
Iodine Supplementation in Pregnancy in an Iodine-Deficient Region: A Cross-Sectional Survey

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Assessment of Urinary Iodine Concentration
2.3. Statistical Analyses
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jouanne, M.; Oddoux, S.; Noel, A.; Voisin-Chiret, A.S. Nutrient Requirements during Pregnancy and Lactation. Nutrients 2021, 13, 692. [Google Scholar] [CrossRef] [PubMed]
- Mousa, A.; Naqash, A.; Lim, S. Macronutrient and Micronutrient Intake during Pregnancy: An Overview of Recent Evidence. Nutrients 2019, 11, 443. [Google Scholar] [CrossRef] [Green Version]
- Gernand, A.D.; Schulze, K.J.; Stewart, C.P.; West, K.P., Jr.; Christian, P. Micronutrient deficiencies in pregnancy worldwide: Health effects and prevention. Nat. Rev. Endocrinol. 2016, 12, 274–289. [Google Scholar] [CrossRef] [Green Version]
- Candido, A.C.; Morais, N.S.; Dutra, L.V.; Pinto, C.A.; Franceschini, S.; Alfenas, R.C.G. Insufficient iodine intake in pregnant women in different regions of the world: A systematic review. Arch. Endocrinol. Metab. 2019, 63, 306–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Diaz, E.; Pearce, E.N. Iodine status and supplementation before, during, and after pregnancy. Best Pract. Res. Clin. Endocrinol. Metab. 2020, 34, 101430. [Google Scholar] [CrossRef]
- Toloza, F.J.K.; Motahari, H.; Maraka, S. Consequences of Severe Iodine Deficiency in Pregnancy: Evidence in Humans. Front Endocrinol. 2020, 11, 409. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B. The Importance of Adequate Iodine during Pregnancy and Infancy. World Rev. Nutr. Diet. 2016, 115, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Dineva, M.; Fishpool, H.; Rayman, M.P.; Mendis, J.; Bath, S.C. Systematic review and meta-analysis of the effects of iodine supplementation on thyroid function and child neurodevelopment in mildly-to-moderately iodine-deficient pregnant women. Am. J. Clin. Nutr. 2020, 112, 389–412. [Google Scholar] [CrossRef]
- Levie, D.; Korevaar, T.I.M.; Bath, S.C.; Murcia, M.; Dineva, M.; Llop, S.; Espada, M.; van Herwaarden, A.E.; de Rijke, Y.B.; Ibarluzea, J.M.; et al. Association of Maternal Iodine Status With Child IQ: A Meta-Analysis of Individual Participant Data. J. Clin. Endocrinol. Metab. 2019, 104, 5957–5967. [Google Scholar] [CrossRef] [Green Version]
- Rohner, F.; Zimmermann, M.; Jooste, P.; Pandav, C.; Caldwell, K.; Raghavan, R.; Raiten, D.J. Biomarkers of nutrition for development iodine review. J. Nutr. 2014, 144, 1322S–1342S. [Google Scholar] [CrossRef] [Green Version]
- Secretariat, W.H.O.; Andersson, M.; de Benoist, B.; Delange, F.; Zupan, J. Prevention and control of iodine deficiency in pregnant and lactating women and in children less than 2-years-old: Conclusions and recommendations of the Technical Consultation. Public Health Nutr. 2007, 10, 1606–1611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmermann, M.B.; Gizak, M.; Abbott, K.; Andersson, M.; Lazarus, J.H. Iodine deficiency in pregnant women in Europe. Lancet Diabetes Endocrinol. 2015, 3, 672–674. [Google Scholar] [CrossRef]
- Caldwell, K.L.; Pan, Y.; Mortensen, M.E.; Makhmudov, A.; Merrill, L.; Moye, J. Iodine status in pregnant women in the National Children’s Study and in U.S. women (15–44 years), National Health and Nutrition Examination Survey 2005–2010. Thyroid 2013, 23, 927–937. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.; Brown, R.S.; Daumerie, C.; Hubalewska-Dydejczyk, A.; Negro, R.; Vaidya, B. 2014 European thyroid association guidelines for the management of subclinical hypothyroidism in pregnancy and in children. Eur. Thyroid. J. 2014, 3, 76–94. [Google Scholar] [CrossRef] [Green Version]
- Alexander, E.K.; Pearce, E.N.; Brent, G.A.; Brown, R.S.; Chen, H.; Dosiou, C.; Grobman, W.A.; Laurberg, P.; Lazarus, J.H.; Mandel, S.J.; et al. 2017 Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and the Postpartum. Thyroid 2017, 27, 315–389. [Google Scholar] [CrossRef] [Green Version]
- De Groot, L.; Abalovich, M.; Alexander, E.K.; Amino, N.; Barbour, L.; Cobin, R.H.; Eastman, C.J.; Lazarus, J.H.; Luton, D.; Mandel, S.J.; et al. Management of thyroid dysfunction during pregnancy and postpartum: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2012, 97, 2543–2565. [Google Scholar] [CrossRef] [Green Version]
- Limbert, E.; Prazeres, S.; Sao Pedro, M.; Madureira, D.; Miranda, A.; Ribeiro, M.; Jacome de Castro, J.; Carrilho, F.; Oliveira, M.J.; Reguengo, H.; et al. Iodine intake in Portuguese pregnant women: Results of a countrywide study. Eur. J. Endocrinol. 2010, 163, 631–635. [Google Scholar] [CrossRef] [Green Version]
- Direção-Geral da Saúde (DGS). Orientação da Direção-Geral da Saúde. Aporte de Iodo em Mulheres na Preconceção, Gravidez e Amamentação. Available online: http://www.dgs.pt/?cr=24648 (accessed on 5 March 2022).
- Limbert, E.; Prazeres, S.; Sao Pedro, M.; Madureira, D.; Miranda, A.; Ribeiro, M.; Carrilho, F.; Jacome de Castro, J.; Lopes, M.S.; Cardoso, J.; et al. Iodine intake in Portuguese school children. Acta Med. Port. 2012, 25, 29–36. [Google Scholar]
- Gnat, D.; Dunn, A.D.; Chaker, S.; Delange, F.; Vertongen, F.; Dunn, J.T. Fast colorimetric method for measuring urinary iodine. Clin. Chem. 2003, 49, 186–188. [Google Scholar] [CrossRef] [Green Version]
- Bath, S.C. The effect of iodine deficiency during pregnancy on child development. Proc. Nutr. Soc. 2019, 78, 150–160. [Google Scholar] [CrossRef]
- Zimmermann, M.B.; Andersson, M. Global Endocrinology: Global perspectives in endocrinology: Coverage of iodized salt programs and iodine status in 2020. Eur. J. Endocrinol. 2021, 185, R13–R21. [Google Scholar] [CrossRef] [PubMed]
- Robinson, S.M.; Crozier, S.R.; Miles, E.A.; Gale, C.R.; Calder, P.C.; Cooper, C.; Inskip, H.M.; Godfrey, K.M. Preconception Maternal Iodine Status Is Positively Associated with IQ but Not with Measures of Executive Function in Childhood. J. Nutr. 2018, 148, 959–966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, P.N.; Okosieme, O.E.; Dayan, C.M.; Lazarus, J.H. Therapy of endocrine disease: Impact of iodine supplementation in mild-to-moderate iodine deficiency: Systematic review and meta-analysis. Eur. J. Endocrinol. 2014, 170, R1–R15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volzke, H.; Caron, P.; Dahl, L.; de Castro, J.J.; Erlund, I.; Gaberscek, S.; Gunnarsdottir, I.; Hubalewska-Dydejczyk, A.; Ittermann, T.; Ivanova, L.; et al. Ensuring Effective Prevention of Iodine Deficiency Disorders. Thyroid 2016, 26, 189–196. [Google Scholar] [CrossRef]


{kind=link}
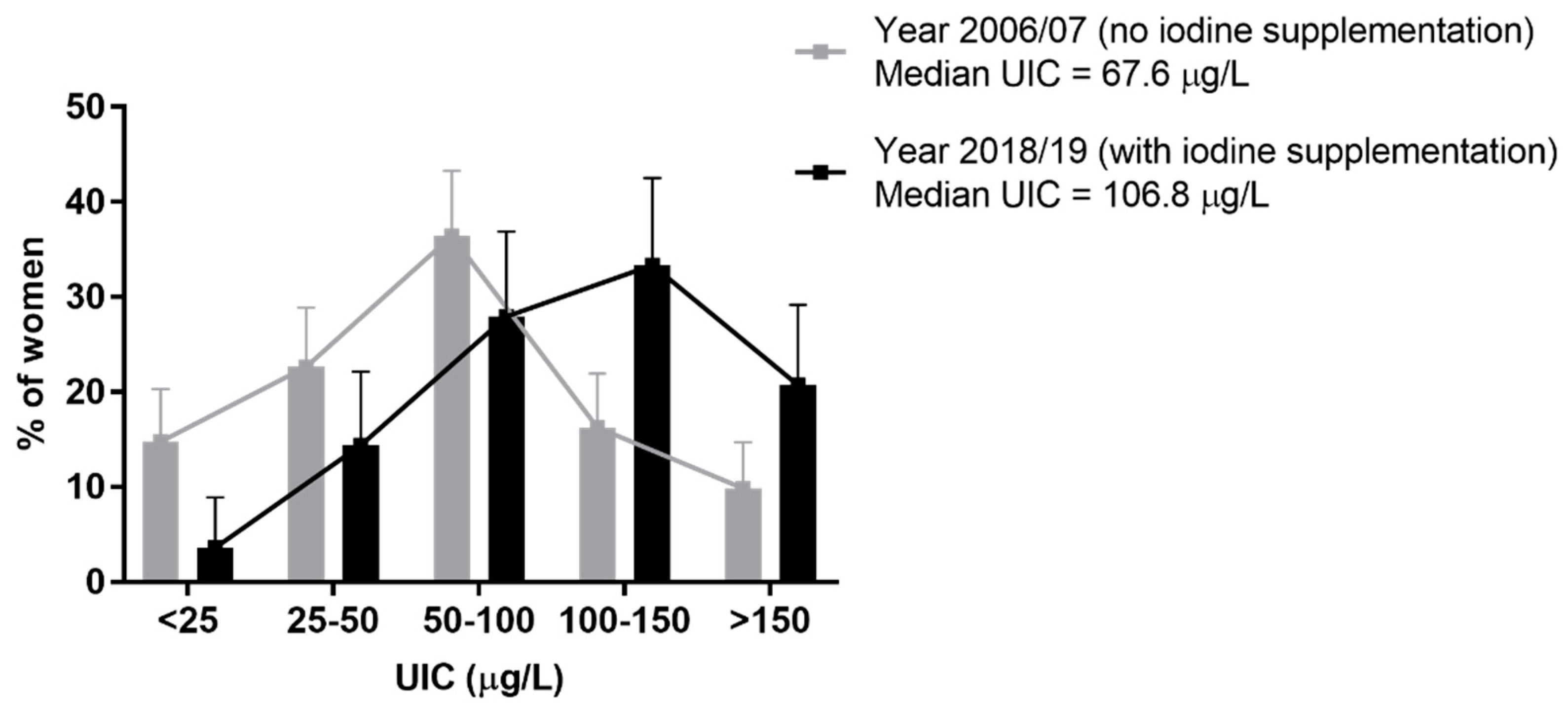
| Year 2006/07 (No Iodine Supplementation) (n = 203; Median UIC = 67.6 µg/L) | Year 2018/19 (No Iodine Supplementation) (n = 25; Median UIC = 50.0 µg/L) | Year 2018/19 (200 µg/Day Iodine Supplementation) (n = 111; Median UIC = 106.8 µg/L) | |
|---|---|---|---|
| UIC (µg/L) | n (%) | n (%) | n (%) |
| <25 | 30 (14.8) | 5 (20.0) | 4 (3.6) |
| 25–50 | 46 (22.7) | 8 (32.0) | 16 (14.4) |
| 50–100 | 74 (36.5) | 4 (16.0) | 31 (27.9) |
| 100–150 | 33 (16.3) | 8 (32.0) | 37 (33.3) |
| 150–200 | 12 (5.9) | 0 | 3 (2.7) |
| 200–300 | 8 (3.9) | 0 | 20 (18.0) |
| p < 0.0001 (a) | |||
| <50 | 76 (37.4) | 13 (52.0) | 20 (18.0) |
| p = 0.0002 (b)/p = 0.0008 (c) | |||
| >150 | 20 (9.9) | 0 | 23 (20.7) |
| p = 0.0069 (b)/p = 0.0058 (c) |
| Gestation Trimester | UIC (µg/L) | Year 2006/07 (No Iodine Supplementation) | Year 2018/19 (No Iodine Supplementation) | Year 2018/19 (200 µg/Day Iodine Supplementation) |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||
| First | <50 | 6 (30.0) | 2 (40.0) | 1 (16.7) |
| 50–150 | 10 (50.0) | 3 (60.0) | 3 (50.0) | |
| >150 | 4 (20.0) | 0 | 2 (33.3) | |
| (median UIC = 78.6 µg/L) | (median UIC = 116.7 µg/L) | (median UIC = 125.0 µg/L) | ||
| Second | <50 | 16 (30.2) | 5 (62.5) | 7 (18.9) (a) |
| 50–150 | 33 (62.3) | 3 (37.5) | 21 (56.8) | |
| >150 | 4 (7.5) | 0 | 9 (24.3) (b) | |
| (median UIC = 73.9 µg/L) | (median UIC = 43.8 µg/L) | (median UIC = 109.1 µg/L) | ||
| Third | <50 | 52 (41.9) | 6 (50.0) | 12 (17.6) (c, d) |
| 50–150 | 60 (48.4) | 6 (50.0) | 44 (64.7) | |
| >150 | 12 (9.7) | 0 | 12 (17.6) | |
| (median UIC = 62.2 µg/L) | (median UIC = 50.0 µg/L) | (median UIC = 101.5 µg/L) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lopes, C.A.; Prazeres, S.; Martinez-de-Oliveira, J.; Limbert, E.; Lemos, M.C. Iodine Supplementation in Pregnancy in an Iodine-Deficient Region: A Cross-Sectional Survey. Nutrients 2022, 14, 1393. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14071393
Lopes CA, Prazeres S, Martinez-de-Oliveira J, Limbert E, Lemos MC. Iodine Supplementation in Pregnancy in an Iodine-Deficient Region: A Cross-Sectional Survey. Nutrients. 2022; 14(7):1393. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14071393
Chicago/Turabian StyleLopes, Carla A., Susana Prazeres, José Martinez-de-Oliveira, Edward Limbert, and Manuel C. Lemos. 2022. "Iodine Supplementation in Pregnancy in an Iodine-Deficient Region: A Cross-Sectional Survey" Nutrients 14, no. 7: 1393. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14071393