
Sex-Specific Mediation Effects of Workplace Bullying on Associations between Employees’ Weight Status and Psychological Health Impairments

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment and Sample
2.2. Measures
2.3. Data Analytics Plan
3. Results
3.1. Weight- and Sex-Specific Differences in Experiences of Workplace Bullying
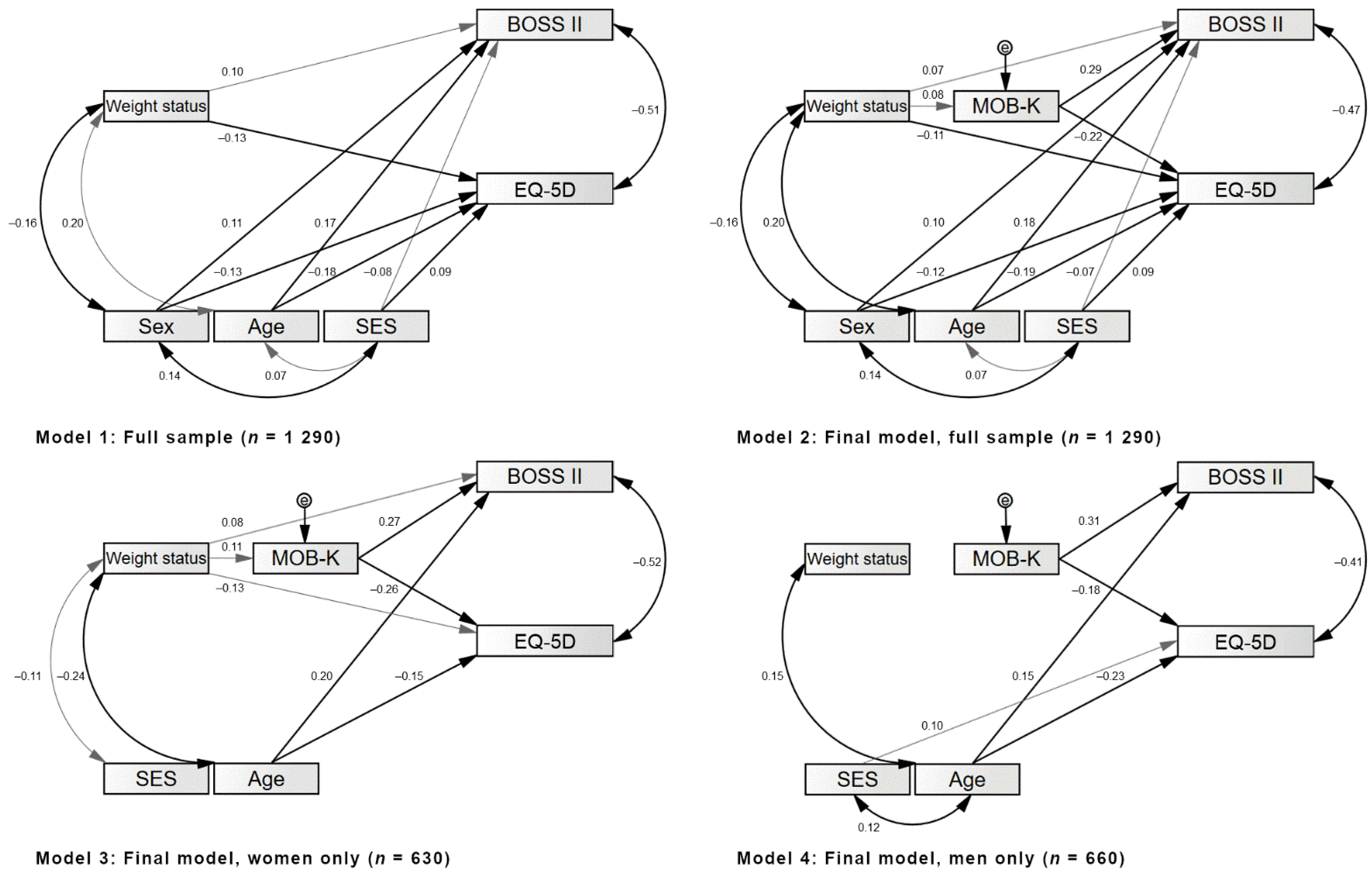
3.2. Associations of Weight Status and Experiences of Workplace Bullying with Psychological Health Impairments
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metabolism 2019, 92, 6–10. [Google Scholar] [CrossRef] [Green Version]
- Afshin, A.; Sur, P.J.; Fay, K.A.; Cornaby, L.; Ferrara, G.; Salama, J.S.; Mullany, E.C.; Abate, K.H.; Abbafati, C.; Abebe, Z.; et al. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- Gakidou, E.; Afshin, A.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulle, A.M.; Abera, S.F.; Aboyans, V.; et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1345–1422. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Obesity and Overweight; World Health Organization: Geneva, Switzerland, 2016; Available online: https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 27 October 2021).
- Corrigan, P.; Bink, A. The Stigma of Mental Illness. In Encyclopedia of Mental Health, 2nd ed.; Elsevier: Amsterdam, The Netherlands, 2016; pp. 230–234. [Google Scholar] [CrossRef]
- Puhl, R.; Suh, Y. Stigma and Eating and Weight Disorders. Curr. Psychiatry Rep. 2015, 17, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Giel, K.E.; Thiel, A.; Teufel, M.; Mayer, J.; Zipfel, S. Weight Bias in Work Settings—A Qualitative Review. Obes. Facts 2010, 3, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Roehling, M.V.; Pichler, S.; Bruce, T.A. Moderators of the effect of weight on job-related outcomes: A meta-analysis of experimental studies. J. Appl. Soc. Psychol. 2013, 43, 237–252. [Google Scholar] [CrossRef]
- Gillen, P.A.; Sinclair, M.; Kernohan, W.G.; Begley, C.M.; Luyben, A.G. Interventions for prevention of bullying in the workplace. Cochrane Database Syst. Rev. 2017, 1, 1465–1858. [Google Scholar] [CrossRef]
- Sliter, K.A.; Sliter, M.T.; Withrow, S.A.; Jex, S.M. Employee adiposity and incivility: Establishing a link and identifying demographic moderators and negative consequences. J. Occup. Health Psychol. 2012, 17, 409–424. [Google Scholar] [CrossRef]
- Vanhove, A.; Gordon, R.A. Weight discrimination in the workplace: A meta-analytic examination of the relationship between weight and work-related outcomes. J. Appl. Soc. Psychol. 2014, 44, 12–22. [Google Scholar] [CrossRef]
- Flint, S.W.; Čadek, M.; Codreanu, S.C.; Ivić, V.; Zomer, C.; Gomoiu, A. Obesity Discrimination in the Recruitment Process: “You’re Not Hired!”. Front. Psychol. 2016, 7, 647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spahlholz, J.; Baer, N.; König, H.-H.; Riedel-Heller, S.G.; Luck-Sikorski, C. Obesity and discrimination—a systematic review and meta-analysis of observational studies. Obes. Rev. 2016, 17, 43–55. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Ahn, R.; Kim, T.H.; Han, E. Impact of Obesity on Employment and Wages among Young Adults: Observational Study with Panel Data. Int. J. Environ. Res. Public Health 2019, 16, 139. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.-K.; Berry, D.C. Impact of weight stigma on physiological and psychological health outcomes for overweight and obese adults: A systematic review. J. Adv. Nurs. 2018, 74, 1030–1042. [Google Scholar] [CrossRef]
- Alshehry, A.S.; Alquwez, N.; Almazan, J.; Namis, I.M.; Moreno-Lacalle, R.C.; Cruz, J.P. Workplace incivility and its influence on professional quality of life among nurses from multicultural background: A cross-sectional study. J. Clin. Nurs. 2019, 28, 2553–2564. [Google Scholar] [CrossRef]
- Viotti, S.; Essenmacher, L.; Hamblin, L.E.; Arnetz, J.E. Testing the reciprocal associations among co-worker incivility, organisational inefficiency, and work-related exhaustion: A one-year, cross-lagged study. Work Stress 2018, 32, 334–356. [Google Scholar] [CrossRef] [Green Version]
- Proper, K.I.; Koppes, L.L.J.; van Zwieten, M.H.J.; Bemelmans, W.J.E. The prevalence of chronic psychological complaints and emotional exhaustion among overweight and obese workers. Int. Arch. Occup. Environ. Health 2012, 85, 537–545. [Google Scholar] [CrossRef]
- Proper, K.I.; Koppes, L.L.; Meijer, S.; Bemelmans, W.J. The Association Between Body Mass Index Status and Sick Leave and the Role of Emotional Exhaustion—A Mediation Analysis Among a Representative Sample of Dutch Employees. J. Occup. Environ. Med. 2013, 55, 1213–1218. [Google Scholar] [CrossRef] [PubMed]
- Aronsson, G.; Theorell, T.; Grape, T.; Hammarström, A.; Hogstedt, C.; Marteinsdottir, I.; Skoog, I.; Träskman-Bendz, L.; Hall, C. A systematic review including meta-analysis of work environment and burnout symptoms. BMC Public Health 2017, 17, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maslach, C.; Leiter, M.P. Burnout and HealthCare–Editorial. Burn. Res. 2014, 1, 57–58. [Google Scholar]
- Zhang, X.; Kuchinke, L.; Woud, M.; Velten, J.; Margraf, J. Survey method matters: Online/offline questionnaires and face-to-face or telephone interviews differ. Comput. Hum. Behav. 2017, 71, 172–180. [Google Scholar] [CrossRef]
- Von der Heyde, C. The ADM-Sampling-System for Face-to-Face Surveys. 2009. Available online: https://www.adm-ev.de/wp-content/uploads/2018/11/Description-ADM-Stichproben-f2f_EN.pdf (accessed on 27 October 2021).
- Pfaff, H.; Bentz, J.; Brähler, E. The “Intensity of Bullying Coming from Co-Workers”-scale (MOB-K): Psychometric evaluation on a representative sample from the general population [Die Skala “Mobbingintensität der Kolleginnen und Kollegen“(MOB-K): Teststatistische Überprüfung an einer repräsentativen Bevölkerungsstichprobe]. Psychosozial 2007, 30, 17–27. [Google Scholar]
- Hagemann, W.; Geuenich, K. Burnout screening scales (BOSS). In Burnout-Screening-Skalen (BOSS); Hogrefe: Göttingen, Germany, 2009. [Google Scholar]
- Hinz, A.; Kohlmann, T.; Stöbel-Richter, Y.; Zenger, M.; Brähler, E. The quality of life questionnaire EQ-5D-5L: Psychometric properties and normative values for the general German population. Qual. Life Res. 2014, 23, 443–447. [Google Scholar] [CrossRef]
- Janssen, M.F.; Pickard, A.S.; Golicki, D.; Gudex, C.; Niewada, M.; Scalone, L.; Swinburn, P.; Busschbach, J. Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: A multi-country study. Qual. Life Res. 2013, 22, 1717–1727. [Google Scholar] [CrossRef] [Green Version]
- Lange, M.; Kamtsiuris, P.; Lange, C.; Rosario, A.S.; Stolzenberg, H.; Lampert, T. Messung soziodemographischer Merkmale im Kinder-und Jugendgesundheitssurvey (KiGGS) und ihre Bedeutung am Beispiel der Einschätzung des allgemeinen Gesundheitszustands. Bundesgesundheitsblatt Gesundh. Gesundh. 2007, 50, 578–589. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, M.; Jensen, R. Common Method Bias in Public Management Studies. Int. Public Manag. J. 2015, 18, 3–30. [Google Scholar] [CrossRef]
- Tehseen, S.; Ramayah, T.; Sajilan, S. Testing and Controlling for Common Method Variance: A Review of Available Methods. J. Manag. Sci. 2017, 4, 142–168. [Google Scholar] [CrossRef]
- Chang, S.-J.; Van Witteloostuijn, A.; Eden, L. Common Method Variance in International Business Research. JIBS Spec. Collect. 2019, 385–398, 385–398. [Google Scholar] [CrossRef]
- Blanca, M.J.; Alarcón, R.; Arnau, J. Non-normal data: Is ANOVA still a valid option? Psicothema 2017, 29, 552–557. [Google Scholar] [CrossRef] [PubMed]
- Schmider, E.; Ziegler, M.; Danay, E.; Beyer, L.; Bühner, M. Is It Really Robust? Methodology 2010, 6, 147–151. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power for the Behavioral Sciences, 2nd ed.; Laurence Erlbaum and Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Hayes, A.F. Beyond Baron and Kenny: Statistical mediation analysis in the new millennium. Commun. Monogr. 2009, 76, 408–420. [Google Scholar] [CrossRef]
- Hayes, A.F. Partial, conditional, and moderated moderated mediation: Quantification, inference, and interpretation. Commun. Monogr. 2018, 85, 4–40. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regession Approach; Guilford Press: New York, NY, USA, 2018; pp. 3–4. [Google Scholar]
- Schermelleh-Engel, K.; Moosbrugger, H.; Müller, H. Evaluating the fit of structural equation models: Tests of significance and descriptive goodness-of-fit measures. MPR-Online 2003, 8, 23–74. [Google Scholar]
- Khubchandani, J.; Price, J.H. Workplace Harassment and Morbidity Among US Adults: Results from the National Health Interview Survey. J. Community Health 2015, 40, 555–563. [Google Scholar] [CrossRef] [PubMed]
- Salvagioni, D.A.J.; Melanda, F.N.; Mesas, A.E.; González, A.D.; Gabani, F.L.; De Andrade, S.M. Physical, psychological and occupational consequences of job burnout: A systematic review of prospective studies. PLoS ONE 2017, 12, e0185781. [Google Scholar] [CrossRef]
- Sliter, M.; Jex, S.; Wolford, K.; McInnerney, J. How rude! Emotional labor as a mediator between customer incivility and employee outcomes. J. Occup. Health Psychol. 2010, 15, 468. [Google Scholar] [CrossRef]
- German Federal Office of Statistics [Statistisches Bundesamt]. Population and Employment. Households and Families. Results of the Microcensus 2017. Subject 1, Series 3 [Bevölkerung und Erwerbstätigkeit. Haushalte und Familien. Ergebnisse des Mikrozensus 2017. Fachserie 1, Reihe 3]. 2018. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bevoelkerung/Haushalte-Familien/Publikationen/Downloads-Haushalte/haushalte-familien-2010300177004.pdf?__blob=publicationFile&v=4 (accessed on 27 October 2021).
- Lampert, T.; Kroll, L.; Müters, S.; Stolzenberg, H. Measurement of socioeconomic status in the German health interview and examination survey for adults (DEGS1). Bundesgesundheitsblatt Gesundh. Gesundh. 2013, 56, 631–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mensink, G.; Schienkiewitz, A.; Haftenberger, M.; Lampert, T.; Ziese, T.; Scheidt-Nave, C. Overweight and obesity in Germany: Results of the German Health Interview and Examination Survey for Adults (DEGS1). Bundesgesundheitsblatt Gesundh. Gesundh. 2013, 56, 131–143. [Google Scholar] [CrossRef] [Green Version]
- Gorber, S.C.; Tremblay, M.; Moher, D.; Gorber, B. A comparison of direct vs. self-report measures for assessing height, weight and body mass index: A systematic review. Obes. Rev. 2007, 8, 307–326. [Google Scholar] [CrossRef]
- Flegal, K.M.; Graubard, B.I.; Ioannidis, J.P.A. Evaluation of a suggested novel method to adjust BMI calculated from self-reported weight and height for measurement error. Obesity 2021, 29, 1700–1707. [Google Scholar] [CrossRef]
- Shiely, F.; Millar, S.R. BMI self-selection: Exploring alternatives to self-reported BMI. Res. Methods Med. Health Sci. 2021, 2, 112–122. [Google Scholar] [CrossRef]
- Salas, X.R.; Alberga, A.S.; Cameron, E.; Estey, L.; Forhan, M.; Kirk, S.; Russell-Mayhew, S.; Sharma, A.M. Addressing weight bias and discrimination: Moving beyond raising awareness to creating change. Obes. Rev. 2017, 18, 1323–1335. [Google Scholar] [CrossRef] [PubMed]
- Täuber, S.; Mulder, L.B.; Flint, S.W. The Impact of Workplace Health Promotion Programs Emphasizing Individual Responsibility on Weight Stigma and Discrimination. Front. Psychol. 2018, 9, 2206. [Google Scholar] [CrossRef]
- Makowski, A.C.; Kim, T.J.; Luck-Sikorski, C.; Knesebeck, O.V.D. Social deprivation, gender and obesity: Multiple stigma? Results of a population survey from Germany. BMJ Open 2019, 9, e023389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luck-Sikorski, C.; Schomerus, G.; Jochum, T.; Riedel-Heller, S.G. Layered stigma? Co-occurring depression and obesity in the public eye. J. Psychosom. Res. 2018, 106, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Puhl, R.M.; Himmelstein, M.S.; Pearl, R.L. Weight stigma as a psychosocial contributor to obesity. Am. Psychol. 2020, 75, 274–289. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Total Sample (n = 1290) | Women (n = 630, 48.8%) | Men (n = 660, 51.2%) | Sex-Specific Differences | ||
|---|---|---|---|---|---|---|
| M (SD) | M (SD) | M (SD) | T | df | p | |
| Age (years) | 43.06 (12.48) | 43.22 (12.21) | 42.91 (12.74) | −0.45 | 1288 | 0.654 |
| BMI (kg/m2) | 24.86 (3.48) | 24.26 (3.65) | 25.44 (3.20) | 6.19 | 1288 | <0.001 |
| n (%) | n (%) | n (%) | χ2 | df | p | |
| Weight status | 70.82 | 2, 1290 | <0.001 | |||
| Normal weight (18.5 ≤ BMI < 25.0 kg/m2) | 714 (55.3) | 417 (66.2) | 297 (45.0) | |||
| Overweight (25.0 ≤ BMI < 30.0 kg/m2) | 494 (38.3) | 168 (26.7) | 326 (49.4) | |||
| Obesity (BMI ≥ 30.0 kg/m2) | 82 (6.4) | 45 (7.1) | 37 (5.6) | |||
| Socioeconomic status (SES) | 86.35 | 2, 1277 | <0.001 | |||
| Low | 312 (24.2) | 84 (13.3) | 228 (34.5) | |||
| Middle | 770 (59.7) | 447 (71.0) | 323 (49.0) | |||
| High | 195 (15.1) | 92 (14.6) | 103 (15.6) | |||
| German Citizenship | 9.89 | 1, 1290 | <0.01 | |||
| Yes | 1226 (95.0) | 611 (97.0) | 615 (93.2) | |||
| No | 64 (5.0) | 19 (3.0) | 45 (6.8) | |||
| M (SD) | M (SD) | M (SD) | T | df | p | |
| Workplace bullying (MOB-K) | 4.76 (1.63) | 4.76 (1.61) | 4.76 (1.64) | −0.07 | 1288 | 0.948 |
| Burnout symptoms (BOSS-II) | 0.50 (0.60) | 0.54 (0.63) | 0.44 (0.57) | −2.93 | 1286 | <0.01 |
| Quality of life (EQ-5D) | 24.08 (1.65) | 23.92 (1.80) | 24.24 (1.49) | 3.50 | 1288 | <0.001 |
| Model Fit Indices | n | χ2 | df | p | CMIN/DF | CFI | RMSEA | TLI | NFI |
|---|---|---|---|---|---|---|---|---|---|
| 1: Weight status only | 1290 | 0.201 | 1 | 0.654 | 0.201 | 1.000 | 0.000 | 1.025 | 1.000 |
| 2: Final Model, total sample | 1290 | 0.889 | 3 | 0.828 | 0.296 | 1.000 | 0.000 | 1.025 | 0.999 |
| 3: Final Model, women only | 630 | 1.232 | 1 | 0.267 | 1.232 | 1.000 | 0.019 | 0.989 | 0.997 |
| 4: Final Model, men only | 660 | 0.116 | 1 | 0.734 | 0.116 | 1.000 | 0.000 | 1.061 | 1.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Puls, H.-C.; Schmidt, R.; Zenger, M.; Kampling, H.; Kruse, J.; Brähler, E.; Hilbert, A. Sex-Specific Mediation Effects of Workplace Bullying on Associations between Employees’ Weight Status and Psychological Health Impairments. Nutrients 2021, 13, 3867. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13113867
Puls H-C, Schmidt R, Zenger M, Kampling H, Kruse J, Brähler E, Hilbert A. Sex-Specific Mediation Effects of Workplace Bullying on Associations between Employees’ Weight Status and Psychological Health Impairments. Nutrients. 2021; 13(11):3867. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13113867
Chicago/Turabian StylePuls, Hans-Christian, Ricarda Schmidt, Markus Zenger, Hanna Kampling, Johannes Kruse, Elmar Brähler, and Anja Hilbert. 2021. "Sex-Specific Mediation Effects of Workplace Bullying on Associations between Employees’ Weight Status and Psychological Health Impairments" Nutrients 13, no. 11: 3867. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13113867