
Perceptions of Tailored Dietary Advice to Improve the Nutrient Adequacy of the Diet in French Pregnant Women


 , , and
, , and
Abstract
:1. Background
2. Methods
2.1. Study Design and Ethics
2.2. Background Information: Stepwise Dietary Counseling, Based on Three Types of Dietary Changes to Improve the Nutrient Adequacy of the Diet
2.3. Data Collection in the Focus Group Study
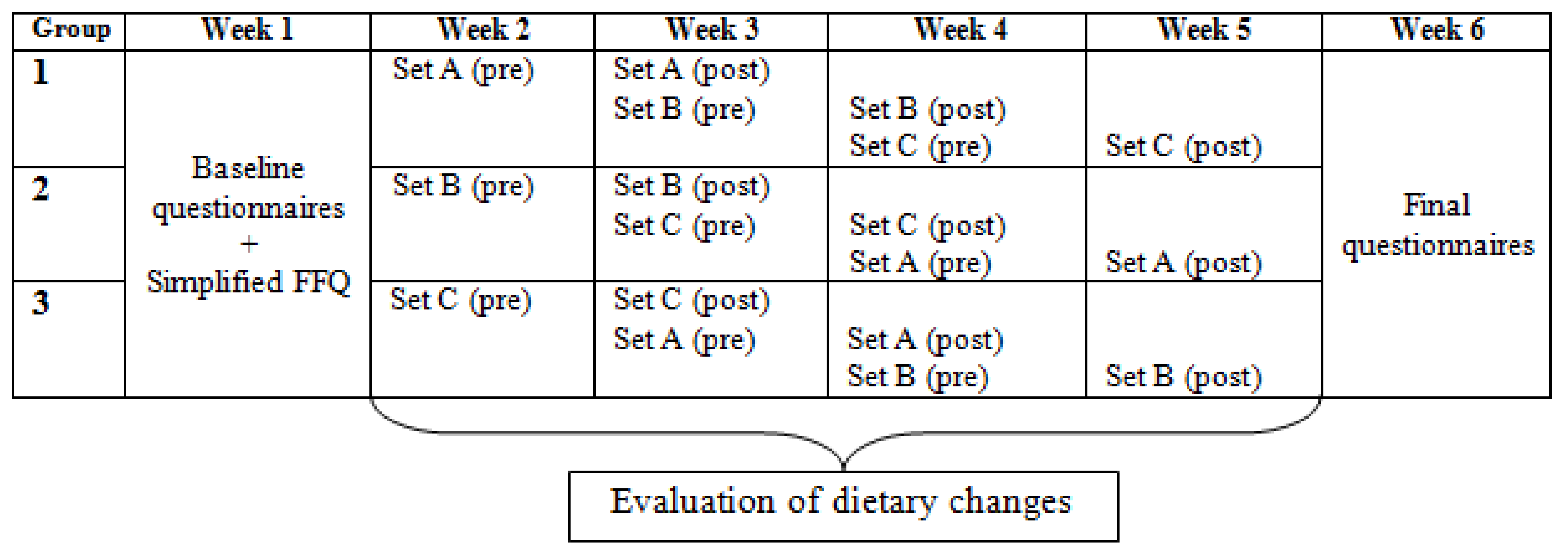
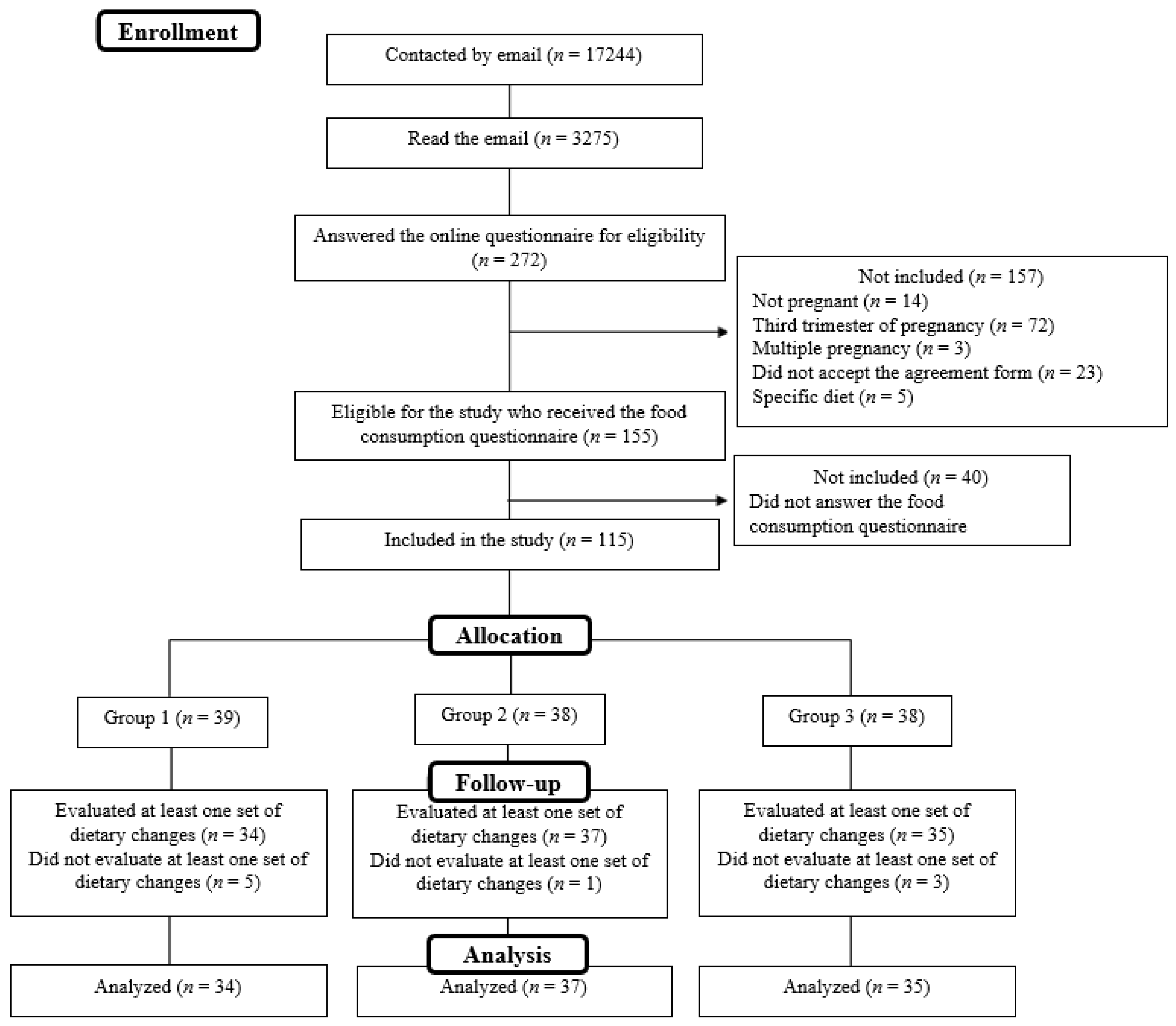
2.4. Data Collection in the 6-Week Online Longitudinal Study
2.5. Analysis of Qualitative Data
2.6. Statistical Analysis of Quantitative Data
3. Results
3.1. Modification of Dietary Habits during Pregnancy
3.1.1. Qualitative Data from the Focus Group Study
3.1.2. Quantitative Data from the Online Longitudinal Study
3.2. A Dietary Advice Tool for Use during Pregnancy
3.2.1. Qualitative Data from the Focus Group Study
3.2.2. Quantitative Data from the Online Longitudinal Study
3.3. Barriers and Enablers to the Implementation of Each Type of Dietary Advice
Qualitative Data from the Focus Group and from the Online Longitudinal Studies
3.4. Favorite Types of Dietary Changes
3.4.1. Qualitative Data from the Focus Group Study
3.4.2. Quantitative Data from the Online Longitudinal Study
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| FG | focus group study |
| OLS | online longitudinal study |
References
- Herman, D.R.; Baer, M.T.; Adams, E.; Cunningham-Sabo, L.; Duran, N.; Johnson, D.B.; Yakes, E. Life Course Perspective: Evidence for the Role of Nutrition. Matern. Child Health J. 2014, 18, 450–461. [Google Scholar] [CrossRef] [PubMed]
- Wethington, E. An Overview of the Life Course Perspective: Implications for Health and Nutrition. J. Nutr. Educ. Behav. 2005, 37, 115–120. [Google Scholar] [CrossRef]
- Devine, C.M.; Bove, C.F.; Olson, C.M. Continuity and change in women’s weight orientations and lifestyle practices through pregnancy and the postpartum period: The influence of life course trajectories and transitional events. Soc. Sci. Med. 2000, 50, 567–582. [Google Scholar] [CrossRef]
- Blondel, B.; Kermarrec, M. Enquête Nationale Périnatale 2010—Les Naissances en 2010 et leur Évolution Depuis 2003 [Internet]; Ministère du Travail, de l’Emploi et de la Santé: Paris, France, 2011; p. 132. Available online: http://www.epopé-inserm.fr/wp-content/uploads/2015/01/Rapport-Naisances-ENP2010.pdf (accessed on 7 June 2017).
- Centers for Disease Control and Prevention (CDC). Alcohol consumption among women who are pregnant or who might become pregnant--United States, 2002. MMWR Morb. Mortal. Wkly. Rep. 2004, 53, 1178–1181. [Google Scholar]
- Lelong, N.; Kaminski, M.; Saurel-Cubizolles, M.-J.; Bouvier-Colle, M.-H. Postpartum return to smoking among usual smokers who quit during pregnancy. Eur. J. Public Health 2001, 11, 334–339. [Google Scholar] [CrossRef] [Green Version]
- Szwajcer, E.M.; Hiddink, G.J.; Koelen, M.A.; van Woerkum, C.M. Nutrition awareness and pregnancy: Implications for the life course perspective. Eur. J. Obstet. Gynecol. Reprod. Biol. 2007, 135, 58–64. [Google Scholar] [CrossRef]
- Szwajcer, E.; Hiddink, G.J.; Maas, L.; Koelen, M.; Van Woerkum, C. Nutrition awareness before and throughout different trimesters in pregnancy: A quantitative study among Dutch women. Fam. Pr. 2012, 29, i82–i88. [Google Scholar] [CrossRef] [Green Version]
- Bianchi, C.M.; Huneau, J.-F.; Le Goff, G.; Verger, E.O.; Mariotti, F.; Gurviez, P. Concerns, attitudes, beliefs and information seeking practices with respect to nutrition-related issues: A qualitative study in French pregnant women. BMC Pregnancy Childbirth 2016, 16, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Szwajcer, E.M.; Hiddink, G.J.; Koelen, M.A.; Van Woerkum, C.M.J. Nutrition-related information-seeking behaviours before and throughout the course of pregnancy: Consequences for nutrition communication. Eur. J. Clin. Nutr. 2005, 59, S57–S65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szwajcer, E.M.; Hiddink, G.J.; Maas, L.; Koelen, M.A.; Van Woerkum, C.M.J. Nutrition-related information-seeking behaviours of women trying to conceive and pregnant women: Evidence for the life course perspective. Fam. Pr. 2008, 25, i99–i104. [Google Scholar] [CrossRef]
- Goodrich, K.; Cregger, M.; Wilcox, S.; Liu, J. A Qualitative Study of Factors Affecting Pregnancy Weight Gain in African American Women. Matern. Child Health J. 2013, 17, 432–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitaker, K.M.; Wilcox, S.; Liu, J.; Blair, S.N.; Pate, R.R. African American and White women’s perceptions of weight gain, physical activity, and nutrition during pregnancy. Midwifery 2016, 34, 211–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kominiarek, M.A.; Gay, F.; Peacock, N. Obesity in Pregnancy: A Qualitative Approach to Inform an Intervention for Patients and Providers. Matern. Child Health J. 2015, 19, 1698–1712. [Google Scholar] [CrossRef] [PubMed]
- Graham, J.E.; Mayan, M.; McCargar, L.J.; Bell, R.C.; Sweet Moms Team. Making compromises: A qualitative study of sugar con-sumption behaviors during pregnancy. J. Nutr. Educ. Behav. 2013, 45, 578–585. [Google Scholar] [CrossRef]
- Whitaker, K.M.; Wilcox, S.; Liu, J.; Blair, S.N.; Pate, R.R. Patient and Provider Perceptions of Weight Gain, Physical Activity, and Nutrition Counseling during Pregnancy: A Qualitative Study. Women’s Health Issues 2016, 26, 116–122. [Google Scholar] [CrossRef] [Green Version]
- Blumfield, M.L.; Hure, A.J.; Macdonald-Wicks, L.; Smith, R.; Collins, C.E. Systematic review and meta-analysis of energy and mac-ronutrient intakes during pregnancy in developed countries. Nutr. Rev. 2012, 70, 322–336. [Google Scholar] [CrossRef]
- Blumfield, M.L.; Hure, A.J.; MacDonald-Wicks, L.; Smith, R.; Collins, C.E. A systematic review and meta-analysis of micronutrient intakes during pregnancy in developed countries. Nutr. Rev. 2013, 71, 118–132. [Google Scholar] [CrossRef]
- Christian, P.; Stewart, C.P. Maternal Micronutrient Deficiency, Fetal Development, and the Risk of Chronic Disease. J. Nutr. 2010, 140, 437–445. [Google Scholar] [CrossRef] [Green Version]
- Barker, D.J.P. EDITORIAL: The developmental origins of adult disease. Eur. J. Epidemiol. 2002, 18, 733–736. [Google Scholar] [CrossRef]
- Celis-Morales, C.; Lara, J.; Mathers, J.C. Personalising nutritional guidance for more effective behaviour change. Proc. Nutr. Soc. 2015, 74, 130–138. [Google Scholar] [CrossRef] [Green Version]
- Eyles, H.; Mhurchu, C.N. Tailored nutrition education: Is it really effective? Public Health Nutr. 2011, 15, 561–566. [Google Scholar] [CrossRef] [Green Version]
- Eyles, H.C.; Mhurchu, C.N. Does tailoring make a difference? A systematic review of the long-term effectiveness of tailored nu-trition education for adults. Nutr. Rev. 2009, 67, 464–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broekhuizen, K.; Kroeze, W.; van Poppel, M.N.; Oenema, A.; Brug, J. A Systematic Review of Randomized Controlled Trials on the Effectiveness of Computer-Tailored Physical Activity and Dietary Behavior Promotion Programs: An Update. Ann. Behav. Med. 2012, 44, 259–286. [Google Scholar] [CrossRef] [Green Version]
- De Vries, H.; Brug, J. Computer-tailored interventions motivating people to adopt health promoting behaviours: Introduction to a new approach. Patient Educ Couns. 1999, 36, 99–105. [Google Scholar] [PubMed]
- Krebs, P.; Prochaska, J.O.; Rossi, J.S. Defining what works in tailoring: A meta-analysis of computer-tailored interventions for health behavior change. Prev. Med. 2010, 51, 214–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lairson, D.R.; Newmark, G.R.; Rakowski, W.; Tiro, J.A.; Vernon, S.W. Development costs of a computer-generated tailored interven-tion. Eval. Program Plann. 2004, 27, 161–169. [Google Scholar] [CrossRef]
- Bianchi, C.M.; Huneau, J.-F.; Barbillon, P.; Lluch, A.; Egnell, M.; Fouillet, H. Les Conseils Alimentaires Personnalisés Améliorant le plus Efficacement l’Adéquation Nutritionnelle des Régimes en Début de Grossesse sont les Moins Acceptables; Journées Francophones de Nutrition: Montpellier, France, 2016. [Google Scholar]
- Bianchi, C.M.; Mariotti, F.; Verger, E.O.; Huneau, J.-F. Pregnancy Requires Major Changes in the Quality of the Diet for Nutritional Adequacy: Simulations in the French and the United States Populations. PLoS ONE 2016, 11, e0149858. [Google Scholar] [CrossRef]
- Vandelanotte, C.; Bourdeaudhuij, I.D.; Brug, J. Acceptability and feasibility of an interactive computer-tailored fat intake inter-vention in Belgium. Health Promot. Int. 2004, 19, 463–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinrich, N.K. Hands-On Social Marketing A Step-by-Step Guide to Designing Change for Good, 2nd ed.; SAGE Publishing: Los Angeles, CA, USA, 2011. [Google Scholar]
- Pluye, P.; Hong, Q.N. Combining the Power of Stories and the Power of Numbers: Mixed Methods Research and Mixed Studies Reviews. Annu. Rev. Public Health 2014, 35, 29–45. [Google Scholar] [CrossRef]
- Hackley, B.; Kennedy, H.P.; Berry, D.C.; Melkus, G.D. A mixed-methods study on factors influencing prenatal weight gain in eth-nic-minority women. J. Midwifery Womens Health 2014, 59, 388–398. [Google Scholar] [CrossRef]
- Sui, Z.; Turnbull, D.A.; Dodd, J.M. Overweight and Obese Women’s Perceptions about Making Healthy Change during Pregnancy: A Mixed Method Study. Matern. Child Health J. 2013, 17, 1879–1887. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for inter-views and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Fade, S.A.; Swift, J.A. Qualitative research in nutrition and dietetics: Data analysis issues. J. Hum. Nutr. Diet. 2010, 24, 106–114. [Google Scholar] [CrossRef]
- Gardner, B.; Croker, H.; Barr, S.; Briley, A.; Poston, L.; Wardle, J.; On Behalf Of The Upbeat Trial. Psychological predictors of dietary intentions in pregnancy. J. Hum. Nutr. Diet. 2012, 25, 345–353. [Google Scholar] [CrossRef]
- Mullan, B.; Henderson, J.; Kothe, E.; Allom, V.; Orbell, S.; Hamilton, K. The Role of Habit and Perceived Control on Health Behav-ior among Pregnant Women. Am. J. Health Behav. 2016, 40, 291–301. [Google Scholar] [CrossRef]
- Whitaker, K.M.; Wilcox, S.; Liu, J.; Blair, S.N.; Pate, R.R. Pregnant women’s perceptions of weight gain, physical activity, and nutri-tion using Theory of Planned Behavior constructs. J. Behav. Med. 2016, 39, 41–54. [Google Scholar] [CrossRef]
- Lange, D.; Corbett, J.; Lippke, S.; Knoll, N.; Schwarzer, R. The interplay of intention, autonomy, and sex with dietary planning: A conditional process model to predict fruit and vegetable intake. Br. J. Health Psychol. 2015, 20, 859–876. [Google Scholar] [CrossRef] [PubMed]
- Sheeran, P. Intention—Behavior Relations: A Conceptual and Empirical Review. Eur. Rev. Soc. Psychol. 2002, 12, 1–36. [Google Scholar] [CrossRef]
- Hawkins, M.; Hosker, M.; Marcus, B.H.; Rosal, M.C.; Braun, B.; Stanek, E.J.; Markenson, G.; Chasan-Taber, L. A pregnancy lifestyle intervention to prevent gesta-tional diabetes risk factors in overweight Hispanic women: A feasibility randomized controlled trial. Diabet. Med. 2015, 32, 108–115. [Google Scholar] [CrossRef]
- Chasan-Taber, L.; Marcus, B.H.; Rosal, M.C.; Tucker, K.L.; Hartman, S.J.; Pekow, P.; Stanek, E.; Braun, B.; Solomon, C.G.; Manson, J.E.; et al. Proyecto Mamá: A lifestyle intervention in overweight and obese Hispanic women: A randomised controlled trial—Study protocol. BMC Pregnancy Childbirth 2015, 15, 157. [Google Scholar] [CrossRef] [Green Version]
- Willcox, J.C.; Campbell, K.J.; McCarthy, E.A.; Wilkinson, S.A.; Lappas, M.; Ball, K.; Fjeldsoe, B.; Griffiths, A.; Whittaker, R.; Maddison, R.; et al. Testing the feasibility of a mobile technology intervention promoting healthy gestational weight gain in pregnant women (txt4two)—Study protocol for a randomised con-trolled trial. Trials 2015, 16, 209. [Google Scholar] [CrossRef] [Green Version]
- Di Carlo, C.; Iannotti, G.; Sparice, S.; Chiacchio, M.P.; Greco, E.; Tommaselli, G.A.; Nappi, C. The role of a personalized dietary interven-tion in managing gestational weight gain: A prospective, controlled study in a low-risk antenatal population. Arch. Gynecol. Obstet. 2014, 289, 765–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, M.-W.; Nitzke, S.; Guilford, E.; Adair, C.H.; Hazard, D.L. Motivators and Barriers to Healthful Eating and Physical Activity among Low-Income Overweight and Obese Mothers. J. Am. Diet. Assoc. 2008, 108, 1023–1028. [Google Scholar] [CrossRef] [PubMed]
- Hromi-Fiedler, A.; Chapman, D.; Segura-Pérez, S.; Damio, G.; Clark, P.; Martinez, J.; Pérez-Escamilla, R. Barriers and Facilitators to Improve Fruit and Vegetable Intake Among WIC-Eligible Pregnant Latinas: An Application of the Health Action Process Approach Framework. J. Nutr. Educ. Behav. 2016, 48, 468–477.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reyes, N.R.; Klotz, A.A.; Herring, S.J. A Qualitative Study of Motivators and Barriers to Healthy Eating in Pregnancy for Low-Income, Overweight, African-American Mothers. J. Acad. Nutr. Diet. 2013, 113, 1175–1181. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Ashford, S.; Sniehotta, F.F.; Dombrowski, S.U.; Bishop, A.; French, D.P. A refined taxonomy of behaviour change tech-niques to help people change their physical activity and healthy eating behaviours: The CALO-RE taxonomy. Psychol. Health 2011, 26, 1479–1498. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Aix-en-Provence (n = 13) | Paris (n = 27) | Total (n = 40) | |
|---|---|---|---|
| Age 1 (years) | 31.9 ± 5.5 | 29.7 ± 3.4 | 30.5 ± 4.2 |
| Pre-pregnancy BMI 1 (kg/m2) | 21.8 ± 3.0 | 22.5 ± 3.7 | 22.2 ± 3.4 |
| Trimester of pregnancy 2 | |||
| 1st | 15.4% (2) | 11.1% (3) | 12.5% (5) |
| 2nd | 23.1% (3) | 63.0% (17) | 50.0% (20) |
| 3rd | 61.5% (8) | 25.9% (7) | 37.5% (15) |
| Primiparous 2 | 46.2% (6) | 51.9% (14) | 50.0% (20) |
| Household income 2 (EUR per month) | |||
| <2000 | 23.1% (3) | 11.1% (3) | 15.0% (6) |
| 2000–4000 | 38.5% (5) | 55.6% (15) | 50.0% (20) |
| >4000 | 30.8% (4) | 22.2% (6) | 25.0% (10) |
| Did not wish to answer | 7.7% (1) | 11.1% (3) | 10.0% (4) |
| Had previously followed a diet 2 | |||
| Never | 30.8% (4) | 51.9% (14) | 45.0% (18) |
| Once | 30.8% (4) | 11.1% (3) | 17.5% (7) |
| Several times | 38.5% (5) | 37.0% (10) | 37.5% (15) |
| Summary of Key Questions |
|---|
| Have you heard about any materials (app, internet, guide book) which provide tailored dietary advice during pregnancy? If yes, do you use one of them, and why? |
| If you had to design the perfect dietary advice tool for pregnancy, what would it be like? |
| I have explained the tailored dietary counseling approach that we have designed for pregnancy; what would the pregnant women using it be like? And those not using it? |
| Might you adopt this tailored dietary counseling approach during your pregnancy? |
| Among the dietary changes I have presented, which type would be your favorite? |
| Total (n = 115) | Group 1 (n = 39) | Group 2 (n = 38) | Group 3 (n = 38) | |
|---|---|---|---|---|
| Age (years) 1,4 | 31.1 ± 4.2 | 32.0 ± 4.2 | 31.2 ± 4.4 | 30.2 ± 4.1 |
| Months of pregnancy 2,5 | ||||
| Less than 3 | 39.1% (45) | 35.9% (14) | 36.8% (14) | 44.7% (17) |
| 3 or 4 | 32.2% (37) | 33.3% (13) | 28.9% (11) | 34.2% (13) |
| 5 or 6 | 28.7% (33) | 30.8% (12) | 34.2% (13) | 21.1% (8) |
| Primiparous 2,5 | 47.8% (55) | 41.0% (16) | 55.3% (21) | 47.4% (18) |
| Number of people composing the household 2,5 | ||||
| 1 | 0.9% (1) | 0.0% (0) | 2.6% (1) | 0.0% (0) |
| 2 | 52.2% (60) | 51.3% (20) | 52.6% (20) | 52.6% (20) |
| 3 | 36.5% (42) | 38.5% (15) | 34.2% (13) | 36.8% (14) |
| 4 | 7.0% (8) | 2.6% (1) | 10.5% (4) | 7.9% (3) |
| 5 | 1.7% (2) | 5.1% (2) | 0.0% (0) | 0.0% (0) |
| 6 or more | 1.7% (2) | 2.6% (1) | 0.0% (0) | 2.6% (1) |
| Number of children 2,5 | ||||
| 0 | 47.8% (55) | 41.0% (16) | 52.6% (20) | 50.0% (19) |
| 1 | 40.0% (47) | 46.2% (18) | 34.2% (13) | 39.5% (15) |
| 2 | 7.8% (9) | 5.1% (2) | 10.5% (4) | 7.9% (3) |
| 3 | 1.7% (2) | 5.1% (2) | 0.0% (0) | 0.0% (0) |
| 4 or more | 0.9% (1) | 2.6% (1) | 0.0% (0) | 0.0% (0) |
| No answer | 0.9% (1) | 0.0% (0) | 2.6% (1) | 0.0% (0) |
| Occupation 2 | ||||
| Farmer, Craftsperson, Storekeeper | 0.9% (1) | 0.0% (0) | 0.0% (0) | 2.6% (1) |
| Professional, executive | 20.0% (23) | 15.4% (6) | 23.7% (9) | 21.1% (8) |
| Intermediate profession | 14.8% (17) | 20.5% (8) | 13.2% (5) | 10.5% (4) |
| Employee | 50.4% (58) | 51.3% (20) | 55.3% (21) | 44.7% (17) |
| Manual worker | 0.0% (0) | 0.0% (0) | 0.0% (0) | 0.0% (0) |
| Student | 0.9% (1) | 0.0% (0) | 2.6% (1) | 0.0% (0) |
| Inactive | 13.1% (15) | 12.8% (5) | 5.3% (2) | 21.1% (8) |
| Socio-professional category 2,3,5 | ||||
| High | 35.7% (41) | 35.9% (14) | 36.8% (14) | 34.2% (13) |
| Low | 50.4% (58) | 51.3% (20) | 55.3% (21) | 44.7% (17) |
| Unemployed | 13.9% (16) | 12.8% (5) | 7.9% (3) | 21.1% (8) |
| Urbanization of the place of residence 2,5 | ||||
| Paris | 8.7% (10) | 7.7% (3) | 13.2% (5) | 5.3% (2) |
| Major city (>100,000 inhab.) | 26.1% (30) | 33.3% (13) | 23.7% (9) | 21.1% (8) |
| Medium-sized town (20–100,000 inhab.) | 24.3% (28) | 23.1% (9) | 18.2% (7) | 31.6% (12) |
| Small-sized town (2–20,000 inhab.) | 25.2% (29) | 17.9% (7) | 26.3% (10) | 31.6% (12) |
| Rural area | 13.0% (15) | 15.4% (6) | 18.4% (7) | 5.3% (2) |
| No answer | 2.6% (3) | 2.6% (1) | 0.0% (0) | 5.3% (2) |
| Nutrition awareness during pregnancy 2,5 | ||||
| Much more aware | 25.2% (29) | 23.1% (9) | 23.7% (9) | 28.9% (11) |
| A little more aware | 59.1% (68) | 56.4% (22) | 60.5% (23) | 60.5% (23) |
| Not really more aware | 14.8% (17) | 20.5% (8) | 13.2% (5) | 10.5% (4) |
| Not more aware at all | 0.9% (1) | 0.0% (0) | 2.6% (1) | 0.0% (0) |
| Enablers | Barriers | |
|---|---|---|
| Type 1 | No modifications to the shopping list “it is just a matter of simplicity […] my shopping list is not modified” (Participant 2, FG4) Adequacy with food preferences and cravings “It’s all psychological what we want to eat, if I plan [to eat] a drumstick, I will eat a drumstick!” (Participant 6, FG6) No profound change “The decrease being negligible, it seems very feasible to me” (Participant 1, OLS) Identification of mistakes to control weight gain (when decreasing amounts) “I feel more in control of my weight gain when I am required to reduce my food intake […] it highlights our mistakes and we are just required to adjust the amounts” (Participant 5, FG1) | No idea about the amount consumed (no weighing scales at home) “My problem is that I do not weigh what I eat” (Participant 3, FG2) Reducing amounts means being on a diet “This type is super restrictive because it is about weight so it is frustrating” (Participant 5, FG2) Not hungry enough to increase amounts “I eat until satiety and I don’t want to force myself to eat more than I need” (Participant 3, OLS) Increasing amounts means putting on weight “I don’t want to increase my consumption so as not to put on weight” (Participant 4, OLS) |
| Type 2 | Easy to implement small changes “They are both fruits, so you just have to substitute one for another” (Participant 8, OLS) New ideas without markedly changing dietary habits “It gives us news ideas and small alternatives” (Participant 4, FG1) No reduction in pleasure foods “It means we eat something nutritionally better without being too frustrated” (Participant 1, FG7) | Seasonality “What’s the point of replacing a seasonal product [tomatoes] […] with a processed one (lamb’s lettuce)?” (Participant 6, OLS) |
| Type 3 | New ideas which represent a means of shifting from deep-rooted habits “It gives us ideas and breaks the routine of our usual diet” (Participant 7, FG6) | Changes too far removed from their instantaneous cravings “I am sorry, but I don’t want to eat fish when I crave meat” (Participant 1, FG3) Foods not used on the same occasion “I used mainly cheese to cook sauces or gratins so it is difficult for me to replace it with nuts” (Participant 9, OLS) Price “I really like fish but it is more expensive than cold cuts” (Participant 10, OLS) |
| Types 2 and 3 | Preference for the food items proposed “It’s easy because we love spinach in my family” (Participant 1, OLS) | Less variety in the diet when the proposed food item is already consumed “Eating a huge variety of foods makes me feel really good […], to give up on one food for another is nonsensical... ” (Participant 6, OLS) Strong preference for the food to be replaced “I like pasta too much to replace it” (Participant 2, OLS) Do not like the proposed food “I don’t like rapeseed oil, it tastes too strong” (Participant 5, OLS) Do not know how to cook the proposed food “ I don’t cook fish very often” (Participant 7, OLS) |
| Dietary Changes from Type 1 Are Easy to Implement in the Diet | |
| Strongly agree | 32.5% (26) 1 |
| Agree | 48.8% (39) |
| Disagree | 17.5% (14) |
| Strongly disagree | 1.3% (1) |
| Dietary changes from Type 2 are easy to implement in the diet | |
| Strongly agree | 33.8% (27) |
| Agree | 58.8% (47) |
| Disagree | 5.0% (4) |
| Strongly disagree | 1.3% (1) |
| No answer | 1.3% (1) |
| Dietary changes from Type 3 are easy to implement in the diet | |
| Strongly agree | 23.8% (19) |
| Agree | 51.3% (41) |
| Disagree | 23.8% (19) |
| Strongly disagree | 1.3% (1) |
| If I had to choose, I would favor dietary changes from | |
| Type 1 | 32.5% (26) |
| Type 2 | 45.0% (36) |
| Type 3 | 22.5% (18) |
| If I had to choose, I would not favor dietary changes from | |
| Type 1 | 35.0% (28) |
| Type 2 | 15.0% (12) |
| Type 3 | 48.8% (39) |
| No answer | 1.3% (1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bianchi, C.M.; Mariotti, F.; Reulet, E.; Le Goff, G.; Lluch, A.; Verger, E.O.; Huneau, J.-F.; Gurviez, P. Perceptions of Tailored Dietary Advice to Improve the Nutrient Adequacy of the Diet in French Pregnant Women. Nutrients 2022, 14, 85. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14010085
Bianchi CM, Mariotti F, Reulet E, Le Goff G, Lluch A, Verger EO, Huneau J-F, Gurviez P. Perceptions of Tailored Dietary Advice to Improve the Nutrient Adequacy of the Diet in French Pregnant Women. Nutrients. 2022; 14(1):85. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14010085
Chicago/Turabian StyleBianchi, Clélia M., François Mariotti, Elodie Reulet, Gaëlle Le Goff, Anne Lluch, Eric O. Verger, Jean-François Huneau, and Patricia Gurviez. 2022. "Perceptions of Tailored Dietary Advice to Improve the Nutrient Adequacy of the Diet in French Pregnant Women" Nutrients 14, no. 1: 85. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14010085