
A Cross-Sectional Study of Bitter-Taste Receptor Genotypes, Oral Health, and Markers of Oral Inflammation

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics Approval
2.2. Study Population and Participant Recruitment
2.3. Questionnaires
2.4. Sample Collection and Processing
2.5. Saliva Testing and Oral Examination
2.6. Genotyping
2.7. Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.2. Relationships between Bitter-Taste Genotypes and Oral Health Outcomes
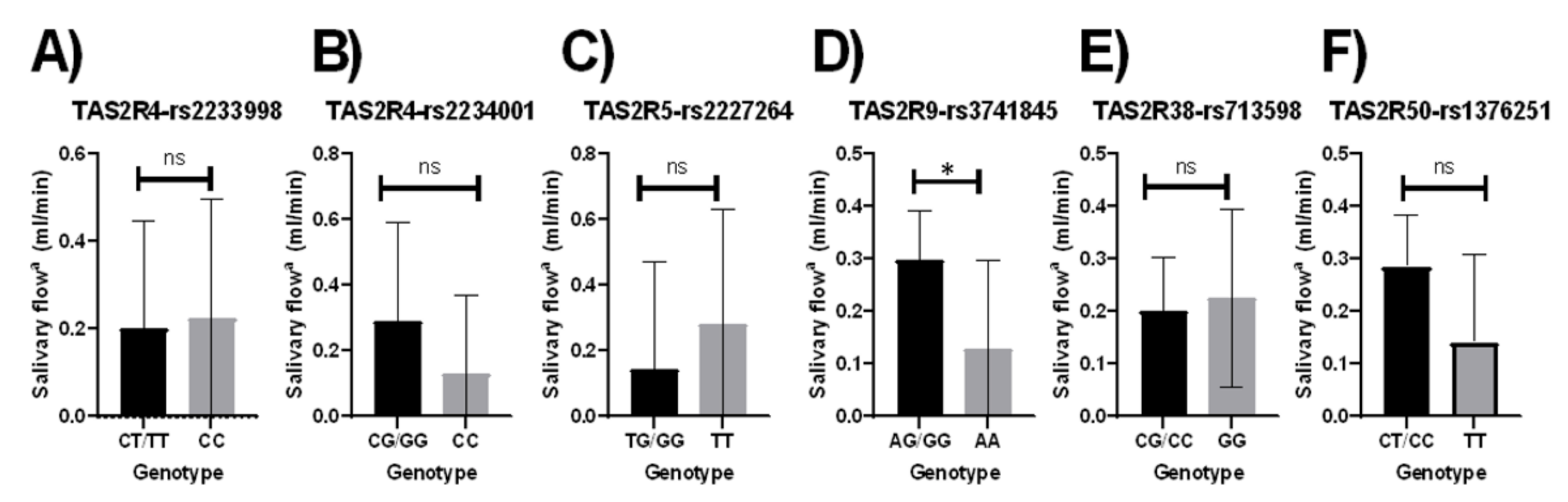
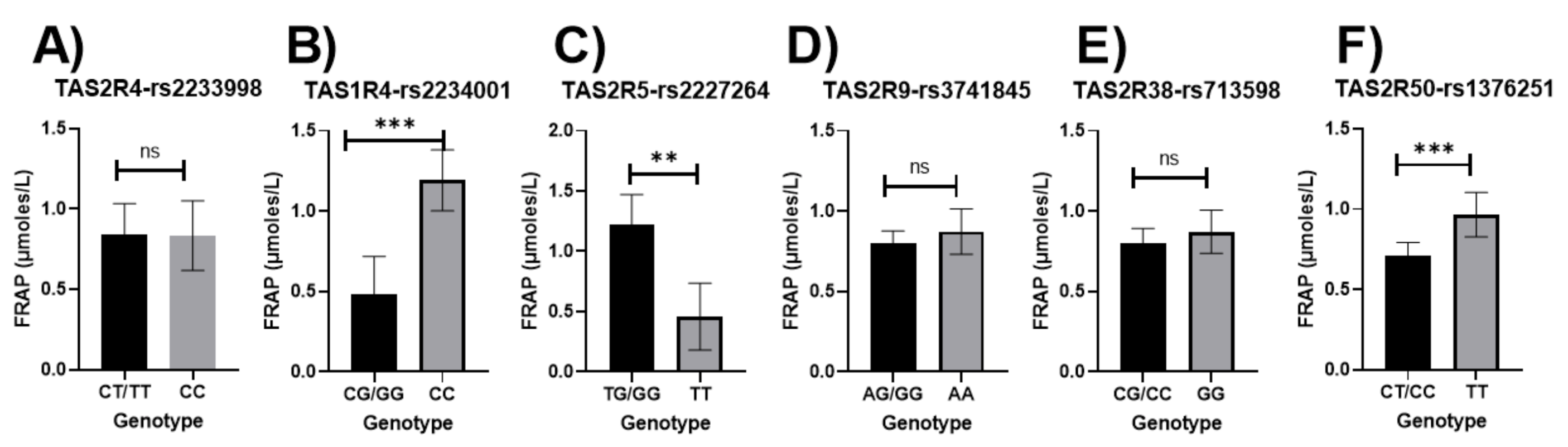
3.3. Relationships between Bitter-Taste Receptor Genotypes and Clinical Markers of Oral Health
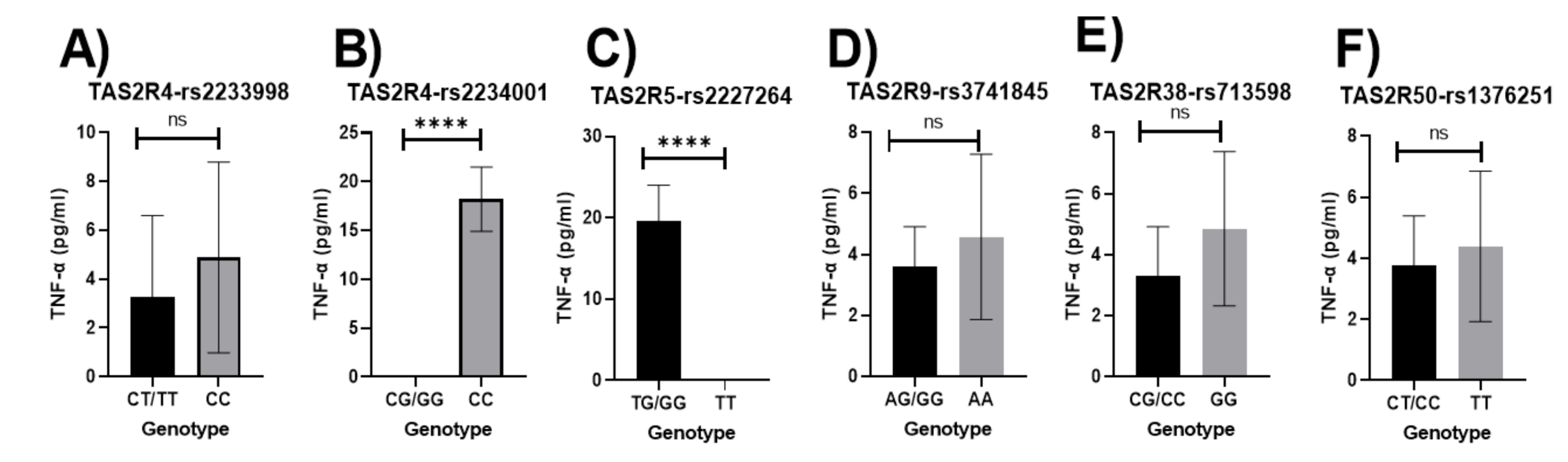
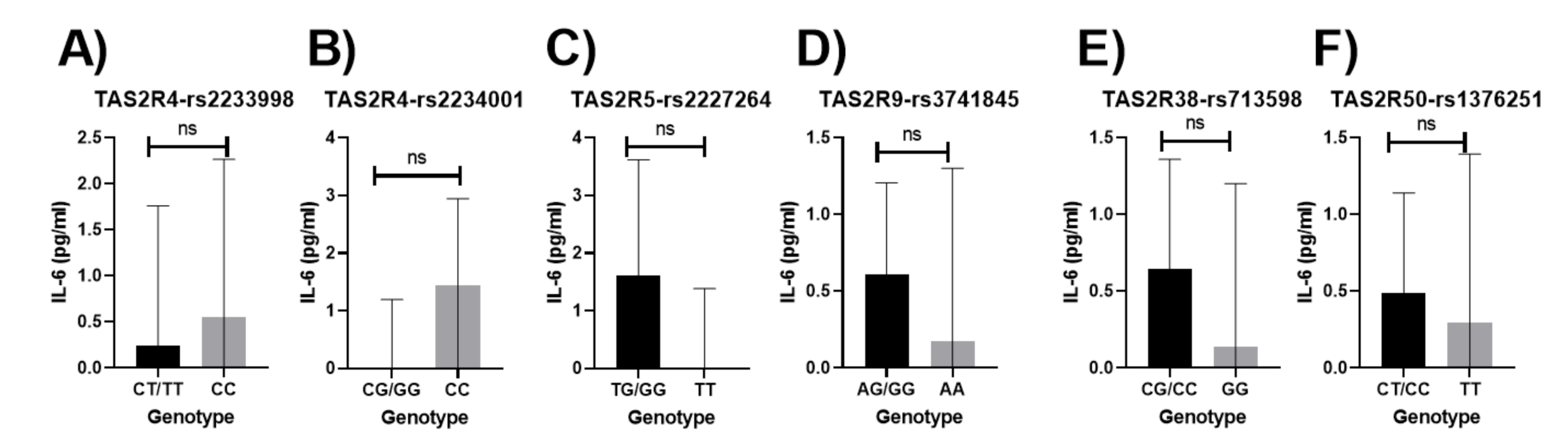
3.4. Relationships between Bitter-Taste Receptor Genotypes and Salivary Inflammatory Mediators
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kassebaum, N.J.; Smith, A.G.C.; Bernabé, E.; Fleming, T.D.; Reynolds, A.E.; Vos, T.; Murray, C.J.L.; Marcenes, W. Global, Regional, and National Prevalence, Incidence, and Disability-Adjusted Life Years for Oral Conditions for 195 Countries, 1990–2015: A Systematic Analysis for the Global Burden of Diseases, Injuries, and Risk Factors. J. Dent. Res. 2017, 96, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Disease, G.B.D.; Injury, I.; Prevalence, C. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 354 Diseases and Injuries for 195 Countries and Territories, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- AIHW. Oral Health and Dental Care in Australia; AIHW: Canberra, Australia, 2020. [Google Scholar]
- Griffin, S.O.; Jones, J.A.; Brunson, D.; Griffin, P.M.; Bailey, W.D. Burden of Oral Disease among Older Adults and Implications for Public Health Priorities. Am. J. Public Health 2012, 102, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral Diseases: A Global Public Health Challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Jamieson, L.M.; Paradies, Y.C.; Gunthorpe, W.; Cairney, S.J.; Sayers, S.M. Oral Health and Social and Emotional Well-being in a Birth Cohort of Aboriginal Australian Young Adults. BMC Public Health 2011, 11, 656. [Google Scholar] [CrossRef] [Green Version]
- Savoca, M.R.; Arcury, T.A.; Leng, X.; Chen, H.; Bell, R.A.; Anderson, A.M.; Kohrman, T.; Frazier, R.J.; Gilbert, G.H.; Quandt, S.A. Severe Tooth Loss in Older Adults as a Key Indicator of Compromised Dietary Quality. Public Health Nutr. 2010, 13, 466–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapple, I.L.; Genco, R. Diabetes and Periodontal Diseases: Consensus Report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J. Periodontol. 2013, 84, S106–S112. [Google Scholar] [CrossRef] [PubMed]
- Ide, M.; Papapanou, P.N. Epidemiology of Association between Maternal Periodontal Disease and Adverse Pregnancy Outcomes—Systematic Review. J. Periodontol. 2013, 84, S181–S194. [Google Scholar] [CrossRef]
- Humphrey, L.L.; Fu, R.; Buckley, D.I.; Freeman, M.; Helfand, M. Periodontal Disease and Coronary Heart Disease Incidence: A Systematic Review and Meta-analysis. J. Gen. Intern. Med. 2008, 23, 2079–2086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanz, M.; D’Aiuto, F.; Deanfield, J.; Fernandez-Avilés, F. European Workshop in Periodontal Health and Cardiovascular Disease—Scientific Evidence on the Association between Periodontal and Cardiovascular Diseases: A Review of the Literature. Eur. Heart J. Suppl. 2010, 12, B3–B12. [Google Scholar] [CrossRef]
- Lamster, I.B.; Lalla, E.; Borgnakke, W.S.; Taylor, G.W. The Relationship between Oral Health and Diabetes Mellitus. J. Am. Dent. Assoc. 2008, 139, 19S–24S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pazos, P.; Leira, Y.; Domínguez, C.; Pías-Peleteiro, J.M.; Blanco, J.; Aldrey, J.M. Association between Periodontal Disease and Dementia: A Literature Review. Neurologia 2018, 33, 602–613. [Google Scholar] [CrossRef] [PubMed]
- AlJehani, Y.A. Risk Factors of Periodontal Disease: Review of the Literature. Int. J. Dent. 2014, 2014, 182513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Najeeb, S.; Zafar, M.S.; Khurshid, Z.; Zohaib, S.; Almas, K. The Role of Nutrition in Periodontal Health: An Update. Nutrients 2016, 8, 530. [Google Scholar] [CrossRef] [PubMed]
- Kaur, K.; Sculley, D.; Wallace, J.; Turner, A.; Ferraris, C.; Veysey, M.; Lucock, M.; Beckett, E.L. Micronutrients and Bioactive Compounds in Oral Inflammatory Diseases. J. Nutr. Intermed. Metab. 2019, 18, 100105. [Google Scholar] [CrossRef]
- Wendell, S.; Wang, X.; Brown, M.; Cooper, M.E.; DeSensi, R.S.; Weyant, R.J.; Crout, R.; McNeil, D.W.; Marazita, M.L. Taste Genes Associated with Dental Caries. J. Dent. Res. 2010, 89, 1198–1202. [Google Scholar] [CrossRef] [PubMed]
- Leone, C.W.; Oppenheim, F.G. Physical and Chemical Aspects of Saliva as Indicators of Risk for Dental Caries in Humans. J. Dent. Educ. 2001, 65, 1054–1062. [Google Scholar] [CrossRef]
- Syrjälä, A.M.; Raatikainen, L.; Komulainen, K.; Knuuttila, M.; Ruoppi, P.; Hartikainen, S.; Sulkava, R.; Ylöstalo, P. Salivary Flow Rate and Periodontal Iinfection-a Study among Subjects Aged 75 Years or Older. Oral Dis. 2011, 17, 387–392. [Google Scholar] [CrossRef]
- Sculley, D.; Langley-Evans, S. Salivary Antioxidants and Periodontal Disease Status. Proc. Nutr. Soc. 2002, 61, 137–143. [Google Scholar] [CrossRef] [Green Version]
- Preethi, B.P.; Reshma, D.; Anand, P. Evaluation of Flow Rate, pH, Buffering Capacity, Calcium, Total Proteins and Total Antioxidant Capacity Levels of Saliva in Caries Free and Caries Active Children: An In Vivo Study. Indian J. Clin. Biochem. 2010, 25, 425–428. [Google Scholar] [CrossRef] [Green Version]
- Animireddy, D.; Reddy Bekkem, V.T.; Vallala, P.; Kotha, S.B.; Ankireddy, S.; Mohammad, N. Evaluation of pH, Buffering Capacity, Viscosity and Flow Rate Levels of Saliva in Caries-free, Minimal Caries and Nursing Caries Children: An in Vivo Study. Contemp. Clin. Dent. 2014, 5, 324–328. [Google Scholar] [CrossRef]
- Pan, W.; Wang, Q.; Chen, Q. The Cytokine Network Involved in the Host Immune Response to Periodontitis. Int. J. Oral Sci. 2019, 11, 30. [Google Scholar] [CrossRef] [Green Version]
- Feeney, E.; O’Brien, S.; Scannell, A.; Markey, A.; Gibney, E.R. Genetic Variation in Taste Perception: Does it have a Role in Healthy Eating? Proc. Nutr. Soc. 2011, 70, 135–143. [Google Scholar] [CrossRef] [Green Version]
- Yildiz, G.; Ermis, R.B.; Calapoglu, N.S.; Celik, E.U.; Türel, G.Y. Gene-environment Interactions in the Etiology of Dental Caries. J. Dent. Res. 2016, 95, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.P. Caries Experience in Children with Various Genetic Sensitivity Levels to the Bitter Taste of 6-n-propylthiouracil (PROP): A Pilot Study. Pediatr. Dent. 2003, 25, 37–42. [Google Scholar]
- Furquim, T.R.; Poli-Frederico, R.C.; Maciel, S.M.; Gonini-Júnior, A.; Walter, L.R. Sensitivity to Bitter and Sweet Taste Perception in Schoolchildren and Their Relation to Dental Caries. Oral Health Prev. Dent. 2010, 8, 253–259. [Google Scholar] [PubMed]
- Pidamale, R.; Sowmya, B.; Thomas, A.; Jose, T. Genetic Sensitivity to Bitter Taste of 6-n Propylthiouracil: A Useful Diagnostic Aid to Detect Early Childhood Caries in Pre-school Children. Indian J. Hum. Genet. 2012, 18, 101–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orsmark-Pietras, C.; James, A.; Konradsen, J.R.; Nordlund, B.; Söderhäll, C.; Pulkkinen, V.; Pedroletti, C.; Daham, K.; Kupczyk, M.; Dahlén, B.; et al. Transcriptome Analysis Reveals Upregulation of Bitter Taste Receptors in Severe Asthmatics. Eur. Respir. J. 2013, 42, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welcome, M.O. The Bitterness of Genitourinary Infections: Properties, Ligands of Genitourinary Bitter Taste Receptors and Mechanisms Linking Taste Sensing to Inflammatory Processes in the Genitourinary Tract. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 247, 101–110. [Google Scholar] [CrossRef]
- Tizzano, M.; Gulbransen, B.D.; Vandenbeuch, A.; Clapp, T.R.; Herman, J.P.; Sibhatu, H.M.; Churchill, M.E.A.; Silver, W.L.; Kinnamon, S.C.; Finger, T.E. Nasal Chemosensory Cells Use Bitter Taste Signaling to Detect Irritants and Bacterial Signals. Proc. Natl. Acad. Sci. USA 2010, 107, 3210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saunders, C.J.; Christensen, M.; Finger, T.E.; Tizzano, M. Cholinergic Neurotransmission Links Solitary Chemosensory Cells to Nasal Inflammation. Proc. Natl. Acad. Sci. USA 2014, 111, 6075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, P.; Yi, R.; Nayak, A.P.; Wang, N.; Tang, F.; Knight, M.J.; Pan, S.; Oliver, B.; Deshpande, D.A. Bitter Taste Receptor Agonists Mitigate Features of Allergic Asthma in Mice. Sci. Rep. 2017, 7, 46166. [Google Scholar] [CrossRef] [PubMed]
- Kok, B.P.; Galmozzi, A.; Littlejohn, N.K.; Albert, V.; Godio, C.; Kim, W.; Kim, S.M.; Bland, J.S.; Grayson, N.; Fang, M.; et al. Intestinal Bitter Taste Receptor Activation Alters Hormone Secretion and Imparts Metabolic Benefits. Mol. Metab. 2018, 16, 76–87. [Google Scholar] [CrossRef]
- Patel, N.N.; Workman, A.D.; Cohen, N.A. Role of Taste Receptors as Sentinels of Innate Immunity in the Upper Airway. J. Pathog. 2018, 2018, 9541987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carey, R.M.; Adappa, N.D.; Palmer, J.N.; Lee, R.J.; Cohen, N.A. Taste Receptors: Regulators of Sinonasal Innate Immunity. Laryngoscope Investig. Otolaryngol. 2016, 1, 88–95. [Google Scholar] [CrossRef]
- Gil, S.; Coldwell, S.; Drury, J.L.; Arroyo, F.; Phi, T.; Saadat, S.; Kwong, D.; Chung, W.O. Genotype-specific Regulation of Oral Innate Immunity by T2R38 Taste Receptor. Mol. Immunol. 2015, 68, 663–670. [Google Scholar] [CrossRef] [Green Version]
- Tiroch, J.; Sterneder, S.; Di Pizio, A.; Lieder, B.; Hoelz, K.; Holik, A.-K.; Pignitter, M.; Behrens, M.; Somoza, M.; Ley, J.P.; et al. Bitter Sensing TAS2R50 Mediates the Trans-Resveratrol-Induced Anti-inflammatory Effect on Interleukin 6 Release in HGF-1 Cells in Culture. J. Agric. Food Chem. 2021. [Google Scholar] [CrossRef]
- Medapati, M.R.; Singh, N.; Bhagirath, A.Y.; Duan, K.; Triggs-Raine, B.; Batista, E.L., Jr.; Chelikani, P. Bitter Taste Receptor T2R14 Detects Quorum Sensing Molecules from Cariogenic Streptococcus Mutans and Mediates Innate Immune Responses in Gingival Epithelial Cells. FASEB J. 2021, 35, e21375. [Google Scholar] [CrossRef]
- Feng, P.; Jyotaki, M.; Kim, A.; Chai, J.; Simon, N.; Zhou, M.; Bachmanov, A.A.; Huang, L.; Wang, H. Regulation of Bitter Taste Responses by Tumor Necrosis Factor. Brain Behav. Immun. 2015, 49, 32–42. [Google Scholar] [CrossRef] [Green Version]
- Paxton, A.E.; Strycker, L.A.; Toobert, D.J.; Ammerman, A.S.; Glasgow, R.E. Starting The Conversation: Performance of a Brief Dietary Assessment and Intervention Tool for Health Professionals. Am. J. Prev. Med. 2011, 40, 67–71. [Google Scholar] [CrossRef]
- Isohelix. Instructions for Use of Isohelix SK-1S/MS-01 Buccal Swabs. Available online: https://isohelix.com/wp-content/uploads/2020/06/ROW-SK-1S-and-MS-01-instructions-June-2019.pdf (accessed on 1 June 2019).
- Salimetrics. Collection Methods: Passive Drool Using the Saliva Collection Aid. Available online: https://salimetrics.com/wp-content/uploads/2018/02/passive-drool-saliva-collection-instructions.pdf (accessed on 1 June 2019).
- Salimetrics. Salimetrics Collection Handbook. Available online: https://salimetrics.com/saliva-collection-handbook/ (accessed on 1 June 2019).
- GC America Corporation, Saliva-Check BUFFER Testing Mat. Available online: http://www.gcamerica.com/products/preventive/Saliva_Check_BUFFER/Saliva_Check_TestingMat.pdf (accessed on 1 June 2019).
- WHO. Mean Number of Decayed, Missing, and Filled Permanent Teeth (Mean DMFT) among the 12-year-old Age Group. Available online: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/3812 (accessed on 1 December 2020).
- Primal, K.S.; Esther, S.R.; Boehm, T.K. Periodontal Screening and Recording (PSR) Index Scores Predict Periodontal Diagnosis. J. Dent. Appl. 2014, 1, 8–12. [Google Scholar]
- Landry, R.G.; Jean, M. Periodontal Screening and Recording (PSR) Index: Precursors, Utility and Limitations in a Clinical Setting. Int. Dent. J. 2002, 52, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Benzie, I.F.; Strain, J.J. The Ferric Reducing Ability of Plasma (FRAP) as a Measure of “Antioxidant Power”: The FRAP Assay. Anal. Biochem. 1996, 239, 70–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salimetrics. Salimetrics IL-1β ELISA Kit. Available online: https://salimetrics.com/wp-content/uploads/2018/03/il-1-beta-saliva-elisa-kit.pdf (accessed on 1 April 2020).
- Isohelix. Instructions for Isohelix Xtreme DNA Kit: XME-5/50. Available online: https://isohelix.com/wp-content/uploads/2020/06/XME-5-50-Xtreme-DNA-kit-Instructions-FD-PK-Version-Dec-2017.pdf (accessed on 1 June 2019).
- ThermoFisher. TaqMan® SNP Genotyping Assays USER GUIDE. Available online: https://assets.thermofisher.com/TFS-Assets/LSG/manuals/4454239_IntrotoGeneEx_GSG.pdf (accessed on 1 December 2019).
- Turner, A.; Veysey, M.; Keely, S.; Scarlett, C.J.; Lucock, M.; Beckett, E.L. Genetic Variation in the Bitter Receptors Responsible for Epicatechin Detection Are Associated with BMI in an Elderly Cohort. Nutrients 2021, 13, 571. [Google Scholar] [CrossRef] [PubMed]
- Winn, D.M. Tobacco Use and Oral Disease. J. Dent. Educ. 2001, 65, 306–312. [Google Scholar] [CrossRef]
- Moynihan, P. The Interrelationship between Diet and Oral Health. Proc. Nutr. Soc. 2005, 64, 571–580. [Google Scholar] [CrossRef] [Green Version]
- Rheu, G.B.; Ji, S.; Ryu, J.J.; Lee, J.B.; Shin, C.; Lee, J.Y.; Huh, J.B.; Shin, S.W. Risk Assessment for Clinical Attachment Loss of Periodontal Tissue in Korean Adults. J. Adv. Prosthodont. 2011, 3, 25–32. [Google Scholar] [CrossRef]
- Hodge, P.; Binnie, V. Smoking Cessation and Periodontal Health—A Missed Opportunity? Evid. Based Dent. 2009, 10, 18–19. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Palacios, R.D.; Ramírez-Amador, V.; Jarillo-Soto, E.C.; Irigoyen-Camacho, M.E.; Mendoza-Núñez, V.M. Relationship between Gender, Income and Education and Self-perceived Oral Health among Elderly Mexicans. An Exploratory Study. Ciência Saúde Coletiva 2015, 20, 997–1004. [Google Scholar] [CrossRef] [Green Version]
- Sabbah, W.; Tsakos, G.; Sheiham, A.; Watt, R.G. The Effects of Income and Education on Ethnic Differences in Oral Health: A Study in US Adults. J. Epidemiol. Community Health 2009, 63, 516. [Google Scholar] [CrossRef]
- Bettaieb, A.; Cremonini, E.; Kang, H.; Kang, J.; Haj, F.G.; Oteiza, P.I. Anti-inflammatory Actions of (-)-epicatechin in the Adipose Tissue of Obese Mice. Int. J. Biochem. Cell Biol. 2016, 81, 383–392. [Google Scholar] [CrossRef] [Green Version]
- Lee, R.J.; Xiong, G.; Kofonow, J.M.; Chen, B.; Lysenko, A.; Jiang, P.; Abraham, V.; Doghramji, L.; Adappa, N.D.; Palmer, J.N.; et al. T2R38 Taste Receptor Polymorphisms Underlie Susceptibility to Upper Respiratory Infection. J. Clin. Investig. 2012, 122, 4145–4159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krawczyk, D.; Błaszczak, J.; Borowicz, J.; Mielnik-Błaszczak, M. Life Style and Risk of Development of Dental Caries in a Population of Adolescents. Ann. Agric. Environ. Med. 2014, 21, 576–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hariri, B.M.; Cohen, N.A. New Insights into Upper Airway Innate Immunity. Am. J. Rhinol. Allergy 2016, 30, 319–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hegde, M.; Hegde, N.; Ashok, A.; Shetty, S. Evaluation of Total Antioxidant Capacity of Saliva and Serum in Caries-free and Caries-active Adults: An in-Vivo Study. Indian J. Dent. Res. 2013, 24, 164–167. [Google Scholar] [CrossRef]
- Ahmadi-Motamayel, F.; Goodarzi, M.T.; Hendi, S.S.; Kasraei, S.; Moghimbeigi, A. Total Antioxidant Capacity of Saliva and Dental Caries. Med. Oral Patol. Oral Cir. Bucal 2013, 18, e553–e556. [Google Scholar] [CrossRef]
- Idrees, M.; Nassani, M.; Kujan, O. Assessing the Association between Unstimulated Whole Salivary Flow Rate (UWSFR) and Oral Health Status among Healthy Adult Subjects: A Cross-sectional Study. Med. Oral Patol. Oral Cir. Bucal 2018, 23, e384–e390. [Google Scholar] [CrossRef]
- Sinor, Z.; Azirrawani, A. Association between Salivary Parameters and Periodontal. Int. Med. J. 2013, 20, 1–5. [Google Scholar]
- Rajesh, K.S.; Zareena, H.S.; Arun Kumar, M.S. Assessment of Salivary Calcium, Phosphate, Magnesium, pH, and Flow Rate in Healthy Subjects, Periodontitis, and Dental Caries. Contemp. Clin. Dent. 2015, 6, 461–465. [Google Scholar] [CrossRef]
- Yucel Lindberg, T.; Båge, T. Inflammatory Mediators in the Pathogenesis of Periodontitis. Expert Rev. Mol. Med. 2013, 15, e7. [Google Scholar] [CrossRef] [Green Version]
- Jain, S.; Bansal, K.; Marwaha, M.; Sehrawat, N.; Singla, S. Effect of Diet Modification on Salivary Parameters and Oratest in High-caries-risk Individuals. Int. J. Clin. Pediatr. Dent. 2018, 11, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Shulman, J.D.; Cappelli, D.P. Chapter 1-Epidemiology of Dental Caries. In Prevention in Clinical Oral Health Care; Cappelli, D.P., Mobley, C.C., Eds.; Mosby: Saint Louis, MO, USA, 2008; pp. 2–13. [Google Scholar] [CrossRef]
- Methven, L.; Ellis, L.; Kavaliauskaite, G. Investigating Perception and Liking of Non-nutritiven Sweeteners in Individuals Representing Different Taste Receptor Genotypes. In Proceedings of the 15th Weurman Flavour Research Symposium, Graz, Austria, 18–22 September 2017; pp. 193–198. [Google Scholar] [CrossRef]
- Allen, A.L.; McGeary, J.E.; Hayes, J.E. Rebaudioside A and Rebaudioside D Bitterness do not Covary with Acesulfame K Bitterness or Polymorphisms in TAS2R9 and TAS2R31. Chemosens. Percept. 2013, 6, 109–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rezaei-Soufi, L.; Raedi, S.; Alikhani, M.; Vahdatinia, F.; Farazyani, A.; Hosseini, S.M.; Jazaeri, M. Comparison the Effect of Stevia Extract with Glucose and Fructose on Dental Enamel Caries Formation. J. Chem. Pharm. Sci. 2016, 9, 685–689. [Google Scholar]
- Rai, K.; Hegde, A.M.; Jose, N. Salivary Antioxidants and Oral Health in Children with Autism. Arch. Oral Biol. 2012, 57, 1116–1120. [Google Scholar] [CrossRef]
- Ahmadi-Motamayel, F.; Goodarzi, M.T.; Jamshidi, Z.; Kebriaei, R. Evaluation of Salivary and Serum Antioxidant and Oxidative Stress Statuses in Patients with Chronic Periodontitis: A Case-Control Study. Front. Physiol. 2017, 8, 189. [Google Scholar] [CrossRef] [Green Version]
- Zhang, T.; Andrukhov, O.; Haririan, H.; Müller-Kern, M.; Liu, S.; Liu, Z.; Rausch-Fan, X. Total Antioxidant Capacity and Total Oxidant Status in Saliva of Periodontitis Patients in Relation to Bacterial Load. Front. Cell Infect. Microbiol. 2015, 5, 97. [Google Scholar] [CrossRef]
- Vahabi, S.; Sattari, M.; Taheraslani, M.; Bagheban, A. Correlation between Interleukin-42, Interleukin-6 and Tumor Necrosis Factor 0± and Clinical Parameters in Chronic and Aggressive Periodontal Disease. J. Periodontol. Implant. Dent. 2012, 3, 51–56. [Google Scholar]
- Batool, H.; Nadeem, A.; Kashif, M.; Shahzad, F.; Tahir, R.; Afzal, N. Salivary Levels of IL-6 and IL-17 Could Be an Indicator of Disease Severity in Patients with Calculus Associated Chronic Periodontitis. BioMed Res. Int. 2018, 2018, 8531961. [Google Scholar] [CrossRef] [Green Version]
- Irwin, C.R.; Myrillas, T.T. The Role of IL-6 in the Pathogenesis of Periodontal Disease. Oral Dis. 1998, 4, 43–47. [Google Scholar] [CrossRef]
- Cheng, R.; Wu, Z.; Li, M.; Shao, M.; Hu, T. Interleukin-1β is a Potential Therapeutic Target for Periodontitis: A Narrative Review. Int. J. Oral Sci. 2020, 12, 2. [Google Scholar] [CrossRef] [Green Version]
- Williamson, S.; Munro, C.; Pickler, R.; Grap, M.J.; Elswick, R.K. Comparison of Biomarkers in Blood and Saliva in Healthy Adults. Nurs. Res. Pract. 2012, 2012, 246178. [Google Scholar] [CrossRef] [PubMed]
- Munro, C.L.; Grap, M.J.; Jablonski, R.; Boyle, A. Oral Health Measurement in Nursing Research: State of the Science. Biol. Res. Nurs. 2006, 8, 35–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Distribution (Mean ± SD) |
|---|---|
| Age (years) | 36.72 ± 15.17 |
| Body mass index (BMI) | 24.25 ± 5.89 |
| Dietary index | 17.97 ± 2.18 |
| Variable | Distribution (n, %) |
|---|---|
| Sex | |
| Females | 59 (90.77%) |
| Males | 6 (9.23%) |
| Income | |
| <$20,000 | 18 (30.00%) |
| $20,000–$60,000 | 20 (33.33%) |
| $60,000–$100,000 | 9 (15.00%) |
| >$100,000 | 13 (21.67%) |
| Education | |
| ≤Year 12 or equivalent | 16 (26.23%) |
| Bachelor’s degree | 18 (29.51%) |
| TAFE or technical qualification | 21 (34.43%) |
| Post-graduate degree | 6 (9.84%) |
| BMI Status | |
| Underweight | 2 (0.04%) |
| Normal | 41 (71.93%) |
| Overweight | 5 (0.09%) |
| Obese | 9 (0.16%) |
| Smoking Status | |
| Never | 47 (78.33%) |
| Ever | 13 (21.67%) |
| Gene/SNP | Major/Minor Allele | MAF | % Major Allele Presence |
|---|---|---|---|
| TAS2R4-rs2233998 | T/C | 0.42 | 71.19 |
| TAS2R4rs2234001 | G/C | 0.48 | 67.24 |
| TAS2R5-rs2227264 | G/T | 0.44 | 71.67 |
| TAS2R9-rs3741845 | G/A | 0.49 | 77.05 |
| TAS2R38-rs713598 | C/G | 0.46 | 80.70 |
| TAS2R50-rs1376251 | C/T | 0.29 | 81.67 |
| Variables | Distribution (Mean ± SD) |
|---|---|
| FRAP value (μmoles/L) | 0.76 ± 0.24 |
| TNF-α (pg/mL) | 3.67 ± 5.03 |
| IL-1β (pg/mL) | 12.28 ± 13.34 |
| IL-6 (pg/mL) | 0.68 ± 1.22 |
| Salivary flow rate a (mL/min) | 0.28 ± 0.22 |
| DMFT Index | 7.23 ± 7.22 |
| Dental caries | 0.66 ± 1.76 |
| Missing teeth | 2.82 ± 4.28 |
| Filled teeth | 3.80 ± 4.41 |
| Highest PSR Score | 1.87 ± 0.97 |
| Variable | Distribution (n, %) |
|---|---|
| Hydration a | |
| <30 s | 35 (70.00%) |
| >30 s | 15 (30.00%) |
| Viscosity of saliva | |
| Frothy/Bubbly | 13 (26.00%) |
| Watery/Clear | 37 (74.00%) |
| pH (Unstimulated saliva) | |
| 6.0–6.6 | 9 (17.65%) |
| 6.8–7.8 | 42 (82.35%) |
| Quantity (Stimulated saliva) | |
| <5 mL | 4 (8.00%) |
| >5 mL | 46 (92.00%) |
| pH (Stimulated saliva) | |
| 6.0–6.6 | 7 (14.00%) |
| 6.8–7.8 | 43 (86.00%) |
| Buffering capacity | |
| 6–9 points | 8 (16.00%) |
| 10–12 points | 42 (84.00%) |
| Dental Caries | |
| Yes | 10 (16.39%) |
| No | 51 (83.61%) |
| Missing teeth | |
| Yes | 33 (55.00%) |
| No | 27 (45.00%) |
| Filled teeth | |
| Yes | 45 (73.77%) |
| No | 16 (26.23%) |
| Periodontal disease b | |
| Yes | 54 (91.53%) |
| No | 5 (8.48%) |
| LS Means a (95% CI) | p | LS Means a (95% CI) | p | LS Means a (95% CI) | p | LS Means a (95% CI) | p | LS Means a (95% CI) | p | LS Means a (95% CI) | p | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TAS2R4- rs2233998 Major Allele | TAS2R4- rs2234001 Major Allele | TAS2R5- rs2227264 Major allele | TAS2R9- rs3741845 Major allele | TAS2R38- rs713598 Major allele | TAS2R50- rs1376251 Major allele | |||||||||||||
| + | − | + | − | + | − | + | − | + | − | + | − | |||||||
| DMFT | 11.05 (2.91– 19.1) | 5.04 (−4.18– 14.27) | 0.4 | −0.08 (−10.11–9.94) | 16.18 (8.28– 24.07) | 0.05 | 11.69 (0.86– 22.53) | 4.39 (−7.33– 16.13) | 0.5 | 5.79 (2.59– 8.99) | 10.30 (4.57– 16.04) | 0.1 | 9.47 (5.97– 12.98) | 6.62 (0.78– 12.46) | 0.3 | 8.19 (4.77– 11.62) | 7.89 (2.25– 13.55) | 0.9 |
| Dental caries | −0.33 (−2.25–1.60) | 1.04 (−1.15– 3.22) | 0.5 | 0.59 (−1.78– 2.97) | 0.12 (−1.75– 1.99) | 0.8 | 0.63 (−1.93– 3.20) | 0.08 (−2.69– 2.8) | 0.8 | 0.76 (0.01– 1.53) | −0.05 (−1.41– 1.30) | 0.2 | 0.20 (−0.63– 1.03) | 0.51 (−0.87– 1.89) | 0.7 | 0.63 (−0.18– 1.45) | 0.08 (−1.26–1.42) | 0.4 |
| Missing teeth | 7.19 (2.23– 12.15) | 0.11 (−5.48– 5.70) | 0.1 | 2.69 (−3.44– 8.83) | 4.61 (−0.18– 9.39) | 0.7 | 0.85 (−5.72– 7.41) | 6.46 (−0.70– 13.62) | 0.4 | 1.79 (−0.18– 3.76) | 5.51 (2.02– 9.01) | 0.03 | 4.43 (2.27– 6.59) | 2.87 (−0.68– 6.42) | 0.4 | 3.35 (1.27– 5.42) | 3.96 (0.42– 7.49) | 0.7 |
| Filled teeth | 4.35 (−0.61–9.30) | 3.93 (−1.69– 9.56) | 0.9 | −3.13 (−9.24– 2.98) | 11.41 (6.59– 16.22) | 0.005 | 10.17 (3.56– 16.78) | −1.89 (−9.04– 5.26) | 0.07 | 3.34 (1.39– 5.29) | 4.94 (1.44– 8.43) | 0.3 | 4.95 (2.82– 7.09) | 3.33 (−0.24– 6.89) | 0.4 | 4.17 (2.08– 6.26) | 4.11 (0.67– 7.55) | 0.9 |
| Highest PSR score | 1.53 (0.31– 2.75) | 2.56 (1.66– 3.96) | 0.4 | 1.43 (−0.10– 2.97) | 2.66 (1.47– 3.85) | 0.3 | 3.04 (1.41–4.66) | 1.06 (−0.70– 2.82) | 0.2 | 1.89 (1.39– 2.39) | 2.19 (1.32– 3.07) | 0.5 | 2.04 (1.51– 2.57) | 2.05 (1.12– 2.98) | 0.9 | 2.04 (1.51– 2.57) | 2.06 (1.19– 2.92) | 0.9 |
| Gene/SNP | TAS2R4- rs2233998 | TAS2R4- rs2234001 | TAS2R5- rs2227264 | TAS2R9- rs3741845 | TAS2R38- rs713598 | TAS2R50- rs1376251 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| χ2 | p | χ2 | p | χ2 | p | χ2 | p | χ2 | p | χ2 | p | |
| Hydration a | 0.00 | 0.994 | 0.00 | 0.995 | 0.00 | 1.00 | 0.02 | 0.885 | 2.38 | 0.123 | 2.07 | 0.150 |
| Viscosity of saliva | 0.00 | 0.995 | 0.00 | 0.995 | 0.00 | 1.00 | 0.00 | 0.999 | 0.61 | 0.435 | 0.18 | 0.668 |
| pH b | 0.00 | 0.997 | 0.00 | 0.997 | 0.00 | 1.00 | 0.18 | 0.675 | 0.00 | 0.996 | 0.00 | 0.996 |
| Quantity c | 0.00 | 0.995 | 0.00 | 0.995 | 0.00 | 1.00 | 0.55 | 0.458 | 0.35 | 0.554 | 0.99 | 0.320 |
| pH d | 0.00 | 0.995 | 0.00 | 0.995 | 0.00 | 1.00 | 1.22 | 0.269 | 0.00 | 0.993 | 0.00 | 0.994 |
| Buffering capacity | 0.00 | 0.997 | 0.00 | 0.998 | 0.00 | 1.00 | 3.02 | 0.082 | 1.58 | 0.209 | 0.00 | 0.997 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaur, K.; Turner, A.; Jones, P.; Sculley, D.; Veysey, M.; Lucock, M.; Wallace, J.; Beckett, E.L. A Cross-Sectional Study of Bitter-Taste Receptor Genotypes, Oral Health, and Markers of Oral Inflammation. Oral 2021, 1, 122-138. https://0-doi-org.brum.beds.ac.uk/10.3390/oral1020013
Kaur K, Turner A, Jones P, Sculley D, Veysey M, Lucock M, Wallace J, Beckett EL. A Cross-Sectional Study of Bitter-Taste Receptor Genotypes, Oral Health, and Markers of Oral Inflammation. Oral. 2021; 1(2):122-138. https://0-doi-org.brum.beds.ac.uk/10.3390/oral1020013
Chicago/Turabian StyleKaur, Kiranjit, Alexandria Turner, Patrice Jones, Dean Sculley, Martin Veysey, Mark Lucock, Janet Wallace, and Emma L. Beckett. 2021. "A Cross-Sectional Study of Bitter-Taste Receptor Genotypes, Oral Health, and Markers of Oral Inflammation" Oral 1, no. 2: 122-138. https://0-doi-org.brum.beds.ac.uk/10.3390/oral1020013