
Very High Fascioliasis Intensities in Schoolchildren from Nile Delta Governorates, Egypt: The Old World Highest Burdens Found in Lowlands

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
3. Discussion
3.1. Characterisation of the High Intensities
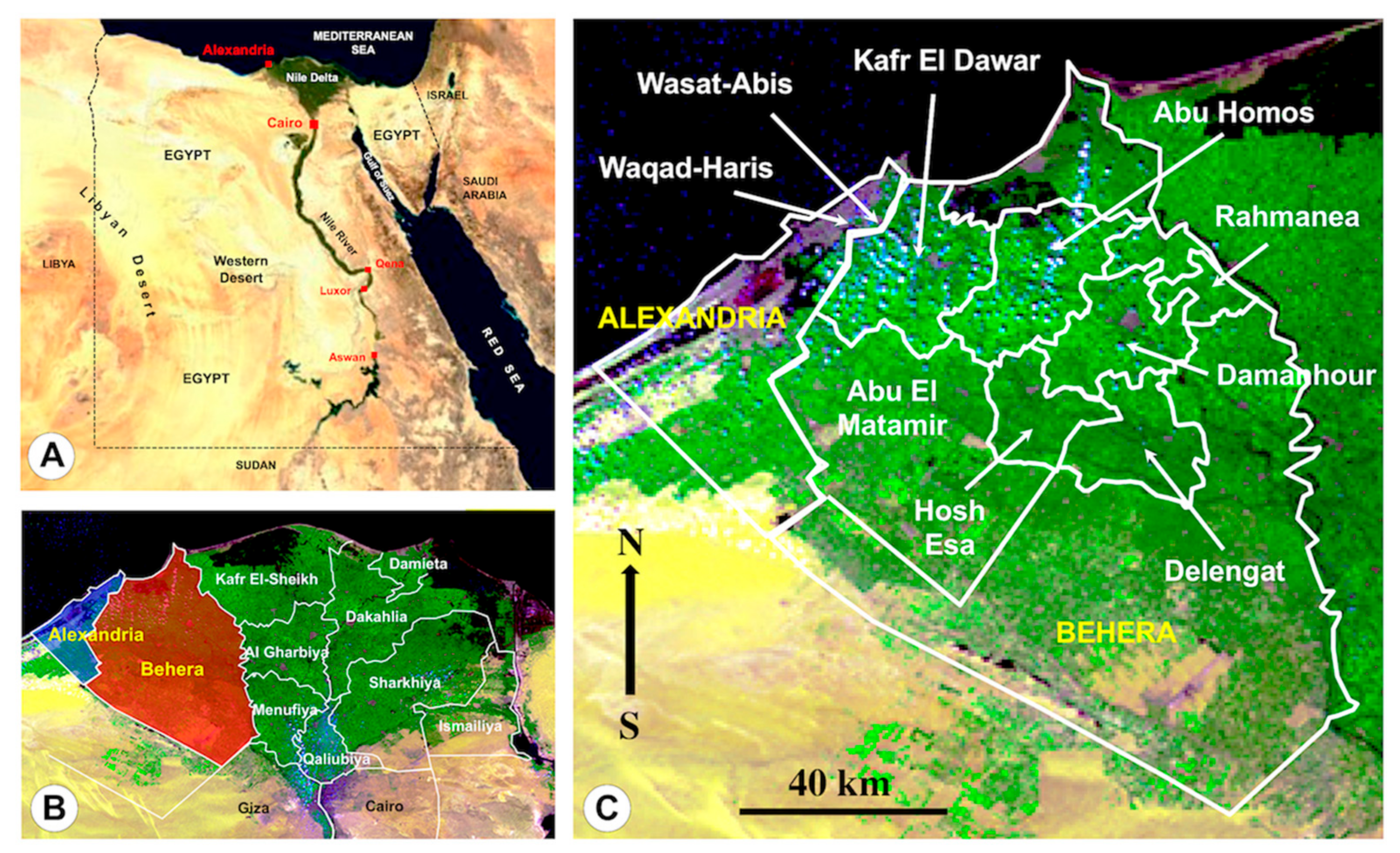
3.2. Relationship with Geographical Distribution
- The man-made irrigation systems of the wide plant culture fields frequently using livestock manure for fertilisation;
- The overall distribution of livestock reservoir species among which the absence of the pig and the addition of the buffalo should be mainly highlighted when comparing to Latin America endemic areas.
- The coexistence of small-superficial and large-deeper irrigation canals allowing for the wide distribution of smaller, more amphibious lymnaeid species of the Galba/Fossaria group assuring F. hepatica transmission, and bigger, more aquatic lymnaeid species of the Radix group assuring F. gigantica transmission, respectively, as well as together assuring the viability of intermediate hybrid forms [52].
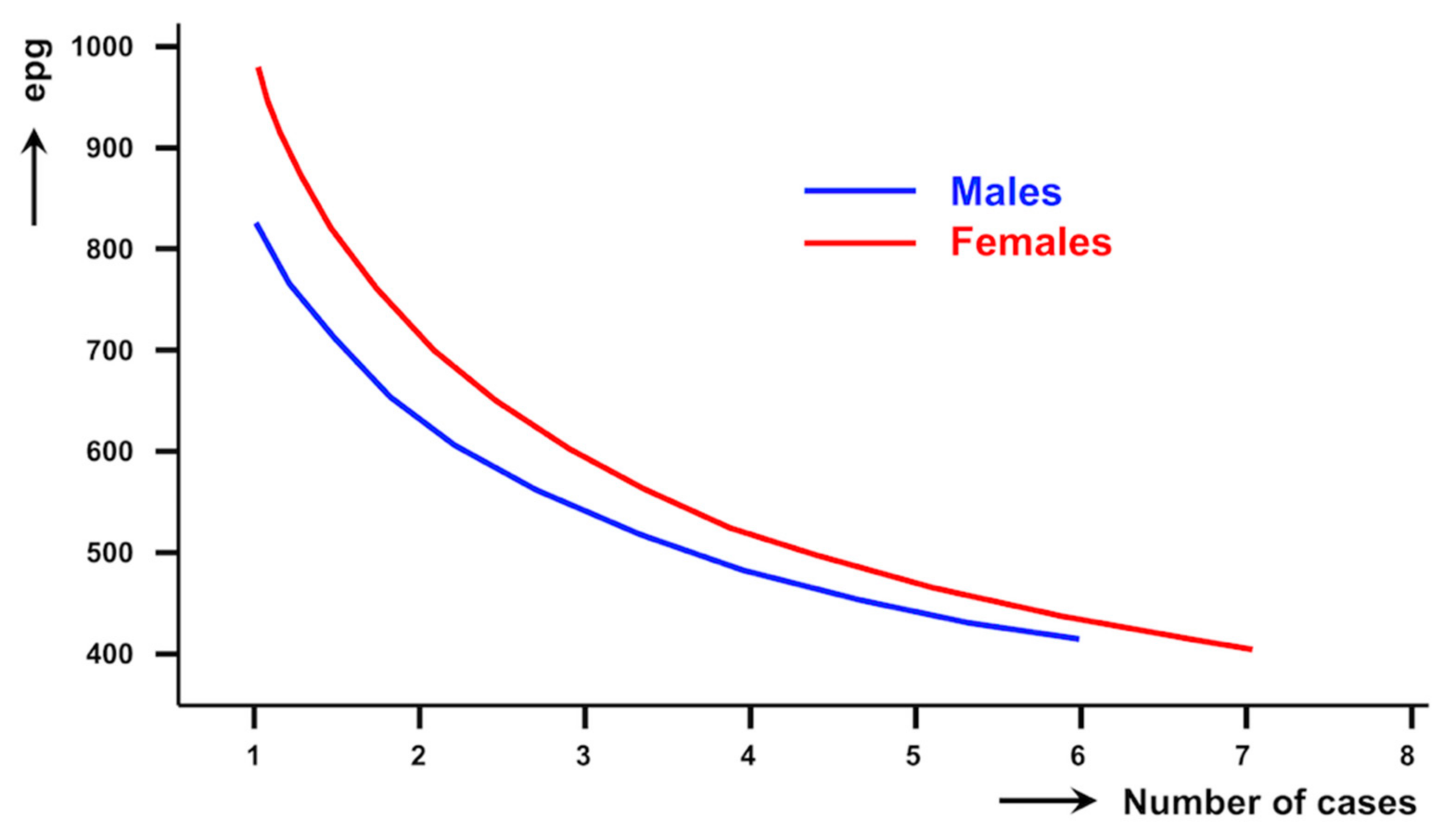
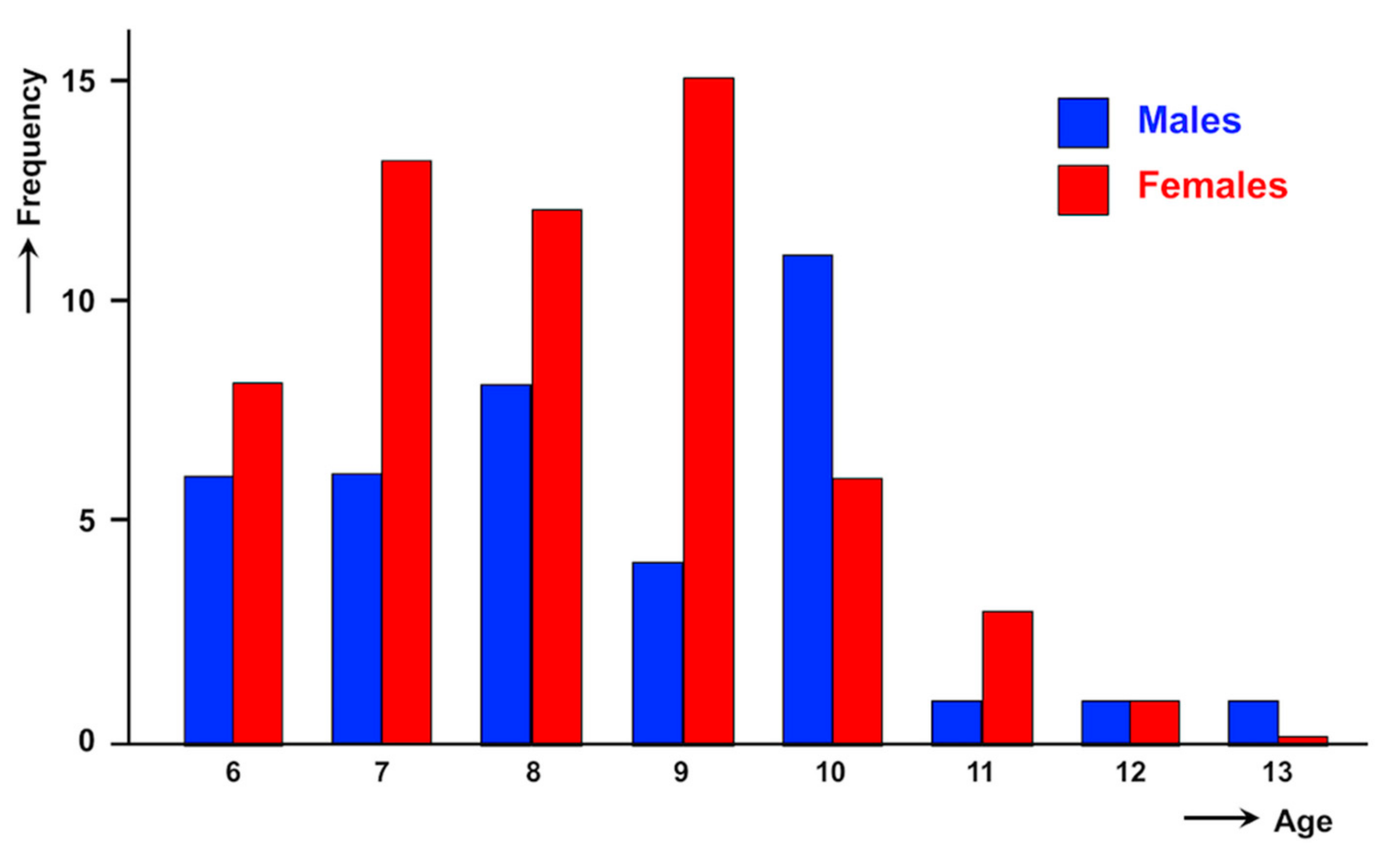
3.3. Relationship with Gender
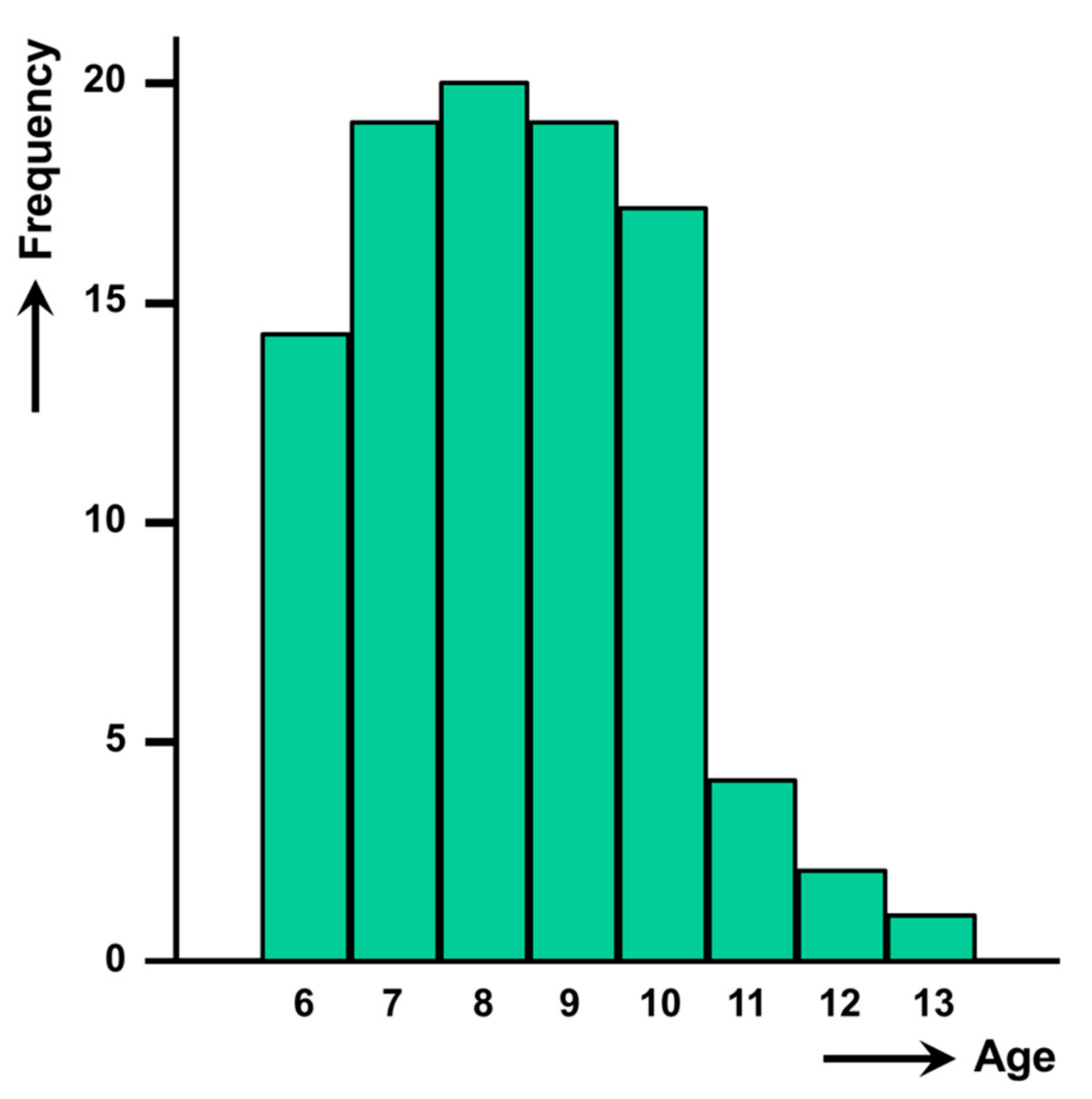
3.4. Relationship with Age
3.5. Observations on Seasonality
3.6. Observations on Schistosomiasis Coinfection
3.7. Repercussions on Health
4. Concluding Remarks
- Liver fluke infection intensities found in the 96 schoolchildren from the governorates of Alexandria and Behera, higher than 400 epg and up to 2304 epg, are the highest intensities hitherto reported not only in Egypt but also in the whole Old World.
- The lower frequency of such high intensity cases in Egypt when compared to those in Bolivia and Peru suggests the difference in the Nile Delta lowlands to be in part related to the high-altitude-enhanced fasciolid transmission observed in the Andean highlands.
- The high intensities here reported in children highlight a problem of very high infection burdens concentrated in infancy, with their consequent higher pathogenicity, morbidity and underdevelopment of individuals and communities.
- In subjects in whom numerous liver fluke eggs are observed in a qualitative diagnostic analysis, exact epg counts should be assessed and preventive measures should be taken in the cases of more than 400 epg, by treating with reduced triclabendazole spaced doses and by additional hospitalisation for post-treatment follow-up enabling quick reaction if potential colic episodes appear.
5. Materials and Methods
5.1. Study Population
- 123 children from Wasat-Abis 8 district: (1) Abdel Aziz Haroun, Abis 8; (2) Suzanne Mubarak, Abis 8;
- 164 children from Waqad-Haris district: (3) Ola Garbea, Ola Gharbea; (4) El Missiry, El Missiry.
- 815 children from Abu El Matamir district: (5) Abu El Matamir, Abu El Bahany; (6) Bahany, Abu El Bahany; (7) Amen Aloba, Abu El Bahany; (8) El Ezba El Hamraa, Abu El Bahany; (9) Abd El Malek El Sayed, Abu El Bahany; (10) Barakat Abd El Malek, Abu El Bahany;
- 836 children from Abu Homos district: (11) Besentway, Besentway; (12) Demesna, Demesna;
- 250 children from Damanhour district: (13) Dorbok, Dorbok;
- 886 children from Delengat district: (14) Yunis Hemeda, Delengat; (15) Azhar Delengat, Delengat; (16) Abu Baki, Delengat; (17) Wagaa Sad, Delengat; (18) Sad Lohaeem, Delengat; (19) El Saieda Fatma, Delengat; (20) Azhar, Tiba; (21) Al Khelalia, Al Khelalia;
- 1284 children from Hosh Esa district: (22) Feraz, Feraz; (23) El Dermerdash, El Kaza; (24) El Roda, El Kaza; (25) Mehress, El Kaza; (26) El Sotomia, El Kaza; (27) El Bostan, Kobry-Abd; (28) Harara, Harara; (29) Azhar Harara, Harara; (30) El Hadad El Bahany, El Hadad; (31) El Hadad El Westany, El Hadad; (32) Abu Malout, El Karnin; (33) El Kardood, El Karnin; (34) Richo, Richo;
- 1882 children from Kafr El Dawar district: (35) Abis 1, Abis 1; (36) Abis 5, Abis 5; (37) El Shahed Saied Sarhan, Kom El Berka; (38) Azhar Bolin, Bolin; (39) Kombaniat Loken, Zuhra; (40) El Malka, Zuhra;
- 417 children from Rahmanea district: (41) Somekrat, Somekrat; (42) Azhar, Menet Salama.
5.2. Stool Collection and Laboratory Methods
5.3. Data Management and Statistical Analysis
5.4. Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mas-Coma, S.; Valero, M.A.; Bargues, M.D. Fasciola, lymnaeids and human fascioliasis, with a global overview on disease transmission, epidemiology, evolutionary genetics, molecular epidemiology and control. Adv. Parasitol. 2009, 69, 41–146. [Google Scholar]
- Bargues, M.D.; Artigas, P.; Mera y Sierra, R.; Pointier, J.P.; Mas-Coma, S. Characterisation of Lymnaea cubensis, L. viatrix and L. neotropica n. sp., the main vectors of Fasciola hepatica in Latin America, by analysis of their ribosomal and mitochondrial DNA. Ann. Trop. Med. Parasitol. 2007, 101, 621–641. [Google Scholar] [CrossRef]
- Bargues, M.D.; Artigas, P.; Khoubbane, M.; Flores, R.; Glöer, P.; Rojas-Garcia, R.; Ashrafi, K.; Falkner, G.; Mas-Coma, S. Lymnaea schirazensis, an overlooked snail distorting fascioliasis data: Genotype, phenotype, ecology, worldwide spread, susceptibility, applicability. PLoS ONE 2011, 6, e24567. [Google Scholar] [CrossRef]
- Mas-Coma, S.; Bargues, M.D.; Valero, M.A. Human fascioliasis infection sources, their diversity, incidence factors, analytical methods and prevention measures. Parasitology 2018, 145, 1665–1699. [Google Scholar] [CrossRef] [Green Version]
- Afshan, K.; Fortes-Lima, C.A.; Artigas, P.; Valero, M.A.; Qayyum, M.; Mas-Coma, S. Impact of climate change and man-made irrigation systems on the transmission risk, long-term trend and seasonality of human and animal fascioliasis in Pakistan. Geospat. Health 2014, 8, 317–334. [Google Scholar] [CrossRef] [PubMed]
- Bargues, M.D.; Artigas, P.; Angles, R.; Osca, D.; Duran, P.; Buchon, P.; Gonzales-Pomar, R.K.; Pinto-Mendieta, J.; Mas-Coma, S. Genetic uniformity, geographical spread and anthropogenic habitat modifications of lymnaeid vectors found in a One Health initiative in the highest human fascioliasis hyperendemic of the Bolivian Altiplano. Parasit. Vectors 2020, 13, 171. [Google Scholar] [CrossRef] [PubMed]
- Mas-Coma, S. Human fascioliasis emergence risks in developed countries: From individual patients and small epidemics to climate and global change impacts. Enferm. Infecc. Microbiol. Clin. 2020, 38, 253–256. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.G.; Mott, K.E. Progress in assessment of morbidity due to Fasciola hepatica infection: A review of recent literature. Trop. Dis. Bull. 1990, 87, R1–R38. [Google Scholar]
- Hillyer, G.V.; Soler de Galanes, M.; Rodriguez-Perez, J.; Bjorland, J.; Silva de Lagrava, M.; Ramirez Guzman, S.; Bryan, R.T. Use of the Falcon Assay Screening Test—Enzyme-Linked Immunosorbent Assay (FAST-ELISA) and the Enzyme-Linked Immunoelectrotransfer Blot (EITB) to determine the prevalence of human Fascioliasis in the Bolivian Altiplano. Am. J. Trop. Med. Hyg. 1992, 46, 603–609. [Google Scholar] [CrossRef]
- Esteban, J.G.; Flores, A.; Angles, R.; Mas-Coma, S. High endemicity of human fascioliasis between Lake Titicaca and La Paz valley, Bolivia. Trans. R. Soc. Trop. Med. Hyg. 1999, 93, 151–156. [Google Scholar] [CrossRef]
- Esteban, J.G.; Gonzalez, C.; Bargues, M.D.; Angles, R.; Sanchez, C.; Naquira, C.; Mas-Coma, S. High fascioliasis infection in children linked to a man-made irrigation zone in Peru. Trop. Med. Int. Health 2002, 7, 339–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez, L.C.; Esteban, J.G.; Bargues, M.D.; Valero, M.A.; Ortiz, P.; Naquira, C.; Mas-Coma, S. Hyperendemic human fascioliasis in Andean valleys: An altitudinal transect analysis in children of Cajamarca province, Peru. Acta Trop. 2011, 120, 119–129. [Google Scholar] [CrossRef]
- Esteban, J.G.; Gonzalez, C.; Curtale, F.; Muñoz-Antoli, C.; Valero, M.A.; Bargues, M.D.; El Sayed, M.; El Wakeel, A.; Abdel-Wahab, Y.; Montresor, A.; et al. Hyperendemic fascioliasis associated with schistosomiasis in villages in the Nile Delta of Egypt. Am. J. Trop. Med. Hyg. 2003, 69, 429–437. [Google Scholar] [CrossRef]
- Mera y Sierra, R.; Agramunt, V.H.; Cuervo, P.; Mas-Coma, S. Human fascioliasis in Argentina: Retrospective overview, critical analysis and baseline for future research. Parasit. Vectors 2011, 4, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mas-Coma, S.; Agramunt, V.H.; Valero, M.A. Neurological and ocular fascioliasis in humans. Adv. Parasitol. 2014, 84, 27–149. [Google Scholar]
- Gonzalez-Miguel, J.; Valero, M.A.; Reguera-Gomez, M.; Mas-Bargues, C.; Bargues, M.D.; Simon-Martin, F.; Mas-Coma, S. Numerous Fasciola plasminogen-binding proteins may underlie blood-brain barrier leakage and explain neurological disorder complexity and heterogeneity in the acute and chronic phases of human fascioliasis. Parasitology 2019, 146, 284–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rondelaud, D.; Dreyfuss, G.; Vignoles, P. Clinical and biological abnormalities in patients after fasciolosis treatment. Med. Mal. Infect. 2006, 36, 466–468. [Google Scholar] [CrossRef]
- Dalton, J.P.; Robinson, M.W.; Mulcahy, G.; O’Neill, S.M.; Donnelly, S. Immunomodulatory molecules of Fasciola hepatica: Candidates for both vaccine and immunotherapeutic development. Vet. Parasitol. 2013, 195, 272–285. [Google Scholar] [CrossRef]
- Aldridge, A.; O’Neill, S.M. Fasciola hepatica tegumental antigens induce anergic like T cells via dendritic cells in a mannose receptor dependent manner. Eur. J. Immunol. 2016, 46, 1180–1192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valero, M.A.; Perez-Crespo, I.; Chillon-Marinas, C.; Khoubbane, M.; Quesada, C.; Reguera-Gomez, M.; Mas-Coma, S.; Fresno, M.; Girones, N. Fasciola hepatica reinfection potentiates a mixed Th1/Th2/Th17/Treg response and correlates with the clinical phenotypes of anemia. PLoS ONE 2017, 12, e0173456. [Google Scholar]
- Girones, N.; Valero, M.A.; Garcia-Bodelon, M.A.; Chico-Calero, M.I.; Punzon, C.; Fresno, M.; Mas-Coma, S. Immune suppression in advanced chronic fascioliasis: An experimental study in a rat model. J. Infect. Dis. 2007, 195, 1504–1512. [Google Scholar] [CrossRef]
- Valero, M.A.; Girones, N.; Reguera-Gomez, M.; Perez-Crespo, I.; Lopez-Garcia, M.P.; Quesada, C.; Bargues, M.D.; Fresno, M.; Mas-Coma, S. Impact of fascioliasis reinfection on Fasciola hepatica egg shedding: Relationship with the immune-regulatory response. Acta Trop. 2020, 209, 105518. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Sustaining the Drive to Overcome the Global Impact of Neglected Tropical Diseases; Department of Control of Neglected Tropical Diseases, World Health Organization: Geneva, Switzerland, 2013; pp. 1–128. [Google Scholar]
- World Health Organization. Ending the Neglect to Attain the Sustainable Development Goals. A Road Map for Neglected Tropical Diseases 2021–2030; World Health Organization: Geneva, Switzerland, 2020; pp. 1–47. Available online: https://www.who.int/neglected_diseases/Ending-the-neglect-to-attain-the-SDGs--NTD-Roadmap.pdf (accessed on 23 July 2020).
- Curtale, F. Treatment of human fascioliasis with triclabendazole: Good news. Trans. R. Soc. Trop. Med. Hyg. 2008, 102, 508. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Report of the WHO Informal Meeting on Use of Triclabendazole in Fascioliasis Control; WHO/CDS/NTD/PCT/2007.1; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Villegas, F.; Angles, R.; Barrientos, R.; Barrios, G.; Valero, M.A.; Hamed, K.; Grueningr, H.; Ault, S.K.; Montresor, A.; Engels, D.; et al. Administration of triclabendazole is safe and effective in controlling fascioliasis in an endemic community of the Bolivian Altiplano. PLoS Negl. Trop. Dis. 2012, 6, e1720. [Google Scholar] [CrossRef] [Green Version]
- Valero, M.A.; Periago, M.V.; Perez-Crespo, I.; Angles, R.; Villegas, F.; Aguirre, C.; Strauss, W.; Espinoza, J.R.; Herrera, P.; Terashima, A.; et al. Field evaluation of a coproantigen detection test for fascioliasis diagnosis and surveillance in human hyperendemic areas of Andean countries. PLoS Negl. Trop. Dis. 2012, 6, e1812. [Google Scholar] [CrossRef]
- Katz, N.; Chaves, A.; Pellegrino, J. A simple device for quantitative stool thick-smear technique in Schistosomiasis mansoni. Rev. Inst. Med. Trop. Sao Pãulo 1972, 14, 397–402. [Google Scholar]
- Ash, L.R.; Orihel, T.C.; Savioli, L. Bench Aids for the Diagnosis of Intestinal Parasites; World Health Organization: Geneva, Switzerland, 1994; pp. 1–23. [Google Scholar]
- Curtale, F.; Nabil, M.; El Wakeel, A.; Shamy, M.Y.; Behera Survey Team. Anaemia and intestinal parasitic infections among school age children in Behera Governorate, Egypt. J. Trop. Ped. 1998, 44, 323–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mas-Coma, S.; Funatsu, I.R.; Angles, R.; Buchon, P.; Mas-Bargues, C.; Artigas, P.; Valero, M.A.; Bargues, M.D. Domestic pig prioritized in one health action against fascioliasis in human endemic areas: Experimental assessment of transmission capacity and epidemiological evaluation of reservoir role. One Health 2021, 13, 100249. [Google Scholar] [CrossRef]
- Bargues, M.D.; Angles, R.; Coello, J.; Artigas, P.; Funatsu, I.R.; Cuervo, P.F.; Buchon, P.; Mas-Coma, S. One Health initiative in the Bolivian Altiplano human fascioliasis hyperendemic area: Lymnaeid biology, population dynamics, microecology and climatic factor influences. Braz. J. Vet. Parasitol. 2021, 30, e025620. [Google Scholar] [CrossRef] [PubMed]
- Montresor, A.; Crompton, D.W.T.; Bundy, D.A.P.; Hall, A.; Savioli, L. Guidelines for the Evaluation of Soil-Transmitted Helminthiasis and Schistosomiasis at Community Level. A Guide for Managers of Control Programmes; WHO/CTD/SIP/98.1; Schistosomiasis and Intestinal Parasites Unit, Division of Control of Tropical Diseases, World Health Organization: Geneva, Switzerland, 1998; pp. 1–45. [Google Scholar]
- Mas-Coma, S.; Angles, R.; Esteban, J.G.; Bargues, M.D.; Buchon, P.; Franken, M.; Strauss, W. The Northern Bolivian Altiplano: A region highly endemic for human fascioliasis. Trop. Med. Int. Health 1999, 4, 454–467. [Google Scholar] [CrossRef]
- O’Neill, S.M.; Parkinson, M.; Strauss, W.; Angles, R.; Dalton, J.P. Immunodiagnosis of Fasciola hepatica (fascioliasis) in a human population in the Bolivian Altiplano using purified cathepsin L cysteine proteinase. Am. J. Trop. Med. Hyg. 1998, 58, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Mas-Coma, S.; Funatsu, I.R.; Bargues, M.D. Fasciola hepatica and lymnaeid snails occurring at very high altitude in South America. Parasitology 2001, 123, S115–S127. [Google Scholar] [CrossRef]
- Valero, M.A.; Perez-Crespo, I.; Khoubbane, M.; Artigas, P.; Panova, M.; Ortiz, P.; Maco, V.; Espinoza, J.R.; Mas-Coma, S. Fasciola hepatica phenotypic characterisation in Andean human endemic areas: Valley versus altiplanic patterns analysed in liver flukes from sheep from Cajamarca and Mantaro, Peru. Infect. Genet. Evol. 2012, 12, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Curtale, F.; Hammoud, E.S.; El Wakeel, A.; Mas-Coma, S.; Savioli, L. Human fascioliasis, an emerging public health problem in the Nile Delta, Egypt. Res. Rev. Parasitol. 2000, 60, 129–134. [Google Scholar]
- Haseeb, A.N.; El Shazly, A.M.; Arafa, M.A.S.; Morsy, A.T.A. A review on fascioliasis in Egypt. J. Egypt. Soc. Parasitol 2002, 32, 317–354. [Google Scholar]
- World Health Organization. Control of Foodborne Trematode Infections; WHO Technical Report Series; World Health Organization: Geneva, Switzerland, 1995; Volume 849, pp. 1–157. [Google Scholar]
- El Shazly, A.M.; El-Nahas, H.A.; Abdel-Mageed, A.A.; El Beshbishi, S.N.; Azab, M.S.; Abou El Hasan, M.; Arafa, W.A.S.; Morsy, T.A. Human fascioliasis and anaemia in Dakhalia governorate, Egypt. J. Egypt. Soc. Parasitol. 2005, 35, 421–432. [Google Scholar] [PubMed]
- Curtale, F.; Hassanein, Y.A.E.; Savioli, L. Control of human fascioliasis by selective chemotherapy: Design, cost and effect of the first public health, school-based intervention implemented in endemic areas of the Nile Delta, Egypt. Trans. R. Soc. Trop. Med. Hyg. 2005, 99, 599–609. [Google Scholar] [CrossRef]
- Curtale, F.; Hassanein, Y.A.; Barduagni, P.; Yousef, M.M.; Wakeel, A.E.; Hallaj, Z.; Mas-Coma, S. Human fascioliasis infection: Gender differences within school-age children from endemic areas of the Nile Delta, Egypt. Trans. R. Soc. Trop. Med. Hyg. 2007, 101, 155–160. [Google Scholar] [CrossRef]
- Soliman, M.S. Control of veterinary fascioliasis. In Infectious Diseases and Public Health. A Research and Clinical Update; Angelico, M., Rocchi, G.G., Eds.; Balaban Publishers: Philadelphia, PA, USA; L’Aquila, Italy, 1998; pp. 334–346. [Google Scholar]
- Valero, M.A.; Panova, M.; Comes, A.M.; Fons, R.; Mas-Coma, S. Patterns in size and shedding of Fasciola hepatica eggs by naturally and experimentally infected murid rodents. J. Parasitol. 2002, 88, 308–313. [Google Scholar] [CrossRef]
- Esteban, J.G.; Flores, A.; Aguirre, C.; Strauss, W.; Angles, R.; Mas-Coma, S. Presence of very high prevalence and intensity of infection with Fasciola hepatica among Aymara children from the Northern Bolivian Altiplano. Acta Trop. 1997, 66, 1–14. [Google Scholar] [CrossRef]
- El Bahy, M.M. Fascioliasis among animal, snail and human hosts in Kafr El-Sheikh Governorate with special reference to species infecting humans. Vet. Med. J. Giza 1997, 45, 187–209. [Google Scholar]
- Massoud, A.M.A.; El-Kholy, N.M.B.; El-Shennawy, F.A.; Farag, R.E. Study of some immune aspects in patients with fascioliasis before and after Chommiphora molmol (Mirazid) treatment. J. Egypt. Soc. Parasitol. 2004, 34, 315–332. [Google Scholar]
- El Shazly, A.M.; Soliman, M.; Gabr, A.; Haseeb, A.N.; Morsy, A.T.A.; Arafa, M.A.S.; Morsy, T.A. Clinico-epidemiological study of human fascioliasis in an endemic focus in Dakahlia governorate, Egypt. J. Egypt. Soc. Parasitol. 2001, 31, 725–736. [Google Scholar]
- Esteban, J.G.; Flores, A.; Angles, R.; Strauss, W.; Aguirre, C.; Mas-Coma, S. A population-based coprological study of human fascioliasis in a hyperendemic area of the Bolivian Altiplano. Trop. Med. Int. Health 1997, 2, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Periago, M.V.; Valero, M.A.; El Sayed, M.; Ashrafi, K.; El Wakeel, A.; Mohamed, M.Y.; Desquesnes, M.; Curtale, F.; Mas-Coma, S. First phenotypic description of Fasciola hepatica/Fasciola gigantica intermediate forms from the human endemic area of the Nile Delta, Egypt. Infect. Genet. Evol. 2008, 8, 51–58. [Google Scholar] [CrossRef]
- Curtale, F.; Mas-Coma, S.; Hassanein, Y.A.E.W.; Barduagni, P.; Pezzotti, P.; Savioli, L. Clinical signs and household characteristics associated with human fascioliasis among rural population in Egypt: A case-control study. Parassitologia 2003, 45, 5–11. [Google Scholar] [PubMed]
- Bargues, M.D.; Artigas, P.; Khoubbane, M.; Ortiz, P.; Naquira, C.; Mas-Coma, S. Molecular characterisation of Galba truncatula, Lymnaea neotropica and L. schirazensis from Cajamarca, Peru and their potential role in transmission of human and animal fascioliasis. Parasit. Vectors 2012, 5, 174. [Google Scholar] [CrossRef] [Green Version]
- Bardales-Valdivia, J.N.; Bargues, M.D.; Hoban-Vergara, C.; Bardales-Bardales, C.; Goicoechea-Portal, C.; Bazan-Zurita, H.; Del Valle-Mendoza, J.; Ortiz, P.; Mas-Coma, S. Spread of the fascioliasis endemic area assessed by seasonal follow-up of rRNA ITS-2 sequenced lymnaeid populations in Cajamarca, Peru. One Health 2021, 13, 100265. [Google Scholar] [CrossRef]
- Curtale, F.; Hassanein, Y.A.E.; El Wakeel, A.; Mas-Coma, S.; Montresor, A. Distribution of human fascioliasis by age and gender among rural population in the Nile Delta, Egypt. J. Trop. Ped. 2003, 49, 264–268. [Google Scholar] [CrossRef] [Green Version]
- De, N.V.; Le, T.H.; Agramunt, V.H.; Mas-Coma, S. Early postnatal and preschool age infection by Fasciola spp.: Report of five cases from Vietnam and worldwide review. Am. J. Trop. Med. Hyg. 2020, 103, 1578–1589. [Google Scholar] [CrossRef]
- Fuentes, M.V.; Malone, J.B.; Mas-Coma, S. Validation of a mapping and predicting model for human fasciolosis transmission in Andean very high altitude endemic areas using remote sensing data. Acta Trop. 2001, 79, 87–95. [Google Scholar] [CrossRef]
- Ollerenshaw, C.B. A comment on the epidemiology of Fasciola hepatica in Italy. Ann. Fac. Med. Vet. 1973, 20, 83–121. [Google Scholar]
- Claxton, J.R.; Sutherst, J.; Ortiz, P.; Clarkson, M.J. The effect of cyclic temperatures on the growth of Fasciola hepatica and Lymnaea viatrix. Vet. J. 1999, 157, 166–171. [Google Scholar] [CrossRef]
- Farag, H.F.; Salem, A.; Khalil, S.S.; Farahat, A. Studies on human fascioliasis in Egypt. 1—Seasonality of transmission. J. Egypt. Soc. Parasitol. 1993, 23, 331–340. [Google Scholar]
- Valero, M.A.; Navarro, M.; Garcia-Bodelon, M.A.; Marcilla, A.; Morales, M.; Garcia, J.E.; Hernandez, J.L.; Mas-Coma, S. High risk of bacterobilia in advanced experimental chronic fasciolosis. Acta Trop. 2006, 100, 17–23. [Google Scholar] [CrossRef]
- Valero, M.A.; Girones, N.; Garcia-Bodelon, M.A.; Periago, M.V.; Chico-Calero, I.; Khoubbane, M.; Fresno, M.; Mas-Coma, S. Anaemia in advanced chronic fasciolosis. Acta Trop. 2008, 108, 35–43. [Google Scholar] [CrossRef]
- Valero, M.A.; Bargues, M.D.; Khoubbane, M.; Artigas, P.; Quesada, C.; Berinde, L.; Ubeira, F.M.; Mezo, M.; Hernandez, J.L.; Agramunt, V.H.; et al. Higher physiopathogenicity by Fasciola gigantica than by the genetically close F. hepatica: Experimental long-term follow-up of biochemical markers. Trans. R. Soc. Trop. Med. Hyg. 2016, 110, 55–66. [Google Scholar] [CrossRef]
- Mas-Coma, S.; Bargues, M.D.; Valero, M.A. Diagnosis of human fascioliasis by stool and blood techniques: Update for the present global scenario. Parasitology 2014, 141, 1918–1946. [Google Scholar] [CrossRef] [PubMed]
- Zumaquero-Rios, J.L.; Sarracent-Perez, J.; Rojas-Garcia, R.; Rojas-Rivero, L.; Martinez-Tovilla, Y.; Valero, M.A.; Mas-Coma, S. Fascioliasis and intestinal parasitoses affecting schoolchildren in Atlixco, Puebla State, Mexico: Epidemiology and treatment with nitazoxanide. PLoS Negl. Trop. Dis. 2013, 7, e2553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Consultation to Develop a Strategy to Estimate the Global Burden of Foodborne Diseases. Taking Stock and Charting the Way Forward; Department of Food Safety, Zoonoses and Foodborne Diseases, World Health Organization: Geneva, Switzerland, 2006; Available online: http://www.who.int/foodsafety/publications/foodborne_disease/burden_sept06/en (accessed on 21 January 2008).
- Valero, M.A.; Perez-Crespo, I.; Periago, M.V.; Khoubbane, M.; Mas-Coma, S. Fluke egg characteristics for the diagnosis of human and animal fascioliasis by Fasciola hepatica and F. gigantica. Acta Trop. 2009, 111, 150–159. [Google Scholar] [CrossRef] [PubMed]
- Curtale, F.; Hassanein, Y.A.W.; El Wakeel, A.; Barduagni, P.; Savioli, L. The School Health Programme in Behera: An integrated helminth control programme at Governorate level in Egypt. Acta Trop. 2003, 86, 295–307. [Google Scholar] [CrossRef]
- Farag, H.F.; Barakat, R.M.R.; Ragab, M.; Omar, E. A focus of human fascioliasis in the Nile Delta, Egypt. J. Trop. Med. Hyg. 1979, 82, 188–190. [Google Scholar]
- Savioli, L.; Chitsulo, L.; Montresor, A. New opportunities for the control of fascioliasis. Bull. WHO 1999, 77, 300. [Google Scholar] [PubMed]
- Gandhi, P.; Schmitt, E.K.; Chen, C.W.; Samantray, S.; Venishetty, V.K.; Hughes, D. Triclabendazole in the treatment of human fascioliasis: A review. Trans. R. Soc. Trop. Med. Hyg. 2019, 113, 797–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valero, M.A.; Panova, M.; Mas-Coma, S. Phenotypic analysis of adults and eggs of Fasciola hepatica by computer image analysis system. J. Helminthol. 2005, 79, 217–225. [Google Scholar] [CrossRef]
- Stephenson, L.S. Appendix VI: Statistical treatments of egg count data. In The Impact of Helminth Infection on Human Nutrition; Taylor and Francis Ltd.: London, UK, 1997; pp. 224–227. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Districts | No. of Intensity Re-Checked Children | Children with Several Eggs per Slide * | No. Children with epg >400 (%) | epg | |||
|---|---|---|---|---|---|---|---|
| No. | % | Range | Arithm. Mean | Geom. Mean | |||
| Governorate of Alexandria | |||||||
| Wasat-Abis 8 | 123 | 6 | 4.9 | 3 (2.4%) | 408–2040 | 1072.0 | 861.4 |
| Waqad-Haris | 164 | 9 | 5.4 | 3 (1.8%) | 408–432 | 416.0 | 415.9 |
| Governorate of Behera | |||||||
| Abu El Matamir | 815 | 52 | 6.4 | 9 (1.1%) | 408–1008 | 650.7 | 618.2 |
| Abu Homos | 836 | 56 | 6.6 | 10 (1.2%) | 456–1680 | 832.8 | 751.9 |
| Damanhour | 250 | 8 | 0.3 | 1 (0.4%) | 576 | 576.0 | 576.0 |
| Delengat | 886 | 58 | 6.5 | 9 (1.0%) | 408–1752 | 621.3 | 547.8 |
| Hosh Esa | 1284 | 95 | 7.4 | 34 (2.6%) | 408–2304 | 730.6 | 650.5 |
| Kafr El Dawar | 1882 | 64 | 3.4 | 25 (1.3%) | 408–1752 | 659.5 | 612.3 |
| El Rahmannia | 417 | 15 | 3.6 | 2 (0.5%) | 456–552 | 504.0 | 501.7 |
| TOTAL | 6657 | 362 | 5.4 | 96 (1.4%) | 408–2304 | 673.6 | 615.1 |
| epg | Cases No. (%) | Gender | Age (Years) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Males | Females | 6 y | 7 y | 8 y | 9 y | 10 y | 11 y | 12 y | 13 y | ||
| No. (%) | No. (%) | No. (%) | No. (%) | No. (%) | No. (%) | No. (%) | No. (%) | No. (%) | No. (%) | ||
| 408 | 12 (12.5) | 4 (10.5) | 8 (13.8) | 2 (14.3) | 2 (10.5) | 2 (10.0) | 1 (5.3) | 2 (11.8) | 1 (25.0) | 2 (100.0) | –– |
| 432 | 11 (11.5) | 5 (13.2) | 6 (10.3) | –– | 3 (15.8) | –– | 4 (21.1) | 3 (17.6) | 1 (25.0) | –– | –– |
| 456 | 9 (9.4) | 2 (5.3) | 7 (12.1) | –– | 1 (5.3) | 2 (10.0) | 4 (21.1) | 2 (11.8) | –– | –– | –– |
| 480 | 7 (7.3) | 4 (10.5) | 3 (5.2) | –– | 3 (15.8) | 1 (5.0) | 2 (10.5) | 1 (5.9) | –– | –– | –– |
| 504 | 4 (4.2) | 1 (2.6) | 3 (5.2) | 2 (14.3) | 1 (5.3) | –– | 1 (5.3) | –– | –– | –– | –– |
| 528 | 3 (3.1) | 2 (5.3) | 1 (1.7) | 1 (7.14) | –– | 1 (5.0) | –– | 1 (5.9) | –– | –– | –– |
| 552 | 4 (4.2) | 1 (2.6) | 3 (5.2) | –– | 2 (10.5) | 1 (5.0) | –– | 1 (5.9) | –– | –– | –– |
| 576 | 4 (4.2) | 1 (2.6) | 2 (3.4) | –– | 1 (5.3) | –– | 1 (5.3) | 2 (11.8) | –– | –– | –– |
| 600 | 2 (2.1) | 1 (2.6) | 1 (1.7) | –– | –– | 1 (5.0) | –– | 1 (5.9) | –– | –– | –– |
| 624 | 1 (1.0) | 1 (2.6) | 0 (0.0) | –– | –– | 1 (5.0) | –– | –– | –– | –– | –– |
| 648 | 4 (4.2) | 2 (5.3) | 2 (3.4) | 2 (14.3) | –– | 1 (5.0) | 1 (5.3) | –– | –– | –– | –– |
| 672 | 3 (3.1) | 1 (2.6) | 2 (3.4) | –– | 1 (5.3) | 1 (5.0) | –– | 1 (5.9) | –– | –– | –– |
| 696 | 1 (1.0) | 1 (2.6) | 0 (0.0) | –– | –– | –– | –– | –– | 1 (25.0) | –– | –– |
| 720 | 4 (4.2) | 1 (2.6) | 3 (5.2) | 1 (7.14) | 1 (5.3) | 2 (10.0) | –– | –– | –– | –– | –– |
| 744 | 1 (1.0) | 0 (0.0) | 1 (1.7) | –– | –– | –– | 1 (5.3) | –– | –– | –– | –– |
| 768 | 3 (3.1) | 2 (5.3) | 1 (1.7) | 1 (7.14) | –– | –– | –– | –– | 1 (25.0) | –– | 1 (100) |
| 792 | 2 (2.1) | 2 (5.3) | 0 (0.0) | 1 (7.14) | –– | 1 (5.0) | –– | –– | –– | –– | –– |
| 816 | 1 (1.0) | 0 (0.0) | 1 (1.7) | –– | 1 (5.3) | –– | –– | –– | –– | –– | –– |
| 864 | 1 (1.0) | 0 (0.0) | 1 (1.7) | 1 (7.14) | –– | –– | –– | –– | –– | –– | –– |
| 888 | 1 (1.0) | 0 (0.0) | 1 (1.7) | –– | 1 (5.3) | –– | –– | –– | –– | –– | –– |
| 936 | 2 (2.1) | 2 (5.3) | 0 (0.0) | –– | 1 (5.3) | 1 (5.0) | –– | –– | –– | –– | –– |
| 984 | 1 (1.0) | 0 (0.0) | 1 (1.7) | –– | –– | –– | –– | 1 (5.9) | –– | –– | –– |
| 1008 | 1 (1.0) | 0 (0.0) | 1 (1.7) | –– | 1 (5.3) | –– | –– | –– | –– | –– | –– |
| 1056 | 1 (1.0) | 0 (0.0) | 1 (1.7) | 1 (7.14) | –– | –– | –– | –– | –– | –– | –– |
| 1080 | 1 (1.0) | 0 (0.0) | 1 (1.7) | –– | –– | –– | 1 (5.3) | –– | –– | –– | –– |
| 1152 | 1 (1.0) | 0 (0.0) | 1 (1.7) | –– | –– | 1 (5.0) | –– | –– | –– | –– | –– |
| 1224 | 1 (1.0) | 0 (0.0) | 1 (1.7) | 1 (7.14) | –– | –– | –– | –– | –– | –– | –– |
| 1296 | 2 (2.1) | 0 (0.0) | 2 (3.4) | –– | –– | 1 (5.0) | –– | 1 (5.9) | –– | –– | –– |
| 1320 | 1 (1.0) | 1 (2.6) | 0 (0.0) | 1 (7.14) | –– | –– | –– | –– | –– | –– | –– |
| 1344 | 1 (1.0) | 0 (0.0) | 1 (1.7) | –– | –– | 1 (5.0) | –– | –– | –– | –– | –– |
| 1560 | 1 (1.0) | 1 (2.6) | –– | 1 (5.0) | –– | –– | –– | –– | –– | ||
| 1680 | 1 (1.0) | 0 (0.0) | 1 (1.7) | –– | –– | –– | 1 (5.3) | –– | –– | –– | –– |
| 1752 | 2 (2.1) | 1 (2.6) | 1 (1.7) | –– | –– | –– | 1 (5.3) | 1 (5.9) | –– | –– | –– |
| 2040 | 1 (1.0) | 1 (2.6) | 0 (0.0) | –– | –– | 1 (5.0) | –– | –– | –– | –– | –– |
| 2304 | 1 (1.0) | 0 (0.0) | 1 (1.7) | –– | –– | –– | 1 (5.3) | –– | –– | –– | –– |
| Total | 96 (100) | 38 (39.6) | 58 (60.4) | 14 (14.6) | 19 (19.8) | 20 (20.8) | 19 (19.8) | 17 (17.7) | 4 (4.2) | 2 (2.1) | 1 (1.0) |
| Epg Counts | Children | Males | Females | ||||
|---|---|---|---|---|---|---|---|
| Groups | No. | % | Mean | No. | % | No. | % |
| 400–699 | 65 | 67.7 | 8.5 | 27 | 41.5 | 38 | 58.5 |
| 700–999 | 16 | 16.7 | 7.9 | 7 | 43.8 | 9 | 56.3 |
| 1000–1299 | 7 | 7.3 | 7.7 | 0 | 0 | 7 | 100.0 |
| 1300–1599 | 4 | 4.2 | 7.8 | 2 | 50.0 | 2 | 50.0 |
| 1600–1899 | 2 | 2.1 | 9.5 | 1 | 50.0 | 1 | 50.0 |
| ≥1900 | 2 | 2.1 | 8.5 | 1 | 50.0 | 1 | 50.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Periago, M.V.; Valero, M.A.; Artigas, P.; Agramunt, V.H.; Bargues, M.D.; Curtale, F.; Mas-Coma, S. Very High Fascioliasis Intensities in Schoolchildren from Nile Delta Governorates, Egypt: The Old World Highest Burdens Found in Lowlands. Pathogens 2021, 10, 1210. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10091210
Periago MV, Valero MA, Artigas P, Agramunt VH, Bargues MD, Curtale F, Mas-Coma S. Very High Fascioliasis Intensities in Schoolchildren from Nile Delta Governorates, Egypt: The Old World Highest Burdens Found in Lowlands. Pathogens. 2021; 10(9):1210. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10091210
Chicago/Turabian StylePeriago, M. Victoria, M. Adela Valero, Patricio Artigas, Verónica H. Agramunt, M. Dolores Bargues, Filippo Curtale, and Santiago Mas-Coma. 2021. "Very High Fascioliasis Intensities in Schoolchildren from Nile Delta Governorates, Egypt: The Old World Highest Burdens Found in Lowlands" Pathogens 10, no. 9: 1210. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens10091210