
Gastrointestinal Symptoms in Autism Spectrum Disorder: A Systematic Review

 ,
,
Abstract
:1. Introduction
1.1. Gastrointestinal Symptoms in Autism Spectrum Disorder
1.2. Current Study
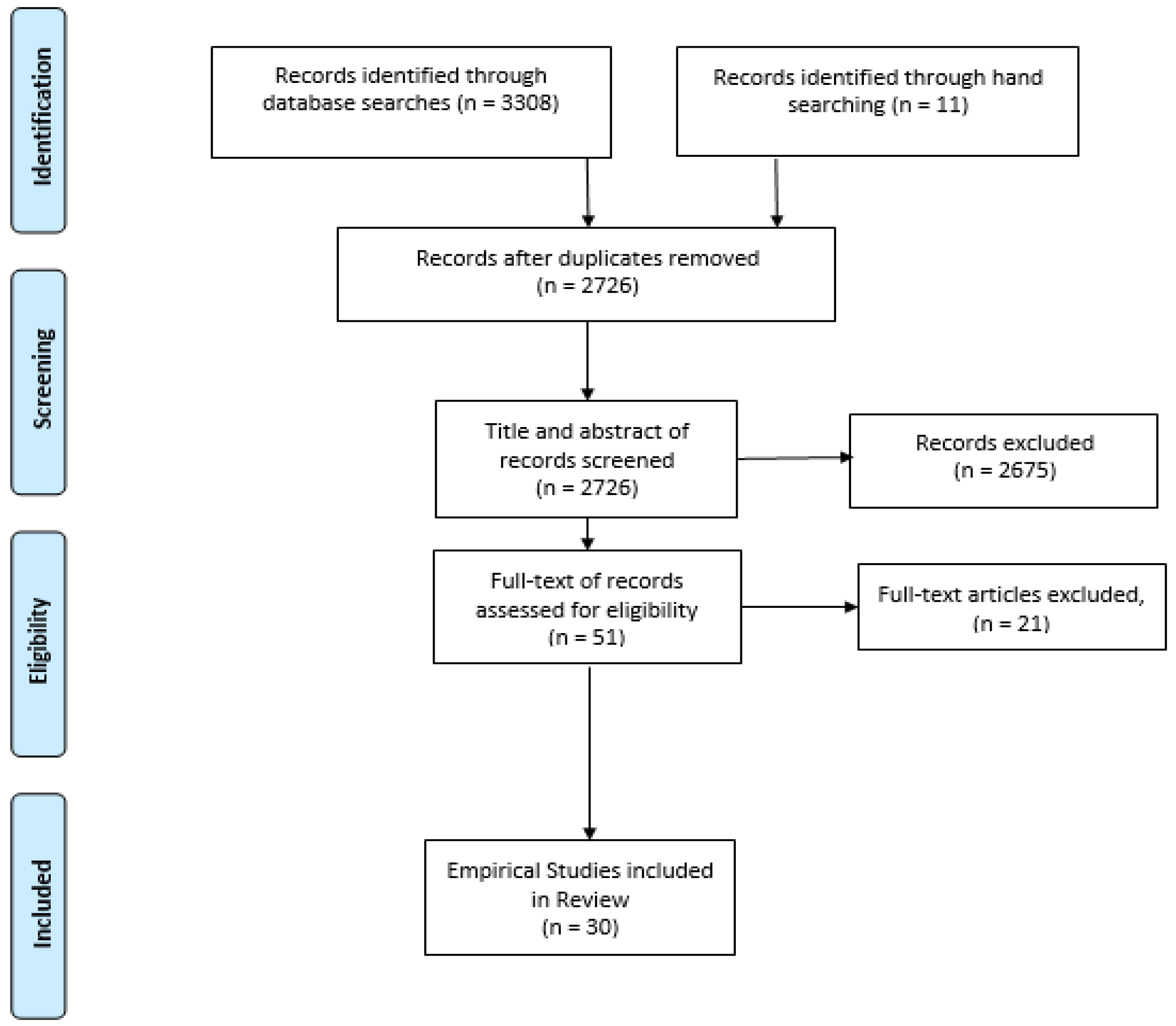
2. Materials and Methods
2.1. Search Procedures
2.2. Eligibility Criteria and Paper Selection Process
2.3. Quality Appraisal and Data Extraction
3. Results
3.1. Summary of Studies
3.2. The Prevalence and the Nature of GIS
3.3. GIS and ASD Severity
3.4. GIS and Regression
3.5. GIS and Language/Communication
3.6. GIS and Challenging Behavior
3.7. GIS and Comorbid Psychopathology
3.8. GIS and Sleep Problems
3.9. GIS and Sensory Issues
4. Discussion
4.1. Future Research
4.2. Review Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders: DSM-5; APA: Arlington, VA, USA, 2013. [Google Scholar]
- Matson, J.L.; Goldin, R.L. Comorbidity and autism: Trends, topics and future directions. Res. Autism Spectr. Disord. 2013, 7, 1228–1233. [Google Scholar] [CrossRef]
- Wasilewska, J.; Klukowski, M. Gastrointestinal symptoms and autism spectrum disorder: Links and risks—A possible new overlap syndrome. Pediatric Health Med. Ther. 2015, 6, 153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mannion, A.; Leader, G. Gastrointestinal symptoms in autism spectrum disorder: A literature review. Rev. J. Autism Dev. Disord. 2014, 1, 11–17. [Google Scholar] [CrossRef] [Green Version]
- Jyonouchi, H. Autism spectrum disorders and allergy: Observation from a pediatric allergy/immunology clinic. Expert Rev. Clin. Immunol. 2010, 6, 397–411. [Google Scholar] [CrossRef]
- Buie, T.; Campbell, D.B.; Fuchs, G.J.; Furuta, G.T.; Levy, J.; VandeWater, J.; Whitaker, A.H.; Atkins, D.; Bauman, M.L.; Beaudet, A.L. Evaluation, diagnosis, and treatment of gastrointestinal disorders in individuals with ASDs: A consensus report. Pediatrics 2010, 125, S1–S18. [Google Scholar] [CrossRef] [Green Version]
- Madra, M.; Ringel, R.; Margolis, K.G. Gastrointestinal issues and autism spectrum disorder. Child Adolesc. Psychiatr. Clin. N. Am. 2020, 29, 501–513. [Google Scholar] [CrossRef]
- Chaidez, V.; Hansen, R.L.; Hertz-Picciotto, I. Gastrointestinal problems in children with autism, developmental delays or typical development. J. Autism Dev. Disord. 2014, 44, 1117–1127. [Google Scholar] [CrossRef] [Green Version]
- Mannion, A.; Leader, G. An analysis of the predictors of comorbid psychopathology, gastrointestinal symptoms and epilepsy in children and adolescents with autism spectrum disorder. Res. Autism Spectr. Disord. 2013, 7, 1663–1671. [Google Scholar] [CrossRef] [Green Version]
- Williams, K.C.; Fuchs, G.J.; Furuta, G.T.; Marcon, M.A.; Coury, D.L. 511 Clinical Features Associated With GI Symptoms in Autism Spectrum Disorders (ASD). Gastroenterology 2010, 5, S-74. [Google Scholar] [CrossRef]
- Mazurek, M.O. Loneliness, friendship, and well-being in adults with autism spectrum disorders. Autism 2014, 18, 223–232. [Google Scholar] [CrossRef]
- Hsiao, E.Y. Gastrointestinal issues in autism spectrum disorder. Harv. Rev. Psychiatry 2014, 22, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Troisi, J.; Autio, R.; Beopoulos, T.; Bravaccio, C.; Carraturo, F.; Corrivetti, G.; Cunningham, S.; Devane, S.; Fallin, D.; Fetissov, S. Genome, Environment, Microbiome and Metabolome in Autism (GEMMA) Study Design: Biomarkers Identification for Precision Treatment and Primary Prevention of Autism Spectrum Disorders by an Integrated Multi-Omics Systems Biology Approach. Brain Sci. 2020, 10, 743. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, B.J.; Dovgan, K.; Takahashi, N.; Beversdorf, D.Q. The relationship among gastrointestinal symptoms, problem behaviors, and internalizing symptoms in children and adolescents with autism spectrum disorder. Front. Psychiatry 2019, 10, 194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crane, L.; Batty, R.; Adeyinka, H.; Goddard, L.; Henry, L.A.; Hill, E.L. Autism diagnosis in the United Kingdom: Perspectives of autistic adults, parents and professionals. J. Autism Dev. Disord. 2018, 48, 3761–3772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brereton, A.V. Regression in Autism. ACT NOW Autism Consult. Train. Now 2012. Available online: http://www.timeforafuture.com.au/factsheets/Regression%20in%20Autism.pdf (accessed on 20 January 2022).
- Valicenti-McDermott, M.D.; McVicar, K.; Cohen, H.J.; Wershil, B.K.; Shinnar, S. Gastrointestinal symptoms in children with an autism spectrum disorder and language regression. Pediatric Neurol. 2008, 39, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Chandler, S.; Carcani-Rathwell, I.; Charman, T.; Pickles, A.; Loucas, T.; Meldrum, D.; Simonoff, E.; Sullivan, P.; Baird, G. Parent-reported gastro-intestinal symptoms in children with autism spectrum disorders. J. Autism Dev. Disord. 2013, 43, 2737–2747. [Google Scholar] [CrossRef] [Green Version]
- Molloy, C.A.; Manning-Courtney, P. Prevalence of chronic gastrointestinal symptoms in children with autism and autistic spectrum disorders. Autism 2003, 7, 165–171. [Google Scholar] [CrossRef]
- Gorrindo, P.; Williams, K.C.; Lee, E.B.; Walker, L.S.; McGrew, S.G.; Levitt, P. Gastrointestinal dysfunction in autism: Parental report, clinical evaluation, and associated factors. Autism Res. 2012, 5, 101–108. [Google Scholar] [CrossRef]
- Williams, K.C.; Christofi, F.L.; Clemmons, T.; Rosenberg, D.; Fuchs, G.J. 342 chronic GI symptoms in children with autism spectrum disorders are associated with clinical anxiety. Gastroenterology 2012, 5, S-79–S-80. [Google Scholar] [CrossRef]
- Wang, L.W.; Tancredi, D.J.; Thomas, D.W. The prevalence of gastrointestinal problems in children across the United States with autism spectrum disorders from families with multiple affected members. J. Dev. Behav. Pediatrics 2011, 32, 351–360. [Google Scholar] [CrossRef]
- Harrison, R.; Jones, B.; Gardener, P.; Lawton, R. Quality assessment with diverse studies (QuADS): An appraisal tool for methodological and reporting quality in systematic reviews of mixed-or multi-method studies. BMC Health Serv. Res. 2021, 21, 144. [Google Scholar]
- Babinska, K.; Celusakova, H.; Belica, I.; Szapuova, Z.; Waczulikova, I.; Nemcsicsova, D.; Tomova, A.; Ostatnikova, D. Gastrointestinal symptoms and feeding problems and their associations with dietary interventions, food supplement use, and behavioral characteristics in a sample of children and adolescents with autism spectrum disorders. Int. J. Environ. Res. Public Health 2020, 17, 6372. [Google Scholar] [CrossRef] [PubMed]
- Schneider, C.K.; Melmed, R.D.; Barstow, L.E.; Enriquez, F.J.; Ranger-Moore, J.; Ostrem, J.A. Oral human immunoglobulin for children with autism and gastrointestinal dysfunction: A prospective, open-label study. J. Autism Dev. Disord. 2006, 36, 1053–1064. [Google Scholar] [CrossRef] [PubMed]
- Bresnahan, M.; Hornig, M.; Schultz, A.F.; Gunnes, N.; Hirtz, D.; Lie, K.K.; Magnus, P.; Reichborn-Kjennerud, T.; Roth, C.; Schjølberg, S. Association of maternal report of infant and toddler gastrointestinal symptoms with autism: Evidence from a prospective birth cohort. JAMA Psychiatry 2015, 72, 466–474. [Google Scholar] [CrossRef] [Green Version]
- Esposito, M.; Sloan, J.; Nappo, R.; Fadda, R.; Fotia, F.; Napoli, E.; Vicari, E. Sensory processing, gastrointestinal symptoms and parental feeding practices in the explanation of food selectivity: Clustering children with and without autism. Int. J. Autism Relat. Disabil. 2019, 2, 1. [Google Scholar]
- Badalyan, V.; Schwartz, R.H. Mealtime feeding behaviors and gastrointestinal dysfunction in children with classic autism compared with normal sibling controls. J. Pediatrics 2012, 2, 19868. [Google Scholar] [CrossRef] [Green Version]
- Fields, V.L.; Soke, G.N.; Reynolds, A.; Tian, L.H.; Wiggins, L.; Maenner, M.; DiGuiseppi, C.; Kral, T.V.; Hightshoe, K.; Ladd-Acosta, C. Association between pica and gastrointestinal symptoms in preschoolers with and without autism spectrum disorder: Study to Explore Early Development. Disabil. Health J. 2021, 14, 101052. [Google Scholar] [CrossRef]
- Fulceri, F.; Morelli, M.; Santocchi, E.; Cena, H.; Del Bianco, T.; Narzisi, A.; Calderoni, S.; Muratori, F. Gastrointestinal symptoms and behavioral problems in preschoolers with Autism Spectrum Disorder. Dig. Liver Dis. 2016, 48, 248–254. [Google Scholar] [CrossRef]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA Preschool Forms and Profiles; University of Vermont, Research Center for Children: Burlington, VT, USA, 2000; Volume 30. [Google Scholar]
- Ghalichi, F.; Ghaemmaghami, J.; Malek, A.; Ostadrahimi, A. Effect of gluten free diet on gastrointestinal and behavioral indices for children with autism spectrum disorders: A randomized clinical trial. World J. Pediatrics 2016, 12, 436–442. [Google Scholar] [CrossRef]
- Rasquin, A.; Di Lorenzo, C.; Forbes, D.; Guiraldes, E.; Hyams, J.S.; Staiano, A.; Walker, L.S. Childhood functional gastrointestinal disorders: Child/adolescent. Gastroenterology 2006, 130, 1527–1537. [Google Scholar] [CrossRef]
- Grimaldi, R.; Cela, D.; Swann, J.; Vulevic, J.; Gibson, G.; Tzortzis, G.; Costabile, A. In Vitro Fermentation of B-GOS: Impact on Faecal Bacterial Populations and Metabolic Activity in Autistic and Non-Autistic Children. Microbiol. Ecol. 2017, 93, 233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, S.J.; Heaton, K.W. Stool form scale as a useful guide to intestinal transit time. Scand. J. Gastroenterol. 1997, 32, 920–924. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Matson, J.L.; Cervantes, P.E.; Matheis, M.; Burns, C.O. Gastrointestinal issues in infants and children with autism and developmental delays. J. Dev. Phys. Disabil. 2017, 29, 407–417. [Google Scholar] [CrossRef]
- Kang, D.-W.; Adams, J.B.; Gregory, A.C.; Borody, T.; Chittick, L.; Fasano, A.; Khoruts, A.; Geis, E.; Maldonado, J.; McDonough-Means, S. Microbiota transfer therapy alters gut ecosystem and improves gastrointestinal and autism symptoms: An open-label study. Microbiome 2017, 5, 10. [Google Scholar] [CrossRef]
- Kang, D.W.; Adams, J.B.; Coleman, D.M.; Pollard, E.L.; Maldonado, J.; McDonough-Means, S.; Caporaso, J.G.; Krajmalnik-Brown, R. Long-term benefit of Microbiota Transfer Therapy on autism symptoms and gut microbiota. Sci. Rep. 2019, 9, 5821. [Google Scholar] [CrossRef]
- Revicki, D.A.; Wood, M.; Wiklund, I.; Crawley, J. Reliability and validity of the Gastrointestinal Symptom Rating Scale in patients with gastroesophageal reflux disease. Qual. Life Res. 1997, 7, 75–83. [Google Scholar] [CrossRef]
- Khalil, M.; Azouz, H.G.; Ahmed, S.A.; Gad, H.A.; Omar, O.M. Sensory Processing and Gastrointestinal Manifestations in Autism Spectrum Disorders: No Relation to Clostridium difficile. J. Mol. Neurosci. 2021, 71, 153–161. [Google Scholar] [CrossRef]
- Leader, G.; O’Reilly, M.; Gilroy, S.P.; Chen, J.L.; Ferrari, C.; Mannion, A. Comorbid feeding and gastrointestinal symptoms, challenging behavior, sensory issues, adaptive functioning and quality of life in children and adolescents with autism spectrum disorder. Dev. Neurorehabilit. 2021, 24, 35–44. [Google Scholar] [CrossRef]
- Network, A.T. GI Symptom Inventory Questionnaire; Version 3.0; Autism Speak: New York, NY, USA, 2005. [Google Scholar]
- Mannion, A.; Leader, G. An investigation of comorbid psychological disorders, sleep problems, gastrointestinal symptoms and epilepsy in children and adolescents with autism spectrum disorder: A two year follow-up. Res. Autism Spectr. Disord. 2016, 22, 20–33. [Google Scholar] [CrossRef] [Green Version]
- Mazefsky, C.A.; Schreiber, D.R.; Olino, T.M.; Minshew, N.J. The association between emotional and behavioral problems and gastrointestinal symptoms among children with high-functioning autism. Autism 2014, 18, 493–501. [Google Scholar] [CrossRef] [Green Version]
- McCue, L.M.; Flick, L.H.; Twyman, K.A.; Xian, H. Gastrointestinal dysfunctions as a risk factor for sleep disorders in children with idiopathic autism spectrum disorder: A retrospective cohort study. Autism 2017, 21, 1010–1020. [Google Scholar] [CrossRef] [PubMed]
- Neuhaus, E.; Bernier, R.A.; Tham, S.W.; Webb, S.J. Gastrointestinal and psychiatric symptoms among children and adolescents with autism spectrum disorder. Front. Psychiatry 2018, 9, 515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neumeyer, A.M.; Anixt, J.; Chan, J.; Perrin, J.M.; Murray, D.; Coury, D.L.; Bennett, A.; Farmer, J.; Parker, R.A. Identifying associations among co-occurring medical conditions in children with autism spectrum disorders. Acad. Pediatrics 2019, 19, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Prosperi, M.; Santocchi, E.; Balboni, G.; Narzisi, A.; Bozza, M.; Fulceri, F.; Apicella, F.; Igliozzi, R.; Cosenza, A.; Tancredi, R. Behavioral phenotype of ASD preschoolers with gastrointestinal symptoms or food selectivity. J. Autism Dev. Disord. 2017, 47, 3574–3588. [Google Scholar] [CrossRef]
- Prosperi, M.; Santocchi, E.; Muratori, F.; Narducci, C.; Calderoni, S.; Tancredi, R.; Morales, M.A.; Guiducci, L. Vocal and motor behaviors as a possible expression of gastrointestinal problems in preschoolers with Autism Spectrum Disorder. BMC Pediatrics 2019, 19, 466. [Google Scholar] [CrossRef]
- Restrepo, B.; Angkustsiri, K.; Taylor, S.L.; Rogers, S.J.; Cabral, J.; Heath, B.; Hechtman, A.; Solomon, M.; Ashwood, P.; Amaral, D.G. Developmental–behavioral profiles in children with autism spectrum disorder and co-occurring gastrointestinal symptoms. Autism Res. 2020, 13, 1778–1789. [Google Scholar] [CrossRef]
- Reynolds, A.M.; Soke, G.N.; Sabourin, K.R.; Croen, L.A.; Daniels, J.L.; Fallin, M.D.; Kral, T.V.; Lee, L.-C.; Newschaffer, C.J.; Pinto-Martin, J.A. Gastrointestinal Symptoms in 2-to 5-Year-Old Children in the Study to Explore Early Development. J. Autism Dev. Disord. 2021, 51, 3806–3817. [Google Scholar] [CrossRef]
- Rose, D.R.; Yang, H.; Serena, G.; Sturgeon, C.; Ma, B.; Careaga, M.; Hughes, H.K.; Angkustsiri, K.; Rose, M.; Hertz-Picciotto, I. Differential immune responses and microbiota profiles in children with autism spectrum disorders and co-morbid gastrointestinal symptoms. Brain Behav. Immun. 2018, 70, 354–368. [Google Scholar] [CrossRef]
- Sanctuary, M.R.; Kain, J.N.; Chen, S.Y.; Kalanetra, K.; Lemay, D.G.; Rose, D.R.; Yang, H.T.; Tancredi, D.J.; German, J.B.; Slupsky, C.M. Pilot study of probiotic/colostrum supplementation on gut function in children with autism and gastrointestinal symptoms. PLoS ONE 2019, 14, e0210064. [Google Scholar] [CrossRef]
- Shaaban, S.Y.; El Gendy, Y.G.; Mehanna, N.S.; El-Senousy, W.M.; El-Feki, H.S.A.; Saad, K.; El-Asheer, O.M. The role of probiotics in children with autism spectrum disorder: A prospective, open-label study. Nutr. Neurosci. 2018, 21, 676–681. [Google Scholar] [CrossRef]
- Thulasi, V.; Steer, R.A.; Monteiro, I.M.; Ming, X. Overall severities of gastrointestinal symptoms in pediatric outpatients with and without autism spectrum disorder. Autism 2019, 23, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Tomova, A.; Husarova, V.; Lakatosova, S.; Bakos, J.; Vlkova, B.; Babinska, K.; Ostatnikova, D. Gastrointestinal microbiota in children with autism in Slovakia. Physiol. Behav. 2015, 138, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Vargason, T.; McGuinness, D.L.; Hahn, J. Gastrointestinal symptoms and oral antibiotic use in children with autism spectrum disorder: Retrospective analysis of a privately insured US population. J. Autism Dev. Disord. 2019, 49, 647–659. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.; Leader, G.; Mannion, A.; Chen, J. An investigation of anxiety in children and adolescents with autism spectrum disorder. Res. Autism Spectr. Disord. 2015, 10, 30–40. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.-L.; Liang, S.; Zou, M.-Y.; Sun, C.-H.; Han, P.-P.; Jiang, X.-T.; Xia, W.; Wu, L.-J. Are gastrointestinal and sleep problems associated with behavioral symptoms of autism spectrum disorder? Psychiatry Res. 2018, 259, 229–235. [Google Scholar] [CrossRef]
- Zickgraf, H.; Mayes, S.D. Psychological, health, and demographic correlates of atypical eating behaviors in children with autism. J. Dev. Phys. Disabil. 2019, 31, 399–418. [Google Scholar] [CrossRef]
- Lindgren, S.D.; Koeppl, G.K. Assessing child behavior problems in a medical setting: Development of the Pediatric Behavior Scale. Adv. Behav. Assess. Child. Fam. 1987, 3, 57–90. [Google Scholar]
- Le Couteur, A.; Rutter, M.; Lord, C.; Rios, P.; Robertson, S.; Holdgrafer, M.; McLennan, J. Autism diagnostic interview: A standardized investigator-based instrument. J. Autism Dev. Disord. 1989, 19, 363–387. [Google Scholar] [CrossRef]
- Lord, C.; Rutter, M.; Le Couteur, A. Autism Diagnostic Interview-Revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. J. Autism Dev. Disord. 1994, 24, 659–685. [Google Scholar] [CrossRef]
- Dunn, W. Sensory Profile: User’s Manual; Psychological Corp.: San Antonio, TX, USA, 1999. [Google Scholar]
- Nikolov, R.N.; Bearss, K.E.; Lettinga, J.; Erickson, C.; Rodowski, M.; Aman, M.G.; McCracken, J.T.; McDougle, C.J.; Tierney, E.; Vitiello, B. Gastrointestinal symptoms in a sample of children with pervasive developmental disorders. J. Autism Dev. Disord. 2009, 39, 405–413. [Google Scholar] [CrossRef]
- Niehus, R.; Lord, C. Early medical history of children with autism spectrum disorders. J. Dev. Behav. Pediatrics 2006, 27, S120–S127. [Google Scholar] [CrossRef] [PubMed]
- Mazurek, M.O.; Kanne, S.M.; Wodka, E.L. Physical aggression in children and adolescents with autism spectrum disorders. Res. Autism Spectr. Disord. 2013, 7, 455–465. [Google Scholar] [CrossRef]
- Maenner, M.J.; Arneson, C.L.; Levy, S.E.; Kirby, R.S.; Nicholas, J.S.; Durkin, M.S. Brief report: Association between behavioral features and gastrointestinal problems among children with autism spectrum disorder. J. Autism Dev. Disord. 2012, 42, 1520–1525. [Google Scholar] [CrossRef] [PubMed]
- Khanijow, V.; Prakash, P.; Emsellem, H.A.; Borum, M.L.; Doman, D.B. Sleep dysfunction and gastrointestinal diseases. Gastroenterol. Hepatol. 2015, 11, 817. [Google Scholar]
- Cremonini, F.; Camilleri, M.; Zinsmeister, A.R.; Herrick, L.M.; Beebe, T.; Talley, N.J. Sleep disturbances are linked to both upper and lower gastrointestinal symptoms in the general population. Neurogastroenterol. Motil. 2009, 21, 128–135. [Google Scholar] [CrossRef] [Green Version]
- Taylor, D.J.; Mallory, L.J.; Lichstein, K.L.; Durrence, H.H.; Riedel, B.W.; Bush, A.J. Comorbidity of chronic insomnia with medical problems. Sleep 2007, 30, 213–218. [Google Scholar] [CrossRef]
- Thenhausen, N.; Kuss, M.; Wiater, A.; Schlarb, A.A. Sleep problems in adolescents with Asperger syndrome or high-functioning autism. Somnologie 2017, 21, 28–36. [Google Scholar] [CrossRef]
- Kelmanson, I.A. Sleep disturbances and their associations with emotional/behavioural problems in 5-year-old boys with autism spectrum disorders. Early Child Dev. Care 2018, 190, 236–251. [Google Scholar] [CrossRef]
- Lyu, J.; Ye, X.; Chen, Y.; Xia, Y.; Zhu, J.; Tong, S.; Yin, Y.; Qu, J.; Li, S. Children’s Sleep May Depend on Maternal Sleep Duration During Pregnancy: A Retrospective Study. Nat. Sci. Sleep 2020, 12, 197. [Google Scholar] [CrossRef] [Green Version]
- Verhoeff, M.E.; Blanken, L.M.; Kocevska, D.; Mileva-Seitz, V.R.; Jaddoe, V.W.; White, T.; Verhulst, F.; Luijk, M.P.; Tiemeier, H. The bidirectional association between sleep problems and autism spectrum disorder: A population-based cohort study. Mol. Autism 2018, 9, 8. [Google Scholar] [CrossRef] [Green Version]
- McElhanon, B.O.; McCracken, C.; Karpen, S.; Sharp, W.G. Gastrointestinal Symptoms in Autism Spectrum Disorder: A Meta-analysis. Pediatrics 2014, 133, 872–883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quan, J.; Panaccione, N.; Jeong, J.; Underwood, F.E.; Coward, S.; Windsor, J.W.; Ronksley, P.E.; Gidrewicz, D.; de Bruyn, J.; Turner, J.M.; et al. Association Between Celiac Disease and Autism Spectrum Disorder: A Systematic Review. J Pediatr. Gastroenterol. Nutr. 2021, 72, 704–711. [Google Scholar] [CrossRef] [PubMed]
- Prosperi, M.; Santocchi, E.; Brunori, E.; Cosenza, A.; Tancredi, R.; Muratori, F.; Calderoni, S. Prevalence and Clinical Features of Celiac Disease in a Cohort of Italian Children with Autism Spectrum Disorders. Nutrients 2021, 13, 3046. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Chen, X.; Zhang, J.; Tong, G.; Sun, Y. Association of food hypersensitivity in children with the risk of autism spectrum disorder: A meta-analysis. Eur. J. Pediatr. 2021, 180, 999–1008. [Google Scholar] [CrossRef]
- Kushak, R.I.; Winter, H.S. Intestinal microbiota, metabolome and gender dimorphism in autism spectrum disorders. Res. Autism Spectr. Disord. 2018, 49, 65–74. [Google Scholar] [CrossRef]
- Hyman, S.L.; Levy, S.E.; Myers, S.M. Identification, evaluation, and management of children with autism spectrum disorder. Pediatrics 2020, 145, e20193447. [Google Scholar] [CrossRef] [Green Version]
- Sathe, N.; Andrews, J.C.; McPheeters, M.; Warren, Z.E. Nutritional and Dietary Interventions for Autism Spectrum Disorder: A Systematic Review. Pediatrics 2017, 139, e20170346. [Google Scholar] [CrossRef]
- Salvatore, S.; Pensabene, L.; Borrelli, O.; Saps, M.; Thapar, N.; Concolino, D.; Staiano, A.; Vandenplas, Y. Mind the gut: Probiotics in Paediatric Neurogastroenterology. Benef. Microbes 2018, 9, 883–898. [Google Scholar] [CrossRef]


{kind=link}
| Study ID | Study Design | Aim(s) | Sample–Size and Age | Measure of GI Symptoms | Results | QuADS Result |
|---|---|---|---|---|---|---|
| Babinska et al. [24] | Case-control study | Investigated the prevalence and types of GIS, frequency of food selectivity, mealtime difficulties. | n = 247 (ASD) n = 267 (TD) 2–18 years | GI severity index questionnaire [25]. | Higher prevalence GIS in autistic girls than boys. High rates food selectivity 69.1% and mealtime difficulties 64.3%. Weak but significant correlation of behavior characteristics with GIS frequency, | 21 |
| Bresnahan et al. [26] | Cohort Study | Investigated GIS frequency in children registered in Norwegian Mother & Child study, and when these present during first 3 years of life. | n = 195 (ASD) n = 4636 (DD) n = 4095 (TD) 6–36 months | Study Maternal report questionnaires. | Mothers of children with ASD were significantly more likely to report constipation, food allergy/intolerance in the 6–18 month and diarrhea, constipation and food allergy/intolerance in the 18–36 month periods. | 29 |
| Chaidez, et al. [8] | Population-based case-control study | Compared GI problems in children registered in the CHARGE study examining the relationship between GIS and maladaptive behaviors. | n = 499 (ASD) n = 137 (DD) n = 324 (TD) 24–60 months | CHARGE GI questionnaire | Children with more severe ASD had 10% more frequent diarrhea than those with less severe ASD. ASD children more likely to have at least on frequent GIS than TD. Maladaptive behaviors correlate with GIS. | 21 |
| Esposito et al. [27] | Case-control study | To clarify key factors associated with food selectivity. | n = 41 (ASD) n = 48 (TD) 25–98 months | Questionnaire interviews [28] | Parenting style, sensory anomalies, and GIS were associated with food refusal of children. Presence of GIS were associated with hypersensitivity to smell, and moving visual stimuli in ASD children. | 26 |
| Ferguson et al. [14] | Cohort study | Examined the relationship between GIS, problem behaviors and internalizing symptoms in children with ASD and adolescents. | n = 340 (ASD) 2–18 years | Questionnaires completed at clinic visits by caregivers | Aggression was a predictor of nausea in younger children. Older children with anxiety were 11% more likely to have constipation, 9% less likely to have stomachaches. | 23 |
| Fields et al. [29] | Case-control study | Examined the relationship between Pica, GIS, and ASD. | n = 1244 (ASD) n = 1593 (DD) n = 1487 (TD) 2–5 years | Parental information on health history | Pica was associated with vomiting, diarrhea, and loose stools in all groups. Without pica, increased GIS is still evident in ASD. | 19 |
| Fulceri et al. [30] | Population-based case-control study | Explored the type and the prevalence of GIS in ASD, TD controls, and investigated their association with behavioral problems. | n = 115 (ASD) mean (SD) age = 3.8 (1.1) years and n = 115 (TD) | Somatic Scale of Child Behavior Check List 1.5–5 [31] | ASD children with GIS had more anxiety problems, somatic complaints, externalizing, and total problems than those without GIS. | 32 |
| Ghalichi, et al. [32] | RCT open design | Investigated the effect of a gluten-free diet on GIS and behavior in ASD children. | n = 80 (ASD) 4–16 years | ROME III questionnaire [33] | GI abnormalities in 53.9%. In the gluten-free diet group, the prevalence of GIS decreased significantly to 17.10%. Gluten-free diet resulted in a significant decrease in behavioral disorders (80.03 ± 14.07 vs. 75.82 ± 15.37, p < 0.05). | 26 |
| Grimaldi et al. [34] | RCT double-blind | Investigated effect of exclusion diet and prebiotic on gut microbiota, metabolism and behavior. | n = 30 (ASD) 4–11 years | GIS symptom Diaries Bristol Stool Chart [35] | Significant changes in GIS due to prebiotic, metabolism, and reduction in antisociability scores. | 21 |
| Jiang et al. [36] | Case-control study | Investigated the association between GIS and ASD symptom severity and developmental functioning. | n = 28 (ASD + GIS) n = 28 (ASD) n = 28 (DD) n = −28 (DD + GIS) 17–37 months | Study clinical information questionnaire. | Although the prevalence of GIS was higher in participants with ASD than those without, this difference was not significant. GIS were unrelated to ASD symptom severity or developmental functioning. | 23 |
| Kang et al. [37] Kang et al. [38] | Open-label clinical trial | Investigated the safety and tolerability of microbiota transfer therapy and its effects on microbiota, GIS, and other ASD-related symptoms. | n = 18 (ASD) 7–17 years | The GI Symptom Rating Scale [39]. | Reduction of 80% and 23% of GIS and ASD severity, respectively, after treatment. Significant improvements in constipation, diarrhea, indigestion, and abdominal pain. Improvements maintained at 8 weeks, and 2-year follow-ups. | 22 |
| Khalil et al. [40] | Case-control study | Assessed Clostridium difficile in the stool & its relation to GI comorbidities, ASD severity, and sensory impairment. | n = 58 (ASD) n = 45 (TD siblings) n = 45 (controls) 3–10 years | Short Version of GI Severity Index; 6-GSI Questionnaire [25]. | No statistically significant difference between groups in Clostridium difficile, qualitative, quantitative, and toxin production results. Sensory symptoms and GIS are common comorbidities in ASD. | 26 |
| Leader et al. [41] | Cohort study | Investigated frequency of feeding problems and their relationship to GIS, challenging behavior, sensory problems and comorbid psychopathology. | n = 136 (ASD) 3–17 years | GI Symptom Inventory [42]. | Food selectivity was present in 84.6% of the sample. Participants with feeding problems had a higher rate GIS and of challenging behavior and sensory issues. | 23 |
| Mannion & Leader [43] | Cohort study | Examined change in comorbid symptoms of ASD over two years and the relationship between symptoms, family medical history, including autoimmune diseases. | n = 56 (ASD) 5–19 years | GI Symptom Inventory [42] | GIS persisted in 84.4% of participants and 92.9% had family history of autoimmune disease. | 29 |
| Mazefsky, et al. [44] | Cohort study | Explored the association between GIS and emotional behavior concerns in children with ASD without intellectual disability (ID). | n = 95 (ASD) 7–19 years | GI Symptom Inventory [42]. | Participants with/without GIS did not differ regarding adaptive behavior, or total internalizing or externalizing problem scores but those with GIS had significantly higher levels of affective problems. | 27 |
| McCue, et al. [45] | Retrospective cohort study | Investigated whether GI dysfunctions increased the odds of sleep disorders in children with idiopathic ASD. | n = 610 (ASD) 2–18 years | Autism Genetic Resource Exchange Data Source, 2013. | Sign more sleep disorder s/s for children with GI problems (64.1%; 150/234) than for those without GI problems (50.8%; 156/307). | 24 |
| Neuhaus, et al. [46] | Cohort study | Explored the relationship between GI concerns and psychiatric symptoms in children and adolescents with ASD | n = 2756 (ASD) 4–18 years | Parental interviews relating to GI concerns. | Higher levels of psychiatric symptoms were associated with more ASD symptoms, higher verbal IQ, lower family income, and lower adaptive behavior skills. GIS accounted for unique variance in psychiatric outcomes over &above these factors. | 26 |
| Neumeyer et al. [47] | Cohort study | Identified associations among co-occurring medical conditions in children with ASD spectrum disorders. | n = 2114 (17 months–5 years) n = 1221 (6–17 years) | Somatic Scale of Child Behavior Checklist (CBCL/1½–5) [31]. | Confirmed association between sleep disorders and anxiety symptoms, in older children; Associations between feeding with sleep disorders (younger children only) and speech disorders; constipation with sleep disorders and speech disorders. | 26 |
| Prosperi et al. [48] | Cohort study | Investigated the prevalence and type of GIS and food selectivity (FS) problems and examined the association with ASD severity, cognitive ability, behavioral problems. | n = 163 (ASD) (20–71 months) | Somatic Scale of Child Behavior Checklist (CBCL/1½–5) [31]. | At least one severe GI symptom or FS in 40.5% of participants. Levels of behavioral problems were significantly different for participants with/without GIS and FS. No significant difference in the performance of IQ and autistic severity. | 25 |
| Prosperi et al. [49] | Observational case-control study | Investigated the presence and type of associated verbal and motor behaviors determined their correlation with GIS. | n = 85 (ASD) (2.18–6.11 years) | GI Severity Index [25]. | GIS group had 35% higher scores in behaviors than the non-GI group. | 22 |
| Restrepo et al. [50] | Cohort study | Examined the association of GIS with gender, developmental and behavioral measures. | n = 255 (ASD) n = 129 (TD) (2–3.5 years) | GI History (CHARGE GH) Questionnaire. [8] | Somatic complaints increased with number of GIS. Children with ASD and co-occurring GIS experienced more behavioral problems than individuals with ASD without GI concerns. | 25 |
| Reynolds et al. [51] | Case-control study | Evaluated associations between GIS and neurodevelopmental phenotypes. | n = 672 (ASD) n = 938 (DDs) n = 851 (TD) (2–5 years) | Study GI Questionnaire | Children with ASD with regression had increased odds of several GIS than ASD children without regression. | 25 |
| Rose et al. [52] | Cohort study | Investigated biological signatures to immune dysfunction and microbiota composition in ASD children with GIS. | n = 103 (ASD) (3–12 years) | CHARGE GI History [8]. | The ASD GI group produced increased mucosa-relevant cytokines compared to ASD no GI group. | 25 |
| Sanctuary et al. [53] | RCT double-blind | Assessed tolerability of combined probiotic-BCP supplement. | n = 8 (ASD) (2–11 years) | CHARGE GI History (Chaidex et al. 2014) | Five weeks of treatment was tolerated well. Children on both treatments saw a reduction in the frequency of certain GIS. | 30 |
| Shaaban et al. [54] | Prospective, open-label study | Evaluated the efficacy and tolerability of probiotic supplement. | n = 30 (ASD) (5–9 years) | GI Severity Index questionnaire [25]. | Reduced GIS after 3 months of therapy, which was well-tolerated. | 23 |
| Thuslai et al., [55] | Case-control study | Examined gastrointestinal symptoms in pediatric outpatients. | n = 135 (ASD) n = 146 (with and without GIS). | GI Severity Index questionnaire [25]. | The Gastrointestinal Severity Index was more effective in screening for gastrointestinal disorders in comparison. | 21 |
| Tomova et al. [56] | Pilot study | Examined changes in fecal microbiota and determined its role in the development of GI disorders. | n = 10 (ASD) n = 9 (TD siblings) n = 10 controls 2–9 years (ASD) 2–11 years (controls). | Study Parental Questionnaire. | The participants demonstrated strong positive correlation of ASD severity with the severity of GI dysfunction. | 21 |
| Vargason et al. [57] | Retrospective cohort study | Examined the association between early antibiotic use and the occurrence of later GIS. | n = 3253 (ASD) n = 278,370 (Controls). | Analyzed claims from US health insurer for antibiotic use and GI diagnosis. | More antibiotic prescriptions early in life were associated with increased rate of later GI diagnosis (adjusted hazard ratio 1.48; 95% confidence interval 1.34, 1.63) for children with and without ASD | 30 |
| Williams, et al. [58] | Cohort study | Examined the relationship between anxiety and GIS, sleep problems and challenging behavior. | n = 109 (ASD) 6–17 years | GI Symptom Inventory [42]. | Demographic factors, GIS, sleep problems, and challenging behavior accounted for 34% of the variance in anxiety. Sleep, severity of self-injurious behavior, age, and ID diagnosis are significant predictors. | 26 |
| Yang et al. [59] | Case-control study | Examined associations between GI and sleep problems, severity of ASD and behavioral symptoms. | n = 169 (ASD) n = 170 (TD) 3–12 years | Study Clinical Information Questionnaire | ASD + GIS associated with more severe ASD core symptoms than those without GIS. GIS were associated with maternal sleep problems in pregnancy, breast/formula feeding 0–6 months, and picky eating. | 23 |
| Zickgraf et al. [60] | Cohort study | Examined psychological, health, and demographic correlates of atypical eating. | n = 1112 (ASD) 1–17 years | Pediatric Behavior Scale [61]. | Found atypical eating behaviors in 70.5% of participants. These positively related to age (most common at ages 1–3), increasing ASD severity, poor appetite, and constipation. | 28 |
| Relationship | Factor | |
|---|---|---|
| No Association | Age [8,14,24] | |
| Contradictory Evidence | Positive Association [47] | Language and Communication Ability |
| No Association [49] | ||
| Positive Association [36,40,44,50] | ASD Severity | |
| No Association [37,38,52,56,59,60,62] | ||
| Positive Association [24,44] | Gender | |
| No Association [48,49,50] | ||
| Positive Association | Presence of ASD [8,24,26]. | |
| Regression in ASD [51]. | ||
| Comorbid Anxiety [30,58]. | ||
| Sensory Issues [27]. | ||
| Sleep Problems [45,47,51,59]. | ||
| Challenging Behaviors [14,29,32,44,48,50]. | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leader, G.; Abberton, C.; Cunningham, S.; Gilmartin, K.; Grudzien, M.; Higgins, E.; Joshi, L.; Whelan, S.; Mannion, A. Gastrointestinal Symptoms in Autism Spectrum Disorder: A Systematic Review. Nutrients 2022, 14, 1471. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14071471
Leader G, Abberton C, Cunningham S, Gilmartin K, Grudzien M, Higgins E, Joshi L, Whelan S, Mannion A. Gastrointestinal Symptoms in Autism Spectrum Disorder: A Systematic Review. Nutrients. 2022; 14(7):1471. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14071471
Chicago/Turabian StyleLeader, Geraldine, Cathal Abberton, Stephen Cunningham, Katie Gilmartin, Margo Grudzien, Emily Higgins, Lokesh Joshi, Sally Whelan, and Arlene Mannion. 2022. "Gastrointestinal Symptoms in Autism Spectrum Disorder: A Systematic Review" Nutrients 14, no. 7: 1471. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14071471