
Hepatitis E Virus in Finland: Epidemiology and Risk in Blood Donors and in the General Population
Abstract
:1. Introduction
2. Materials and Methods
2.1. Blood Donor Samples
2.2. National Data on Hepatitis E in the Finnish Infectious Disease Registry
2.3. HEV RNA Screening of Blood Donor Samples with Procleix HEV Assay
2.4. Anti-HEV IgG and Anti-HEV IgM Analysis of Blood Donor Samples
2.5. HEV RNA Analysis with the Confirmatory PCR Test and HEV Genotyping
2.6. Risk Assessment Modelling
- (1)
- The HEV RNA prevalence in fresh components is the same as that in whole blood donors,
- (2)
- A total of 42% of HEV RNA-positive donations result in a transfusion transmission infection (viremia, seroconversion) [11],
- (3)
- A total of 5% of the HEV-infected recipients will have an adverse outcome (symptomatic infection) [11],
- (4)
- A total of 1% of the HEV-infected recipients have a severe adverse outcome (e.g., untreatable chronic infection) [11],
- (5)
- Background immunity in the recipient population is not considered,
- (6)
- A total of 99% of issued red cells and 90% of issued platelet components are transfused.
3. Results
3.1. HEV RNA in Blood Donors
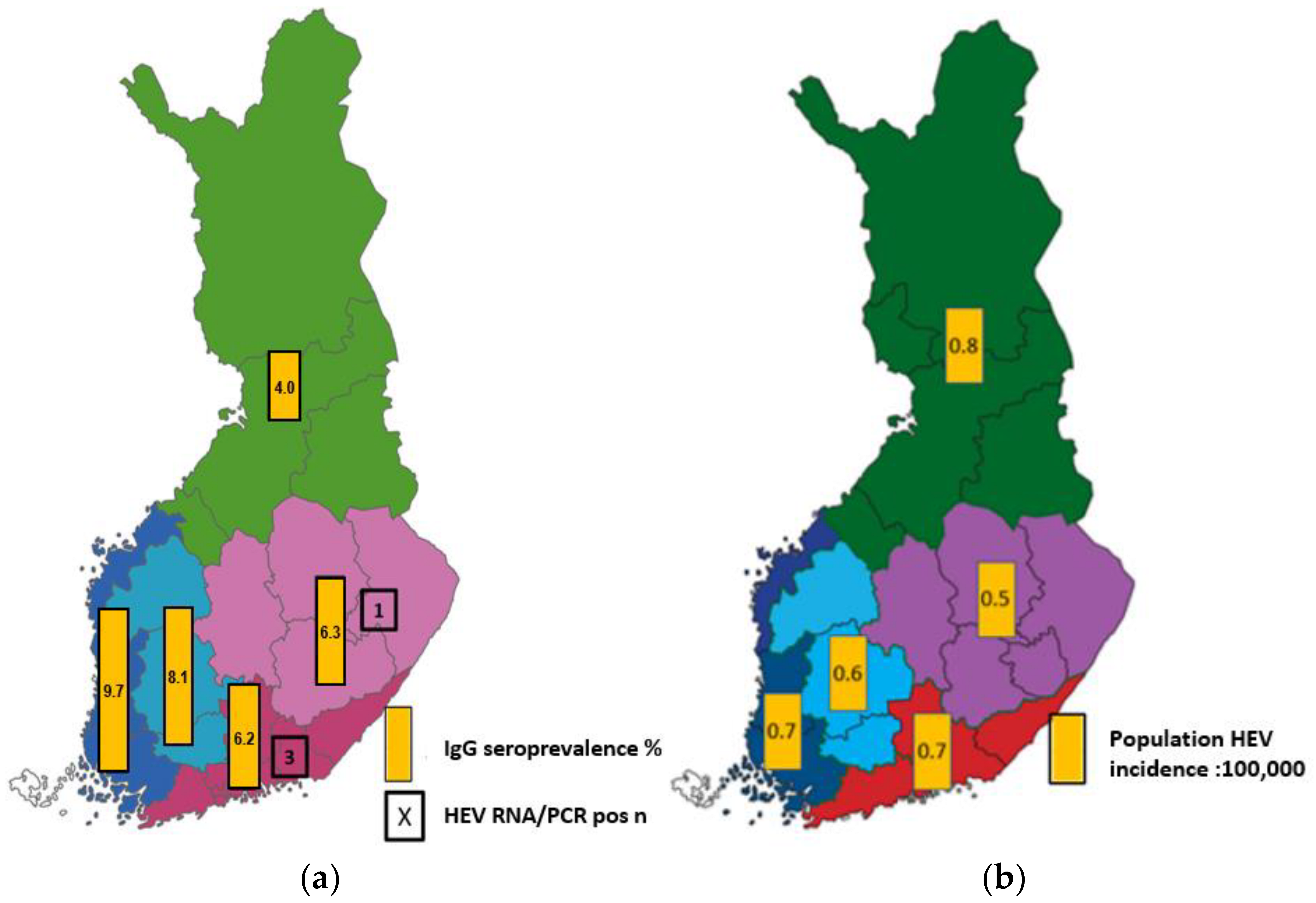
3.2. HEV Seroprevalence in Blood Donors
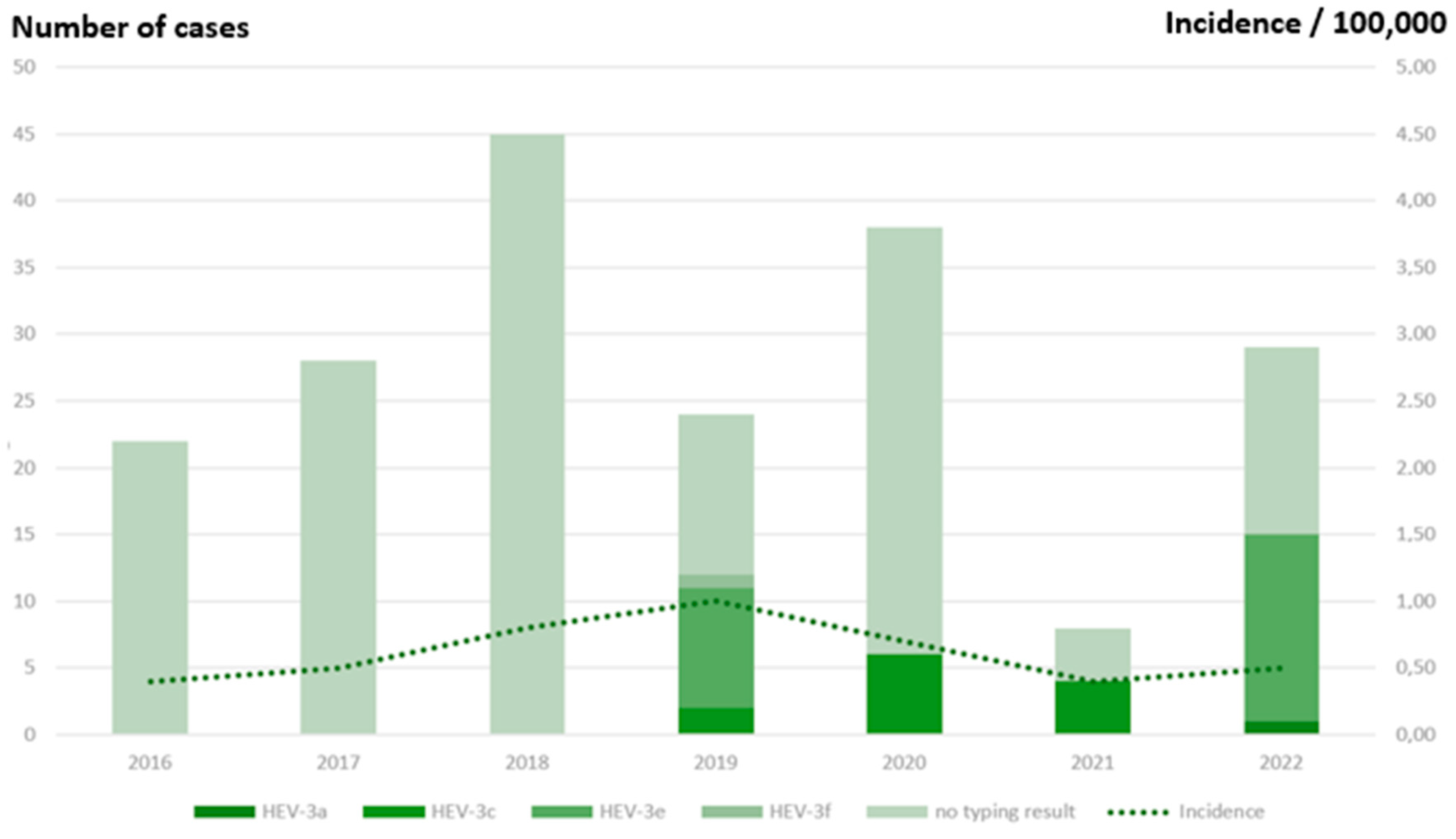
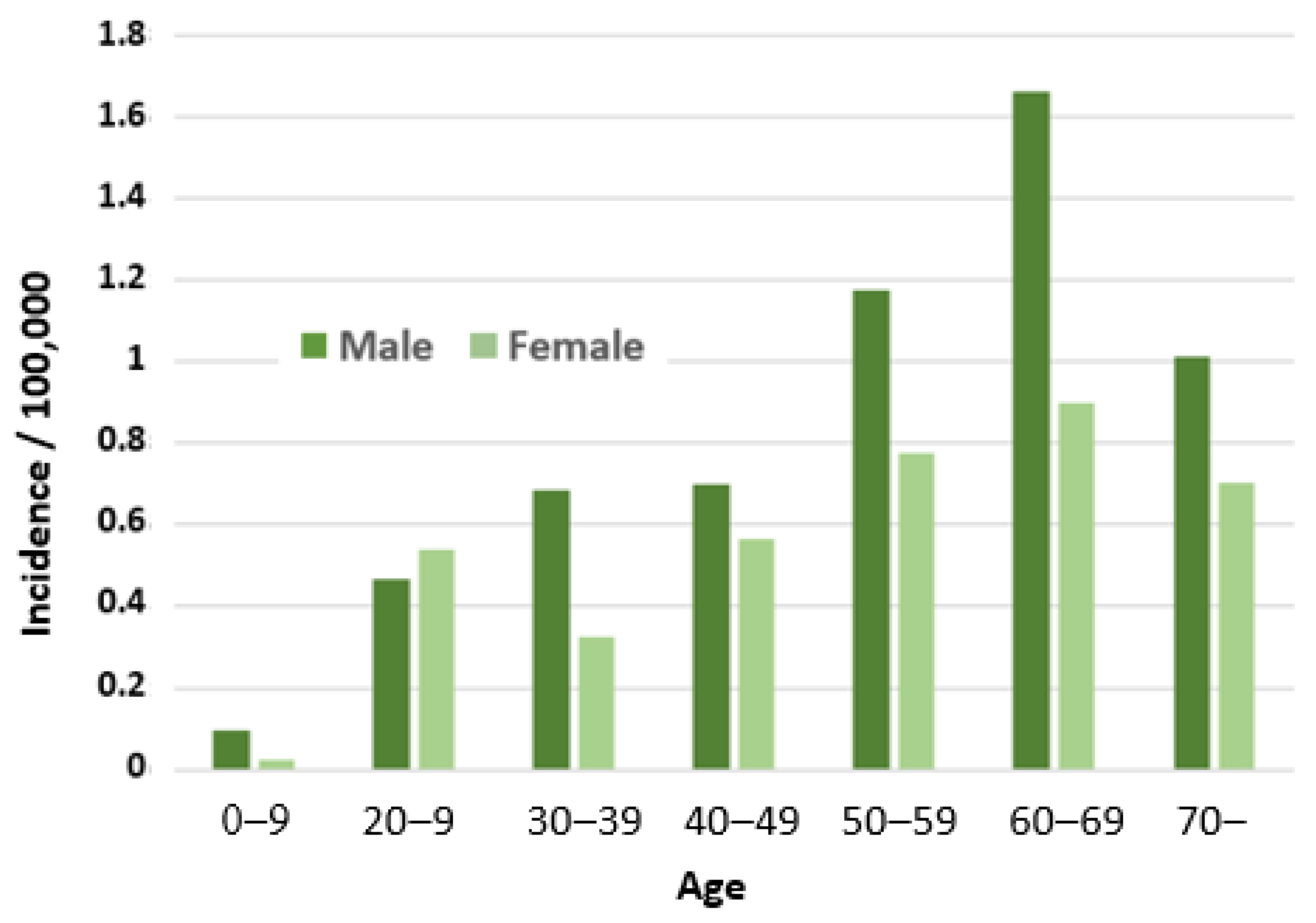
3.3. HEV Notifications in Finnish Infectious Disease Registry
3.4. Assessment of Blood Transfusion-transmitted HEV Infection
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khuroo, M.S.; Khuroo, M.S.; Khuroo, N.S. Hepatitis E: Discovery, global impact, control and cure. World J. Gastroenterol. 2016, 22, 7030–7045. [Google Scholar] [CrossRef]
- Anckorn, M.J.; Tedder, R.S. Hepatitis E: The current state of play. Transfus. Med. 2017, 27, 84–95. [Google Scholar] [CrossRef] [PubMed]
- Adlhoch, C.; Avellon, A.; Baylis, S.A.; Ciccaglione, A.R.; Couturier, E.; Sousa, R.; Epštein, J.; Ethelberg, S.; Faber, M.; Fehér, Á.; et al. Hepatitis E virus: Assessment of the epidemiological situation in humans in Europe, 2014/15. J. Clin. Virol. 2016, 82, 9–16. [Google Scholar] [CrossRef]
- Aspinall, E.J.; Couturier, E.; Faber, M.; Said, B.; Ijaz, S.; Tavoschi, L.; Takkinen, J.; Adlhoch, C.; on behalf of the country experts. Hepatitis E virus infection in Europe: Surveillance and descriptive epidemiology of confirmed cases, 2005 to 2015. Euro Surveill. 2017, 22, 30561. [Google Scholar] [CrossRef] [Green Version]
- Horvatits, T.; Schulze zur Wiesch, J.; Lütgehetmann, M.; Lohse, A.W.; Pischke, S. The clinical perspective on hepatitis E. Viruses 2019, 11, 617. [Google Scholar] [CrossRef] [Green Version]
- Woo, P.C.; Lau, S.K.; Teng, J.L.; Tsang, A.K.; Joseph, M.; Wong, E.Y.; Tang, Y.; Sivakumar, S.; Xie, J.; Bai, R.; et al. New hepatitis E virus genotype in camels, the Middle East. Emerg. Infect. Dis. 2014, 20, 1044–1048. [Google Scholar] [CrossRef]
- Lee, G.H.; Tan, B.H.; Teo, E.C.; Lim, S.G.; Dan, Y.Y.; Wee, A.; Aw, P.P.; Zhu, Y.; Hibberd, M.L.; Tan, C.K.; et al. Chronic infection with camelid hepatitis E virus in a liver transplant recipient who regularly consumes camel meat and milk. Gastroenterology 2016, 150, 355–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaussade, H.; Rigaud, E.; Allix, A.; Carpentier, A.; Touzé, A.; Delzescaux, D.; Choutet, P.; Garcia-Bonnet, N.; Coursaget, P. Hepatitis E virus seroprevalence and risk factors for individuals in working contact with animals. J. Clin. Virol. 2013, 58, 504–508. [Google Scholar] [CrossRef]
- Krumbholz, A.; Mohn, U.; Lange, J.; Motz, M.; Wenzel, J.J.; Jilg, W.; Walther, M.; Straube, E.; Wutzler, P.; Zell, R. Prevalence of hepatitis E virus-specific antibodies in humans with occupational exposure to pigs. Med. Microbiol. Immunol. 2012, 201, 239–244. [Google Scholar] [CrossRef]
- Cheung, C.K.M.; Wong, S.H.; Law, A.W.H.; Law, M.F. Transfusion-transmitted hepatitis E: What we know so far? World J. Gastroenterol. 2022, 28, 47–75. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, P.E.; Ijaz, S.; Brailsford, S.R.; Brett, R.; Dicks, S.; Haywood, B.; Kennedy, I.T.R.; Kitchen, A.; Patel, P.; Poh, J.; et al. Hepatitis E virus in blood components: A prevalence and transmission study in southeast England. Lancet 2014, 384, 1766–1773. [Google Scholar] [CrossRef] [Green Version]
- Hoad, V.C.; Gibbs, T.; Ravikumara, M.; Nash, M.; Levy, A.; Tracy, S.L.; Mews, C.; Perkowska-Guse, Z.; Faddy, H.M.; Bowden, S. First confirmed case of transfusion-transmitted hepatitis E in Australia. Med. J. Aust. 2017, 206, 289–290. [Google Scholar] [CrossRef] [PubMed]
- Tedder, R.S.; Tettmar, K.I.; Brailsford, S.R.; Said, B.; Ushiro-Lumb, I.; Kitchen, A.; Morgan, D.; Lattimore, S.; Tossell, J.; Ijaz, S.; et al. Virology, serology, and demography of hepatitis E viremic blood donors in South East England. Transfusion 2016, 56, 1529–1536. [Google Scholar] [CrossRef]
- Bi, H.; Yang, R.; Wu, C.; Xia, J. Hepatitis E virus and blood transfusion safety. Epidemiol. Infect. 2020, 148, 1–9. [Google Scholar] [CrossRef]
- Hauser, L.; Roque-Afonso, A.M.; Beylouné, A.; Simonet, M.; Deau Fischer, B.; Burin des Roziers, N.; Mallet, V.; Tiberghien, P.; Bierling, P. Hepatitis E transmission by transfusion of intercept blood system-treated plasma. Blood 2014, 123, 796–797. [Google Scholar] [CrossRef] [Green Version]
- Boland, F.; Martinez, A.; Pomeroy, L.; O’Flaherty, N. Blood donor screening for hepatitis E virus in the European union. Transfus. Med. Hemother. 2019, 46, 95–103. [Google Scholar] [CrossRef]
- Harvala, H.; Hewitt, P.E.; Reynolds, C.; Pearson, C.; Haywood, B.; Tettmar, K.I.; Ushiro-Lumb, I.; Brailsford, S.R.; Tedder, R.; Ijaz, S. Hepatitis E virus in blood donors in England, 2016 to 2017: From selective to universal screening. Euro Surveill. 2019, 24, 1800386. [Google Scholar] [CrossRef] [Green Version]
- de Vos, A.; Janssen, M.P.; Zaaijer, H.L.; Hogema, B.M. Cost-effectiveness of the screening of blood donations for hepatitis E virus in the Netherlands. Transfusion 2017, 57, 258–266. [Google Scholar] [CrossRef] [PubMed]
- O’Riordan, J.; Boland, F.; Williams, P.; Donnellan, J.; Hogema, B.M.; Ijaz, S.; Murphy, W.G. Hepatitis E virus infection in the Irish blood donor population. Transfusion 2016, 56, 2868–2876. [Google Scholar] [CrossRef] [PubMed]
- Vollmer, T.; Diekmann, J.; Knabbe, C.; Dreier, J. Hepatitis E virus blood donor NAT screening: As much as possible or as much as needed? Transfusion 2019, 59, 612–622. [Google Scholar] [CrossRef]
- Gallian, P.; Lhomme, S.; Piquet, Y.; Sauné, K.; Abravanel, F.; Assal, A.; Tiberghien, P.; Izopet, J. Hepatitis E virus infections in blood donors, France. Emerg. Infect. Dis. 2014, 20, 1914–1917. [Google Scholar] [CrossRef]
- Pillonel, J.; Maugard, C.; Sommen, C.; Figoni, J.; Pierre, C.; LeCam, S.; Richard, P.; Morel, P.; Gallian, P.; Laperche, S. Risk of a blood donation contaminated with hepatitis E virus entering the blood supply before the implementation of universal RNA screening in France. Vox Sang. 2022, 117, 1411–1414. [Google Scholar] [CrossRef]
- Niederhauser, C.; Widmer, N.; Hotz, M.; Tinguely, C.; Fontana, S.; Allemann, G.; Borri, M.; Infanti, L.; Sarraj, A.; Sigle, J.; et al. Current hepatitis E virus seroprevalence in Swiss blood donors and apparent decline from 1997 to 2016. Euro Surveill. 2018, 23, 1700616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bes, M.; Costafreda, M.I.; Riveiro-Barciela, M.; Piron, M.; Rico, A.; Quer, J.; Puig, L.; Sauleda, S. Effect of hepatitis E virus RNA universal blood donor screening, Catalonia, Spain, 2017–2020. Emerg. Infect. Dis. 2022, 28, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Harritshøj, L.H.; Holm, D.K.; Saekmose, S.G.; Jensen, B.A.; Hogema, B.M.; Fischer, T.K.; Midgley, S.E.; Krog, J.S.; Erikstrup, C.; Henrik Ullum, H. Low transfusion transmission of hepatitis E among 25,637 single-donation, nucleic acid-tested blood donors. Transfusion 2016, 56, 2225–2232. [Google Scholar] [CrossRef] [PubMed]
- Kantala, T. Presence of Hepatitis E Virus (HEV) and Markers for HEV Infection in Production Swine, Human Patients with Unexplained Hepatitis, and Veterinarians in Finland. PhD Thesis, University of Helsinki, Helsinki, Finland, 28 April 2017. [Google Scholar]
- Kantala, T.; Kinnunen, P.M.; Oristo, S.; Jokelainen, P.; Vapalahti, O.; Maunula, L. Hepatitis E virus antibodies in finnish veterinarians. Zoonoses Public Health 2017, 64, 165–184. [Google Scholar] [CrossRef]
- Kettunen, O.; Vuorela, M.; Kuusi, M.; Kantala, T.; Maunula, L.; Jalava, K.; Blomster, T.; Koskela, R.; Haapasaari, K.M. Suomalaismiehen kotoperäinen E-hepatiittitartunta [A domestic human case of hepatitis E in Finland]. Duodecim 2013, 129, 2169–2173. (In Finnish) [Google Scholar]
- Ebeling, F.; Rasi, V. Hepatitis E virus: No evidence of parenteral transmission in Finland. Thromb Haemost. 1995, 74, 1385–1386. [Google Scholar]
- Boxman, I.L.A.; Jansen, C.C.C.; Hägele, G.; Zwartkruis-Nahuis, A.; Cremer, J.; Vennema, H.; Tijsma, A.S.L. Porcine blood used as ingredient in meat productions may serve as a vehicle for hepatitis E virus transmission. Int. J. Food Microbiol. 2017, 257, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Nix, W.A.; Oberste, M.S.; Pallansch, M.A. Sensitive, seminested PCR amplification of VP1 sequences for direct identification of all enterovirus serotypes from original clinical specimens. J. Clin. Microbiol. 2006, 44, 2698–2704. [Google Scholar] [CrossRef] [Green Version]
- Tamura, K.; Dudley, J.; Nei, M.; Kumar, S. MEGA4: Molecular evolutionary genetics analysis (MEGA) software version 4.0. Mol. Biol. Evol. 2007, 24, 1596–1599. [Google Scholar] [CrossRef]
- Saitou, N.; Nei, M. The neighbor-joining method: A new method for reconstructing phylogenetic trees. Mol. Biol. Evol. 1987, 4, 406–425. [Google Scholar] [PubMed]
- Hoad, V.C.; Seed, C.R.; Fryk, J.J.; Harley, R.R.; Flower, R.L.P.; Hogema, B.M.; Kiely, P.; Faddy, H.M. Hepatitis E virus RNA in Australian blood donors: Prevalence and risk assessment. Vox Sang. 2017, 112, 614–621. [Google Scholar] [CrossRef] [PubMed]
- Goel, A.; Vijay, H.J.; Katiyar, H.; Aggarwal, R. Prevalence of hepatitis E viraemia among blood donors: A systematic review. Vox Sang. 2020, 115, 120–132. [Google Scholar] [CrossRef] [PubMed]
- Vercouter, A.S.; Van Houtte, F.; Verhoye, L.; González Fraile, I.; Blanco, L.; Compernolle, V.; Meuleman, P. Hepatitis E virus prevalence in Flemish blood donors. J. Viral. Hepat. 2019, 26, 1218–1223. [Google Scholar] [CrossRef] [PubMed]
- Fischer, C.; Hofmann, M.; Danzer, M.; Hofer, K.; Kaar, J.; Gabriel, C. Seroprevalence and incidence of hepatitis E in blood donors in Upper Austria. PLoS ONE 2015, 10, e0119576. [Google Scholar] [CrossRef] [PubMed]
- Abravanel, F.; Goutagny, N.; Joffray, R.; Eichenlaub, E.; Baron, S.; Aversenq, A.; Bourg, S.; Mercier, L.; Larue Triolet, A.; Poiraul, D.; et al. Performance characteristics of the VIDAS® ANTI-HEV IgM and IgG assays. J. Clin. Virol. 2019, 112, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Cattoir, L.; Vercauteren, K.O.A.; Padalko, E.; De Beenhouwer, H.; Van Vaerenbergh, K.; Boel, A. Are VIDAS® anti-HEV IgM and IgG assays fit for reliable diagnosis of hepatitis E virus infections? Comparison & case story telling. Acta Clin. Belg. 2019, 76, 25–31. [Google Scholar]
- Kamar, N.; Bendall, R.; Legrand-Abravanel, F.; Xia, N.S.; Ijaz, S.; Izopet, J.; Dalton, H.R. Hepatitis E. Lancet 2012, 379, 2477–2488. [Google Scholar] [CrossRef]
- Fredriksson-Ahomaa, M.; London, L.; Skrzypczak, T.; Kantala, T.; Laamanen, I.; Biström, M.; Maunula, L.; Gadd, T. Foodborne zoonoses common in hunted wild boars. Ecohealth 2020, 17, 512–522. [Google Scholar] [CrossRef]
- Loikkanen, E.; Oristo, S.; Hämäläinen, N.; Jokelainen, P.; Kantala, T.; Sukura, A.; Maunula, L. Antibodies against hepatitis E virus (HEV) in European moose and white-tailed deer in Finland. Food Environ. Virol. 2020, 12, 333–341. [Google Scholar] [CrossRef]
- Tedder, R.S.; Ijaz, S.; Kitchen, A.; Ushiro-Lumb, I.; Tettmar, K.I.; Hewitt, P.; Andrews, N. Hepatitis E risks: Pigs or blood-that is the question. Transfusion 2017, 57, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Baymakova, M.; Terzieva, K.; Popov, R.; Grancharova, E.; Kundurzhiev, T.; Pepovich, R.; Tsachev, I. Seroprevalence of hepatitis E virus infection among blood donors in Bulgaria. Viruses 2021, 16, 492. [Google Scholar] [CrossRef]
- Miletić, M.; Vuk, T.; Hećimović, A.; Stojić Vidović, M.; Jemeršić, L.; Jukić, I. Estimation of the hepatitis E assay-dependent seroprevalence among Croatian blood donors. Transfus. Clin. Biol. 2019, 26, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Holm, D.K.; Moessner, B.K.; Engle, R.E.; Zaaijer, H.L.; Georgsen, J.; Purcell, R.H.; Christensen, P.B. Declining prevalence of hepatitis E antibodies among Danish blood donors. Transfusion 2015, 55, 1662–1667. [Google Scholar] [CrossRef] [PubMed]
- Mansuy, J.M.; Gallian, P.; Dimeglio, C.; Saune, K.; Arnaud, C.; Pelletier, B.; Morel, P.; Legrand, D.; Tiberghien, P.; Izopet, J. A nationwide survey of hepatitis E viral infection in French blood donors. Hepatology 2016, 63, 1145–1154. [Google Scholar] [CrossRef]
- Vollmer, T.; Diekmann, J.; Johne, R.; Eberhardt, M.; Knabbe, C.; Dreier, J. Novel approach for detection of hepatitis E virus infection in German blood donors. J. Clin. Microbiol. 2012, 50, 2708–2713. [Google Scholar] [CrossRef] [Green Version]
- Spada, E.; Pupella, S.; Pisani, G.; Bruni, R.; Chionne, P.; Madonna, E.; Villano, U.; Simeoni, M.; Fabi, S.; Marano, G. A nationwide retrospective study on prevalence of hepatitis E virus infection in Italian blood donors. Blood Transfus. 2018, 16, 413–421. [Google Scholar]
- Lucarelli, C.; Spada, E.; Taliani, G.; Chionne, P.; Madonna, M.; Marcantonio, C.; Pezzotti, P.; Bruni, R.; La Rosa, G.; Pisani, G.; et al. High prevalence of anti-hepatitis E virus antibodies among blood donors in central Italy, February to March 2014. Euro Surveill. 2016, 21, 30299. [Google Scholar] [CrossRef]
- Slot, E.; Hogema, B.M.; Riezebos-Brilman, A.; Kok, T.M.; Molier, M.; Zaaijer, H.L. Silent hepatitis E virus infection in Dutch blood donors, 2011 to 2012. Euro Surveill. 2013, 18, 20550. [Google Scholar] [CrossRef] [Green Version]
- Hogema, B.M.; Molier, M.; Sjerps, M.; de Waal, M.; van Swieten, P.; van de Laar, T.; Molenaar-de Backer, M.; Zaaijer, H.L. Incidence and duration of hepatitis E virus infection in Dutch blood donors. Transfusion 2016, 56, 722–728. [Google Scholar] [CrossRef] [PubMed]
- Grabarczyk, P.; Sulkowska, E.; Gdowska, J.; Kopacz, A.; Liszewski, G.; Kubicka-Russel, D.; Baylis, S.A.; Corman, V.M.; Noceń, E.; Piotrowski, D.; et al. Molecular and serological infection marker screening in blood donors indicates high endemicity of hepatitis E virus in Poland. Transfusion 2018, 58, 1245–1253. [Google Scholar] [CrossRef]
- Sauleda, S.; Ong, E.; Bes, M.; Janssen, A.; Cory, R.; Babizki, M.; Linnen, J.M. Seroprevalence of hepatitis E virus (HEV) and detection of HEV RNA with a transcription-mediated amplification assay in blood donors from Catalonia (Spain). Transfusion 2015, 55, 972–979. [Google Scholar] [CrossRef]
- Norder, H.; Karlsson, M.; Mellgren, Å.; Konar, J.; Sandberg, E.; Lasson, A.; Castedal, M.; Magnius, L.; Lagging, M. Diagnostic performance of five assays for anti-hepatitis E virus IgG and IgM in a large cohort study. J. Clin. Microbiol. 2016, 54, 549–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baylis, S.A.; Gärtner, T.; Nick, S.; Ovemyr, J.; Blümel, J. Occurrence of hepatitis E virus RNA in plasma donations from Sweden, Germany and the United States. Vox Sang. 2012, 103, 89–90. [Google Scholar] [CrossRef] [PubMed]
- Honkanen, E. Prevalence of Hepatitis E Virus in Finnish Slaughterhouses. Master’s thesis, University of Helsinki, Helsinki, Finland, 2018. [Google Scholar]
- Mitronen, A. Prevalence of Hepatitis E Virus in Finnish Beef. Master’s thesis, University of Helsinki, Helsinki, Finland, 2021. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Healthcare Region * | Population in Finland (31 December 2020) | HEV Cases in FIDR Year 2020 | HEV Incidence/100,000 | Blood Donations 3/2020–3/2021 | Blood Donor HEV Samples ** | Blood Donor Anti-HEV IgG Samples ** |
|---|---|---|---|---|---|---|
| HYKS | 2,198,182 | 16 | 0.7 | 82,739 (37%) | 9138 (39%) | 386 (38%) |
| TYKS | 869,004 | 12 | 1.4 | 36,590 (17%) | 5762 (25%) | 186 (18%) |
| TAYS | 902,681 | 4 | 0.4 | 37,693 (17%) | 4304 (19%) | 268 (26%) |
| KYS | 797,234 | 3 | 0.4 | 25,389 (11%) | 3551 (15%) | 143 (14%) |
| OYS | 736,563 | 3 | 0.4 | 37,664 (17%) | 355 (2%) | 25 (2%) |
| Åland | 30,129 | 0 | 0 | 956 (0.4%) | 84 (0.4%) | 3 (0.3%) |
| Total | 5,533,793 | 38 | 0.7 | 221,031 | 23,199 | 1012 |
| Sample | Collection Time | HEV RNA (Procleix NAT) | HEV RNA (PCR) | Geno-Type | Serology | ||
|---|---|---|---|---|---|---|---|
| Interpretation | Signal Per Cut-Off | Anti-HEV IgG | Anti-HEV IgM | ||||
| HEV RNA-positive samples | |||||||
| 1 | July 2020 | RR | 11.66/10.42 | na | na | negative | negative |
| 2 | Aug 2020 | RR | 58.51/40.83 | positive | 3c | negative | negative |
| 3 | Sept 2020 | RR | 32.14/31.85 | positive | 3c | negative | negative |
| 4 | July 2020 | IR | 10.44/0.0 | positive | 3c | negative | negative |
| HEV RNA initially reactive samples | |||||||
| 5 | July 2020 | IR | 1.7/0.0/0.07 | negative | na | positive (2/3) | negative |
| 6 | July 2020 | IR | 8.44/0.0 | negative | na | negative | negative |
| 7 | July 2020 | IR | 2.32/0.0 | negative | na | negative | negative |
| 8 | July 2020 | IR | 1.99/0.0 | negative | na | negative | negative |
| 9 | Aug 2020 | IR | 6.99/0.03/0.0 | negative | na | negative | negative |
| 10 | Sept 2020 | IR | 1.76/0.0 | negative | na | negative | negative |
| 11 | Oct 2020 | IR | 2.09/0.0 | negative | na | negative | negative |
| 12 | Oct 2020 | IR | 1.64/0.0 | negative | na | negative | negative |
| 13 | Jan 2021 | IR | 1.14/0.14 | negative | na | negative | negative |
| 14 | Jan 2021 | IR | 1.16/0.06/0.0 | negative | na | negative | negative |
| 15 | Feb 2021 | IR | 3.88/0.0/0.0 | negative | na | negative | negative |
| 16 | Mar 2021 | IR | 1.67/0.08/0.0 | na | na | na | na |
| Age Group | Anti-HEV IgG: All | Anti-HEV IgG: Males | Anti-HEV IgG: Females | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n Total | n Positive | % Positive | 95% CI | n Total | n Positive | % Positive | n Total | n Positive | % Positive | |
| 18–29 | 170 | 7 | 4.1 | 1.7–8.3 | 61 | 2 | 3.3 | 109 | 5 | 4.6 |
| 30–39 | 146 | 12 | 8.2 | 4.3–13.9 | 59 | 7 | 11.9 | 87 | 5 | 5.7 |
| 40–49 | 197 | 8 | 4.1 | 1.8–7.8 | 97 | 4 | 4.1 | 100 | 4 | 4.0 |
| 50–59 | 244 | 22 | 9.0 | 5.7–13.3 | 139 | 12 | 8.6 | 105 | 10 | 9.5 |
| 60–70 | 255 | 26 | 10.2 | 6.8–14.6 | 115 | 11 | 9.6 | 140 | 15 | 10.7 |
| Total | 1012 | 75 | 7.4 | 5.9–9.2 | 471 | 36 | 7.6 | 541 | 39 | 7.2 |
| Region | Anti-HEV IgG | ||
|---|---|---|---|
| n Total | n Positive | % Positive (95% CI) | |
| HYKS | 386 | 24 | 6.2 (4.0–9.1) |
| TYKS | 268 | 26 | 9.7 (6.4–13.9) |
| TAYS | 186 | 15 | 8.1 (4.6–12.9) |
| KYS | 143 | 9 | 6.3 (2.9–11.6) |
| OYS | 25 | 1 | 4.0 (0.1–20.3) |
| Åland | 3 | 0 | 0.0 |
| Total | 1012 * | 75 | 7.4 (5.9–9.2) |
| Blood Component | Risk of One Adverse Event Per x Component Transfused (95% CI) | |||
|---|---|---|---|---|
| Red Cell Components | Platelets * | Total n (95% CI) | ||
| Number of components issued in Finland 2020 | 179,387 | 31,381 | 210,768 | |
| Number (proportion) transfused | 177,593 (99%) | 28,243 (90%) | 205,836 | |
| A. Risk of viremia (1:5784 = 0.017% of donations; 95%CI 0.005–0.044%) in x components | 30.7 | 4.9 | 35.6 (9.7–91.2) | |
| B. Number of transmissions resulting in infection; estimated 42% of viremic products (0.42 * A) | 12.9 | 2.1 | 14.9 (4.1–38.3) | 1:13,772 (1:50,204–1:5375) |
| C. Number of symptomatic infections = 5% (0.05 * B) | 0.6 | 0.1 | 0.7 (0.2–1.9) | 1:275,440 (1:1,013,171–1:107,492) |
| D. Number of severe infections = 1% (0.01 * B) | 0.13 | 0.02 | 0.15 (0.04–0.38) | 1: 1,377,202 (1:5,065,856–1:537,461) |
| Risk of one symptomatic infection in x years ** | 1 in 1 year (95% CI 1 in 5 years to 1 in 0.5 years) | |||
| Risk of one severe infection in x years ** | 1 in 7 years (95% CI 1 in 25 years to 1 in 3 years) | |||
| Country | Blood Donor Screening | HEV IgG Seroprevalence, % | HEV RNA Positivity Rate (%) | References |
|---|---|---|---|---|
| Finland | No | 7.4 | 1:5784 (0.017) | This study |
| Austria | No | 13.6 | 1:8416 (0.012) | [37] |
| Belgium | No | 8.7 | 1:5448 (0.018) | [36] |
| Bulgaria | No | 25.9 | na | [44] |
| Croatia | No | 21.5 | na | [45] |
| Denmark | No | 19.8 | 1:2330 (0.043) | [25,46] |
| France | Yes | 22.4 | 1:2218 (0.045) | [21,47] |
| Germany | Yes | 29.5 | 1:1268 (0.079); 1:597 (0.17) * | [20,48] |
| Ireland | Yes | 5.3 | 1:4997 (0.02) | [19] |
| Italy | No | 8.7 | 0; 1:157 ** | [49,50] |
| Netherlands | Yes | 26.7 | 1:762 (0.13) | [51,52] |
| Poland | No | 43.5 | 1:2109 (0.047) | [53] |
| Spain | Yes *** | 20.0 | 1:4341 (0.023); 1:3333 (0.030) | [24,54] |
| Sweden | No | 17.0 | 1:7986 (0.01) | [55,56] |
| Switzerland | Yes | 20.4 | na | [23] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mättö, J.; Putkuri, N.; Rimhanen-Finne, R.; Laurila, P.; Clancy, J.; Ihalainen, J.; Ekblom-Kullberg, S. Hepatitis E Virus in Finland: Epidemiology and Risk in Blood Donors and in the General Population. Pathogens 2023, 12, 484. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens12030484
Mättö J, Putkuri N, Rimhanen-Finne R, Laurila P, Clancy J, Ihalainen J, Ekblom-Kullberg S. Hepatitis E Virus in Finland: Epidemiology and Risk in Blood Donors and in the General Population. Pathogens. 2023; 12(3):484. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens12030484
Chicago/Turabian StyleMättö, Jaana, Niina Putkuri, Ruska Rimhanen-Finne, Päivi Laurila, Jonna Clancy, Jarkko Ihalainen, and Susanne Ekblom-Kullberg. 2023. "Hepatitis E Virus in Finland: Epidemiology and Risk in Blood Donors and in the General Population" Pathogens 12, no. 3: 484. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens12030484