
What Is the Impact of Early and Subsequent Epidemic Characteristics on the Pre-delta COVID-19 Epidemic Size in the United States?

 ,
,
Abstract
:1. Introduction
2. Results
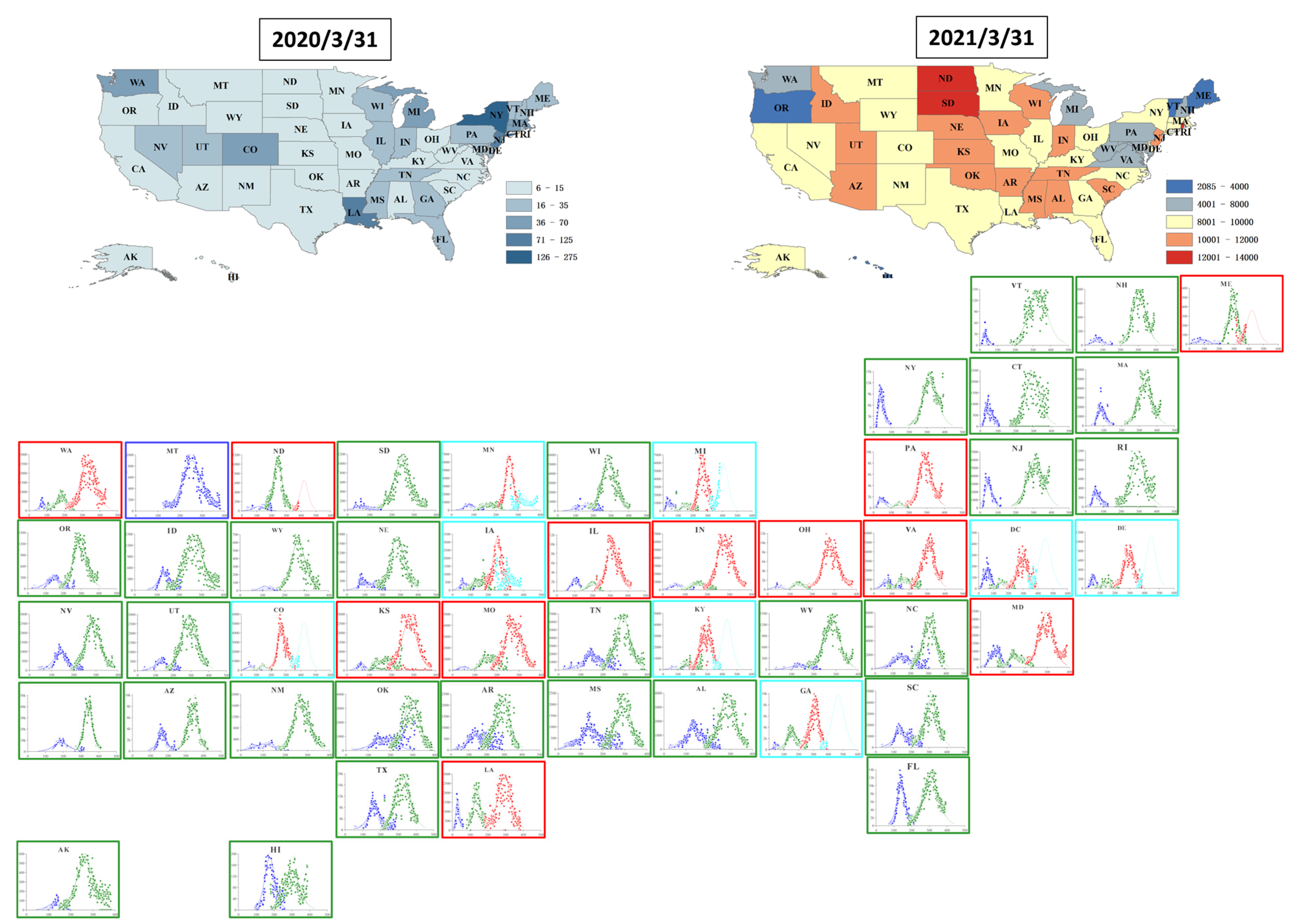
2.1. Spatiotemporal Changes of COVID-19 Pandemic in the United States
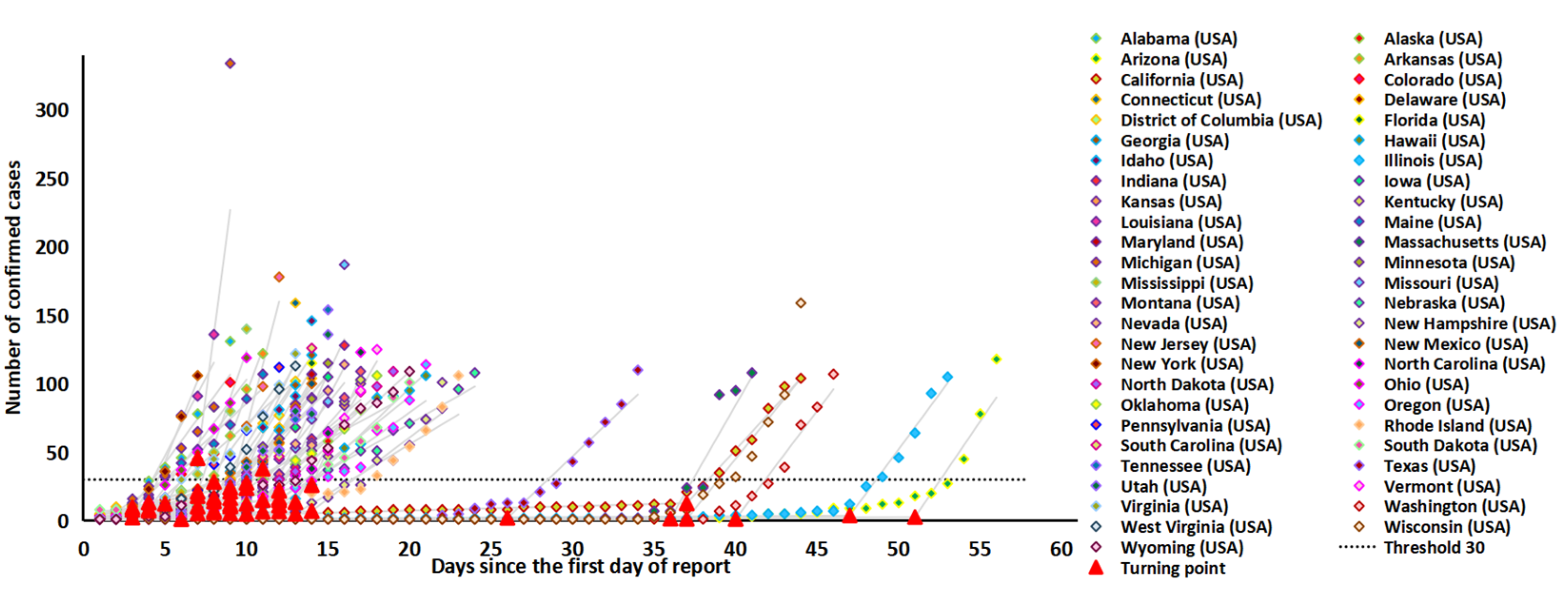
2.2. Early Epidemic Characteristics of the COVID-19 Epidemic in the US
2.3. Subsequent Epidemic Characteristics Based on Multi-Logistic Fitting
2.4. Epidemic Size and Associated Characteristics
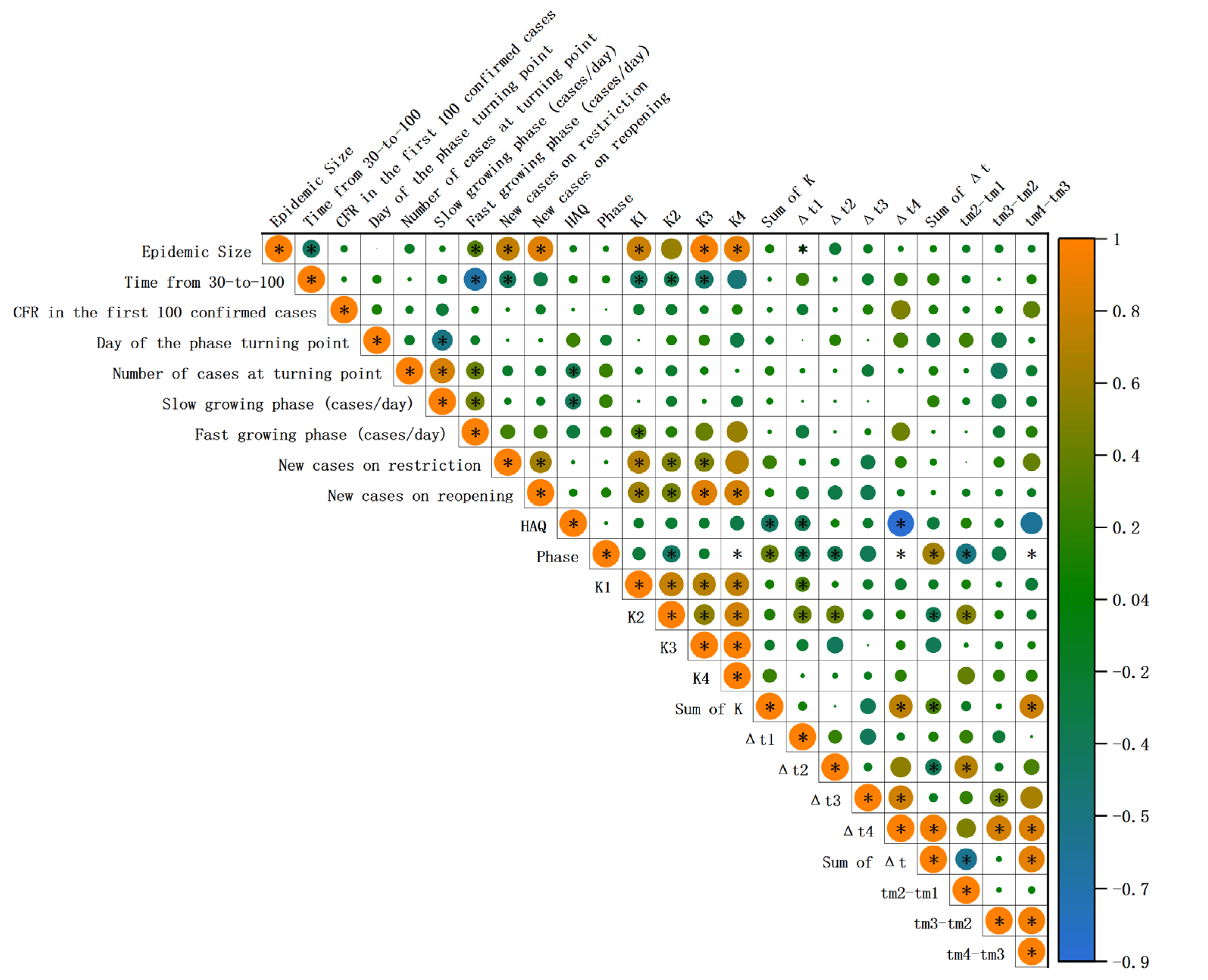
2.5. Correlation between Early and Subsequent Epidemic Characteristics
3. Discussion
4. Materials and Methods
4.1. Data Source
4.2. Selection of Epidemic Characteristics Indicators
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef] [PubMed]
- To, K.K.; Sridhar, S.; Chiu, K.H.; Hung, D.L.; Li, X.; Hung, I.F.; Tam, A.R.; Chung, T.W.; Chan, J.F.; Zhang, A.J.; et al. Lessons learned 1 year after SARS-CoV-2 emergence leading to COVID-19 pandemic. Emerg. Microbes Infect. 2021, 10, 507–535. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus Resource Center of Johns Hopkins University & Medicine. Available online: https://0-coronavirus-jhu-edu.brum.beds.ac.uk/ (accessed on 31 March 2021).
- Coronavirus in the U.S.: Latest Map and Case Count. Available online: https://www.nytimes.com/interactive/2021/us/covid-cases.html (accessed on 5 April 2021).
- Holshue, M.L.; DeBolt, C.; Lindquist, S.; Lofy, K.H.; Wiesman, J.; Bruce, H.; Spitters, C.; Ericson, K.; Wilkerson, S.; Tural, A.; et al. First Case of 2019 Novel Coronavirus in the United States. N. Engl. J. Med. 2020, 382, 929–936. [Google Scholar] [CrossRef] [PubMed]
- US Coronavirus Vaccine Tracker. Available online: https://usafacts.org/visualizations/covid-vaccine-tracker-states/ (accessed on 16 May 2021).
- Viral Variant Proportions in the United States. Available online: https://covid.cdc.gov/covid-data-tracker/#variant-proportions (accessed on 8 May 2021).
- What Doctors Wish Patients Knew about the Dangerous Delta Variant. Available online: https://www.ama-assn.org/delivering-care/public-health/what-doctors-wish-patients-knew-about-dangerous-delta-variant (accessed on 30 May 2021).
- Friston, K.J.; Parr, T.; Zeidman, P.; Razi, A.; Flandin, G.; Daunizeau, J.; Hulme, O.J.; Billig, A.J.; Litvak, V.; Price, C.J.; et al. Second waves, social distancing, and the spread of COVID-19 across the USA. Wellcome Open Res. 2020, 5, 103. [Google Scholar] [CrossRef]
- Jalali, A.M.; Peterson, B.M.; Galbadage, T. Early COVID-19 Interventions Failed to Replicate 1918 St. Louis vs. Philadelphia Outcomes in the United States. Front. Public Health 2020, 8, 579559. [Google Scholar] [CrossRef]
- Kaxiras, E.; Neofotistos, G. Multiple Epidemic Wave Model of the COVID-19 Pandemic: Modeling Study. J. Med. Internet Res. 2020, 22, e20912. [Google Scholar] [CrossRef]
- Hazem, Y.; Natarajan, S.; Berikaa, E.R. Hasty Reduction of COVID-19 Lockdown Measures Leads to the Second Wave of Infection. medRxiv, 2020; preprint. [Google Scholar] [CrossRef]
- Ridenhour, B.; Kowalik, J.M.; Shay, D.K. Unraveling R0: Considerations for public health applications. Am. J. Public Health 2014, 104, e32–e41. [Google Scholar] [CrossRef]
- Holme, P.; Masuda, N. The Basic Reproduction Number as a Predictor for Epidemic Outbreaks in Temporal Networks. PLoS ONE 2015, 10, e0120567. [Google Scholar] [CrossRef]
- Zhang, L.; Tao, Y.; Wang, J.; Ong, J.J.; Tang, W.; Zou, M.; Bai, L.; Ding, M.; Shen, M.; Zhuang, G.; et al. Early characteristics of the COVID-19 outbreak predict the subsequent epidemic scope. Int. J. Infect. Dis. 2020, 97, 219–224. [Google Scholar] [CrossRef]
- Saqib, M. Forecasting COVID-19 outbreak progression using hybrid polynomial-Bayesian ridge regression model. Appl. Intell. 2021, 51, 2703–2713. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Zheng, X.; Li, J.; Zhu, B. Prediction of epidemic trends in COVID-19 with logistic model and machine learning technics. Chaos Solitons Fractals 2020, 139, 110058. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.D.; Dwivedi, R.; Sharma, D.K. Prediction of Covid-19 trends in Europe using generalized regression neural network optimized by flower pollination algorithm. J. Interdiscip. Math. 2020, 24, 33–51. [Google Scholar] [CrossRef]
- Singh, R.K.; Rani, M.; Bhagavathula, A.S.; Sah, R.; Rodriguez-Morales, A.J.; Kalita, H.; Nanda, C.; Sharma, S.; Sharma, Y.D.; Rabaan, A.A.; et al. Prediction of the COVID-19 Pandemic for the Top 15 Affected Countries: Advanced Autoregressive Integrated Moving Average (ARIMA) Model. JMIR Public Health Surveill. 2020, 6, e19115. [Google Scholar] [CrossRef]
- Bai, L.; Lu, H.; Hu, H.; Smith, M.K.; Harripersaud, K.; Lipkova, V.; Wen, Y.; Guo, X.; Peng, W.; Liu, C.; et al. Evaluation of work resumption strategies after COVID-19 reopening in the Chinese city of Shenzhen: A mathematical modeling study. Public Health 2021, 193, 17–22. [Google Scholar] [CrossRef]
- Shen, M.; Peng, Z.; Guo, Y.; Rong, L.; Li, Y.; Xiao, Y.; Zhuang, G.; Zhang, L. Assessing the effects of metropolitan-wide quarantine on the spread of COVID-19 in public space and households. Int. J. Infect. Dis. 2020, 96, 503–505. [Google Scholar] [CrossRef]
- Shen, M.; Xiao, Y.; Zhuang, G.; Li, Y.; Zhang, L. Mass testing-An underexplored strategy for COVID-19 control. Innovation 2021, 2, 100114. [Google Scholar] [CrossRef]
- Shen, M.; Zu, J.; Fairley, C.K.; Pagan, J.A.; An, L.; Du, Z.; Guo, Y.; Rong, L.; Xiao, Y.; Zhuang, G.; et al. Projected COVID-19 epidemic in the United States in the context of the effectiveness of a potential vaccine and implications for social distancing and face mask use. Vaccine 2021, 39, 2295–2302. [Google Scholar] [CrossRef]
- Shen, M.; Zu, J.; Fairley, C.K.; Pagán, J.A.; Ferket, B.; Liu, B.; Yi, S.S.; Chambers, E.; Li, G.; Guo, Y.; et al. Effects of New York’s Executive Order on Face Mask Use on COVID-19 Infections and Mortality: A Modeling Study. J. Urban Health 2021, 98, 197–204. [Google Scholar] [CrossRef]
- Zhang, L.; Shen, M.; Ma, X.; Su, S.; Gong, W.; Wang, J.; Tao, Y.; Zou, Z.; Zhao, R.; Lau, J.T.F.; et al. What Is Required to Prevent a Second Major Outbreak of SARS-CoV-2 upon Lifting Quarantine in Wuhan City, China. Innovation 2020, 1, 100006. [Google Scholar] [CrossRef]
- Zhang, L.; Tao, Y.; Shen, M.; Fairley, C.K.; Guo, Y. Can self-imposed prevention measures mitigate the COVID-19 epidemic? PLoS Med. 2020, 17, e1003240. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Liu, Y.; Struthers, J.; Lian, M. Spatiotemporal Characteristics of the COVID-19 Epidemic in the United States. Clin. Infect. Dis. 2021, 72, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Courtemanche, C.; Garuccio, J.; Le, A.; Pinkston, J.; Yelowitz, A. Strong Social Distancing Measures In The United States Reduced The COVID-19 Growth Rate. Health Aff. 2020, 39, 1237–1246. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, N.D.; Suder, J.S. Application of state law in the public health emergency response to COVID-19: An example from Delaware in the United States. J. Public Health Policy 2020, 42, 167–175. [Google Scholar] [CrossRef]
- Gu, T.; Mack, J.A.; Salvatore, M.; Sankar, S.P.; Valley, T.S.; Singh, K.; Nallamothu, B.K.; Kheterpal, S.; Lisabeth, L.; Fritsche, L.G.; et al. COVID-19 outcomes, risk factors and associations by race: A comprehensive analysis using electronic health records data in Michigan Medicine. MedRxiv, 2020; preprint. [Google Scholar] [CrossRef]
- Lyu, W.; Wehby, G.L. Comparison of Estimated Rates of Coronavirus Disease 2019 (COVID-19) in Border Counties in Iowa Without a Stay-at-Home Order and Border Counties in Illinois With a Stay-at-Home Order. JAMA Netw. Open 2020, 3, e2011102. [Google Scholar] [CrossRef]
- Ramírez, I.J.; Lee, J. COVID-19 Emergence and Social and Health Determinants in Colorado: A Rapid Spatial Analysis. Int. J. Environ. Res. Public Health 2020, 17, 3856. [Google Scholar] [CrossRef]
- Smith, T.P.; Flaxman, S.; Gallinat, A.S.; Kinosian, S.P.; Stemkovski, M.; Unwin, H.J.T.; Watson, O.J.; Whittaker, C.; Cattarino, L.; Dorigatti, I.; et al. Temperature and population density influence SARS-CoV-2 transmission in the absence of nonpharmaceutical interventions. Proc. Natl. Acad. Sci. USA 2021, 118, e2019284118. [Google Scholar] [CrossRef]
- Zhang, C.H.; Schwartz, G.G. Spatial Disparities in Coronavirus Incidence and Mortality in the United States: An Ecological Analysis as of May 2020. J. Rural. Health 2020, 36, 433–445. [Google Scholar] [CrossRef]
- Patel, U.; Malik, P.; Mehta, D.; Shah, D.; Kelkar, R.; Pinto, C.; Suprun, M.; Dhamoon, M.; Hennig, N.; Sacks, H. Early epidemiological indicators, outcomes, and interventions of COVID-19 pandemic: A systematic review. J. Glob. Health 2020, 10, 020506. [Google Scholar] [CrossRef]
- Reicher, S.; Drury, J. Pandemic fatigue? How adherence to covid-19 regulations has been misrepresented and why it matters. BMJ 2021, 372, n137. [Google Scholar] [CrossRef] [PubMed]
- Lau, H.; Khosrawipour, T.; Kocbach, P.; Ichii, H.; Bania, J.; Khosrawipour, V. Evaluating the massive underreporting and undertesting of COVID-19 cases in multiple global epicenters. Pulmonology 2021, 27, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Pei, S.; Shaman, J.; Dubrow, R.; Chen, K. Role of meteorological factors in the transmission of SARS-CoV-2 in the United States. Nat. Commun. 2021, 12, 3602. [Google Scholar] [CrossRef] [PubMed]
- Fontal, A.; Bouma, M.J.; San-José, A.; López, L.; Pascual, M.; Rodó, X. Climatic signatures in the different COVID-19 pandemic waves across both hemispheres. Nat. Comput. Sci. 2021, 1, 655–665. [Google Scholar] [CrossRef]
- Soiza, R.L.; Scicluna, C.; Thomson, E.C. Efficacy and safety of COVID-19 vaccines in older people. Age Ageing 2021, 50, 279–283. [Google Scholar] [CrossRef]
- Brodin, P. Immune determinants of COVID-19 disease presentation and severity. Nat. Med. 2021, 27, 28–33. [Google Scholar] [CrossRef]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Levin, A.T.; Hanage, W.P.; Owusu-Boaitey, N.; Cochran, K.B.; Walsh, S.P.; Meyerowitz-Katz, G. Assessing the age specificity of infection fatality rates for COVID-19: Systematic review, meta-analysis, and public policy implications. Eur. J. Epidemiol. 2020, 35, 1123–1138. [Google Scholar] [CrossRef]
- Wang, W.; Shen, M.; Tao, Y.; Fairley, C.K.; Zhong, Q.; Li, Z.; Chen, H.; Ong, J.J.; Zhang, D.; Zhang, K.; et al. Elevated glucose level leads to rapid COVID-19 progression and high fatality. BMC Pulm. Med. 2021, 21, 64. [Google Scholar] [CrossRef]
- Team, I.C.-F. Modeling COVID-19 scenarios for the United States. Nat. Med. 2020, 27, 94–105. [Google Scholar] [CrossRef]
- IHME’s COVID-19 Projections. Available online: https://covid19.healthdata.org/ (accessed on 4 April 2021).
- WorldPop Population Counts. Available online: https://www.worldpop.org/project/list/ (accessed on 10 March 2021).
- Measuring performance on the Healthcare Access and Quality Index for 195 countries and territories and selected subnational locations: A systematic analysis from the Global Burden of Disease Study 2016. Lancet 2018, 391, 2236–2271. [CrossRef]
- Joinpoint Software. Available online: https://surveillance.cancer.gov/joinpoint/ (accessed on 17 June 2020).
- COVID-19 Vaccines. Available online: https://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/covid-19-vaccines (accessed on 19 March 2021).




{kind=link}
{kind=link}
{kind=link}
| State | Number of Confirmed Cases at the Date the 100th Cases were Reported | Number of Deaths at the Date the 100th Cases were Reported | Number of Days from 30 to 100 | Case Fatality Rate in the First 100 Confirmed Cases | Day of the Phase Turning Point | Number of Cases at Turning Point | Slow Growing Phase (Cases/Day) | Fast Growing Phase (Cases/Day) |
|---|---|---|---|---|---|---|---|---|
| Alabama | 106 | 0 | 4 | 0.0% | 3 | 9.73 | 2.60 | 16.16 |
| Alaska | 102 | 2 | 6 | 2.0% | 8 | 5.80 | 0.83 | 8.48 |
| Arizona | 104 | 1 | 3 | 1.0% | 51 | 2.60 | 0.04 | 17.49 |
| Arkansas | 100 | 0 | 3 | 0.0% | 8 | 28.21 | 3.91 | 32.41 |
| California | 100 | 0 | 7 | 0.0% | 37 | 12.69 | 0.31 | 13.04 |
| Colorado | 103 | 1 | 4 | 1.0% | 5 | 12.38 | 2.03 | 17.03 |
| Connecticut | 159 | 2 | 4 | 1.3% | 9 | 10.48 | 1.38 | 26.50 |
| Delaware | 104 | 0 | 6 | 0.0% | 7 | 10.36 | 1.68 | 10.11 |
| District of Columbia | 116 | 2 | 7 | 1.7% | 9 | 24.28 | 2.45 | 19.18 |
| Florida | 109 | 4 | 4 | 3.7% | 9 | 11.49 | 1.29 | 16.02 |
| Georgia | 118 | 1 | 6 | 0.8% | 9 | 11.79 | 1.44 | 19.87 |
| Hawaii | 106 | 0 | 7 | 0.0% | 12 | 6.71 | 0.58 | 11.25 |
| Idaho | 123 | 0 | 6 | 0.0% | 8 | 14.07 | 1.92 | 17.73 |
| Illinois | 104 | 0 | 5 | 0.0% | 47 | 3.74 | 0.06 | 16.14 |
| Indiana | 128 | 4 | 5 | 3.1% | 12 | 21.76 | 2.03 | 22.60 |
| Iowa | 105 | 0 | 6 | 0.0% | 10 | 27.65 | 2.58 | 14.21 |
| Kansas | 102 | 2 | 6 | 2.0% | 9 | 5.25 | 0.66 | 10.37 |
| Kentucky | 103 | 3 | 5 | 2.9% | 14 | 26.04 | 2.09 | 26.44 |
| Louisiana | 103 | 2 | 3 | 1.9% | 3 | 2.17 | 0.70 | 22.66 |
| Maine | 107 | 0 | 7 | 0.0% | 3 | 7.93 | 3.58 | 11.10 |
| Maryland | 108 | 1 | 5 | 0.9% | 9 | 16.32 | 1.85 | 16.19 |
| Massachusetts | 110 | 0 | 4 | 0.0% | 36 | 1.41 | 0.02 | 20.75 |
| Michigan | 334 | 3 | 6 | 0.9% | 7 | 45.55 | 7.81 | 90.68 |
| Minnesota | 115 | 0 | 6 | 0.0% | 8 | 7.20 | 1.04 | 14.27 |
| Mississippi | 140 | 1 | 4 | 0.7% | 7 | 21.09 | 3.63 | 34.25 |
| Missouri | 130 | 3 | 4 | 2.3% | 11 | 6.56 | 0.68 | 25.23 |
| Montana | 121 | 1 | 6 | 0.8% | 11 | 14.94 | 1.53 | 13.78 |
| Nebraska | 102 | 0 | 13 | 0.0% | 12 | 16.23 | 1.54 | 6.81 |
| Nevada | 165 | 1 | 5 | 0.6% | 10 | 12.34 | 1.34 | 14.71 |
| New Hampshire | 101 | 1 | 6 | 1.0% | 14 | 7.02 | 0.48 | 8.96 |
| New Jersey | 176 | 2 | 4 | 1.1% | 9 | 21.22 | 2.68 | 46.30 |
| New Mexico | 100 | 0 | 6 | 0.0% | 11 | 37.95 | 3.62 | 21.07 |
| New York | 106 | 0 | 3 | 0.0% | 4 | 13.33 | 4.38 | 29.65 |
| North Carolina | 104 | 0 | 5 | 0.0% | 10 | 5.14 | 0.53 | 11.31 |
| North Dakota | 109 | 2 | 9 | 1.8% | 6 | 1.06 | 0.02 | 6.50 |
| Ohio | 120 | 0 | 5 | 0.0% | 4 | 8.62 | 2.06 | 15.74 |
| Oklahoma | 106 | 3 | 6 | 2.8% | 10 | 4.78 | 0.49 | 10.92 |
| Oregon | 114 | 3 | 9 | 2.6% | 12 | 11.16 | 1.00 | 8.48 |
| Pennsylvania | 101 | 0 | 5 | 0.0% | 7 | 17.83 | 2.89 | 16.65 |
| Rhode Island | 106 | 0 | 6 | 0.0% | 13 | 4.96 | 0.33 | 7.26 |
| South Carolina | 126 | 1 | 5 | 0.8% | 10 | 23.82 | 2.59 | 19.86 |
| South Dakota | 100 | 1 | 7 | 1.0% | 12 | 14.77 | 0.72 | 9.47 |
| Tennessee | 155 | 0 | 6 | 0.0% | 7 | 5.18 | 0.81 | 11.24 |
| Texas | 106 | 1 | 8 | 0.9% | 26 | 1.99 | 0.06 | 11.27 |
| Utah | 112 | 0 | 5 | 0.0% | 8 | 7.16 | 1.03 | 14.20 |
| Vermont | 123 | 8 | 5 | 6.5% | 13 | 13.52 | 1.22 | 20.61 |
| Virginia | 115 | 2 | 8 | 1.7% | 4 | 7.25 | 1.98 | 10.57 |
| Washington | 110 | 9 | 5 | 8.2% | 40 | 1.18 | 0.01 | 15.80 |
| West Virginia | 113 | 0 | 5 | 0.0% | 8 | 16.71 | 2.47 | 19.43 |
| Wisconsin | 106 | 0 | 4 | 0.0% | 37 | 1.27 | 0.01 | 14.65 |
| Wyoming | 121 | 0 | 8 | 0.0% | 12 | 22.14 | 2.09 | 10.84 |
| Total/Mean (95%CI) | 118.8 (108.9–128.7) | 1.3 (0.8–1.8) | 5.6 (5.1–6.1) | 1.1% (0.6–1.6%) | 13 (9.8–16.1) | 12.6 (10–15.3) | 1.6 (1.2–2) | 18.2 (14.5–21.8) |
| State | Phase * | K1 1 | Δt1 2 | tm1 3 | K2 | Δt2 | tm2 | K3 | Δt3 | tm3 | K4 | Δt4 | tm4 | K |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Alabama | 2 | 158,058 | 113.0 | 139.0 | 356,678 | 105 | 287 | - | - | - | - | - | - | 514,736 |
| Alaska | 2 | 4868 | 74.8 | 122.0 | 55,034 | 113 | 265 | - | - | - | - | - | - | 59,902 |
| Arizona | 2 | 219,769 | 76.2 | 166.0 | 621,947 | 82 | 339 | - | - | - | - | - | - | 841,716 |
| Arkansas | 2 | 89,317 | 137.0 | 151.0 | 250,964 | 115 | 289 | - | - | - | - | - | - | 340,281 |
| California | 2 | 937,689 | 124.0 | 188.0 | 2,683,967 | 67.8 | 341 | - | - | - | - | - | - | 3,621,656 |
| Colorado | 4 | 27,074 | 76.9 | 58.8 | 29,840 | 62.8 | 142 | 352,188 | 85.7 | 273 | 402,309 | 86.7 | 422 | 811,411 |
| Connecticut | 2 | 46,842 | 54.6 | 49.9 | 263,325 | 124 | 296 | - | - | - | - | - | - | 310,167 |
| Delaware | 4 | 10,156 | 50.0 | 54.8 | 10,122 | 78.8 | 145 | 71,115 | 103 | 294 | 95,159 | 92.3 | 443 | 186,552 |
| District of Columbia | 4 | 10,694 | 67.2 | 61.3 | 4544 | 87.5 | 156 | 257,73 | 104 | 296 | 45,849 | 113 | 449 | 86,860 |
| Florida | 2 | 676,134 | 70.0 | 141.0 | 1,417,834 | 126 | 309 | - | - | - | - | - | - | 2,093,968 |
| Georgia | 4 | 42,444 | 54.2 | 53.9 | 302,132 | 97.9 | 156 | 651,457 | 92.6 | 307 | 1,051,352 | 119 | 469 | 2,047,385 |
| Hawaii | 2 | 14,189 | 82.8 | 175.0 | 15,304 | 119 | 302 | - | - | - | - | - | - | 29,493 |
| Idaho | 2 | 31,874 | 73.2 | 133.0 | 147,958 | 118 | 266 | - | - | - | - | - | - | 179,832 |
| Illinois | 3 | 129,678 | 52.8 | 101.0 | 122,400 | 63.3 | 198 | 960,542 | 100 | 315 | - | - | - | 1,212,620 |
| Indiana | 3 | 39,662 | 78.6 | 59.4 | 65,411 | 78.1 | 163 | 575,259 | 92.3 | 278 | - | - | - | 680,332 |
| Iowa | 4 | 23,273 | 60.0 | 60.0 | 52,000 | 90 | 150 | 208,015 | 70.8 | 252 | 65,336 | 81 | 326 | 348,624 |
| Kansas | 3 | 16,721 | 50.0 | 65.0 | 43,685 | 75 | 170 | 241,620 | 96.1 | 280 | - | - | - | 302,026 |
| Kentucky | 4 | 14,453 | 64.4 | 73.3 | 58,258 | 87.7 | 178 | 331,578 | 106 | 288 | 381,435 | 93.5 | 433 | 785,724 |
| Louisiana | 3 | 43,792 | 30.0 | 30.0 | 114,559 | 58.4 | 140 | 289,018 | 106 | 292 | - | - | - | 447,369 |
| Maine | 3 | 4594 | 117.0 | 86.2 | 40,123 | 84.9 | 296 | 35,078 | 107 | 422 | - | - | - | 79,795 |
| Maryland | 3 | 63,754 | 65.7 | 67.0 | 59,507 | 78.4 | 156 | 279,222 | 89.6 | 296 | - | - | - | 402,483 |
| Massachusetts | 2 | 114,764 | 62.1 | 91.4 | 515,403 | 112 | 334 | - | - | - | - | - | - | 630,167 |
| Michigan | 4 | 65,674 | 65.7 | 45.0 | 66,908 | 78.2 | 157 | 479,761 | 77.1 | 265 | 480,316 | 90.8 | 409 | 1,092,659 |
| Minnesota | 4 | 42,237 | 60.9 | 81.5 | 56,831 | 69.2 | 172 | 304,990 | 50 | 259 | 101,135 | 60.6 | 326 | 505,193 |
| Mississippi | 2 | 112,294 | 140.0 | 147.0 | 194,676 | 96.4 | 293 | - | - | - | - | - | - | 306,970 |
| Missouri | 3 | 16,177 | 55.0 | 50.0 | 102,000 | 80 | 165 | 399,748 | 97.2 | 271 | - | - | - | 517,925 |
| Montana | 1 | 102,982 | 126.0 | 253.0 | - | - | - | - | - | - | - | - | - | 102,982 |
| Nebraska | 2 | 26,763 | 106.0 | 108.0 | 179,197 | 114 | 283 | - | - | - | - | - | - | 205,960 |
| Nevada | 2 | 79,921 | 96.3 | 141.0 | 221,403 | 94.9 | 286 | - | - | - | - | - | - | 301,324 |
| New Hampshire | 2 | 6231 | 78.4 | 72.2 | 76,994 | 110 | 306 | - | - | - | - | - | - | 83,225 |
| New Jersey | 2 | 180,120 | 64.5 | 49.2 | 738,290 | 131 | 310 | - | - | - | - | - | - | 918,410 |
| New Mexico | 2 | 22,510 | 108.0 | 102.0 | 166,650 | 101 | 272 | - | - | - | - | - | - | 189,160 |
| New York | 2 | 411,495 | 49.5 | 46.6 | 1,495,624 | 121 | 318 | - | - | - | - | - | - | 1,907,119 |
| North Carolina | 2 | 240,328 | 146.0 | 153.0 | 687,653 | 104 | 308 | - | - | - | - | - | - | 927,981 |
| North Dakota | 3 | 9515 | 109.0 | 118.0 | 88,707 | 83.1 | 242 | 46,699 | 77.4 | 421 | - | - | - | 144,921 |
| Ohio | 3 | 32,254 | 58.9 | 42.0 | 76,174 | 50 | 139 | 893,327 | 97.3 | 281 | - | - | - | 1,001,755 |
| Oklahoma | 2 | 115,630 | 137.0 | 169.0 | 325,333 | 97.5 | 296 | - | - | - | - | - | - | 440,963 |
| Oregon | 2 | 27,810 | 116.0 | 141.0 | 135,919 | 112 | 294 | - | - | - | - | - | - | 163,729 |
| Pennsylvania | 3 | 82,241 | 52.0 | 45.0 | 44,856 | 50 | 144 | 900,730 | 110 | 292 | - | - | - | 1,027,827 |
| Rhode Island | 2 | 17,323 | 62.2 | 63.4 | 118,673 | 122 | 295 | - | - | - | - | - | - | 135,996 |
| South Carolina | 2 | 156,103 | 112.0 | 145.0 | 405,559 | 105 | 311 | - | - | - | - | - | - | 561,662 |
| South Dakota | 2 | 6409 | 89.6 | 58.9 | 108,453 | 108 | 246 | - | - | - | - | - | - | 114,862 |
| Tennessee | 2 | 207,342 | 126.0 | 150.0 | 577,027 | 95.1 | 290 | - | - | - | - | - | - | 784,369 |
| Texas | 2 | 786,183 | 116.0 | 169.0 | 2,110,206 | 122 | 326 | - | - | - | - | - | - | 2,896,389 |
| Utah | 2 | 46,055 | 104.0 | 134.0 | 346,926 | 130 | 289 | - | - | - | - | - | - | 392,981 |
| Vermont | 2 | 1114 | 41.6 | 33.9 | 20,062 | 153 | 327 | - | - | - | - | - | - | 21,176 |
| Virginia | 3 | 61,158 | 88.4 | 76.7 | 106,055 | 91.3 | 170 | 454,702 | 98 | 308 | - | - | - | 621,915 |
| Washington | 3 | 17,699 | 47.5 | 76.0 | 53,412 | 76.8 | 178 | 294,323 | 122 | 331 | - | - | - | 365,434 |
| West Virginia | 2 | 11,017 | 101.0 | 130.0 | 129,068 | 105 | 281 | - | - | - | - | - | - | 140,085 |
| Wisconsin | 2 | 56,786 | 109.0 | 142.0 | 568,147 | 114 | 288 | - | - | - | - | - | - | 624,933 |
| Wyoming | 2 | 2915 | 56.0 | 109.0 | 52,500 | 93.7 | 261 | - | - | - | - | - | - | 55,415 |
| Total/Mean (95%CI) | - | 111,060.5 (56,996.6–165,124.4) | 83.5 (75–92) | 101.5 (87.6–115.5) | 329,686 (178,465.5–480,906.5) | 96.7 (90.2–103.1) | 246.5 (226.9–266.1) | 389,757.3 (256,873.4–522,641.1) | 94.1 (86.6–101.6) | 301.1 (279.8–322.3) | 327,861.4 (43,631.9–612,090.8) | 92.1 (76.9–107.3) | 409.6 (364–455.3) | 638,557.2 (434,066.4–843,048.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, H.; Tao, Y.; Shen, M.; Li, R.; Zou, M.; Zhang, L.; Zhang, L. What Is the Impact of Early and Subsequent Epidemic Characteristics on the Pre-delta COVID-19 Epidemic Size in the United States? Pathogens 2022, 11, 576. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11050576
Lai H, Tao Y, Shen M, Li R, Zou M, Zhang L, Zhang L. What Is the Impact of Early and Subsequent Epidemic Characteristics on the Pre-delta COVID-19 Epidemic Size in the United States? Pathogens. 2022; 11(5):576. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11050576
Chicago/Turabian StyleLai, Hao, Yusha Tao, Mingwang Shen, Rui Li, Maosheng Zou, Leilei Zhang, and Lei Zhang. 2022. "What Is the Impact of Early and Subsequent Epidemic Characteristics on the Pre-delta COVID-19 Epidemic Size in the United States?" Pathogens 11, no. 5: 576. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens11050576