
Cat Respiratory Nematodes: Current Knowledge, Novel Data and Warranted Studies on Clinical Features, Treatment and Control

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Clinical Knowledge
2.1. Clinical Signs
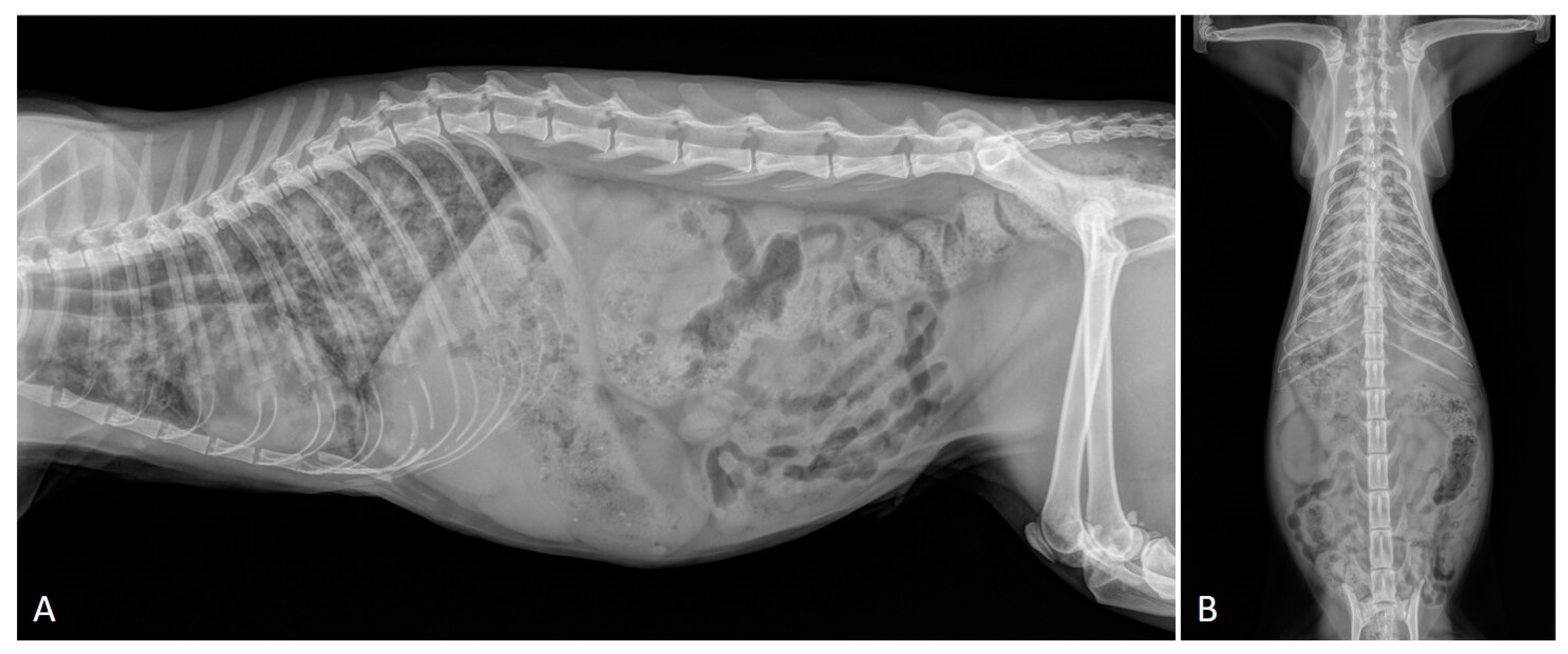
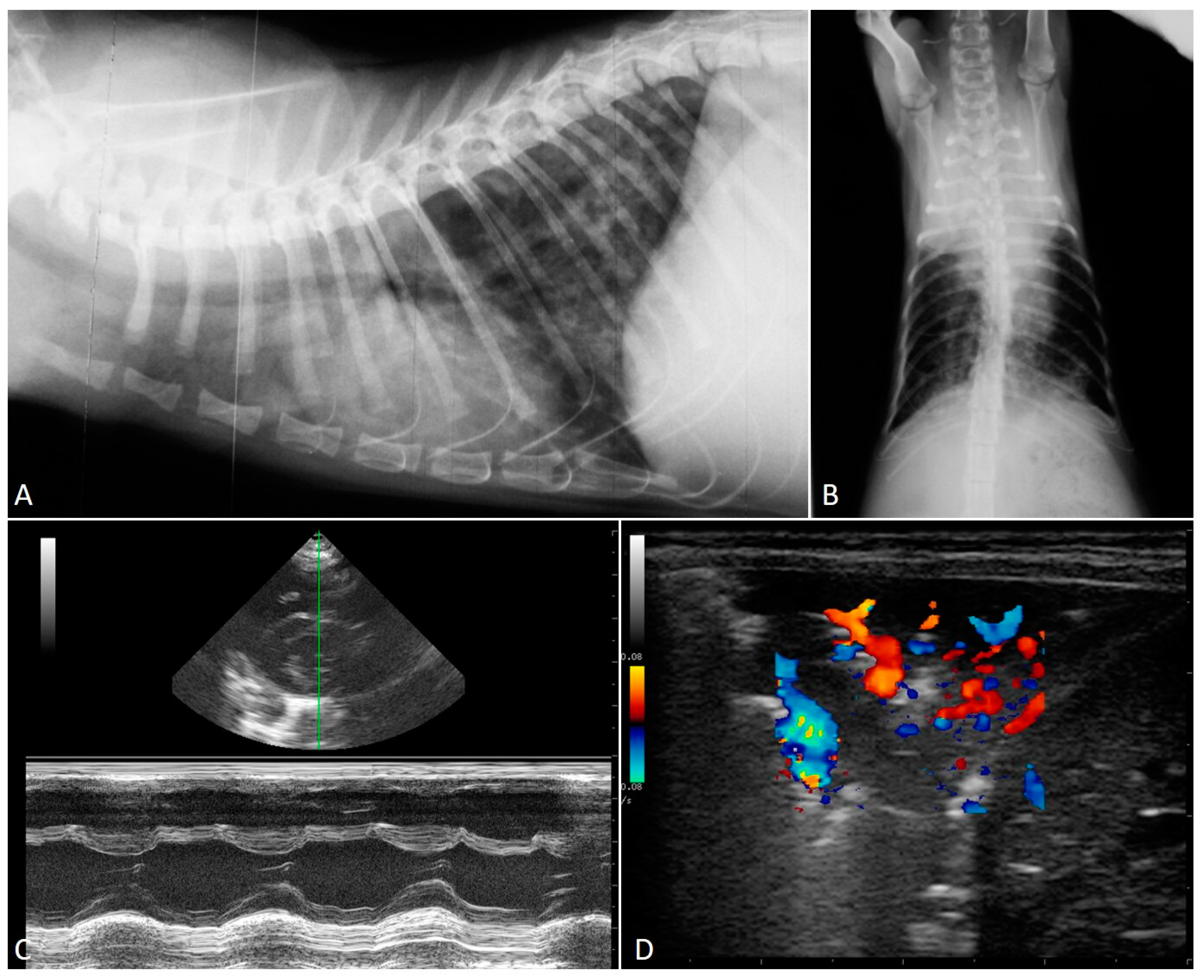
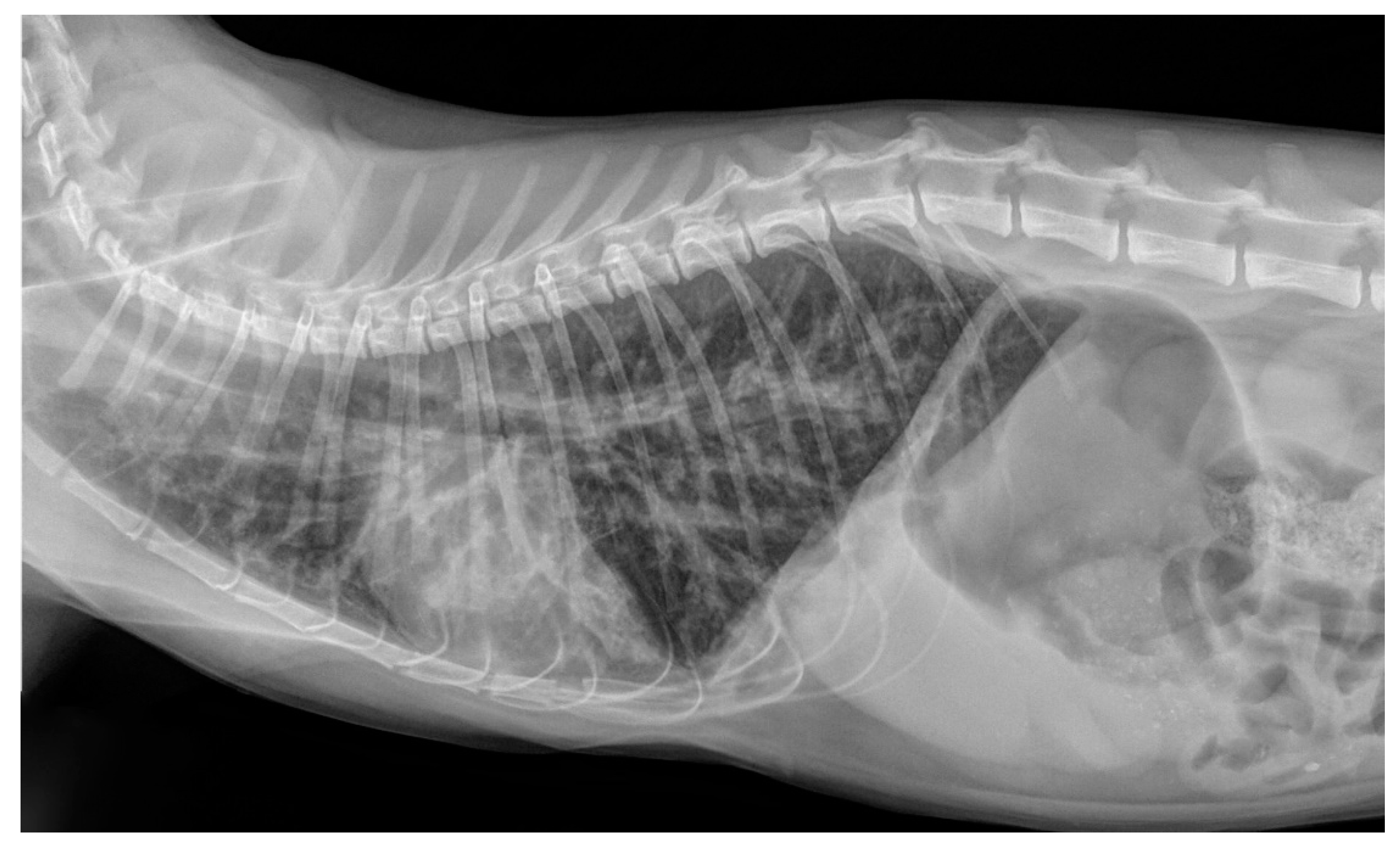
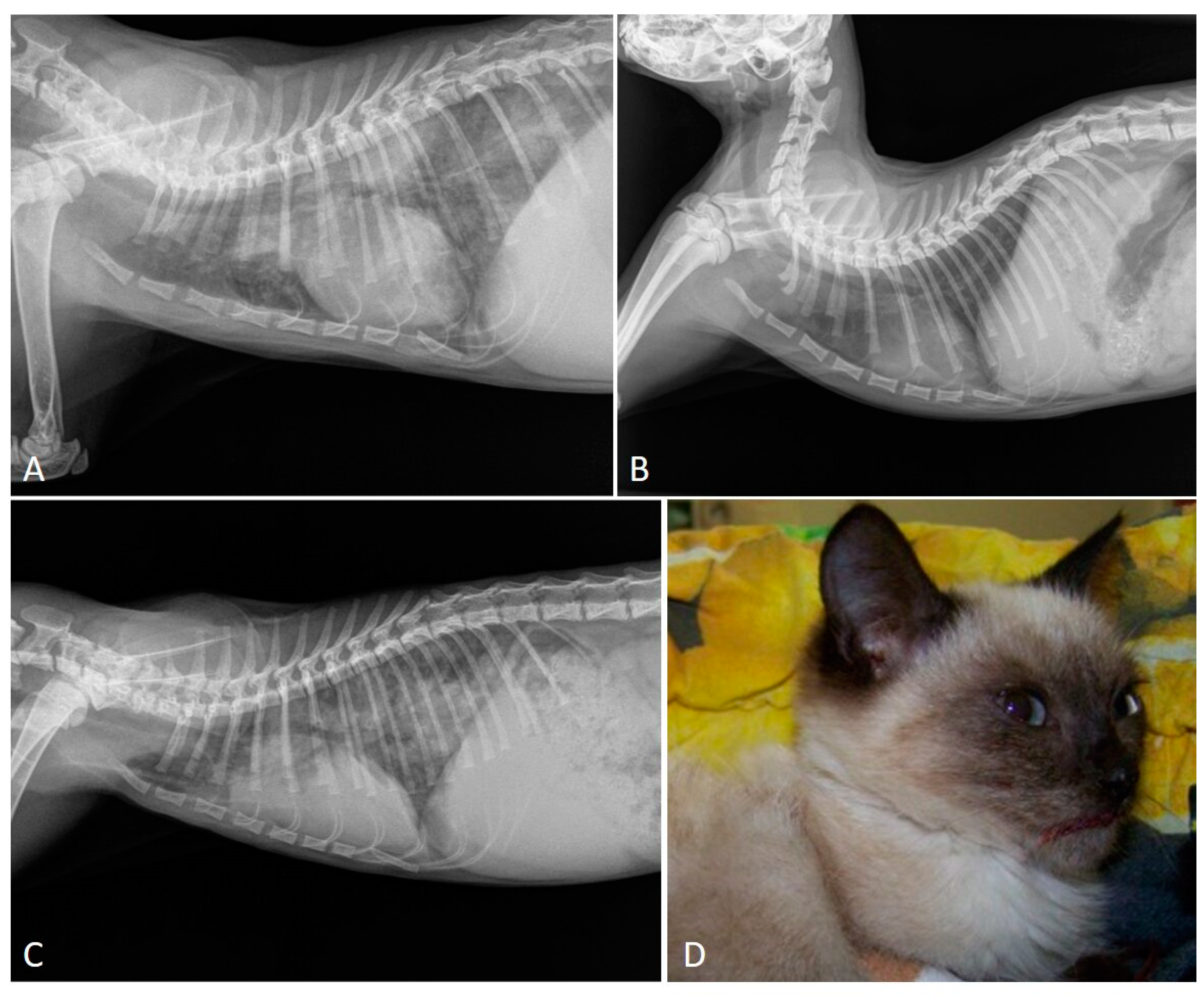
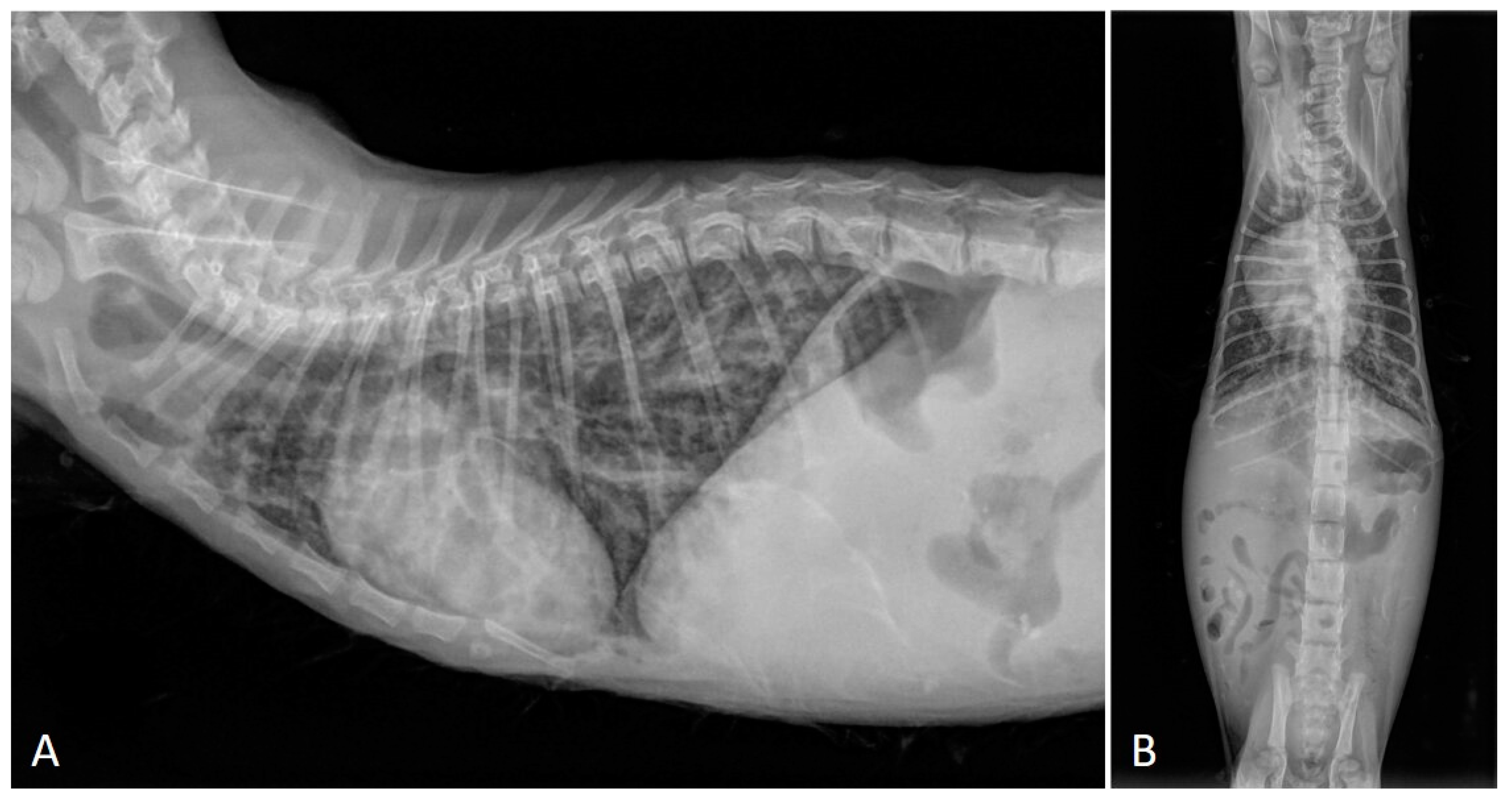
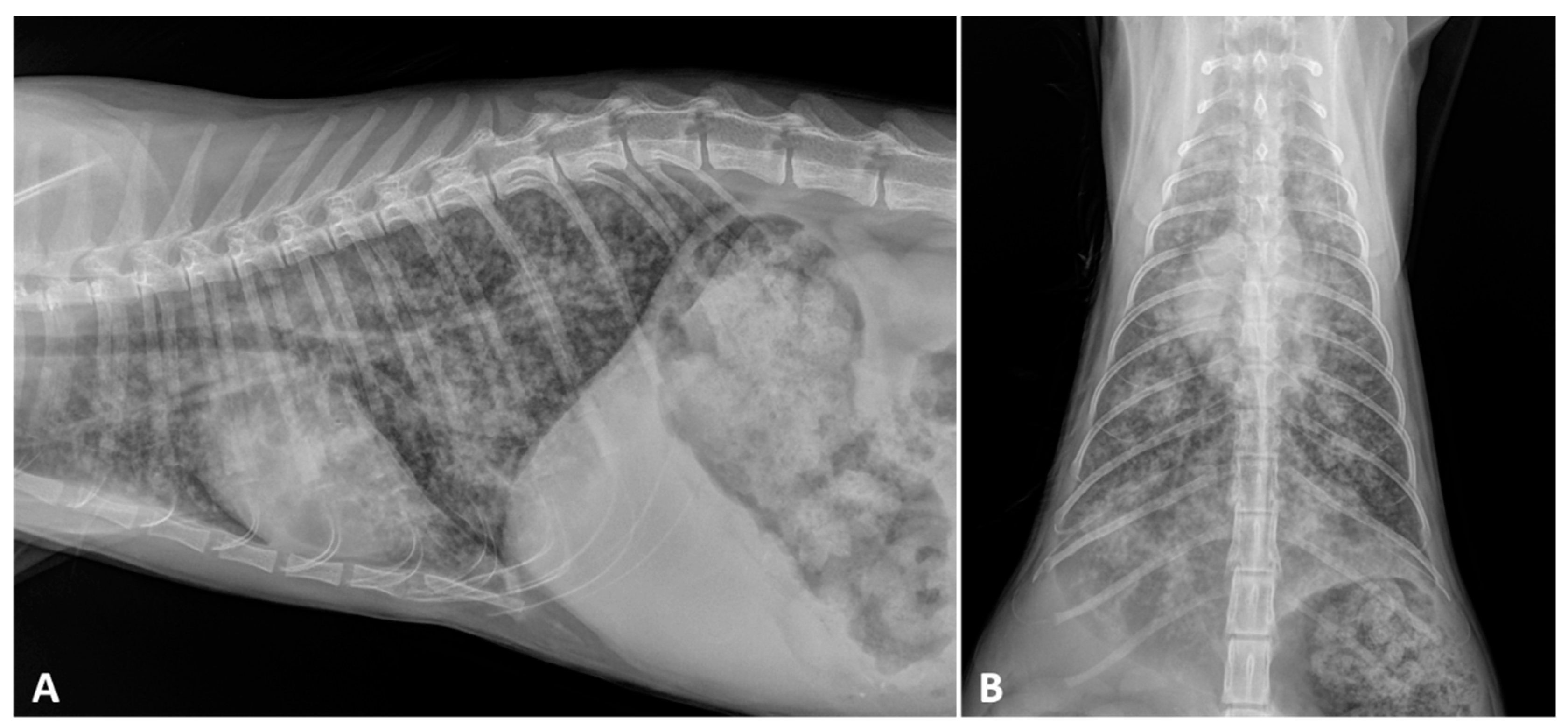
2.2. Radiographic Findings
2.3. Echocardiography
2.4. Computed Tomography Scan
3. Parasitological Diagnosis
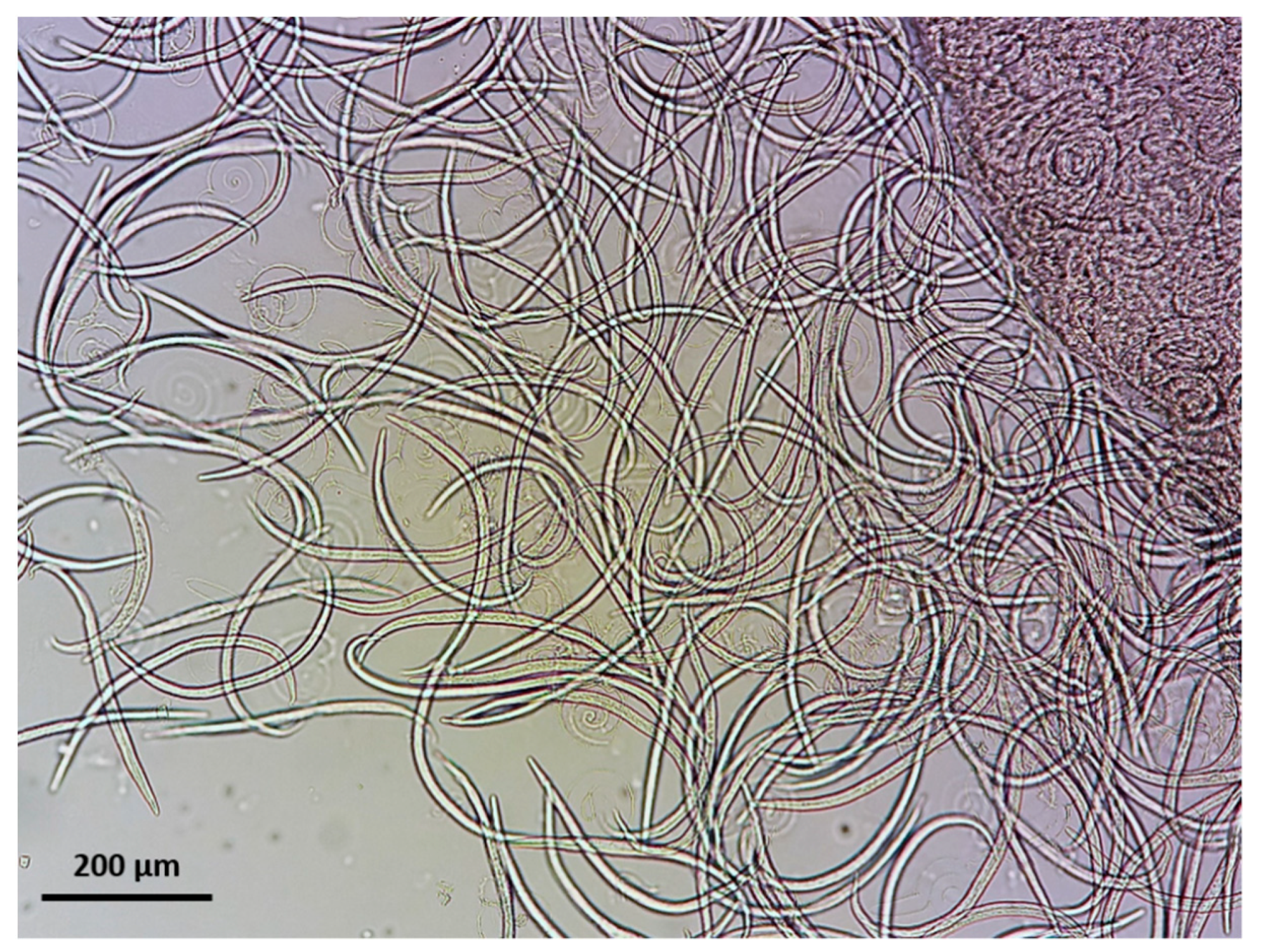
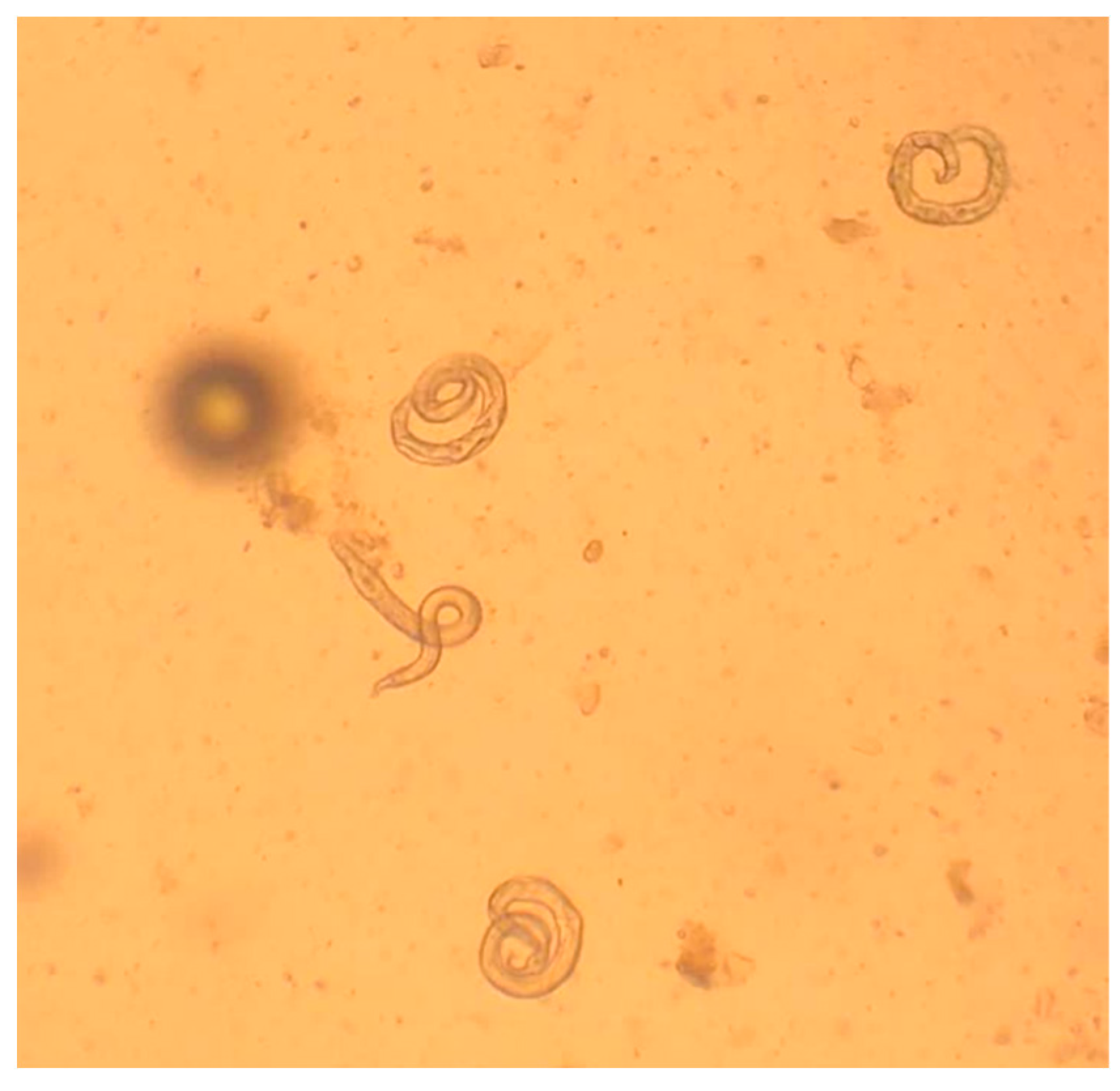
3.1. Microscopic Methods
3.2. Serology
3.3. Endoscopy and Bronchoalveolar Washing
3.4. DNA-Based Assays
4. Treatment and Control
4.1. Aelurostrongylosis
4.1.1. Off Label Treatments
4.1.2. Licensed Products
4.1.3. Novel Acquisitions and Open Perspectives
4.2. Troglostrongylosis
4.2.1. Single Clinical Cases
4.2.2. Labelled Formulation
4.2.3. Novel Acquisitions and Future Perspectives
4.3. Capillariosis
4.3.1. Single Clinical Cases
4.3.2. One Labelled Formulation
4.3.3. Novel Acquisitions and Future Perspectives
4.4. Clinical Efficacy
5. Concluding Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Traversa, D.; Morelli, S.; Di Cesare, A.; Diakou, A. Felid Cardiopulmonary Nematodes: Dilemmas solved and new questions posed. Pathogens 2021, 10, 30. [Google Scholar] [CrossRef] [PubMed]
- Di Cesare, A.; Veronesi, F.; Grillotti, E.; Manzocchi, S.; Perrucci, S.; Beraldo, P.; Cazzin, S.; De Liberato, C.; Barros, L.A.; Simonato, G.; et al. Respiratory nematodes in cat populations of Italy. Parasitol. Res. 2015, 114, 4463–4469. [Google Scholar] [CrossRef] [Green Version]
- Di Cesare, A.; Veronesi, F.; Traversa, D. Felid lungworms and heartworms in Italy: More questions than answers? Trends Parasitol. 2015, 31, 665–675. [Google Scholar] [CrossRef]
- Traversa, D.; Di Cesare, A. Diagnosis and management of lungworm infections in cats: Cornerstones, dilemmas and new avenues. J. Feline Med. Surg. 2016, 18, 7–20. [Google Scholar] [CrossRef] [Green Version]
- Traversa, D.; Di Cesare, A. Feline lungworms: What a dilemma. Trends Parasitol. 2013, 29, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Conboy, G.; Guselle, N.; Schaper, R. Spontaneous shedding of metastrongyloid third-stage larvae by experimentally infected Limax maximus. Parasitol. Res. 2017, 116, 41–54. [Google Scholar] [CrossRef] [PubMed]
- Giannelli, A.; Colella, V.; Abramo, F.; do Nascimento Ramos, R.A.; Falsone, L.; Brianti, E.; Varcasia, A.; Dantas-Torres, F.; Knaus, M.; Fox, M.T.; et al. Release of lungworm larvae from snails in the environment: Potential for alternative transmission pathways. PLoS Negl. Trop. Dis. 2015, 9, e0003722. [Google Scholar] [CrossRef]
- Stepanović, P.; Despotović, D.; Dimitrijević, S.; Ilić, T. Clinical-parasitological screening for respiratory capillariosis in cats in urban environments. Helminthologia 2020, 57, 322–334. [Google Scholar] [CrossRef] [PubMed]
- Taylor, M.A.; Coop, R.L.; Wall, R. Veterinary Parasitology, 3rd ed.; Blackwell Publishing Ltd.: Oxford, UK, 2007. [Google Scholar]
- Bowman, D.D. Respiratory system parasites of the dog and cat (Part II): Trachea and bronchi, and pulmonary vessels. In Companion and Exotic Animal Parasitology; Bowman, D.D., Ed.; International Veterinary Information Service: Ithaca, NY, USA, 2000. [Google Scholar]
- Traversa, D.; Di Cesare, A.; Conboy, G. Canine and feline cardiopulmonary parasitic nematodes in Europe: Emerging and underestimated. Parasies Vectors 2010, 3, 62. [Google Scholar] [CrossRef]
- Traversa, D.; Morelli, S.; Cassini, R.; Crisi, P.E.; Russi, I.; Grillotti, E.; Manzocchi, S.; Simonato, G.; Beraldo, P.; Viglietti, A.; et al. Occurrence of canine and feline extra-intestinal nematodes in key endemic regions of Italy. Acta Trop. 2019, 193, 227–235. [Google Scholar] [CrossRef]
- Salant, H.; Yasur-Landau, D.; Rojas, A.; Otranto, D.; Mazuz, M.L.; Baneth, G. Troglostrongylus brevior is the dominant lungworm infecting feral cats in Jerusalem. Parasitol. Res. 2020, 119, 3443–3450. [Google Scholar] [CrossRef]
- Diakou, A.; Sofroniou, D.; Di Cesare, A.; Kokkinos, P.; Traversa, D. Occurrence and zoonotic potential of endoparasites in cats of Cyprus and a new distribution area for Troglostrongylus brevior. Parasitol. Res. 2017, 116, 3429–3435. [Google Scholar] [CrossRef]
- Diakou, A.; Di Cesare, A.; Barros, L.A.; Morelli, S.; Halos, L.; Beugnet, F.; Traversa, D. Occurrence of Aelurostrongylus abstrusus and Troglostrongylus brevior in domestic cats in Greece. Parasit. Vectors 2015, 8, 590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rehbein, S.; Capári, B.; Duscher, G.; Keidane, D.; Kirkova, Z.; Petkevičius, S.; Rapti, D.; Wagner, A.; Wagner, T.; Chester, S.T.; et al. Efficacy against nematode and cestode infections and safety of a novel topical fipronil, (S)-methoprene, eprinomectin and praziquantel combination product in domestic cats under field conditions in Europe. Vet. Parasitol. 2014, 202, 10–17. [Google Scholar] [CrossRef] [Green Version]
- Knaus, M.; Shukullari, E.; Rapti, D.; Rehbein, S. Efficacy of Broadline against Capillaria aerophila lungworm infection in cats. Parasitol. Res. 2015, 114, 1971–1975. [Google Scholar] [CrossRef] [PubMed]
- Giannelli, A.; Capelli, G.; Joachim, A.; Hinney, B.; Losson, B.; Kirkova, Z.; René-Martellet, M.; Papadopoulos, E.; Farkas, R.; Napoli, E.; et al. Lungworms and gastrointestinal parasites of domestic cats: A European perspective. Int. J. Parasitol. 2017, 47, 517–528. [Google Scholar] [CrossRef] [PubMed]
- Beugnet, F.; Bourdeau, P.; Chalvet-Monfray, K.; Cozma, V.; Farkas, R.; Guillot, J.; Halos, L.; Joachim, A.; Losson, B.; Miró, G.; et al. Parasites of domestic owned cats in Europe: Co-infestations and risk factors. Parasites Vectors 2014, 7, 291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dimzas, D.; Morelli, S.; Traversa, D.; Di Cesare, A.; Van Bourgonie, Y.R.; Breugelmans, K.; Backeljau, T.; di Regalbono, A.F.; Diakou, A. Intermediate gastropod hosts of major feline cardiopulmonary nematodes in an area of wildcat and domestic cat sympatry in Greece. Parasites Vectors 2020, 13, 345. [Google Scholar] [CrossRef]
- Elsheikha, H.M.; Schnyder, M.; Traversa, D.; Di Cesare, A.; Wright, I.; Lacher, D.W. Updates on feline aelurostrongylosis and research priorities for the next decade. Parasites Vectors 2016, 9, 389. [Google Scholar] [CrossRef] [Green Version]
- Grandi, G.; Calvi, L.E.; Venco, L.; Paratici, C.; Genchi, C.; Memmi, D.; Kramer, L.H. Aelurostrongylus abstrusus (cat lungworm) infection in five cats from Italy. Vet. Parasitol. 2005, 134, 177–182. [Google Scholar] [CrossRef]
- Schnyder, M.; Di Cesare, A.; Basso, W.; Guscetti, F.; Riond, B.; Glaus, T.; Crisi, P.; Deplazes, P. Clinical, laboratory and pathological findings in cats experimentally infected with Aelurostrongylus abstrusus. Parasitol. Res. 2014, 113, 1425–1433. [Google Scholar] [CrossRef] [PubMed]
- Philbey, A.W.; Krause, S.; Jefferies, R. Verminous pneumonia and enteritis due to hyperinfection with Aelurostrongylus abstrusus in a kitten. J. Comp. Pathol. 2014, 150, 357–360. [Google Scholar] [CrossRef]
- Crisi, P.E.; Di Cesare, A.; Boari, A. Feline troglostrongylosis: Current epizootiology, clinical features, and therapeutic options. Front. Vet. Sci. 2018, 5, 126. [Google Scholar] [CrossRef] [PubMed]
- Crisi, P.E.; Aste, G.; Traversa, D.; Di Cesare, A.; Febo, E.; Vignoli, M.; Santori, D.; Luciani, A.; Boari, A. Single and mixed feline lungworm infections: Clinical, radiographic and therapeutic features of 26 cases (2013-2015). J. Feline Med. Surg. 2017, 19, 1017–1029. [Google Scholar] [CrossRef] [PubMed]
- Traversa, D.; Di Cesare, A.; Milillo, P.; Iorio, R.; Otranto, D. Aelurostrongylus abstrusus in a feline colony from central Italy: Clinical features, diagnostic procedures and molecular characterization. Parasitol. Res. 2008, 103, 1191–1196. [Google Scholar] [CrossRef]
- Yildiz, K.; Duru, S.Y.; Gokpinar, S. Alteration in blood gases in cats naturally infected with Aelurostrongylus abstrusus. J. Small Anim. Pract. 2011, 52, 376–379. [Google Scholar] [CrossRef]
- Vezzosi, T.; Perrucci, S.; Parisi, F.; Morelli, S.; Maestrini, M.; Mennuni, G.; Traversa, D.; Poli, A. Fatal pulmonary hypertension and right-sided congestive heart failure in a kitten infected with Aelurostrongylus abstrusus. Animals 2020, 10, 2263. [Google Scholar] [CrossRef]
- Mooney, E.T.; Rozanski, E.A.; King, R.G.P.; Sharp, C.R. Spontaneous pneumothorax in 35 cats (2001–2010). J. Feline Med. Surg. 2012, 14, 384–391. [Google Scholar] [CrossRef]
- Miller, B.H.; Roudebush, P.; Ward, H.G. Pleural effusion as a sequela to aelurostrongylosis in a cat. J. Am. Vet. Med. Assoc. 1984, 185, 556–557. [Google Scholar]
- Dirven, M.; Szatmári, V.; van den Ingh, T.; Nijsse, R. Reversible pulmonary hypertension associated with lungworm infection in a young cat. J. Vet. Cardiol. 2012, 14, 465–474. [Google Scholar] [CrossRef]
- Traversa, D.; Guglielmini, C. Feline aelurostrongylosis and canine angiostrongylosis: A challenging diagnosis for two emerging verminous pneumonia infections. Vet. Parasitol. 2008, 157, 163–174. [Google Scholar] [CrossRef] [PubMed]
- Murad, B.; Yankova, S.; Shiron, M.; Tonev, A.; Iliev, P.; Kirkova, Z.; Tsachev, I. Clinical cases of Aelurostrongylus abstrusus and feline immunodeficiency virus co-infection in cats. Tradit. Mod. Vet. Med. 2019, 4, 46–50. [Google Scholar] [CrossRef]
- Ellis, A.E.; Brown, C.A.; Yabsley, M.J. Aelurostrongylus abstrusus larvae in the colon of two cats. J. Vet. Diagn. Investig. 2010, 22, 652–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrs, V.R.; Swinney, G.R.; Martin, P.; Nicoll, R.G. Concurrent Aelurostrongylus abstrusus infection and salmonellosis in a kitten. Aust. Vet. J. 1999, 77, 229–232. [Google Scholar] [CrossRef] [PubMed]
- Giannelli, A.; Passantino, G.; Ramos, R.A.N.; Lo Presti, G.; Lia, R.P.; Brianti, E.; Dantas-Torres, F.; Papadopoulos, E.; Otranto, D. Pathological and histological findings associated with the feline lungworm Troglostrongylus brevior. Vet. Parasitol. 2014, 204, 416–419. [Google Scholar] [CrossRef] [PubMed]
- Jefferies, R.; Vrhovec, M.G.; Wallner, N.; Catalan, D.R. Aelurostrongylus abstrusus and Troglostrongylus sp. (Nematoda: Metastrongyloidea) infections in cats inhabiting Ibiza, Spain. Vet. Parasitol. 2010, 173, 344–348. [Google Scholar] [CrossRef]
- Sykes, J.E. Pediatric feline upper respiratory disease. Vet. Clin. North Am. Small Anim. Pract. 2014, 44, 331–342. [Google Scholar] [CrossRef]
- Diakou, A.; Di Cesare, A.; Aeriniotaki, T.; Traversa, D. First report of Troglostrongylus brevior in a kitten in Greece. Parasitol. Res. 2014, 113, 3895–3898. [Google Scholar] [CrossRef] [PubMed]
- Crisi, P.E.; Traversa, D.; Di Cesare, A.; Luciani, A.; Civitella, C.; Santori, D.; Boari, A. Irreversible pulmonary hypertension associated with Troglostrongylus brevior infection in a kitten. Res. Vet. Sci. 2015, 102, 223–227. [Google Scholar] [CrossRef]
- Di Cesare, A.; di Regalbono, A.; Tessarin, C.; Seghetti, M.; Iorio, R.; Simonato, G.; Traversa, D. Mixed infection by Aelurostrongylus abstrusus and Troglostrongylus brevior in kittens from the same litter in Italy. Parasitol. Res. 2014, 113, 613–618. [Google Scholar] [CrossRef] [Green Version]
- Conboy, G. Helminth parasites of the canine and feline respiratory tract. Vet. Clin. North Am. Small Anim. Pract. 2009, 39, 1109–1126. [Google Scholar] [CrossRef]
- Traversa, D.; Di Cesare, A.; Di Giulio, E.; Castagna, G.; Schaper, R.; Braun, G.; Lohr, B.; Pampurini, F.; Milillo, P.; Strube, K. Efficacy and safety of imidacloprid 10%/moxidectin 1% spot-on formulation in the treatment of feline infection by Capillaria aerophila. Parasitol. Res. 2012, 111, 1793–1798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Traversa, D.; Di Cesare, A.; Milillo, P.; Iorio, R.; Otranto, D. Infection by Eucoleus aerophilus in dogs and cats: Is another extra-intestinal parasitic nematode of pets emerging in Italy? Res. Vet. Sci. 2009, 87, 270–272. [Google Scholar] [CrossRef] [PubMed]
- Elhamiani Khatat, S.; Rosenberg, D.; Benchekroun, G.; Polack, B. Lungworm Eucoleus aerophilus (Capillaria aerophila) infection in a feline immunodeficiency virus-positive cat in France. J. Feline Med. Surg. Open Rep. 2016, 2, 2055116916651649. [Google Scholar] [CrossRef] [Green Version]
- Febo, E.; Crisi, P.E.; Traversa, D.; Luciani, A.; Di Tommaso, M.; Pantaleo, S.; Santori, D.; Di Cesare, A.; Boari, A.; Terragni, R.; et al. Comparison of clinical and imaging findings in cats with single and mixed lungworm infection. J. Feline Med. Surg. 2019, 21, 581–589. [Google Scholar] [CrossRef]
- Genchi, M.; Ferrari, N.; Fonti, P.; De Francesco, I.; Piazza, C.; Viglietti, A. Relation between Aelurostrongylus abstrusus larvae excretion, respiratory and radiographic signs in naturally infected cats. Vet. Parasitol. 2014, 206, 182–187. [Google Scholar] [CrossRef]
- Lacava, G.; Zini, E.; Marchesotti, F.; Domenech, O.; Romano, F.; Manzocchi, S.; Venco, L.; Auriemma, E. Computed tomography, radiology and echocardiography in cats naturally infected with Aelurostrongylus abstrusus. J. Feline Med. Surg. 2017, 19, 446–453. [Google Scholar] [CrossRef]
- Dennler, M.; Bass, D.A.; Gutierrez-Crespo, B.; Schnyder, M.; Guscetti, F.; Di Cesare, A.; Deplazes, P.; Kircher, P.R.; Glaus, T.M. Thoracic computed tomography, angiographic computed tomography, and pathology findings in six cats experimentally infected with aelurostrongylus abstrusus. Vet. Radiol. Ultrasound 2013, 54, 459–469. [Google Scholar] [CrossRef]
- Losonsky, J.M.; Smith, F.G.; Lewis, R.E. Radiographic findings of Aelurostrongylus abstrusus infection in cats. J. Am. Anim. Hosp. Assoc. 1978, 14, 348–355. [Google Scholar]
- Naylor, J.R.; Hamilton, J.M.; Weatherley, A.J. Changes in the ultrastructure of feline pulmonary arteries following infection with the lungworm Aelurostrongylus abstrusus. Br. Vet. J. 1984, 140, 181–190. [Google Scholar] [CrossRef]
- Macdonald, E.S.; Norris, C.R.; Berghaus, R.B.; Griffey, S.M. Clinicopathologic and radiographic features and etiologic agents in cats with histologically confirmed infectious pneumonia: 39 cases (1991–2000). J. Am. Vet. Med. Assoc. 2003, 223, 1142–1150. [Google Scholar] [CrossRef]
- Malik, R.; Wigney, D.I.; Muir, D.B.; Gregory, D.J.; Love, D.N. Cryptococcosis in cats: Clinical and mycological assessment of 29 cases and evaluation of treatment using orally administered fluconazole. J. Med. Vet. Mycol. 1992, 30, 133–144. [Google Scholar] [CrossRef]
- Hamilton, T.A.; Hawkins, E.C.; DeNicola, D.B. Bronchoalveolar lavage and tracheal wash to determine lung involvement in a cat with cryptococcosis. J. Am. Vet. Med. Assoc. 1991, 198, 655–656. [Google Scholar] [CrossRef]
- Mahaffey, M.B. Radiographic-pathologic findings in experimental Aelurostrongylus abstrusus infection in cats. Vet. Radiol. 1979, 20, 81. [Google Scholar] [CrossRef]
- Losonsky, J.M.; Thrall, D.E.; Prestwood, A.K. Radiographic evaluation of pulmonary abnormalities after Aelurostrongylus abstrusus inoculation in cats. Am. J. Vet. Res. 1983, 44, 478–482. [Google Scholar] [PubMed]
- Hawley, M.M.; Johnson, L.R.; Traversa, D.; Bucy, D.; Vernau, K.M.; Vernau, W. Respiratory distress associated with lungworm infection in a kitten. J. Feline Med. Surg. Open Rep. 2016, 2, 2055116916675801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brianti, E.; Gaglio, G.; Giannetto, S.; Annoscia, G.; Latrofa, M.S.; Dantas-Torres, F.; Traversa, D.; Otranto, D. Troglostrongylus brevior and Troglostrongylus subcrenatus (Strongylida: Crenosomatidae) as agents of broncho-pulmonary infestation in domestic cats. Parasites Vectors 2012, 5, 178. [Google Scholar] [CrossRef] [Green Version]
- Traversa, D.; Salda, L.D.; Diakou, A.; Sforzato, C.; Romanucci, M.; di Regalbono, A.F.; Lorio, R.; Colaberardino, V.; Di Cesare, A. Fatal patent troglostrongylosis in a litter of kittens. J. Parasitol. 2018, 104, 418–423. [Google Scholar] [CrossRef]
- Venco, L.; Clinica Veterinaria Lago Maggiore, Dormelletto, Novara, Italy. Personal communication.
- Stockdale, P.H. The pathogenesis of the lesions elicited by Aelurostrongylus abstrusus during its prepatent period. Pathol. Vet. 1970, 7, 102–115. [Google Scholar] [CrossRef] [PubMed]
- Prather, A.B.; Berry, C.R.; Thrall, D.E. Use of radiography in combination with computed tomography for the assessment of noncardiac thoracic disease in the dog and cat. Vet. Radiol. Ultrasound. 2005, 46, 114–121. [Google Scholar] [CrossRef]
- Nafe, L.A.; DeClue, A.E.; Lee-Fowler, T.M.; Eberhardt, J.M.; Reinero, C.R. Evaluation of biomarkers in bronchoalveolar lavage fluid for discrimination between asthma and chronic bronchitis in cats. Am. J. Vet. Res. 2010, 71, 583–591. [Google Scholar] [CrossRef]
- Payo-Puente, P.; Diez, A.; Gonzalo-Orden, J.M.; Notomi, M.K.; Rodríguez-Altónaga, J.A.; Rojo-Vázquez, F.A.; Orden, M.A. Computed tomography in cats infected by Aelurostrongylus abstrusus: 2 clinic cases. Int. J. Appl. Res. Vet. Med. 2005, 3, 339–343. [Google Scholar]
- Forrester, S.; Moon, M.; Jacobson, J. Diagnostic evaluation of dogs and cats with respiratory distress. Compedium 2001, 23, 56–59. [Google Scholar]
- Fahy, J.V.; Dickey, B.F. Airway mucus function and dysfunction. N. Engl. J. Med. 2010, 363, 2233–2247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lacorcia, L.; Gasser, R.B.; Anderson, G.A.; Beveridge, I. Comparison of bronchoalveolar lavage fluid examination and other diagnostic techniques with the Baermann technique for detection of naturally occurring Aelurostrongylus abstrusus infection in cats. J. Am. Vet. Med. Assoc. 2009, 235, 43–49. [Google Scholar] [CrossRef]
- Thienpont, D.; Rochette, F.; Vanparijs, O.F.J. Diagnosing Helminthiasis by Coprological Examination, 2nd ed.; Janssen Research Foundation: Beerse, Belgium, 1986. [Google Scholar]
- Faust, E.C.; D’Antoni, J.S.; Odom, V.; Miller, M.J.; Peres, C.; Sawitz, W.; Thomen, L.F.; Tobie, J.; Walker, J.H. A critical study of clinical laboratory technics for the diagnosis of protozoan cysts and helminth eggs in feces 1. Am. J. Trop. Med. Hyg. 1938, s1-18, 169–183. [Google Scholar] [CrossRef]
- Manual of Veterinary Parasitological Laboratory Techniques; Ministry of Agriculture, Fisheries and Food (MAAF): London, UK, 1986.
- Brianti, E.; Giannetto, S.; Dantas-Torres, F.; Otranto, D. Lungworms of the genus Troglostrongylus (Strongylida: Crenosomatidae): Neglected parasites for domestic cats. Vet. Parasitol. 2014, 202, 104–112. [Google Scholar] [CrossRef]
- Diakou, A.; Psalla, D.; Migli, D.; Di Cesare, A.; Youlatos, D.; Marcer, F.; Traversa, D. First evidence of the European wildcat (Felis silvestris silvestris) as definitive host of Angiostrongylus chabaudi. Parasitol. Res. 2016, 115, 1235–1244. [Google Scholar] [CrossRef]
- Otranto, D.; Brianti, E.; Dantas-Torres, F. Troglostrongylus brevior and a nonexistent “dilemma”. Trends Parasitol. 2013, 29, 517–518. [Google Scholar] [CrossRef] [PubMed]
- Geng, J.; Elsemore, D.A.; Oudin, N.; Ketzis, J.K. Diagnosis of feline whipworm infection using a coproantigen ELISA and the prevalence in feral cats in southern Florida. Vet. Parasitol. Reg. Stud. Rep. 2018, 14, 181–186. [Google Scholar] [CrossRef]
- Traversa, D.; Di Cesare, A.; Lia, R.P.; Castagna, G.; Meloni, S.; Heine, J.; Strube, K.; Milillo, P.; Otranto, D.; Meckes, O.; et al. New insights into morphological and biological features of Capillaria aerophila (Trichocephalida, Trichuridae). Parasitol. Res. 2011, 109, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Koyama, K. Characteristics and incidence of large eggs in Trichuris muris. Parasitol. Res. 2013, 112, 1925–1928. [Google Scholar] [CrossRef]
- Borba, V.; Enoki, M.; Lopes-Torres, E.J.; Machado-Silva, J.R.; Iñiguez, A.M. New data on eggshell structure of capillariid species: A SEM perspective. Parasitol. Res. 2021, 120, 963–970. [Google Scholar] [CrossRef]
- Hamilton, J.M.; Roberts, R.J. Immunofluorescence as a diagnostic procedure in lungworm disease of the cat. Vet. Rec. 1968, 83, 401–403. [Google Scholar] [CrossRef] [PubMed]
- Briggs, K.R.; Yaros, J.P.; Liotta, J.L.; Lucio-Forster, A.; Lee, A.C.; Bowman, D.D. Detecting Aelurostrongylus abstrusus-specific IgG antibody using an immunofluorescence assay. J. Feline Med. Surg. 2013, 15, 1114–1118. [Google Scholar] [CrossRef]
- Zottler, E.M.; Strube, C.; Schnyder, M. Detection of specific antibodies in cats infected with the lung nematode Aelurostrongylus abstrusus. Vet. Parasitol. 2017, 235, 75–82. [Google Scholar] [CrossRef] [Green Version]
- Von Holtum, C.; Strube, C.; Schnieder, T.; von Samson-Himmelstjerna, G. Development and evaluation of a recombinant antigen-based ELISA for serodiagnosis of cattle lungworm. Vet. Parasitol. 2008, 151, 218–226. [Google Scholar] [CrossRef]
- Cavalera, M.A.; Schnyder, M.; Gueldner, E.K.; Furlanello, T.; Iatta, R.; Brianti, E.; Strube, C.; Colella, V.; Otranto, D. Serological survey and risk factors of Aelurostrongylus abstrusus infection among owned cats in Italy. Parasitol. Res. 2019, 118, 2377–2382. [Google Scholar] [CrossRef]
- Di Cesare, A.; Gueldner, E.K.; Traversa, D.; Veronesi, F.; Morelli, S.; Crisi, P.E.; Pampurini, F.; Strube, C.; Schnyder, M. Seroprevalence of antibodies against the cat lungworm Aelurostrongylus abstrusus in cats from endemic areas of Italy. Vet. Parasitol. 2019, 272, 13–16. [Google Scholar] [CrossRef] [PubMed]
- Gueldner, E.K.; Gilli, U.; Strube, C.; Schnyder, M. Seroprevalence, biogeographic distribution and risk factors for Aelurostrongylus abstrusus infections in Swiss cats. Vet. Parasitol. 2019, 266, 27–33. [Google Scholar] [CrossRef]
- Morelli, S.; Diakou, A.; Di Cesare, A.; Schnyder, M.; Colombo, M.; Strube, C.; Dimzas, D.; Latino, R.; Traversa, D. Feline lungworms in Greece: Copromicroscopic, molecular and serological study. Parasitol. Res. 2020, 119, 2877–2883. [Google Scholar] [CrossRef]
- Ribeiro, V.M.; Lima, W.S. Larval production of cats infected and re-infected with Aelurostrongylus abstrusus (Nematoda: Protostrongylidae). Rev. Med. Vet. 2001, 152, 815–820. [Google Scholar]
- Crisi, P.E.; Johnson, L.R.; Di Cesare, A.; De Santis, F.; Di Tommaso, M.; Morelli, S.; Pantaleo, S.; Luciani, A.; Schaper, R.; Pampurini, F.; et al. Evaluation of bronchoscopy and bronchoalveolar lavage findings in cats with Aelurostrongylus abstrusus in comparison to cats with feline bronchial disease. Front. Vet. Sci. 2019, 6, 337. [Google Scholar] [CrossRef] [PubMed]
- Traversa, D.; Iorio, R.; Otranto, D. Diagnostic and clinical implications of a nested PCR specific for ribosomal DNA of the feline lungworm Aelurostrongylus abstrusus (Nematoda, Strongylida). J. Clin. Microbiol. 2008, 46, 1811–1817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Cesare, A.; Iorio, R.; Crisi, P.; Paoletti, B.; Di Costanzo, R.; Dimitri, C.F.; Traversa, D. Treatment of Troglostrongylus brevior (Metastrongyloidea, Crenosomatidae) in mixed lungworm infections using spot-on emodepside. J. Feline Med. Surg. 2015, 17, 181–185. [Google Scholar] [CrossRef]
- Di Cesare, A.; Veronesi, F.; di Regalbono, A.F.; Iorio, R.; Traversa, D. Novel molecular assay for simultaneous identification of neglected lungworms and heartworms affecting cats. J. Clin. Microbiol. 2015, 53, 3009–3013. [Google Scholar] [CrossRef] [Green Version]
- Traversa, D.; Romanucci, M.; Di Cesare, A.; Malatesta, D.; Cassini, R.; Iorio, R.; Seghetti, M.; Della Salda, L. Gross and histopathological changes associated with Aelurostrongylus abstrusus and Troglostrongylus brevior in a kitten. Vet. Parasitol. 2014, 201, 158–162. [Google Scholar] [CrossRef]
- Traversa, D.; Lepri, E.; Veronesi, F.; Paoletti, B.; Simonato, G.; Diaferia, M.; Di Cesare, A. Metastrongyloid infection by Aelurostrongylus abstrusus, Troglostrongylus brevior and Angiostrongylus chabaudi in a domestic cat. Int. J. Parasitol. 2015, 45, 685–690. [Google Scholar] [CrossRef]
- Fuehrer, H.-P.; Morelli, S.; Bleicher, J.; Brauchart, T.; Edler, M.; Eisschiel, N.; Hering, T.; Lercher, S.; Mohab, K.; Reinelt, S.; et al. Detection of Crenosoma spp., Angiostrongylus vasorum and Aelurostrongylus abstrusus in gastropods in Eastern Austria. Pathogens 2020, 9, 1046. [Google Scholar] [CrossRef]
- Di Cesare, A.; Morelli, S.; Colombo, M.; Simonato, G.; Veronesi, F.; Marcer, F.; Diakou, A.; D’Angelosante, R.; Pantchev, N.; Psaralexi, E.; et al. Is angiostrongylosis a realistic threat for domestic cats? Front. Vet. Sci. 2020, 7, 195. [Google Scholar] [CrossRef]
- Di Cesare, A.; Di Francesco, G.; di Regalbono, A.F.; Eleni, C.; De Liberato, C.; Marruchella, G.; Iorio, R.; Malatesta, D.; Romanucci, M.R.; Bongiovanni, L.; et al. Retrospective study on the occurrence of the feline lungworms Aelurostrongylus abstrusus and Troglostrongylus spp. in endemic areas of Italy. Vet. J. 2015, 203, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Crisi, P.E.; Di Cesare, A.; Traversa, D.; Vignoli, M.; Morelli, S.; Di Tommaso, M.; De Santis, F.; Pampurini, F.; Schaper, R.; Boari, A. Controlled field study evaluating the clinical efficacy of a topical formulation containing emodepside and praziquantel in the treatment of natural cat aelurostrongylosis. Vet. Rec. 2020, 187, E34. [Google Scholar] [CrossRef] [Green Version]
- Annoscia, G.; Latrofa, M.S.; Campbell, B.E.; Giannelli, A.; Ramos, R.A.N.; Dantas-Torres, F.; Brianti, E.; Otranto, D. Simultaneous detection of the feline lungworms Troglostrongylus brevior and Aelurostrongylus abstrusus by a newly developed duplex-PCR. Vet. Parasitol. 2014, 199, 172–178. [Google Scholar] [CrossRef]
- Giannelli, A.; Ramos, R.A.N.; Annoscia, G.; Di Cesare, A.; Colella, V.; Brianti, E.; Dantas-Torres, F.; Mutafchiev, Y.; Otranto, D. Development of the feline lungworms Aelurostrongylus abstrusus and Troglostrongylus brevior in Helix aspersa snails. Parasitology 2014, 141, 563–569. [Google Scholar] [CrossRef]
- Di Cesare, A.; Otranto, D.; Latrofa, M.S.; Veronesi, F.; Perrucci, S.; Lalosevic, D.; Gherman, C.M.; Traversa, D. Genetic variability of Eucoleus aerophilus from domestic and wild hosts. Res. Vet. Sci. 2014, 96, 512–515. [Google Scholar] [CrossRef] [PubMed]
- Foster, S.F.; Martin, P. Lower respiratory tract infections in cats: Reaching beyond empirical therapy. J. Feline Med. Surg. 2011, 13, 313–332. [Google Scholar] [CrossRef] [PubMed]
- Lewis, D.T.; Merchant, S.R.; Neer, T.M. Ivermectin toxicosis in a kitten. J. Am. Vet. Med. Assoc. 1994, 205, 584–586. [Google Scholar] [PubMed]
- Foster, S.F.; Martin, P.; Allan, G.S.; Barrs, V.R.; Malik, R. Lower respiratory tract infections in cats: 21 cases (1995–2000). J. Feline Med. Surg. 2004, 6, 167–180. [Google Scholar] [CrossRef]
- Reinhardt, S.; Ottenjann, M.; Schunack, B.; Kohn, B. Lungworm disease (Aelurostrongylus abstrusus) in a cat. Kleintierpraxis 2004, 49, 239–246. [Google Scholar]
- Iannino, F.; Iannetti, L.; Paganico, D.; Vulpiani, M.P. Evaluation of the efficacy of selamectin spot-on in cats infested with Aelurostrongylus abstrusus (Strongylida, Filariodidae) in a Central Italy cat shelter. Vet. Parasitol. 2013, 197, 258–262. [Google Scholar] [CrossRef]
- Traversa, D.; Di Cesare, A.; Milillo, P.; Lohr, B.; Iorio, R.; Pampurini, F.; Schaper, R.; Paoletti, B.; Heine, J. Efficacy and safety of imidacloprid 10%/moxidectin 1% spot-on formulation in the treatment of feline aelurostrongylosis. Parasitol. Res. 2009, 105 Suppl, 55–62. [Google Scholar] [CrossRef]
- Traversa, D.; Milillo, P.; Di Cesare, A.; Lohr, B.; Iorio, R.; Pampurini, F.; Schaper, R.; Bartolini, R.; Heine, J. Efficacy and safety of emodepside 2.1%/praziquantel 8.6% spot-on formulation in the treatment of feline aelurostrongylosis. Parasitol. Res. 2009, 105, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Böhm, C.; Petry, G.; Schaper, R.; Wolken, S.; Strube, C. Prevention of Lactogenic Toxocara cati Infections in kittens by application of an emodepside/praziquantel spot-on (Profender®) to the pregnant queen. Parasitol. Res. 2015, 114, 175–184. [Google Scholar] [CrossRef] [Green Version]
- Heuer, L.; Petry, G.; Pollmeier, M.; Schaper, R.; Deuster, K.; Schmidt, H.; Blazejak, K.; Strube, C.; Di Cesare, A.; Traversa, D.; et al. Efficacy of imidacloprid 10%/moxidectin 1% spot-on formulation (Advocate®) in the prevention and treatment of feline aelurostrongylosis. Parasites Vectors 2020, 13, 65. [Google Scholar] [CrossRef]
- Knaus, M.; Chester, S.T.; Rosentel, J.; Kühnert, A.; Rehbein, S. Efficacy of a novel topical combination of fipronil, (S)-methoprene, eprinomectin and praziquantel against larval and adult stages of the cat lungworm, Aelurostrongylus abstrusus. Vet. Parasitol. 2014, 202, 64–68. [Google Scholar] [CrossRef] [Green Version]
- Giannelli, A.; Brianti, E.; Varcasia, A.; Colella, V.; Tamponi, C.; Di Paola, G.; Knaus, M.; Halos, L.; Beugnet, F.; Otranto, D. Efficacy of Broadline® spot-on against Aelurostrongylus abstrusus and Troglostrongylus brevior lungworms in naturally infected cats from Italy. Vet. Parasitol. 2015, 209, 273–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raue, K.; Rohdich, N.; Hauck, D.; Zschiesche, E.; Morelli, S.; Traversa, D.; Di Cesare, A.; Roepke, R.K.A.; Strube, C. Efficacy of Bravecto ® Plus spot-on solution for cats (280 mg/ml fluralaner and 14 mg/ml moxidectin) for the prevention of aelurostrongylosis in experimentally infected cats. Parasites Vectors 2021, 14, 110. [Google Scholar] [CrossRef] [PubMed]
- Knaus, M.; Visser, M.; Mayr, S.; Rehbein, S. Efficacy of a topical combination of eprinomectin, praziquantel, fipronil and (S)-methoprene against developing and adult Troglostrongylus brevior lungworms (Nematoda, Crenosomatidae) in cats. Vet. Parasitol. X 2020, 4, 100032. [Google Scholar] [CrossRef]
- Diakou, A.; Morelli, S.; Dimzas, D.; Di Cesare, A.; Capelli, G.; Parrinello, C.; Pollmeier, M.; Schaper, R.; Traversa, D. Efficacy of a moxidectin/imidacloprid spot-on formulation (Advocate®) for the treatment of Troglostrongylus brevior in naturally infected cats in a field study in Greece. Parasites Vectors 2019, 12, 519. [Google Scholar] [CrossRef]
- Traversa, D.; Veronesi, F.; Danesi, P.; Morelli, S.; Crisi, P.E.; Morganti, G.; Iorio, R.; Pampurini, F.; Schaper, R.; Santoro, A.; et al. Pilot study evaluating the efficacy of a topical formulation containing emodepside and praziquantel in the treatment of natural feline troglostrongylosis. Parasites Vectors 2019, 12, 97. [Google Scholar] [CrossRef] [Green Version]
- Morelli, S.; di Regalbono, A.F.; Russi, I.; Crisi, P.E.; Simonato, G.; Pampurini, F.; Traversa, D. Efficacy of a spot-on formulation containing imidacloprid and moxidectin in the chemoprevention of cardiopulmonary nematodes of dogs and cats. Summa Anim. Compagnia 2018, 35, 33–38. [Google Scholar]
- Little, S.E.; Hostetler, J.A.; Thomas, J.E.; Bailey, K.L.; Barrett, A.W.; Gruntmeir, K.; Gruntmeir, J.; Starkey, L.A.; Basel, C.; Blagburn, B.L. Moxidectin steady state prior to inoculation protects cats from subsequent, repeated infection with Dirofilaria immitis. Parasites Vectors 2015, 8, 107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Endres, W.A. Levamisole in treatment of Capillaria aerophilla in a cat. (A case report). Vet. Med. Small Anim. Clin. 1976, 71, 1553. [Google Scholar]
- Norsworthy, G. Feline lungworm treatment case report. Feline Pract. 1975, 5, 14. [Google Scholar]
- Barrs, V.R.; Martin, P.; Nicoll, R.G.; Beatty, J.A.; Malik, R. Pulmonary cryptococcosis and Capillaria aerophila infection in an FIV-positive cat. Aust. Vet. J. 2000, 78, 154–158. [Google Scholar] [CrossRef]
- Di Cesare, A.; Veronesi, F.; Capelli, G.; Deuster, K.; Schaper, R.; Basano, F.S.; Nazzari, R.; Paoletti, B.; Traversa, D. Evaluation of the efficacy and safety of aniImidacloprid 10% / moxidectin 1% spot-on formulation (Advocate®, Advantage® Multi) in cats naturally infected with Capillaria aerophila. Parasitol. Res. 2017, 116, 55–64. [Google Scholar] [CrossRef] [Green Version]
- Rohdich, N.; Zschiesche, E.; Wolf, O.; Loehlein, W.; Pobel, T.; Gil, M.J.; Roepke, R.K.A. Field effectiveness and safety of fluralaner plus moxidectin (Bravecto® Plus) against ticks and fleas: A European randomized, blinded, multicenter field study in naturally-infested client-owned cats. Parasites Vectors 2018, 11, 598. [Google Scholar] [CrossRef]
- Traversa, D.; Venco, L. Parassitologia clinica del cane e del gatto; Le Point Veterinaire Italie: Milano, Italy, 2018; ISBN 8899211345. [Google Scholar]
- Gerdin, J.A.; Slater, M.R.; Makolinski, K.V.; Looney, A.L.; Appel, L.D.; Martin, N.M.; McDonough, S.P. Post-mortem findings in 54 cases of anesthetic associated death in cats from two spay-neuter programs in New York State. J. Feline Med. Surg. 2011, 13, 959–966. [Google Scholar] [CrossRef]
- Diakou, A.; Dimzas, D.; Astaras, C.; Savvas, I.; Di Cesare, A.; Morelli, S.; Neofitos, Κ. Clinical investigations and treatment outcome in a European wildcat (Felis silvestris silvestris) infected by cardio-pulmonary nematodes. Vet. Parasitol. Reg. Stud. Rep. 2020, 19, 100357. [Google Scholar] [CrossRef]
- Stevanović, O.; Diakou, A.; Morelli, S.; Paraš, S.; Trbojević, I.; Nedić, D.; Sladojević, Ž.; Kasagić, D.; Di Cesare, A. Severe verminous pneumonia caused by natural mixed infection with Aelurostrongylus abstrusus and Angiostrongylus chabaudi in a European wildcat from Western Balkan area. Acta Parasitol. 2019, 64, 411–417. [Google Scholar] [CrossRef]
- Morelli, S.; Traversa, D.; Colombo, M.; Raue, K.; Strube, C.; Pollmeier, M.; Di Cesare, A. The effect of the hibernation on the larval development of Troglostrongylus brevior in the land snail Cornu aspersum. Vet. Parasitol. 2020, 282, 109123. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parasite | Anterior End | Posterior End | Length/Reference |
|---|---|---|---|
| Aelurostrongylus abstrusus |
|
| 300–400 ± 21.3 / [5] |
| 360–415 (399.1 ± 11.3) / [74] | |||
| 210.4–495.1 / [18] | |||
| Troglostrongylus brevior |
|
| 300–521 / [5] |
| 300–357 (338.8 ± 15.6) / [74] | |||
| 203.2–382.2 / [18] |
| Molecule | Aa | Tb | Ca | Off Label | Refs |
|---|---|---|---|---|---|
| 2.1% Emodepside | Yes (T) | No | No | Tb (T) Ca (T) | [60,90,107,108,122] |
| 1% Moxidectin | Yes (T/P 1) | No | Yes (T) | Aa (P 4) Tb (T/P 5) | [106,109,112,114,121] |
| 0.4% Eprinomectin | Yes (T/P 2) | Yes (T/P 3) | No | Ca (T) | [18,26,110,111,113] |
| Milbemycin oxime 6 | No | No | No | Aa Tb (T) Ca (T) | [26,42] |
| 6% Selamectin | No | No | No | Aa (T) | [22,104,105] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morelli, S.; Diakou, A.; Colombo, M.; Di Cesare, A.; Barlaam, A.; Dimzas, D.; Traversa, D. Cat Respiratory Nematodes: Current Knowledge, Novel Data and Warranted Studies on Clinical Features, Treatment and Control. Pathogens 2021, 10, 454. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10040454
Morelli S, Diakou A, Colombo M, Di Cesare A, Barlaam A, Dimzas D, Traversa D. Cat Respiratory Nematodes: Current Knowledge, Novel Data and Warranted Studies on Clinical Features, Treatment and Control. Pathogens. 2021; 10(4):454. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10040454
Chicago/Turabian StyleMorelli, Simone, Anastasia Diakou, Mariasole Colombo, Angela Di Cesare, Alessandra Barlaam, Dimitris Dimzas, and Donato Traversa. 2021. "Cat Respiratory Nematodes: Current Knowledge, Novel Data and Warranted Studies on Clinical Features, Treatment and Control" Pathogens 10, no. 4: 454. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10040454