
Vaginal, Cervical and Uterine pH in Women with Normal and Abnormal Vaginal Microbiota

 , , and
, , and 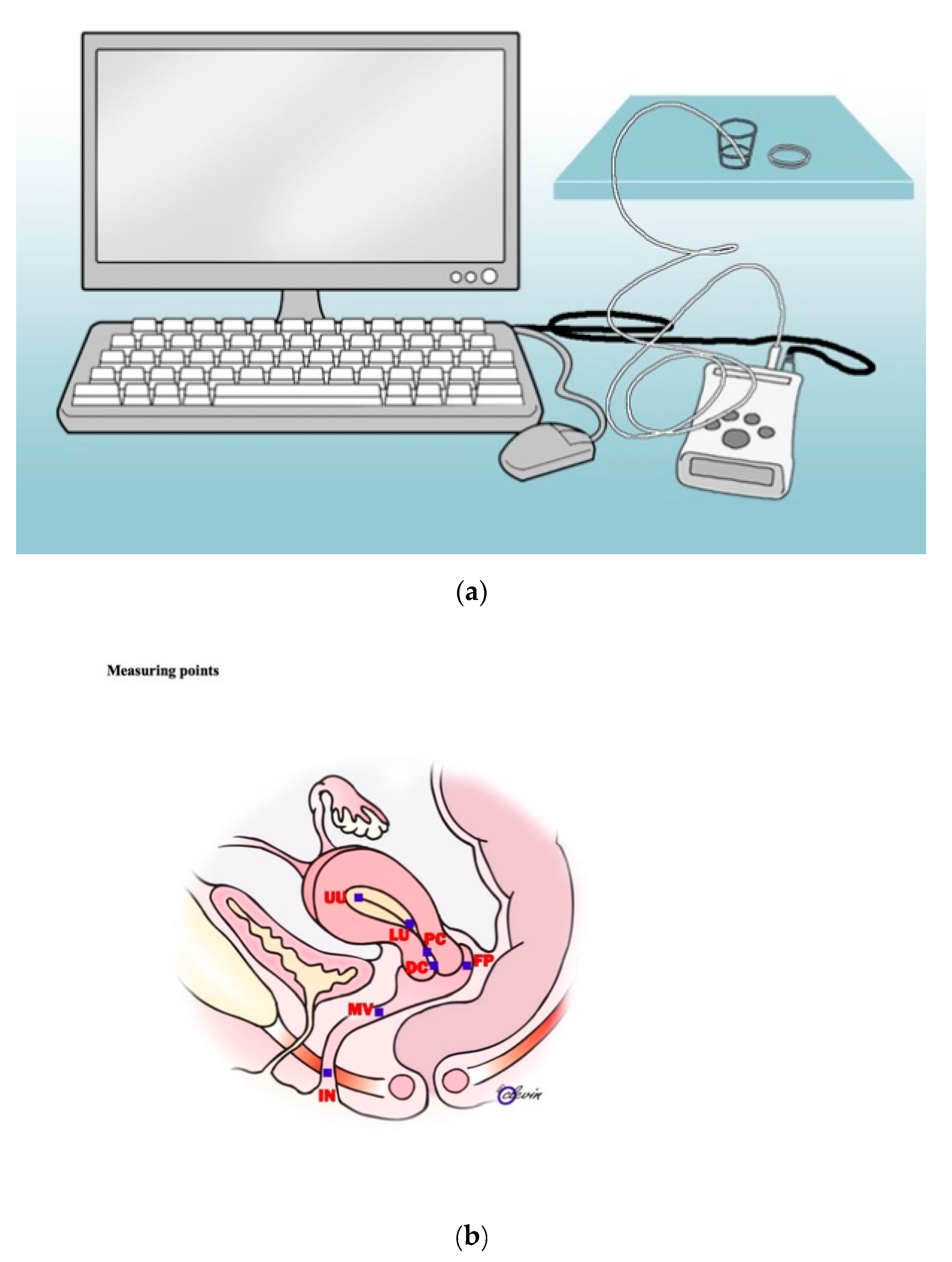{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Participants
4.2. Microbiology
4.3. pH Assessment
4.4. Statistical Methods
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AVM | Abnormal vaginal microbiota |
| BV | Bacterial vaginosis |
| CMP | Cervical mucus plug |
| NVM | Normal vaginal microbiota |
| qPCR | Quantitative polymerase chain reaction |
References
- Donders, G. Diagnosis and management of bacterial vaginosis and other types of abnormal vaginal bacterial flora: A review. Obstet. Gynecol. Surv. 2010, 65, 462–473. [Google Scholar] [CrossRef] [PubMed]
- Ravel, J.; Gajer, P.; Abdo, Z.; Schneider, G.M.; Koenig, S.S.; McCulle, S.L. Vaginal microbiome of reproductive-age women. Proc. Natl. Acad. Sci. USA 2011, 15, 4680–4687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mastromarino, P.; Vitali, B.; Mosca, L. Bacterial vaginosis: A review on clinical trials with probiotics. New Microbiol. 2013, 36, 229–238. [Google Scholar] [PubMed]
- Moreno, I.; Codoner, F.M.; Vilella, F.; Valbuena, D.; Martinez-Blanch, J.F.; Jimenez-Almazan, J. Evidence that the endometrial microbiota has an effect on implantation success or failure. Am. J. Obstet. Gynecol. 2016, 215, 684–703. [Google Scholar] [CrossRef] [Green Version]
- Ralph, S.G.; Rutherford, A.J.; Wilson, J.D. Influence of bacterial vaginosis on conception and miscarriage in the first trimester: Cohort study. BMJ 1999, 24, 220–223. [Google Scholar] [CrossRef] [Green Version]
- Dingens, A.S.; Fairfortune, T.S.; Reed, S.; Mitchell, C. Bacterial vaginosis and adverse outcomes among full-term infants: A cohort study. BMC Pregnancy Childbirth 2016, 22, 278. [Google Scholar] [CrossRef] [Green Version]
- Romero, R.; Hassan, S.S.; Gajer, P.; Tarca, A.L.; Douglas, F.W.; Lorraine, N.; Galuppi, M.; Lamont, R.F.; Chaemsaithong, P.; Miranda, J.; et al. The composition and stability of the vaginal microbiota of normal pregnant women is different from that of non-pregnant women. Microbiome 2014, 2. [Google Scholar] [CrossRef] [Green Version]
- Romero, R.; Hassan, S.S.; Gajer, P.; Tarca, A.L.; Douglas, F.W.; Lorraine, N.; Galuppi, M.; Lamont, R.F.; Chaemsaithong, P.; Miranda, J.; et al. The vaginal microbiota of pregnant women who subsequently have spontaneous preterm labor and delivery and those with a normal delivery at term. Microbiome 2014, 2. [Google Scholar] [CrossRef] [Green Version]
- Becher, N.; Adams, W.K.; Hein, M.; Uldbjerg, N. The cervical mucus plug: Structured review of the literature. Acta Obstet. Gynecol. Scand. 2009, 88, 502–513. [Google Scholar] [CrossRef]
- Brunelli, R.; Papi, M.; Arcovito, G.; Bompiani, A.; Castagnola, M.; Parasassi, T. Globular structure of human ovulatory cervical mucus. FASEB J. 2007, 21, 3872–3876. [Google Scholar] [CrossRef] [Green Version]
- Hansen, L.K.; Becher, N.; Bastholm, S.; Glavind, J.; Ramsing, M.; Kim, C.J. The cervical mucus plug inhibits, but does not block, the passage of ascending bacteria from the vagina during pregnancy. Acta Obstet. Gynecol. Scand. 2014, 93, 102–108. [Google Scholar] [CrossRef]
- Mitchell, C.M.; Haick, A.; Nkwopara, E.; Garcia, R.; Rendi, M.; Agnew, K. Colonization of the upper genital tract by vaginal bacterial species in nonpregnant women. Am. J. Obstet. Gynecol. 2015, 212. [Google Scholar] [CrossRef] [Green Version]
- Swidsinski, A.; Verstraelen, H.; Loening-Baucke, V.; Swidsinski, S.; Mendling, W.; Halwani, Z. Presence of a polymicrobial endometrial biofilm in patients with bacterial vaginosis. PLoS ONE 2013, 8, e53997. [Google Scholar] [CrossRef] [Green Version]
- Nugent, R.P.; Krohn, M.A.; Hillier, S.L. Reliability of diagnosing bacterial vaginosis is improved by a standardized method of gram stain interpretation. J. Clin. Microbiol. 1991, 29, 297–301. [Google Scholar] [CrossRef] [Green Version]
- Gajer, P.; Brotman, R.M.; Bai, G.; Sakamoto, J.; Schutte, U.M.; Zhong, X.; Koenig, S.S.; Fu, L.; Ma, Z.S.; Zhou, X.; et al. Temporal dynamics of the human vaginal microbiota. Sci. Transl. Med. 2012, 4. [Google Scholar] [CrossRef] [Green Version]
- Datcu, R.; Gesink, D.; Mulvad, G.; Montgomery-Andersen, R.; Rink, E.; Koch, A.; Ahrens, P.; Jensen, J.S. Bacterial vaginosis diagnosed by analysis of first-void-urine specimens. J. Clin. Microbiol. 2014, 52, 218–225. [Google Scholar] [CrossRef] [Green Version]
- Menard, J.P.; Fenollar, F.; Henry, M.; Bretelle, F.; Raoult, D. Molecular quantification of Gardnerella vaginalis and Atopobium vaginae loads to predict bacterial vaginosis. Clin. Infect. Dis. 2008, 47, 33–43. [Google Scholar] [CrossRef] [Green Version]
- Yoshimura, K.; Morotomi, N.; Fukuda, K.; Nakano, M.; Kashimura, M.; Hachisuga, T. Intravaginal microbial flora by the 16S rRNA gene sequencing. Am. J. Obstet. Gynecol. 2011, 235. [Google Scholar] [CrossRef]
- Fredricks, D.N.; Fiedler, T.L.; Thomas, K.K.; Oakley, B.B.; Marrazzo, J.M. Targeted PCR for detection of vaginal bacteria associated with bacterial vaginosis. J. Clin. Microbiol. 2007, 45, 3270–3276. [Google Scholar] [CrossRef] [Green Version]
- Prince, A.L.; Antony, K.M.; Ma, J.; Aagaard, K.M. The microbiome and development: A mother’s perspective. Semin. Reprod. Med. 2014, 32, 14–22. [Google Scholar] [CrossRef]
- Aagaard, K.; Riehle, K.; Ma, J.; Segata, N.; Mistretta, T.A.; Coarfa, C. A metagenomic approach to characterization of the vaginal microbiome signature in pregnancy. PLoS ONE 2012, 7. [Google Scholar] [CrossRef]
- Virtanen, S.; Kalliala, I.; Nieminen, P.; Salonen, A. Comparative analysis of vaginal microbiota sampling using 16S rRNA gene analysis. PLoS ONE 2017, 19. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.E.; Wang, Y.; He, Y.; Ji, Y.; Wang, L.P.; Sheng, H.F. Homogeneity of the vaginal microbiome at the cervix, posterior fornix, and vaginal canal in pregnant Chinese women. Microb. Ecol. 2015, 69, 407–414. [Google Scholar] [CrossRef]
- Gorodeski, G.I.; Hopfer, U.; Liu, C.C.; Margles, E. Estrogen acidifies vaginal pH by up-regulation of proton secretion via the apical membrane of vaginal-ectocervical epithelial cells. Endocrinology 2005, 146, 816–824. [Google Scholar] [CrossRef] [Green Version]
- Gorodeski, G.I. Effects of estrogen on proton secretion via the apical membrane in vaginal-ectocervical epithelial cells of postmenopausal women. Menopause 2005, 12, 679–684. [Google Scholar] [CrossRef] [Green Version]
- Walther-Antonio, M.R.; Jeraldo, P.; Berg Miller, M.E.; Yeoman, C.J.; Nelson, K.E.; Wilson, B.A. Pregnancy’s stronghold on the vaginal microbiome. PLoS ONE 2014, 4, e98514. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.Y.; Lai, S.K.; Ensign, L.M.; Zhong, W.; Cone, R.; Hanes, J. The microstructure and bulk rheology of human cervicovaginal mucus are remarkably resistant to changes in pH. Biomacromolecules 2013, 14, 4429–4435. [Google Scholar] [CrossRef] [Green Version]
- Cone, R.A. Barrier properties of mucus. Adv. Drug Deliv. Rev. 2009, 61, 75–85. [Google Scholar] [CrossRef]
- Xie, Y.-D.; Guo, Y.M.; Ren, M.-J.; Yang, J.; Wang, S.F.; Xu, T.-H.; Chen, L.-M.; Liu, Y. The Balance of HCO3− Secretion vs. Reabsorption in the Endometrial Epithelium Regulates Uterine Fluid pH. Front. Physiol. 2018, 9, 12. [Google Scholar] [CrossRef] [Green Version]
- Bolzenius, J.K.; Cushman, R.A.; Perry, G.A. Expression of Na(+)/H(+) exchanger isoforms 1, 2, 3, and 4 in bovine endometrium and the influence of uterine pH at time of fixed-time AI of pregnancy success. Anim. Reprod. Sci. 2016, 171, 98–107. [Google Scholar] [CrossRef]
- O’Hanlon, D.E.; Moench, T.R.; Cone, R.A. Vaginal pH and microbicidal lactic acid when lactobacilli dominate the microbiota. PLoS ONE 2013, 6, e80074. [Google Scholar] [CrossRef]
- Hoyme, U.B.; Huebner, J. Prevention of preterm birth is possible by vaginal pH screening, early diagnosis of bacterial vaginosis or abnormal vaginal flora and treatment. Gynecol. Obstet. Investig. 2010, 70, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Saling, E.; Schreiber, M.; Al-Taie, T. A simple, efficient and inexpensive program for preventing prematurity. J. Perinat. Med. 2001, 29, 199–211. [Google Scholar] [CrossRef] [PubMed]
- Amsel, R.; Totten, P.A.; Spiegel, C.A.; Chen, K.C.; Eschenbach, D.; Holmes, K.K. Nonspecific vaginitis: Diagnostic criteria and microbial and epidemiologic associations. Am. J. Med. 1983, 74, 14–22. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lykke, M.R.; Becher, N.; Haahr, T.; Boedtkjer, E.; Jensen, J.S.; Uldbjerg, N. Vaginal, Cervical and Uterine pH in Women with Normal and Abnormal Vaginal Microbiota. Pathogens 2021, 10, 90. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10020090
Lykke MR, Becher N, Haahr T, Boedtkjer E, Jensen JS, Uldbjerg N. Vaginal, Cervical and Uterine pH in Women with Normal and Abnormal Vaginal Microbiota. Pathogens. 2021; 10(2):90. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10020090
Chicago/Turabian StyleLykke, Malene Risager, Naja Becher, Thor Haahr, Ebbe Boedtkjer, Jørgen Skov Jensen, and Niels Uldbjerg. 2021. "Vaginal, Cervical and Uterine pH in Women with Normal and Abnormal Vaginal Microbiota" Pathogens 10, no. 2: 90. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10020090