Suboptimal Iodine Concentration in Breastmilk and Inadequate Iodine Intake among Lactating Women in Norway

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population and Study Design
2.2. Collection of Breastmilk Samples
2.3. Collection of Urine Samples
2.4. Chemical Analyses
2.5. Iodine Intake from Food and Supplements
2.6. Definitions
2.7. Statistics
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| BMIC | Breast milk iodine concentration. |
| EAR | Estimated average requirement. |
| ID | Iodine deficiency. |
| UIC | Urinary Iodine Concentration. |
References
- Dold, S.; Zimmermann, M.B.; Aboussad, A.; Cherkaoui, M.; Jia, Q.; Jukic, T.; Kusic, Z.; Quirino, A.; Sang, Z.; San Luis, T.O.; et al. Breast milk iodine concentration is a more accurate biomarker of iodine status than urinary iodine concentration in exclusively breastfeeding women. J. Nutr. 2017, 147, 528–537. [Google Scholar] [CrossRef] [PubMed]
- Van den Hove, M.F.; Beckers, C.; Devlieger, H.; de Zegher, F.; De Nayer, P. Hormone synthesis and storage in the thyroid of human preterm and term newborns: Effect of thyroxine treatment. Biochimie 1999, 81, 563–570. [Google Scholar] [CrossRef]
- Azizi, F.; Smyth, P. Breastfeeding and maternal and infant iodine nutrition. Clin. Endocrinol. 2009, 70, 803–809. [Google Scholar] [CrossRef] [PubMed]
- Stinca, S.; Andersson, M.; Herter-Aeberli, I.; Chabaa, L.; Cherkaoui, M.; El Ansari, N.; Aboussad, A.; Weibel, S.; Zimmermann, M.B. Moderate-to-severe iodine deficiency in the “first 1000 days” causes more thyroid hypofunction in infants than in pregnant or lactating women. J. Nutr. 2017, 147, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Nazeri, P.; Zarghani, N.H.; Mirmiran, P.; Hedayati, M.; Mehrabi, Y.; Azizi, F. Iodine status in pregnant women, lactating mothers, and newborns in an area with more than two decades of successful iodine nutrition. Biol. Trace Elem. Res. 2016, 172, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.H. Iodine status in Europe in 2014. Eur. Thyroid J. 2014, 3, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B. Iodine deficiency. Endocr. Rev. 2009, 30, 376–408. [Google Scholar] [CrossRef] [PubMed]
- Andersson, M.; Karumbunathan, V.; Zimmermann, M.B. Global iodine status in 2011 and trends over the past decade. J. Nutr. 2012, 142, 744–750. [Google Scholar] [CrossRef] [PubMed]
- Bath, S.C.; Steer, C.D.; Golding, J.; Emmett, P.; Rayman, M.P. Effect of inadequate iodine status in UK pregnant women on cognitive outcomes in their children: Results from the Avon Longitudinal Study of Parents and Children (ALSPAC). Lancet 2013, 382, 331–337. [Google Scholar] [CrossRef]
- Manousou, S.; Dahl, L.; Heinsbaek Thuesen, B.; Hulthen, L.; Nystrom Filipsson, H. Iodine deficiency and nutrition in Scandinavia. Minerva Med. 2017, 108, 147–158. [Google Scholar] [PubMed]
- Nystrom, H.F.; Brantsaeter, A.L.; Erlund, I.; Gunnarsdottir, I.; Hulthen, L.; Laurberg, P.; Mattisson, I.; Rasmussen, L.B.; Virtanen, S.; Meltzer, H.M. Iodine status in the nordic countries—past and present. Food Nutr. Res. 2016. [Google Scholar] [CrossRef] [PubMed]
- Brantsaeter, A.L.; Abel, M.H.; Haugen, M.; Meltzer, H.M. Risk of suboptimal iodine intake in pregnant Norwegian women. Nutrients 2013, 5, 424–440. [Google Scholar] [CrossRef] [PubMed]
- Bath, S.C.; Rayman, M.P. Iodine deficiency in the UK: An overlooked cause of impaired neurodevelopment. Proc. Nutr. Soc. 2013, 72, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Rayman, M.P.; Bath, S.C. The new emergence of iodine deficiency in the UK: Consequences for child neurodevelopment. Ann. Clin. Biochem. 2015, 52, 705–708. [Google Scholar] [CrossRef] [PubMed]
- Dahl, L.; Meltzer, H.M.; Opsahl, J.A.; Julshamn, K. Iodine intake and status in two groups of Norwegians. Scand. J. Nutr. 2003, 47, 170–178. [Google Scholar] [CrossRef]
- Andersen, S.L.; Sorensen, L.K.; Krejbjerg, A.; Moller, M.; Laurberg, P. Iodine deficiency in Danish pregnant women. Dan. Med. J. 2013, 60, 4657. [Google Scholar]
- Granfors, M.; Andersson, M.; Stinca, S.; Akerud, H.; Skalkidou, A.; Poromaa, I.S.; Wikstrom, A.K.; Nystrom, H.F. Iodine deficiency in a study population of pregnant women in Sweden. Acta Obstet. Gynecol. Scand. 2015, 94, 1168–1174. [Google Scholar] [CrossRef] [PubMed]
- Dahl, L.; Meltzer, H.M. The iodine content of foods and diets: Norwegian perspectives. In Comprehensive Handbook of Iodine; Preedy, V.R., Burrow, G.N., Watson, R.R., Eds.; Academic Press: London, UK, 2009; pp. 345–352. [Google Scholar]
- Frey, H.; Rosenlund, B.; Try, K.; Theodorsen, L. Urinary Excretion of Iodine in Norway. Iodine Deficiency in Europe; Plenum Press: New York, NY, USA, 1993; pp. 297–300. [Google Scholar]
- Dahl, L.; Johansson, L.; Julshamn, K.; Meltzer, H.M. The iodine content of Norwegian foods and diets. Public Health Nutr. 2004, 7, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Dahl, L.; Opsahl, J.A.; Meltzer, H.M.; Julshamn, K. Iodine concentration in Norwegian milk and dairy products. Br. J. Nutr. 2003, 90, 679–685. [Google Scholar] [CrossRef] [PubMed]
- Brantsaeter, A.L.; Haugen, M.; Julshamn, K.; Alexander, J.; Meltzer, H.M. Evaluation of urinary iodine excretion as a biomarker for intake of milk and dairy products in pregnant women in the Norwegian mother and child cohort study (MoBa). Eur. J. Clin. Nutr. 2009, 63, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academies Press: Washington, DC, USA, 2001. [Google Scholar]
- Ma, Z.F.; Skeaff, S.A. Assessment of population iodine status. In Iodine Deficiency Disorders and Their Elimination; Pearce, E.N., Ed.; Springer International Publishing: Cham, Switzerland, 2017; pp. 15–28. [Google Scholar]
- Laurberg, P.; Andersen, S.L. Nutrition: Breast milk—A gateway to iodine-dependent brain development. Nat. Rev. Endocrinol. 2014, 10, 134–135. [Google Scholar] [CrossRef] [PubMed]
- The Norwegian Food Safety Authority. Matvaretabellen-The Norwegian Food Composition Table; The Norwegian Food Safety Authority; The Norwegian Directorate of Health; The University of Oslo: Oslo, Norway, 2016.
- Troan, G.; Dahl, L.; Meltzer, H.M.; Abel, M.H.; Indahl, U.G.; Haug, A.; Prestlokken, E. A model to secure a stable iodine concentration in milk. Food Nutr. Res. 2015, 59, 29829. [Google Scholar] [CrossRef] [PubMed]
- Kielland, E.; Dalane, J.Ø.; Håland, J.T.; Tharaldsen, A. Analyses of Eggs and Chicken, Nutrients and Environmental Contaminants 2016, in Norwegian; Technical Report; The Norwegian Food Safety Authority: Oslo, Norway, 2016.
- Semba, R.D.; Delange, F. Iodine in human milk: Perspectives for infant health. Nutr. Rev. 2001, 59, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Dietary Reference Intakes; National Academy Press: Washington, DC, USA, 2006. [Google Scholar]
- World Health Organization. Nutrient Adequacy of Exclusive Breastfeeding for the Term Infant during the First Six Months of Life; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- World Health Organization. Assessment of Iodine Deficiency Disorders and Monitoring Their Elimination; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Andersson, M.; de Benoist, B.; Delange, F.; Zupan, J. Prevention and control of iodine deficiency in pregnant and lactating women and in children less than 2-years-old: Conclusions and recommendations of the technical consultation. Public Health Nutr. 2007, 10, 1606–1611. [Google Scholar] [PubMed]
- Nordic Council of Ministers. Nordic Nutrition Recommendations 2012, 5th ed.; Nordic Council of Ministers: Copenhagen, Denmark, 2014. [Google Scholar]
- Zimmermann, M.B. Iodine deficiency in pregnancy and the effects of maternal iodine supplementation on the offspring: A review. Am. J. Clin. Nutr. 2009, 89, 668–672. [Google Scholar] [CrossRef] [PubMed]
- Moleti, M.; Trimarchi, F.; Tortorella, G.; Candia Longo, A.; Giorgianni, G.; Sturniolo, G.; Alibrandi, A.; Vermiglio, F. Effects of maternal iodine nutrition and thyroid status on cognitive development in offspring: A pilot study. Thyroid 2016, 26, 296–305. [Google Scholar] [CrossRef] [PubMed]
- Santiago-Fernandez, P.; Torres-Barahona, R.; Muela-Martinez, J.A.; Rojo-Martinez, G.; Garcia-Fuentes, E.; Garriga, M.J.; Leon, A.G.; Soriguer, F. Intelligence quotient and iodine intake: A cross-sectional study in children. J. Clin. Endocrinol. Metab. 2004, 89, 3851–3857. [Google Scholar] [CrossRef] [PubMed]
- Trumpff, C.; De Schepper, J.; Tafforeau, J.; Van Oyen, H.; Vanderfaeillie, J.; Vandevijvere, S. Mild iodine deficiency in pregnancy in Europe and its consequences for cognitive and psychomotor development of children: A review. J. Trace Elem. Med. Biol. 2013, 27, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Abel, M.H.; Caspersen, I.H.; Meltzer, H.M.; Haugen, M.; Brandlistuen, R.E.; Aase, H.; Alexander, J.; Torheim, L.E.; Brantsaeter, A.L. Suboptimal maternal iodine intake is associated with impaired child neurodevelopment at 3 years of age in the Norwegian mother and child cohort study. J. Nutr. 2017. [Google Scholar] [CrossRef] [PubMed]
- Dorea, J.G. Iodine nutrition and breast feeding. J. Trace Elem. Med. Biol. 2002, 16, 207–220. [Google Scholar] [CrossRef]
- Mulrine, H.M.; Skeaff, S.A.; Ferguson, E.L.; Gray, A.R.; Valeix, P. Breast-milk iodine concentration declines over the first 6 mo postpartum in iodine-deficient women. Am. J. Clin. Nutr. 2010, 92, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Osei, J.; Andersson, M.; Reijden, O.V.; Dold, S.; Smuts, C.M.; Baumgartner, J. Breast-milk iodine concentrations, iodine status, and thyroid function of breastfed infants aged 2–4 months and their mothers residing in a south African township. J. Clin. Res. Pediatr. Endocrinol. 2016, 8, 381–391. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, A.; O’Leary, P.; James, I.; Skeaff, S.; Sherriff, J. Assessment of breast milk iodine concentrations in lactating women in Western Australia. Nutrients 2016, 8, 699. [Google Scholar] [CrossRef] [PubMed]
- Dold, S.; Zimmermann, M.B.; Baumgartner, J.; Davaz, T.; Galetti, V.; Braegger, C.; Andersson, M. A dose-response crossover iodine balance study to determine iodine requirements in early infancy. Am. J. Clin. Nutr. 2016, 104, 620–628. [Google Scholar] [CrossRef] [PubMed]
- Kristiansen, A.L.; Lande, B.; Overby, N.C.; Andersen, L.F. Factors associated with exclusive breast-feeding and breast-feeding in Norway. Public Health Nutr. 2010, 13, 2087–2096. [Google Scholar] [CrossRef] [PubMed]
- Hörnell, A.; Lagstrom, H.; Lande, B.; Thorsdottir, I. Breastfeeding, introduction of other foods and effects on health: A systematic literature review for the 5th Nordic nutrition recommendations. Food Nutr. Res. 2013. [Google Scholar] [CrossRef] [PubMed]
- Lande, B.; Helleve, A. Breastfeeding and Infants’ Diet. National Survey 2013, in Norwegian; Techincal Report; The Norwegian Directorate of Health: Oslo, Norway, 2014. [Google Scholar]
- Gunnarsdottir, I.; Gustavsdottir, A.G.; Thorsdottir, I. Iodine intake and status in Iceland through a period of 60 years. Food Nutr. Res. 2009. [Google Scholar] [CrossRef] [PubMed]
- Lahesmaa, P.; Vilkki, P. The iodine content of human milk in Finland. Acta Paediatr. 1960, 49, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Andersen, S.L.; Moller, M.; Laurberg, P. Iodine concentrations in milk and in urine during breastfeeding are differently affected by maternal fluid intake. Thyroid 2014, 24, 764–772. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.M.; Braverman, L.E.; He, X.; Heeren, T.; Pearce, E.N. Breastmilk iodine concentrations following acute dietary iodine intake. Thyroid 2012, 22, 1176–1180. [Google Scholar] [CrossRef] [PubMed]
- Henjum, S.; Kjellevold, M.; Ulak, M.; Chandyo, R.K.; Shrestha, P.S.; Froyland, L.; Strydom, E.E.; Dhansay, M.A.; Strand, T.A. Iodine concentration in breastmilk and urine among lactating women of Bhaktapur, Nepal. Nutrients 2016, 8, 255. [Google Scholar] [CrossRef] [PubMed]
- Etling, N.; Padovani, E.; Fouque, F.; Tato, L. First-month variations in total iodine content of human breast milks. Early Hum. Dev. 1986, 13, 81–85. [Google Scholar] [CrossRef]
- Kirk, A.B.; Kroll, M.; Dyke, J.V.; Ohira, S.; Dias, R.A.; Dasgupta, P.K. Perchlorate, iodine supplements, iodized salt and breast milk iodine content. Sci. Total Environ. 2012, 420, 73–78. [Google Scholar] [CrossRef] [PubMed]
- National Nutrition Council. Risk of Iodine Deficiency in Norway. Identification of an Acute Need for Action, in Norwegian; Technical Report; The Norwegian Directorate of Health: Oslo, Norway, 2016. [Google Scholar]
- Garnweidner-Holme, L.; Aakre, I.; Lilleengen, A.M.; Brantsaeter, A.L.; Henjum, S. Knowledge about iodine in pregnant and lactating women in the Oslo area, Norway. Nutrients 2017, 9, 493. [Google Scholar] [CrossRef] [PubMed]
- Axford, S.; Charlton, K.; Yeatman, H.; Ma, G. Improved iodine status in breastfeeding women following mandatory fortification. Aust. N. Z. J. Public Health 2011, 35, 579–580. [Google Scholar] [CrossRef] [PubMed]
- O'Kane, S.M.; Pourshahidi, L.K.; Farren, K.M.; Mulhern, M.S.; Strain, J.J.; Yeates, A.J. Iodine knowledge is positively associated with dietary iodine intake among women of childbearing age in the UK and Ireland. Br. J. Nutr. 2016. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.C.; Savige, G.S.; Mitchell, E.K. Health knowledge and iodine intake in pregnancy. Aust. N. Z. J. Obstet. Gynaecol. 2014, 54, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Laurberg, P.; Andersen, S.; Knudsen, N.; Ovesen, L.; Nohr, S.B.; Bulow Pedersen, I. Thiocyanate in food and iodine in milk: From domestic animal feeding to improved understanding of cretinism. Thyroid 2002, 12, 897–902. [Google Scholar] [CrossRef] [PubMed]
- Sukkhojaiwaratkul, D.; Mahachoklertwattana, P.; Poomthavorn, P.; Panburana, P.; Chailurkit, L.O.; Khlairit, P.; Pongratanakul, S. Effects of maternal iodine supplementation during pregnancy and lactation on iodine status and neonatal thyroid-stimulating hormone. J. Perinatol. 2014, 34, 594–598. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.F.; Skeaff, S.A. Thyroglobulin as a biomarker of iodine deficiency: A review. Thyroid 2014, 24, 1195–1209. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Matrix | Unit | SRM | Certified Value ± u a | Analytical Value ± SD |
|---|---|---|---|---|
| Breast milk | mg/kg dry mass | ERM®-BD150 Skimmed milk powder | 1.73 ± 0.14 | 1.66 ± 0.05 c |
| ERM®-BD151 Skimmed milk powder | 1.78 ± 0.17 | 1.66 ± 0.11 c | ||
| NIST 1549a Whole milk powder | 3.34 ± 0.30 b | 3.58 ± 0.05 d | ||
| Urine | µg/L | SeronormTM Trace Elements Urine L-1 | 84 ± 12 | 77 ± 1.4 e |
| SeronormTM Trace Elements Urine L-2 | 304 ± 44 | 278 ± 6.0 e |
| Characteristics | Mean (±SD) | BMIC Median | p-Value a |
|---|---|---|---|
| Age mother, years | 32 ± 4.2 | ||
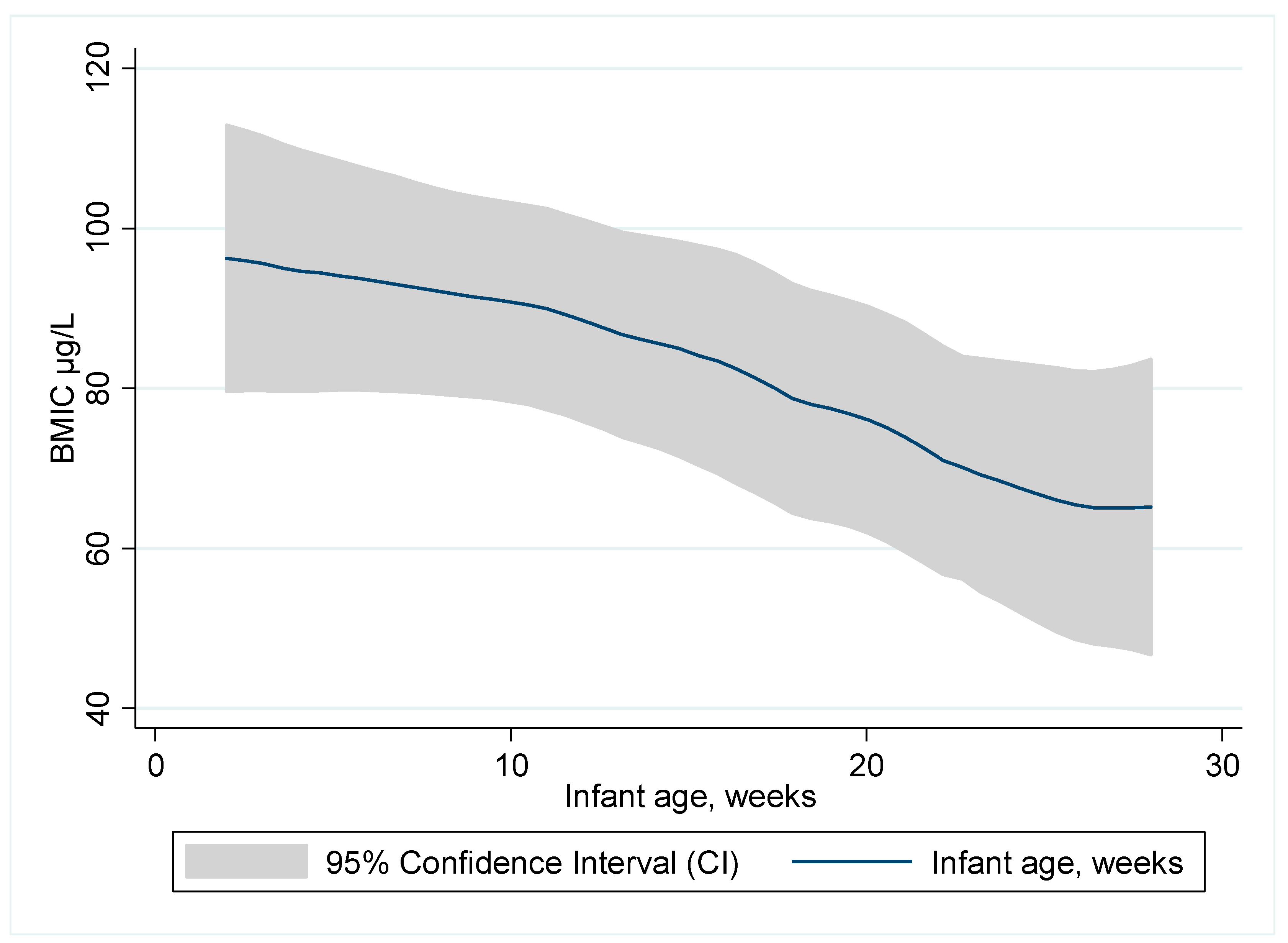
| Infant age, weeks | 11 ± 6.6 | ||
| BMI, kg/m2 | 25 ± 4.7 | ||
| Maternal age, categories | n (%) | ||
| ≤30 years | 66 (37.7) | 66 | 0.220 |
| >30 years | 109 (62.3) | 69 | |
| Infant age, categories | |||
| 2–10 weeks | 89 (50.9) | 70 | 0.034 |
| 11–19 weeks | 54 (30.9) | 71 | |
| 20–28 weeks | 32 (18.3) | 48 | |
| BMI categories | |||
| <24.9 | 108 (61.7) | 69 | 0.098 |
| ≥25–29.9 | 47 (26.9) | 52 | |
| ≥30 | 20 (11.4) | 84 | |
| Number of children | |||
| One child | 106 (60.6) | 70 | 0.382 |
| More than one child | 69 (39.4) | 66 | |
| Lactation | |||
| Exclusive breastfeeding | 140 (80.0) | 80 | 0.096 |
| Partial breastfeeding | 35 (20.0) | 66 | |
| Education | |||
| ≤12 years (high school) | 32 (18.3) | 52 | 0.487 |
| 1–4 years higher education | 53 (30.3) | 70 | |
| >4 years of higher education | 90 (51.4) | 68 | |
| Country of birth | |||
| Norway | 113 (64.6) | 68 | 0.414 |
| Other | 62 (35.4) | 64 | |
| HDI birth country b | |||
| Very high HDI | 134 (76.6) | 67 | 0.808 |
| High HDI | 13 (7.4) | 70 | |
| Medium HDI | 11 (6.3) | 75 | |
| Low HDI | 17 (9.7) | 71 | |
| Smoking | |||
| No | 170 (97.1) | 68 | 0.305 |
| Daily | 5 (2.9) | 57 | |
| Thyroid disease | |||
| No | 164 (93.7) | 67 | 0.130 |
| Yes c | 11 (6.3) | 82 | |
| Iodine supplement use habitually | |||
| No | 124 (70.9) | 60 | <0.001 |
| Yes | 51 (29.1) | 99 | |
| Iodine supplement use last 24 h | |||
| No | 144 (82.3) | 61 | <0.001 |
| Yes | 31 (17.7) | 140 |
| Mean (±SD) | Median | P25 | P75 | |
|---|---|---|---|---|
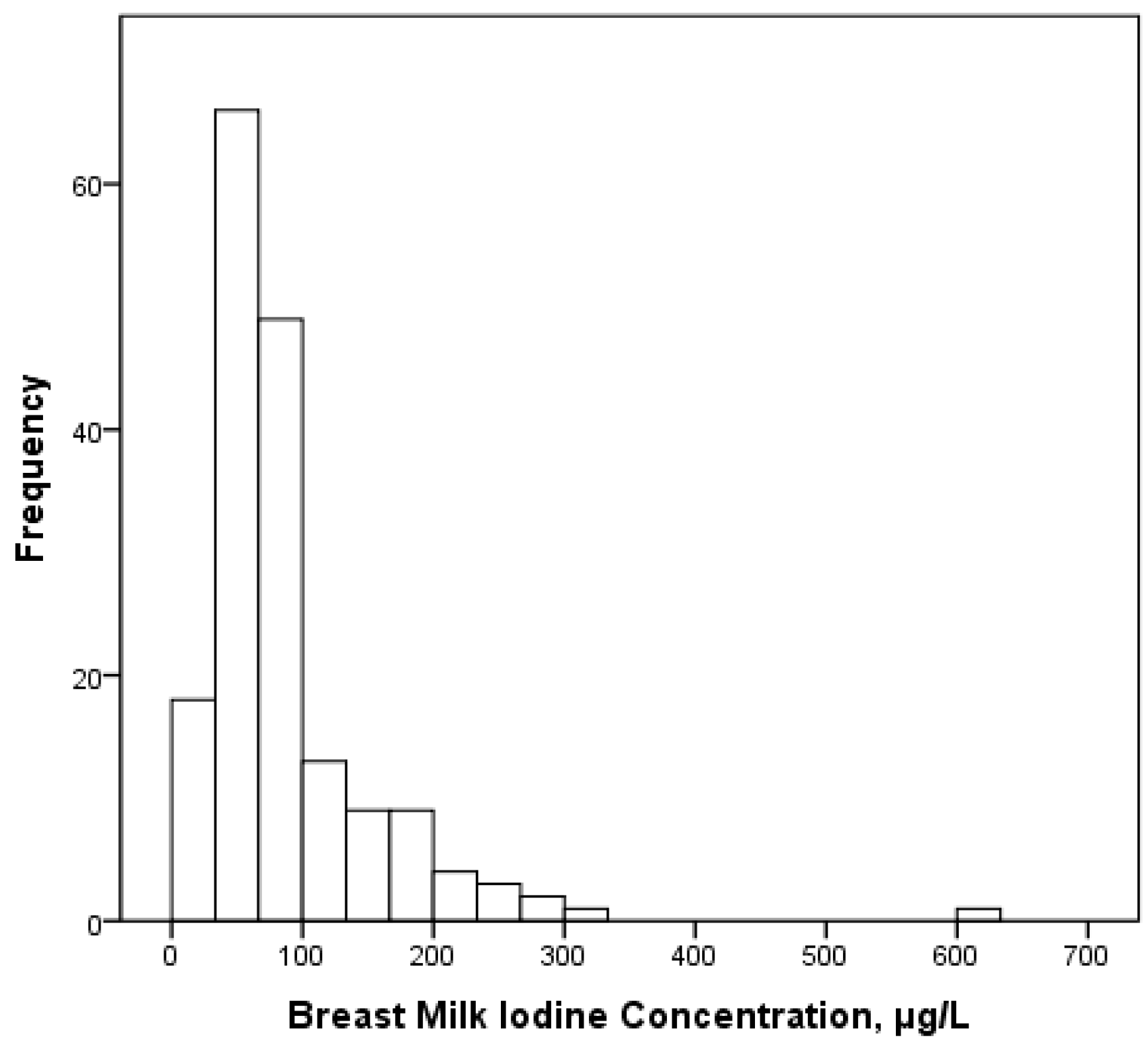
| Breastmilk iodine concentration, µg/L | 87 (70) | 68 | 45 | 98 |
| Urinary iodine concentration, µg/L | 81 (76) | 64 | 39 | 95 |
| Habitual iodine intake | ||||
| Iodine from food only, µg/day | 116 (65) | 106 | 79 | 138 |
| Total iodine intake, µg/day | 158 (97) | 135 | 94 | 211 |
| 24 h iodine intake | ||||
| Iodine from food only, µg/day | 130 (64) | 121 | 82 | 162 |
| Total iodine intake, µg/day | 160 (92) | 134 | 95 | 222 |
| Iodine intake estimated from UIC a, µg/day | 129 (117) | 102 | 58 | 156 |
| Dependent Variables | Predictor Variables | Unadjusted Coefficient (95% CI) | p | Adjusted Coefficient f (95% CI) | p | Stand Beta |
|---|---|---|---|---|---|---|
| BMIC a | Constant | 3.3 (2.8, 3.7) | <0.001 | |||
| Infant age b | −0.02 (−0.03, −0.01) | 0.017 | −0.02 (−0.03, −0.01) | 0.026 | −0.14 | |
| Iodine supple c | 0.03 (0.02, 0.04) | <0.001 | 0.01 (0.01, 0.02) | <0.001 | 0.36 | |
| UIC, µg/L d | 0.03 (0.02, 0.04) | <0.001 | 0.01 (0.01, 0.04) | <0.001 | 0.26 | |
| Smoking e | −0.18 (−0.35, −0.01) | 0.042 | −0.18 (−0.32, −0.03) | 0.016 | −0.16 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Henjum, S.; Lilleengen, A.M.; Aakre, I.; Dudareva, A.; Gjengedal, E.L.F.; Meltzer, H.M.; Brantsæter, A.L. Suboptimal Iodine Concentration in Breastmilk and Inadequate Iodine Intake among Lactating Women in Norway. Nutrients 2017, 9, 643. https://0-doi-org.brum.beds.ac.uk/10.3390/nu9070643
Henjum S, Lilleengen AM, Aakre I, Dudareva A, Gjengedal ELF, Meltzer HM, Brantsæter AL. Suboptimal Iodine Concentration in Breastmilk and Inadequate Iodine Intake among Lactating Women in Norway. Nutrients. 2017; 9(7):643. https://0-doi-org.brum.beds.ac.uk/10.3390/nu9070643
Chicago/Turabian StyleHenjum, Sigrun, Anne Marie Lilleengen, Inger Aakre, Anna Dudareva, Elin Lovise Folven Gjengedal, Helle Margrete Meltzer, and Anne Lise Brantsæter. 2017. "Suboptimal Iodine Concentration in Breastmilk and Inadequate Iodine Intake among Lactating Women in Norway" Nutrients 9, no. 7: 643. https://0-doi-org.brum.beds.ac.uk/10.3390/nu9070643