.8 | 60.1 |
| Rauber, 2018 [27] | UK National Diet and Nutrition Survey (NDNS) | United Kingdom | 2008–2014 | 9364 (4729 adults and 4635 children) | 1.5 year or older | 4-day diary | 56.8 | 34.9 | 78.1 |
| Chen, 2018 [26] | Nutrition and Health Surveys in Taiwan (NAHSIT) | Taiwan | 1993–1996, 2011 | 2062 | 16–18 years old | 24-h dietary recall | 19.5 | 5.4 | 49.8 |
| Martinez Steele, 2017 [25] | National Health and Nutrition Examination Survey (NHANES) | United States | 2009–2010 | 9317 | 1+ years old | two 24-h dietary recalls | 57.5 | 32.6 | 80.7 |
| Moubarac, 2017 [24] | Canadian Community Health Survey (CCHS) | Canada | 2004 | 33,694; 46,5% females | 2+ years old (55,1% aged 2–18 years) | two 24-h dietary recalls | 47.7 | 23.5 | 76.2 |
| Costa Louzada, 2015 [22]; Louzada, 2015 [23] | Brazilian Family Budgets Survey (POF) | Brazil | 2008–2009 | 32,898 | 10+ years old | two 24-h dietary records | 21.5 | 1.8 | 49.2 |
| Variable | Datasets (Studies) | Estimates (95% CI) in Categories of UPF Contribution | p for Slope | |||
|---|---|---|---|---|---|---|
| Ultra-Processed Foods (%) | 15% UPF | 50% UPF | 75% UPF | Slope | ||
| Sugar-sweetened beverages (%) | 10 (9) | 1.20 (0.44; 1.96) | 4.70 (3.43; 5.97) | 7.21 (5.30; 9.11) | 0.10 (0.07; 0.13) | 0.001 |
| Packaged bread (%) | 9 (8) | 2.89 (1.27; 4.51) | 6.52 (5.07; 7.96) | 9.11 (7.55; 10.67) | 0.10 (0.08; 0.13) | <0.001 |
| Processed sweets (%) | 10 (9) | 0.67 (0.35; 1.00) | 2.83 (1.64; 4.01) | 4.36 (2.48; 6.24) | 0.06 (0.03; 0.09) | <0.001 |
| Milk-based drinks (%) | 9 (8) | 1.25 (0.90; 1.59) | 3.78 (2.59; 4.97) | 5.59 (3.77; 7.41) | 0.07 (0.05; 0.10) | 0.037 |
| Processed meats (%) | 10 (9) | 1.32 (1.02; 1.63) | 2.36 (1.34; 3.38) | 3.11 (1.41; 4.81) | 0.03 (0.00; 0.06) | <0.001 |
| Breakfast cereals (%) | 8 (7) | 1.34 (0.65; 2.04) | 2.64 (1.91; 3.36) | 3.56 (2.69; 4.43) | 0.04 (0.03; 0.05) | <0.001 |
| Fast food (%) | 5 (5) | 0.00 (0.00; 1.16) | 3.35 (0.67; 6.02) | 5.94 (1.86; 10.01) | 0.10 (0.04; 0.17) | 0.001 |
| Salty snacks (%) | 8 (8) | 0.75 (0.28; 1.22) | 3.37 (2.48; 4.26) | 5.24 (3.98; 6.50) | 0.07 (0.06; 0.09) | <0.001 |
| Cookies, pastries, and sweet bread (%) | 8 (7) | 1.76 (0.89; 2.63) | 6.63 (3.47; 9.80) | 10.12 (5.28; 14.95) | 0.14 (0.07; 0.21) | <0.001 |
| Sweeteners (%) | 6 (6) | 3.07 (1.86; 4.28) | 1.95 (1.32; 2.57) | 1.14 (0.86; 1.43) | −0.03 (−0.05; −0.01) | <0.001 |
| Unpackaged freshly made bread (%) | 5 (4) | 13.08 (3.51; 22.65) | 6.05 (1.73; 10.38) | 1.04 (−0.42; 2.49) | −0.20 (−0.35; −0.05) | 0.010 |
| Unprocessed foods (%) | 10 (9) | 57.41 (49.98; 64.83) | 34.12 (30.55; 37.69) | 17.49 (16.27; 18.71) | −0.67 (−0.78; −0.55) | <0.001 |
| Red meat (%) | 7 (6) | 7.94 (6.02; 9.86) | 4.62 (3.40; 5.84) | 2.25 (1.48; 3.02) | −0.09 (−0.12; −0.07) | <0.001 |
| Poultry (%) | 7 (6) | 7.57 (3.71; 11.43) | 4.52 (2.27; 6.76) | 2.33 (1.09; 3.58) | −0.09 (−0.14; −0.04) | <0.001 |
| Cereals (%) | 8 (7) | 11.65 (2.85; 20.46) | 7.67 (0.65; 14.68) | 4.82 (−0.98; 10.62) | −0.11 (−0.17; −0.06) | <0.001 |
| Milk (%) | 10 (9) | 5.59 (4.29; 6.89) | 4.26 (3.35; 5.16) | 3.30 (2.65; 3.95) | −0.04 (−0.05; −0.03) | <0.001 |
| Fruits (%) | 10 (9) | 6.74 (5.41; 8.07) | 4.22 (3.29; 5.15) | 2.42 (1.59; 3.24) | −0.07 (−0.09; −0.05) | <0.001 |
| Starchy vegetables (%) | 10 (9) | 4.02 (2.97; 5.08) | 2.41 (1.72; 3.10) | 1.25 (0.76; 1.75) | −0.05 (−0.06; −0.03) | <0.001 |
| Vegetables (%) | 10 (9) | 2.76 (2.09; 3.43) | 1.81 (1.41; 2.21) | 1.13 (0.77; 1.49) | −0.03 (−0.04; −0.02) | <0.001 |
| Eggs (%) | 10 (9) | 2.05 (1.74; 2.37) | 1.33 (1.05; 1.62) | 0.82 (0.52; 1.12) | −0.02 (−0.02; −0.02) | <0.001 |
| Seafood (%) | 10 (9) | 1.86 (1.34; 2.38) | 1.00 (0.69; 1.32) | 0.39 (0.07; 0.71) | −0.02 (−0.03; −0.02) | <0.001 |
| Beans and legumes (%) | 10 (9) | 2.95 (0.95; 4.94) | 1.43 (0.52; 2.35) | 0.35 (0.19; 0.51) | −0.04 (−0.07; −0.01) | 0.006 |
| Processed culinary ingredients (%) | 9 (8) | 9.90 (7.81; 11.98) | 6.13 (4.85; 7.40) | 3.44 (2.48; 4.39) | −0.11 (−0.14; −0.08) | <0.001 |
| Added free sugars (%) | 14 (12) | 9.58 (7.61; 11.56) | 15.31 (13.85; 16.78) | 19.41 (17.94; 20.87) | 0.16 (0.13; 0.19) | <0.001 |
| Plant oils (%) | 8 (7) | 5.04 (3.28; 6.81) | 3.06 (1.77; 4.35) | 1.64 (0.65; 2.64) | −0.06 (−0.07; −0.04) | <0.001 |
| Animal fats (%) | 8 (7) | 1.53 (0.92; 2.14) | 1.06 (0.67; 1.44) | 0.72 (0.41; 1.04) | −0.01 (−0.02; 0.00) | 0.002 |
| Processed foods (%) | 10 (9) | 18.60 (13.01; 24.19) | 10.39 (7.92; 12.86) | 4.52 (3.37; 5.67) | −0.23 (−0.33; −0.14) | <0.001 |
| Cheeses (%) | 9 (8) | 3.48 (2.59; 4.37) | 2.54 (1.96; 3.11) | 1.87 (1.37; 2.37) | −0.03 (−0.04; −0.01) | <0.001 |
| Variable | Datasets (Studies) | Estimates (95% CI) in Categories of UPF Contribution | p for Slope | |||
|---|---|---|---|---|---|---|
| Ultra-Processed Foods (%) | 15% UPF | 50% UPF | 75% UPF | Slope | ||
| Energy (kcal) | 14 (12) | 1915.25 (1804.35; 2026.15) | 2036.70 (1934.50; 2138.90) | 2123.45 (2000.51; 2246.38) | 3.47 (1.47; 5.47) | <0.001 |
| Nutrients | ||||||
| Protein (%) | 13 (11) | 17.23 (15.95; 18.51) | 15.19 (14.38; 16.01) | 13.74 (12.84; 14.64) | −0.06 (−0.08; −0.03) | <0.001 |
| Carbohydrate (%) | 13 (11) | 48.29 (42.46; 54.12) | 48.37 (42.65; 54.09) | 48.43 (42.12; 54.74) | 0.00 (−0.07; 0.08) | 0.949 |
| Total fat (%) | 15 (13) | 29.97 (27.58; 32.36) | 32.27 (30.55; 33.98) | 33.91 (32.41; 35.41) | 0.07 (0.04; 0.10) | <0.001 |
| Saturated fats (%) | 15 (13) | 10.03 (8.94; 11.11) | 11.65 (10.79; 12.50) | 12.81 (11.95; 13.66) | 0.05 (0.03; 0.06) | <0.001 |
| Trans fats (%) | 3 (3) | 0.70 (0.08; 1.33) | 0.96 (−0.05; 1.98) | 1.14 (−0.15; 2.44) | 0.01 (0.00; 0.02) | 0.211 |
| Fiber (g/1000 kcal) | 14 (12) | 13.16 (11.00; 15.33) | 10.73 (8.89; 12.57) | 8.99 (7.26; 10.72) | −0.07 (−0.09; −0.05) | <0.001 |
| Micronutrients | ||||||
| Sodium (mg/1000 kcal) | 12 (10) | 1914.70 (1504.16; 2325.23) | 1977.65 (1551.45; 2403.84) | 2022.61 (1566.01; 2479.21) | 1.80 (−1.62; 5.21) | 0.302 |
| Potassium (mg/1000 kcal) | 11 (10) | 2228.24 (1735.90; 2720.58) | 1881.86 (1456.07; 2307.65) | 1634.45 (1248.90; 2019.99) | −9.90 (−12.60; −7.19) | <0.001 |
| Iron (mg/1000 kcal) | 4 (4) | 10.09 (4.22; 15.95) | 9.04 (4.42; 13.66) | 8.30 (4.53; 12.06) | −0.03 (−0.07; 0.01) | 0.120 |
| Magnesium (mg/1000 kcal) | 4 (4) | 200.63 (141.17; 260.09) | 161.53 (113.10; 209.96) | 133.60 (92.75; 174.46) | −1.12 (−1.46; −0.78) | <0.001 |
| Calcium (mg/1000 kcal) | 5 (5) | 433.84 (299.41; 568.26) | 401.01 (299.50; 502.52) | 377.57 (294.55; 460.58) | −0.94 (−2.13; 0.26) | 0.123 |
| Vitamin A (μg/1000 kcal) | 5 (5) | 431.11 (232.39; 629.83) | 332.65 (221.80; 443.50) | 262.32 (203.20; 321.43) | −2.81 (−5.48; −0.15) | 0.038 |
| Vitamin C (mg/1000 kcal) | 5 (5) | 79.17 (47.78; 110.57) | 66.79 (39.07; 94.52) | 57.95 (32.05; 83.85) | −0.35 (−0.55; −0.16) | <0.001 |
| Vitamin D (μg/1000 kcal) | 4 (4) | 3.73 (2.25; 5.21) | 2.81 (1.75; 3.86) | 2.14 (1.39; 2.90) | −0.03 (−0.04; −0.01) | <0.001 |
| Zinc (mg/1000 kcal) | 3 (3) | 6.60 (6.12; 7.08) | 5.46 (5.01; 5.91) | 4.64 (4.10; 5.19) | −0.03 (−0.04; −0.02) | <0.001 |
| Phosphorus (mg/1000 kcal) | 4 (4) | 666.55 (527.35; 805.76) | 582.91 (475.76; 690.07) | 523.17 (436.17; 610.17) | −2.39 (−3.46; −1.32) | <0.001 |
| Vitamin E (mg/1000 kcal) | 3 (3) | 5.41 (1.12; 9.69) | 4.68 (0.99; 8.37) | 4.16 (0.89; 7.43) | −0.02 (−0.04; 0.00) | 0.016 |
| Vitamin B12 (μg/1000 kcal) | 3 (3) | 3.78 (2.10; 5.45) | 2.95 (1.33; 4.57) | 2.36 (0.77; 3.95) | −0.02 (−0.03; −0.02) | <0.001 |
| Thiamin (mg/1000 kcal) | 3 (3) | 1.06 (0.49; 1.63) | 0.93 (0.65; 1.21) | 0.84 (0.76; 0.93) | 0.00 (−0.01; 0.00) | 0.406 |
| Riboflavin (mg/1000 kcal) | 3 (3) | 1.18 (0.84; 1.53) | 1.07 (0.79; 1.35) | 0.99 (0.72; 1.26) | 0.00 (−0.01; 0.00) | 0.074 |
| Niacin (mg/1000 kcal) | 4 (4) | 16.97 (9.26; 24.68) | 14.18 (8.38; 19.99) | 12.19 (7.72; 16.65) | −0.08 (−0.14; −0.02) | 0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martini, D.; Godos, J.; Bonaccio, M.; Vitaglione, P.; Grosso, G. Ultra-Processed Foods and Nutritional Dietary Profile: A Meta-Analysis of Nationally Representative Samples. Nutrients 2021, 13, 3390. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13103390
Martini D, Godos J, Bonaccio M, Vitaglione P, Grosso G. Ultra-Processed Foods and Nutritional Dietary Profile: A Meta-Analysis of Nationally Representative Samples. Nutrients. 2021; 13(10):3390. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13103390
Chicago/Turabian StyleMartini, Daniela, Justyna Godos, Marialaura Bonaccio, Paola Vitaglione, and Giuseppe Grosso. 2021. "Ultra-Processed Foods and Nutritional Dietary Profile: A Meta-Analysis of Nationally Representative Samples" Nutrients 13, no. 10: 3390. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13103390