
Psychopathological Symptoms and Well-Being in Overweight and Underweight Adolescents: A Network Analysis

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sampling and Recruitment
2.2. Instruments
2.3. Data Analysis
2.4. Sample Size Considerations and Network Stability/Edge Accuracy Calculations
3. Results
3.1. Sample Description
3.2. Psychopathology and Well-Being of Overweight and Underweight Adolescents
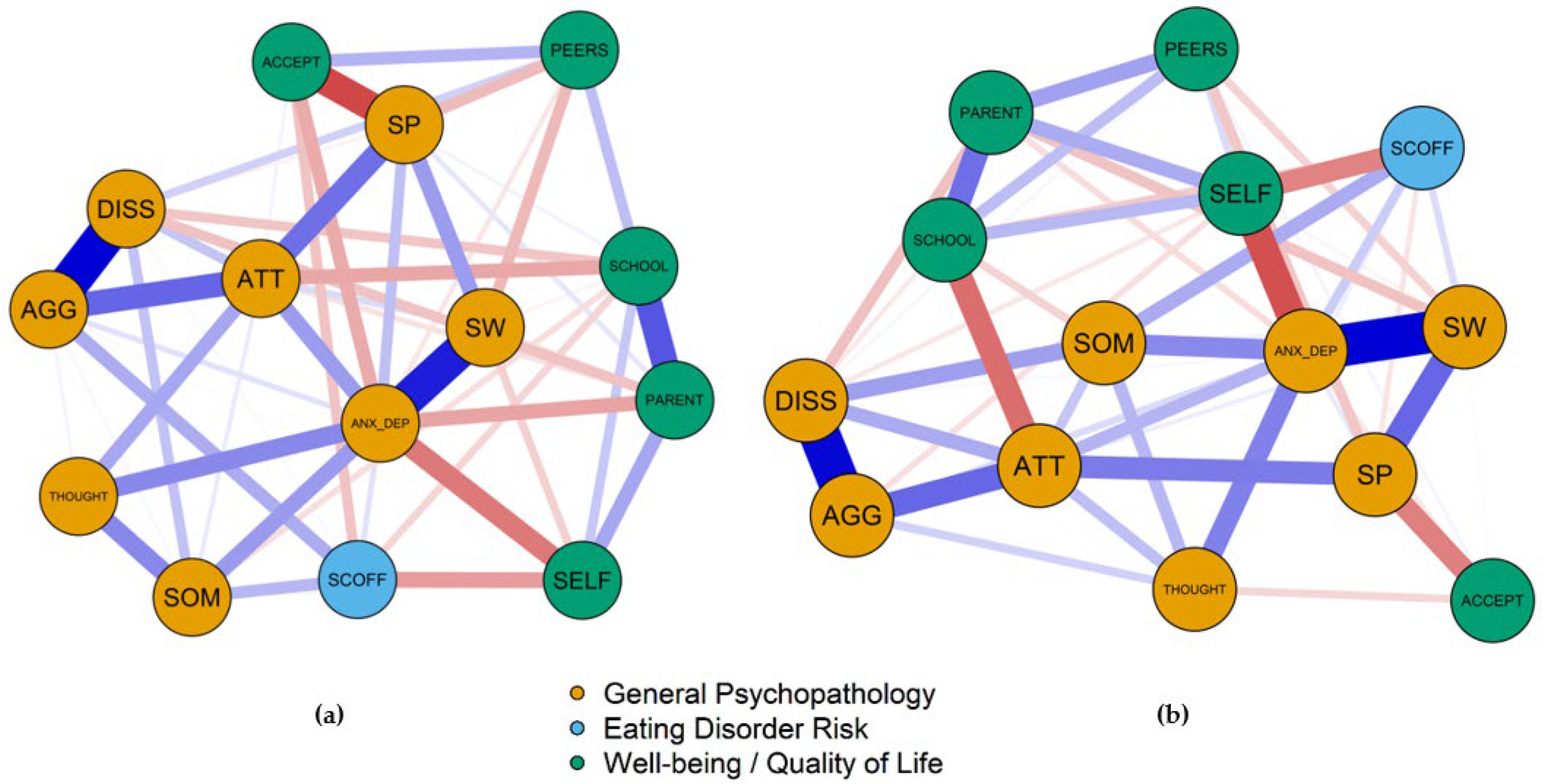
3.3. Results of the Network Analysis
3.3.1. General Network Structure
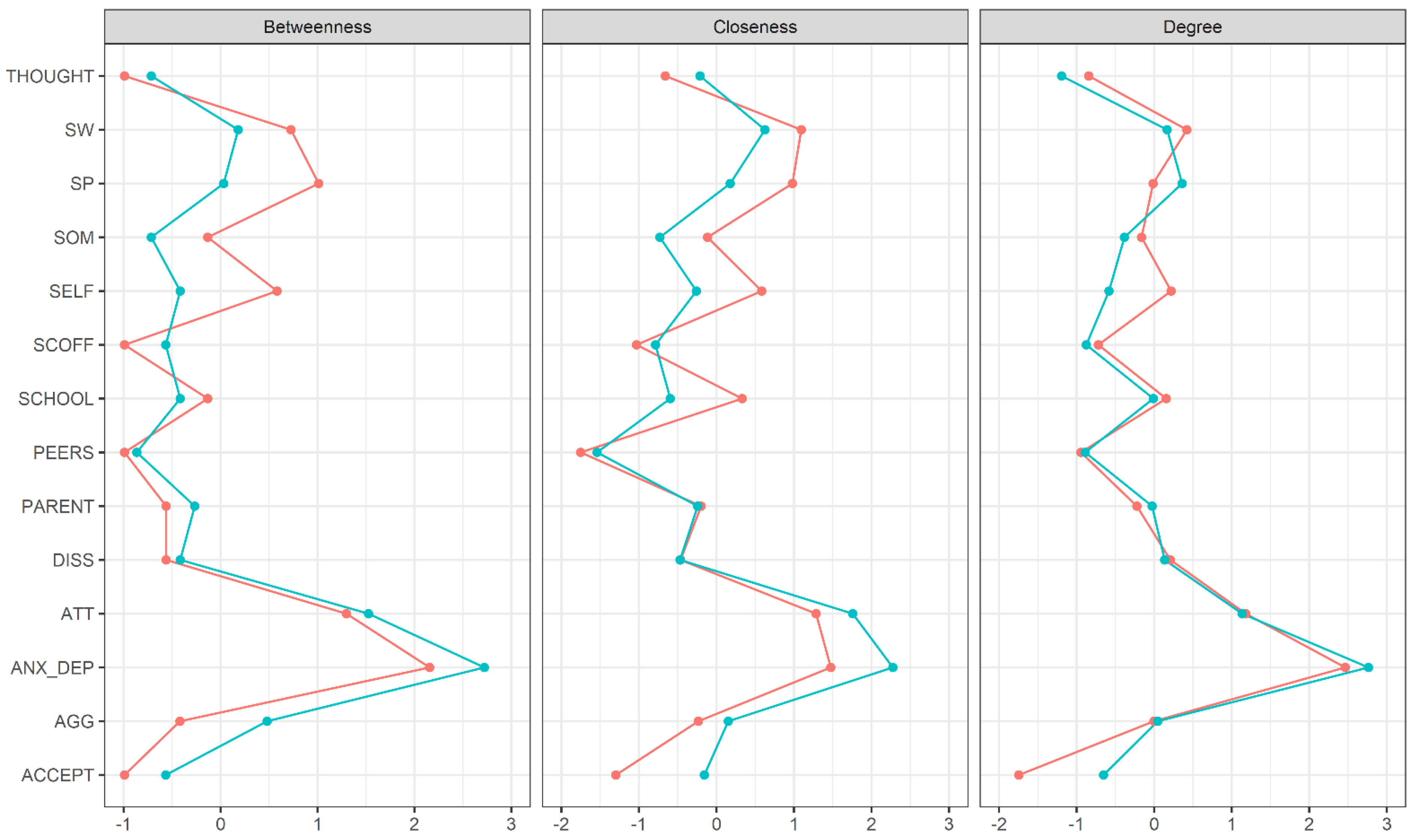
3.3.2. Centrality Indices
3.3.3. Comparison between Overweight and Underweight Adolescents
3.3.4. Stability of Central Indices and Edge Accuracy
3.3.5. Network Structure in Normal Weight Adolescents
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sutaria, S.; Devakumar, D.; Yasuda, S.S.; Das, S.; Saxena, S. Is obesity associated with depression in children? Systematic Review and meta-analysis. Arch. Dis. Child. 2019, 104, 64–74. [Google Scholar] [CrossRef]
- Wang, S.; Sun, Q.; Zhai, L.; Bai, Y.; Wei, W.; Jia, L. The prevalence of depression and anxiety symptoms among overweight/obese and non-overweight/non-obese children/adolescents in China: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2019, 16, 340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanders, R.H.; Han, A.; Baker, J.S.; Cobley, S. Childhood obesity and its physical and psychological co-morbidities: A Systematic review of australian children and adolescents. Eur. J. Pediatr. 2015, 174, 715–746. [Google Scholar] [CrossRef]
- Nujić, D.; Musić Milanović, S.; Milas, V.; Miškulin, I.; Ivić, V.; Milas, J. Association between Child/adolescent overweight/obesity and conduct disorder: A systematic review and meta-analysis. Pediatr. Obes. 2021, 16, e12742. [Google Scholar] [CrossRef] [PubMed]
- Moradi, M.; Mozaffari, H.; Askari, M.; Azadbakht, L. Association between overweight/obesity with depression, anxiety, low self-esteem, and body dissatisfaction in children and adolescents: A systematic review and meta-analysis of observational studies. Crit. Rev. Food Sci. Nutr. 2020, 1–16. [Google Scholar] [CrossRef]
- An, R.; Yan, H.; Shi, X.; Yang, Y. Childhood obesity and school absenteeism: A systematic review and meta-analysis. Obes. Rev. 2017, 18, 1412–1424. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Cai, Z.; Fan, X. Prevalence of binge and loss of control eating among children and adolescents with overweight and obesity: An exploratory meta-analysis. Int. J. Eat. Disord. 2017, 50, 91–103. [Google Scholar] [CrossRef]
- Zeiler, M.; Waldherr, K.; Philipp, J.; Nitsch, M.; Dür, W.; Karwautz, A.; Wagner, G. Prevalence of eating disorder risk and associations with health-related quality of life: Results from a large school-based population screening. Eur. Eat. Disord. Rev. 2016, 24, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Herpertz-Dahlmann, B.; Dempfle, A.; Konrad, K.; Klasen, F.; Ravens-Sieberer, U. The BELLA study group eating disorder symptoms do not just disappear: The implications of adolescent eating-disordered behaviour for body weight and mental health in young adulthood. Eur. Child Adolesc. Psychiatry 2015, 24, 675–684. [Google Scholar] [CrossRef]
- Baile, J.I.; Guevara, R.M.; González-Calderón, M.J.; Urchaga, J.D. The relationship between weight status, health-related quality of life, and life satisfaction in a sample of spanish adolescents. Int. J. Environ. Res. Public. Health 2020, 17, 3106. [Google Scholar] [CrossRef]
- Meixner, L.; Cohrdes, C.; Schienkiewitz, A.; Mensink, G.B.M. Health-related quality of life in children and adolescents with overweight and obesity: Results from the German KIGGS survey. BMC Public Health 2020, 20, 1722. [Google Scholar] [CrossRef]
- Bjornelv, S.; Nordahl, H.M.; Holmen, T.L. Psychological factors and weight problems in adolescents. The role of eating problems, emotional problems, and personality traits: The Young-HUNT study. Soc. Psychiatry Psychiatr. Epidemiol. 2011, 46, 353–362. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira Figueiredo, R.A.; Simola-Ström, S.; Isomaa, R.; Weiderpass, E. Body dissatisfaction and disordered eating symptoms in finnish preadolescents. Eat. Disord. 2019, 27, 34–51. [Google Scholar] [CrossRef] [PubMed]
- Cimino, S.; Cerniglia, L.; Almenara, C.A.; Jezek, S.; Erriu, M.; Tambelli, R. Developmental trajectories of body mass index and emotional-behavioral functioning of underweight children: A longitudinal study. Sci. Rep. 2016, 6, 20211. [Google Scholar] [CrossRef] [PubMed]
- Drosopoulou, G.; Sergentanis, T.N.; Mastorakos, G.; Vlachopapadopoulou, E.; Michalacos, S.; Tzavara, C.; Bacopoulou, F.; Psaltopoulou, T.; Tsitsika, A. Psychosocial health of adolescents in relation to underweight, overweight/obese status: The EU NET ADB survey. Eur. J. Public Health 2021, 31, 379–384. [Google Scholar] [CrossRef]
- Kohlmann, C.-W.; Eschenbeck, H.; Heim-Dreger, U.; Hock, M.; Platt, T.; Ruch, W. Fear of being laughed at in children and adolescents: Exploring the importance of overweight, underweight, and teasing. Front. Psychol. 2018, 9, 1447. [Google Scholar] [CrossRef]
- Jacobs, W.; Merianos, A.L.; Lee Smith, M.; Nabors, L.; Fajayan, A.; Valente, T.W. Examining the role of weight status and Individual attributes on adolescent social relations. J. Adolesc. Health 2020, 67, 108–114. [Google Scholar] [CrossRef]
- Hemmingsson, E. A new model of the role of psychological and emotional distress in promoting obesity: Conceptual review with implications for treatment and prevention. Obes. Rev. 2014, 15, 769–779. [Google Scholar] [CrossRef]
- Krug, I.; Villarejo, C.; Jiménez-Murcia, S.; Perpiñá, C.; Vilarrasa, N.; Granero, R.; Cebolla, A.; Botella, C.; Montserrat-Gil de Bernabe, M.; Penelo, E.; et al. Eating-related environmental factors in underweight eating disorders and obesity: Are there common vulnerabilities during childhood and early adolescence? Eur. Eat. Disord. Rev. 2013, 21, 202–208. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Carracedo, D.; Neumark-Sztainer, D.; López-Guimerà, G. Integrated prevention of obesity and eating disorders: Barriers, developments and opportunities. Public Health Nutr. 2012, 15, 2295–2309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haines, J.; Neumark-Sztainer, D. Prevention of obesity and eating disorders: A consideration of shared risk factors. Health Educ. Res. 2006, 21, 770–782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, T.; Moore, T.H.; Hooper, L.; Gao, Y.; Zayegh, A.; Ijaz, S.; Elwenspoek, M.; Foxen, S.C.; Magee, L.; O’Malley, C.; et al. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2019, 7, CD001871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacDonald, D.E.; Cassin, S.E. Nondieting psychological interventions for individuals who are overweight or obese: A systematic review of the evidence. Psychopathol. Rev. 2017, a4, 290–318. [Google Scholar] [CrossRef]
- Hevey, D. Network analysis: A brief overview and tutorial. Health Psychol. Behav. Med. 2018, 6, 301–328. [Google Scholar] [CrossRef] [Green Version]
- Schlegl, S.; Smith, K.E.; Vierl, L.; Crosby, R.D.; Moessner, M.; Neumayr, C.; Voderholzer, U. Using network analysis to compare diagnosis-specific and age-specific symptom networks in eating disorders. Int. J. Eat. Disord. 2021, 54, 1463–1476. [Google Scholar] [CrossRef]
- Forrest, L.N.; Jones, P.J.; Ortiz, S.N.; Smith, A.R. Core psychopathology in anorexia nervosa and bulimia nervosa: A network analysis. Int. J. Eat. Disord. 2018, 51, 668–679. [Google Scholar] [CrossRef]
- Calugi, S.; Sartirana, M.; Misconel, A.; Boglioli, C.; Dalle Grave, R. Eating Disorder psychopathology in adults and adolescents with anorexia nervosa: A network approach. Int. J. Eat. Disord. 2020, 53, 420–431. [Google Scholar] [CrossRef]
- Solmi, M.; Collantoni, E.; Meneguzzo, P.; Degortes, D.; Tenconi, E.; Favaro, A. network analysis of specific psychopathology and psychiatric symptoms in patients with eating disorders. Int. J. Eat. Disord. 2018, 51, 680–692. [Google Scholar] [CrossRef]
- Monteleone, A.M.; Mereu, A.; Cascino, G.; Criscuolo, M.; Castiglioni, M.C.; Pellegrino, F.; Patriciello, G.; Ruzzi, V.; Monteleone, P.; Vicari, S.; et al. Re-conceptualization of anorexia nervosa psychopathology: A network analysis study in adolescents with short duration of the illness. Int. J. Eat. Disord. 2019, 52, 1263–1273. [Google Scholar] [CrossRef]
- Calugi, S.; Dalle Grave, R. Psychological features in obesity: A network analysis. Int. J. Eat. Disord. 2020, 53, 248–255. [Google Scholar] [CrossRef]
- Dalle Grave, R.; Soave, F.; Ruocco, A.; Dametti, L.; Calugi, S. Quality of life and physical performance in patients with obesity: A network analysis. Nutrients 2020, 12, 602. [Google Scholar] [CrossRef] [Green Version]
- Brogan, A.; Hevey, D.; Wilson, C.; Brinkley, A.; O’Malley, G.; Murphy, S. A network analysis of the causal attributions for obesity in children and adolescents and their parents. Psychol. Health Med. 2019, 24, 1063–1074. [Google Scholar] [CrossRef]
- Byrne, M.E.; Tanofsky-Kraff, M.; Lavender, J.M.; Parker, M.N.; Shank, L.M.; Swanson, T.N.; Ramirez, E.; LeMay-Russell, S.; Yang, S.B.; Brady, S.M.; et al. Bridging executive function and disinhibited eating among youth: A network analysis. Int. J. Eat. Disord. 2021, 54, 721–732. [Google Scholar] [CrossRef] [PubMed]
- Zeiler, M.; Wagner, G.; Philipp, J.; Nitsch, M.; Truttmann, S.; Dür, W.; Karwautz, A.; Waldherr, K. The Mental Health in Austrian Teenagers (MHAT) study: Design, methodology, description of study population. Neuropsychiatrie 2018, 32, 121–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, G.; Zeiler, M.; Waldherr, K.; Philipp, J.; Truttmann, S.; Dür, W.; Treasure, J.L.; Karwautz, A.F.K. Mental health problems in Austrian adolescents: A nationwide, Two-stage epidemiological study applying DSM-5 criteria. Eur. Child Adolesc. Psychiatry 2017, 26, 1483–1499. [Google Scholar] [CrossRef] [Green Version]
- Borsboom, D.; Deserno, M.K.; Rhemtulla, M.; Epskamp, S.; Fried, E.I.; McNally, R.J.; Robinaugh, D.J.; Perugini, M.; Dalege, J.; Costantini, G.; et al. Network analysis of multivariate data in psychological science. Nat. Rev. Methods Primer 2021, 1, 58. [Google Scholar] [CrossRef]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA School-Age Forms & Profiles; University of Vermont, Research Center for Children, Youth, & Families: Burlington, VA, USA, 2001. [Google Scholar]
- Döpfner, M.; Pflück, J.; Bölte, S.; Lenz, K.; Melchers, P.; Heim, K. Fragebogen für Jugendliche. Deutsche Bearbeitung des Youth Self-Report (YSR) der Child Behavior Checklist. Einführung und Anleitung zur Handauswertung.; Arbeitsgruppe Kinder, Jugend- und Familiendiagnostik: Köln, Germany, 1998. [Google Scholar]
- Morgan, J.F.; Reid, F.; Lacey, J.H. The SCOFF questionnaire: Assessment of a new screening tool for eating disorders. BMJ 1999, 319, 1467–1468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kutz, A.M.; Marsh, A.G.; Gunderson, C.G.; Maguen, S.; Masheb, R.M. Eating disorder screening: A systematic review and meta-analysis of diagnostic test characteristics of the SCOFF. J. Gen. Intern. Med. 2020, 35, 885–893. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; Gosch, A.; Rajmil, L.; Erhart, M.; Bruil, J.; Power, M.; Duer, W.; Auquier, P.; Cloetta, B.; Czemy, L.; et al. The KIDSCREEN-52 quality of life measure for children and adolescents: Psychometric results from a cross-cultural survey in 13 European countries. Value Health 2008, 11, 645–658. [Google Scholar] [CrossRef]
- JASP Team JASP. 2020. Available online: https://jasp-stats.org (accessed on 15 September 2021).
- Epskamp, S.; Borsboom, D.; Fried, E.I. Estimating psychological networks and their accuracy: A tutorial paper. Behav. Res. Methods 2018, 50, 195–212. [Google Scholar] [CrossRef] [Green Version]
- Epskamp, S.; Cramer, A.O.J.; Waldorp, L.J.; Schmittmann, V.D.; Borsboom, D. Qgraph: Network visualizations of relationships in psychometric data. J. Stat. Softw. 2012, 48, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Friedman, J.; Hastie, T.; Tibshirani, R. Sparse inverse covariance estimation with the graphical lasso. Biostat. Oxf. Engl. 2008, 9, 432–441. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Chen, Z. Extended bayesian information criteria for model selection with large model spaces. Biometrika 2008, 95, 759–771. [Google Scholar] [CrossRef] [Green Version]
- Fruchterman, T.M.J.; Reingold, E.M. Graph drawing by force-directed placement. Softw. Pract. Exp. 1991, 21, 1129–1164. [Google Scholar] [CrossRef]
- Van Borkulo, C.; van Bork, R.; Boschloo, L.; Kossakowski, J.; Tio, P.; Schoevers, R.; Borsboom, D.; Waldorp, L. Comparing network structures on three aspects: A permutation test. 2017. [CrossRef]
- Lipson, S.; Sonneville, K. Eating disorder symptoms among undergraduate and graduate students at 12 U.S. colleges and universities. Eat. Behav. 2017, 24, 81–88. [Google Scholar] [CrossRef]
- Vander Wal, J.S. Unhealthy weight control behaviors among adolescents. J. Health Psychol. 2012, 17, 110–120. [Google Scholar] [CrossRef]
- Cui, W.; Zack, M.M.; Wethington, H. Health-related quality of life and body mass index among US adolescents. Qual. Life Res. 2014, 23, 2139–2150. [Google Scholar] [CrossRef] [Green Version]
- Ihle, W.; Esser, G. Epidemiology of mental disorders in childhood and adolescence: Prevalence, course, comorbidity and gender differences. Psychol. Rundsch. 2002, 53, 159–169. [Google Scholar] [CrossRef]
- Leme, A.C.B.; Haines, J.; Tang, L.; Dunker, K.L.L.; Philippi, S.T.; Fisberg, M.; Ferrari, G.L.; Fisberg, R.M. Impact of strategies for preventing obesity and risk factors for eating disorders among adolescents: A systematic review. Nutrients 2020, 12, 3134. [Google Scholar] [CrossRef]
- Aparicio, E.; Canals, J.; Arija, V.; De Henauw, S.; Michels, N. The role of emotion regulation in childhood obesity: Implications for prevention and treatment. Nutr. Res. Rev. 2016, 29, 17–29. [Google Scholar] [CrossRef] [Green Version]
- Farhat, T. Stigma, Obesity and adolescent risk behaviors: Current Research and future directions. Curr. Opin. Psychol. 2015, 5, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Rankin, J.; Matthews, L.; Cobley, S.; Han, A.; Sanders, R.; Wiltshire, H.D.; Baker, J.S. Psychological consequences of childhood obesity: Psychiatric comorbidity and prevention. Adolesc. Health Med. Ther. 2016, 7, 125–146. [Google Scholar] [CrossRef] [Green Version]
- Cortese, S.; Moreira-Maia, C.R.; St Fleur, D.; Morcillo-Peñalver, C.; Rohde, L.A.; Faraone, S.V. Association between ADHD and obesity: A systematic review and meta-analysis. Am. J. Psychiatry 2016, 173, 34–43. [Google Scholar] [CrossRef]
- Stavrou, S.; Nicolaides, N.C.; Papageorgiou, I.; Papadopoulou, P.; Terzioglou, E.; Chrousos, G.P.; Darviri, C.; Charmandari, E. The effectiveness of a stress-management intervention program in the management of overweight and obesity in childhood and adolescence. J. Mol. Biochem. 2016, 5, 63–70. [Google Scholar]
- Emmanouil, C.-C.; Pervanidou, P.; Charmandari, E.; Darviri, C.; Chrousos, G.P. The Effectiveness of a health promotion and stress-management intervention program in a sample of obese children and adolescents. Horm. Athens Greece 2018, 17, 405–413. [Google Scholar] [CrossRef]
- Vandenbroeck, P.; Goossens, J.; Clemens, M. Tackling Obesities: Future Choices—Building the Obesity System Map; Department of Innovation Universities and Skills: London, UK, 2007. [Google Scholar]
- Nitsch, M.; Adamcik, T.; Kuso, S.; Zeiler, M.; Waldherr, K. Usability and engagement evaluation of an unguided online program for promoting a healthy lifestyle and reducing the risk for eating disorders and obesity in the school setting. Nutrients 2019, 11, 713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeiler, M.; Kuso, S.; Nitsch, M.; Simek, M.; Adamcik, T.; Herrero, R.; Etchemendy, E.; Mira, A.; Oliver, E.; Jones Bell, M.; et al. Online Interventions to prevent mental health problems implemented in school settings: The perspectives from key stakeholders in Austria and Spain. Eur. J. Public Health 2021, 31, i71–i79. [Google Scholar] [CrossRef] [PubMed]
- Jones Bell, M.; Zeiler, M.; Herrero, R.; Kuso, S.; Nitsch, M.; Etchemendy, E.; Fonseca-Baeza, S.; Oliver, E.; Adamcik, T.; Karwautz, A.; et al. Healthy teens @ school: Evaluating and disseminating transdiagnostic preventive interventions for eating disorders and obesity for adolescents in school settings. Internet Interv. 2019, 16, 65–75. [Google Scholar] [CrossRef]
- Jones, M.; Lynch, K.T.; Kass, A.E.; Burrows, A.; Williams, J.; Wilfley, D.E.; Taylor, C.B. Healthy weight regulation and eating disorder prevention in high school students: A universal and targeted web-based intervention. J. Med. Internet Res. 2014, 16, e57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Vriendt, T.; Huybrechts, I.; Ottevaere, C.; Van Trimpont, I.; De Henauw, S. Validity of self-reported weight and height of adolescents, its impact on classification into BMI-categories and the association with weighing behaviour. Int. J. Environ. Res. Public. Health 2009, 6, 2696–2711. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overweight Sample (n = 344) | Underweight Sample (n = 423) | Reference (Normal Weight Sample) (n = 1.560) | |
|---|---|---|---|
| Female sex (%) | 52.6% | 66.9% | 53.8% |
| Age (Mean, SD) | 14.79 (2.34) | 14.30 (2.38) | 14.77 (2.27) |
| Migration background 1 (%) | 31.7% | 22.6% | 25.3% |
| Living with both parents (%) | 69.3% | 71.3% | 74.3% |
| Residency (living in urban region) 2 (%) | 54.6% | 55.5% | 58.8% |
| Employment status of parents | |||
| Both parents employed (%) | 70.2% | 77.3% | 79.1% |
| No or one parent employed (%) | 29.8% | 22.7% | 20.9% |
| BMI (Mean, SD) | 27.00 (3.30) | 15.67 (1.42) | 19.82 (1.64) |
| BMI-SDS 3 (Mean, SD) | 1.83 (0.46) | −1.92 (0.63) | −0.01 (0.38) |
| Any diagnosed psychiatric disorder (%) | 8.0% | 11.3% | 4.0% |
| Any diagnosed chronic somatic illness (%) | 13.3% | 14.1% | 10.7% |
| Diagnosed psychiatric disorders in family (%) | 6.2% | 7.0% | 4.0% |
| Diagnosed chronic somatic illness in family (%) | 19.0% | 15.4% | 16.4% |
| Overweight Sample (Mean, SD) | Underweight Sample (Mean, SD) | Reference (Normal Weight Sample) (Mean, SD) | Overweight vs. Normal Weight (Tukey Test 1) | Underweight vs. Normal Weight (Tukey Test 1) | |
|---|---|---|---|---|---|
| General Psychopathology | |||||
| Total Problems | 41.06 (23.85) | 33.84 (20.72) | 34.64 (20.48) | p < 0.001 | p = 0.766 |
| Internalizing Problems | 13.16 (11.13) | 12.27 (9.21) | 11.11 (8.70) | p < 0.001 | p = 0.041 |
| Externalizing Problems | 11.22 (6.69) | 8.90 (10.47) | 10.53 (6.67) | p = 0.186 | p < 0.001 |
| Socially withdrawn | 3.46 (2.77) | 3.39 (2.73) | 2.90 (2.58) | p = 0.001 | p = 0.002 |
| Somatic Complaints | 3.50 (3.18) | 3.20 (2.82) | 3.04 (2.78) | p = 0.014 | p = 0.543 |
| Anxious/Depressed | 6.71 (6.48) | 6.14 (5.56) | 5.56 (5.22) | p = 0.001 | p = 0.115 |
| Social Problems | 2.66 (2.44) | 2.17 (2.14) | 1.99 (2.02) | p < 0.001 | p = 0.264 |
| Thought Problems | 1.71 (2.09) | 1.41 (1.88) | 1.53 (1.93) | p = 0.284 | p = 0.509 |
| Attention Problems | 5.10 (3.03) | 4.53 (3.07) | 4.58 (2.93) | p = 0.008 | p = 0.952 |
| Dissocial Behavior | 3.56 (2.53) | 2.78 (2.45) | 3.36 (2.66) | p = 0.412 | p < 0.001 |
| Aggressive Behavior | 7.66 (4.76) | 6.12 (4.38) | 7.17 (4.66) | p = 0.174 | p < 0.001 |
| Eating Disorder Risk | |||||
| SCOFF score | 1.33 (1.18) | 0.74 (1.07) | 0.88 (1.04) | p < 0.001 | p = 0.047 |
| Well-being/Quality of Life | |||||
| KIDSCREEN-10 | 38.08 (7.54) | 37.74 (7.19) | 40.01 (6.77) | p < 0.001 | p = 0.775 |
| Self-Perception | 17.39 (4.60) | 19.42 (4.46) | 19.10 (4.27) | p < 0.001 | p = 0.321 |
| Parent-Relation & Home-Life | 24.90 (5.29) | 25.97 (4.59) | 25.86 (4.64) | p = 0.002 | p = 0.900 |
| Social support & Peers | 16.28 (3.46) | 16.68 (17.05) | 17.03 (2.92) | p < 0.001 | p = 0.094 |
| School Environment | 14.67 (3.57) | 15.60 (3.25) | 15.31 (3.28) | p = 0.004 | p = 0.283 |
| Social Acceptance/Bullying | 13.15 (2.62) | 13.99 (1.81) | 13.86 (2.01) | p < 0.001 | p = 0.484 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zeiler, M.; Philipp, J.; Truttmann, S.; Waldherr, K.; Wagner, G.; Karwautz, A. Psychopathological Symptoms and Well-Being in Overweight and Underweight Adolescents: A Network Analysis. Nutrients 2021, 13, 4096. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13114096
Zeiler M, Philipp J, Truttmann S, Waldherr K, Wagner G, Karwautz A. Psychopathological Symptoms and Well-Being in Overweight and Underweight Adolescents: A Network Analysis. Nutrients. 2021; 13(11):4096. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13114096
Chicago/Turabian StyleZeiler, Michael, Julia Philipp, Stefanie Truttmann, Karin Waldherr, Gudrun Wagner, and Andreas Karwautz. 2021. "Psychopathological Symptoms and Well-Being in Overweight and Underweight Adolescents: A Network Analysis" Nutrients 13, no. 11: 4096. https://0-doi-org.brum.beds.ac.uk/10.3390/nu13114096