
Growth of Gram-Negative Bacteria in Antiseptics, Disinfectants and Hand Hygiene Products in Two Tertiary Care Hospitals in West Africa—A Cross-Sectional Survey

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Definitions of Terms Used in This Study
2.2. Study Design, Setting and Period
2.3. Ward and Pharmacy Visits, Actual Use and Life Cycle of the Products
2.4. Sampling and Transportation to the Laboratory
2.5. Culture Media Inoculation
2.6. Total Colony Count
2.7. Identification and Antimicrobial Susceptibility Testing of Bacterial Isolates
2.8. Data Entry and Analysis
2.9. Additional Methods
3. Results
3.1. In-Use Products Assessed and Wards Visited, Actual Use of Products
3.2. Procurement, Preparation and Distribution of Products, Storage in the Wards
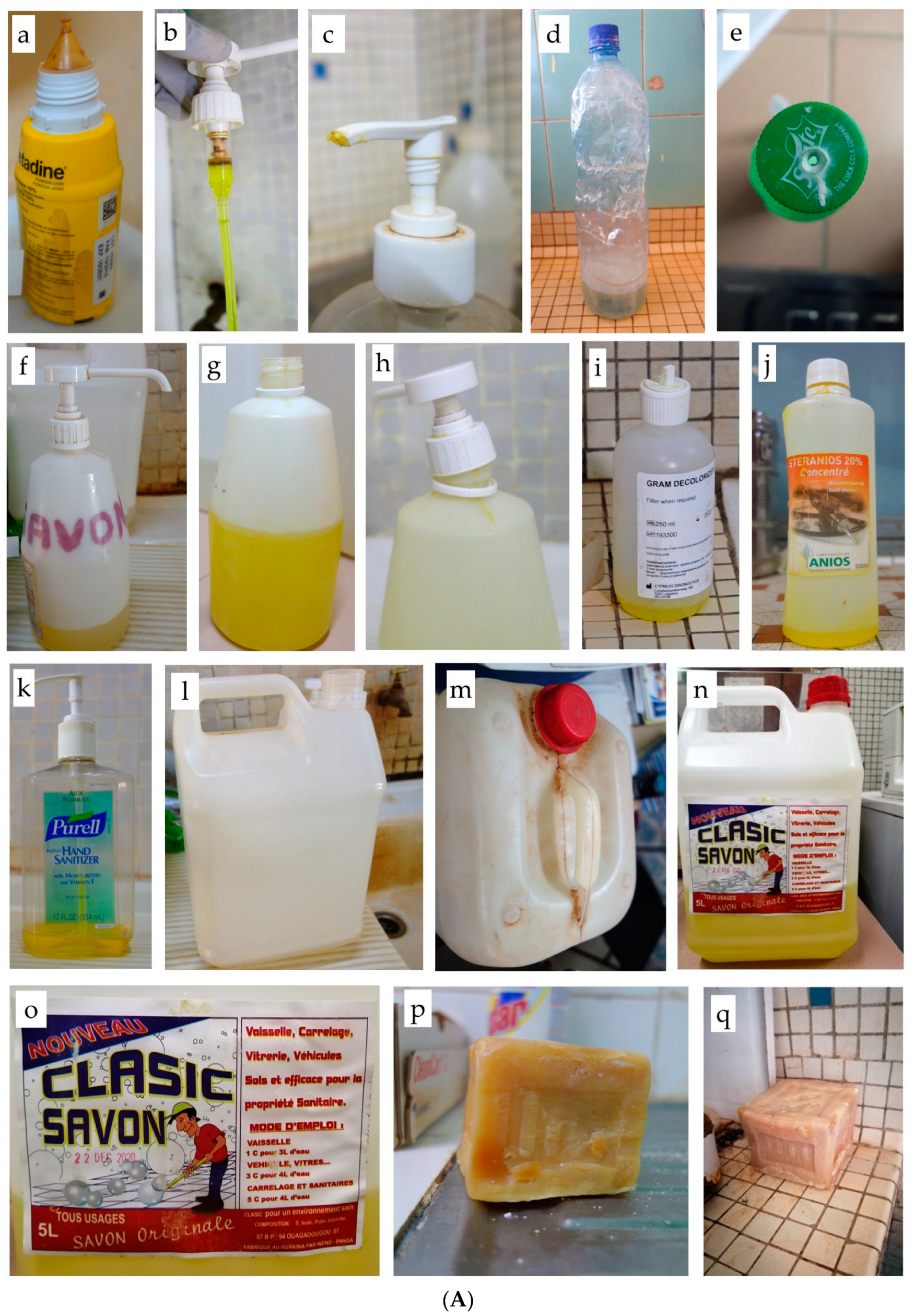
3.3. In-Use Containers: Type and Volumes, Status, Labeling, Practices of Reprocessing and Filling
3.4. Distribution, Stock and Sealed Containers
3.5. Procedures and Practices for In-Use Products
3.6. Growth of Gram-Negative Bacteria from In-Use Products, Association with Total Bacterial Counts
3.7. Growth of Gram-Negative Bacteria from Stock and Distribution Containers
3.8. Antimicrobial Resistance of Gram-Negative Bacterial Species
3.9. Additional Results
4. Discussion
4.1. Main Findings
4.2. Comparison with Previous Findings: Proportion among Products, Bacterial Species
4.3. Multidrug Resistance
4.4. Potential Causes Explaining for the High Proportion of Contaminated Products
4.4.1. Product-Related Factors: Ingredients, Manufacturing, In-Hospital Preparation
4.4.2. Containers
4.4.3. End-User Practices
4.4.4. Factors behind the Causes of Contamination
4.5. Limitations and Strengths
4.6. Relevance
4.7. Generalizability
4.8. Risk Mitigation, Outstanding Issues and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ABHR | Alcohol-based hand rub |
| AS | Antiseptics |
| CFU/ml | Colony forming units per ml |
| CHU-YO | Centre Hospitalier Universitaire Yalgado Ouédraogo |
| CLSI | Clinical and Laboratory Standards Institute |
| CNHU-HKM | Centre National Hospitalier Universitaire Hubert Koutoukou Maga |
| DI | Disinfectants |
| ESBL | Extended spectrum beta-lactamase |
| HAI | Healthcare associated infection |
| HH | Hand hygiene |
| IPC | Infection prevention and control |
| LMIC | Low- and middle-income countries |
| MALDI-TOF | Matrix Assisted Laser Desorption Ionization—Time of Flight |
| MDR | Multi-drug resistance |
| NDM | New Delhi metallo-beta-lactamase |
| NFGNB | Non-fermentative Gram-negative bacteria |
| PET | Polyethylene terephthalate |
| TSA | Tryptic soy agar |
| VIM | Verona Integron-encoded metallo-beta-lactamase |
References
- Jacobs, J.; Hardy, L.; Semret, M.; Lunguya, O.; Phe, T.; Affolabi, D.; Yansouni, C.; Vandenberg, O. Diagnostic Bacteriology in District Hospitals in Sub-Saharan Africa: At the Forefront of the Containment of Antimicrobial Resistance. Front. Med. 2019, 6, 205. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF) Progress on Wash in Health Care Facilities 2000–2021—Special Focus on WASH and Infection Prevention and Control (IPC). Available online: https://www.who.int/publications-detail-redirect/9789240058699 (accessed on 2 April 2023).
- World Health Organization (WHO). WHO Guideline on Hand Hygiene in Health Care—First Global Patient Safety Challenge Clean Care Is Safer Care. Available online: http://whqlibdoc.who.int/publications/2009/9789241597906_eng.pdf (accessed on 28 April 2023).
- Dias, V.M.C.H.; da Silva, D.M.W.; Burger, M.; de Iliveira, A.A.S.; de Capelo, P.J.; Al, E. Active Surveillance of Carbapenemresistant Gram-Negative Healthcare-Associated Infections in a Low-Middle-Income Country City. Braz. J. Infect. Dis. 2021, 25, 101540. [Google Scholar] [CrossRef]
- Rothe, C.; Schlaich, C.; Thompson, S. Healthcare-Associated Infections in Sub-Saharan Africa. J. Hosp. Infect. 2013, 85, 257–267. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Member States Information Session on Infection Prevention and Control (IPC). Available online: https://apps.who.int/iris/handle/10665/80135 (accessed on 28 August 2022).
- Kanamori, H.; Rutala, W.A.; Weber, D.J. The Role of Patient Care Items as a Fomite in Healthcare-Associated Outbreaks and Infection Prevention. Clin. Infect. Dis. 2017, 65, 1412–1419. [Google Scholar] [CrossRef]
- Lompo, P.; Heroes, A.-S.; Agbobli, E.; Kühne, V.; Tinto, H.; Affolabi, D.; Jacobs, J. Bacterial Contamination of Antiseptics, Disinfectants and Products Used for Hand Hygiene in Healthcare Facilities in High-Income Countries: A Scoping Review. Hygienes 2023, 3, 136–175. [Google Scholar] [CrossRef]
- Lompo, P.; Agbobli, E.; Heroes, A.-S.; vanden Poel, B.; Kühne, V.; Kpossou, G.; Zida, A.; Halidou, T.; Dissou, A.; Jacobs, J. Bacterial Contamination of Antiseptics, Disinfectants and Hand Hygiene Products Used in Healthcare Settings in Low- and Middle Income Countries—A Systematic Review. Hygienes 2023, 3, 93–124. [Google Scholar] [CrossRef]
- Chapman, P.; Forde, B.M.; Roberts, L.W.; Bergh, H.; Vesey, D.; Jennison, A.V.; Moss, S.; Paterson, D.L.; Beatson, S.A.; Harris, P.N.A. Genomic Investigation Reveals Contaminated Detergent as the Source of an Extended-Spectrum-β-Lactamase-Producing Klebsiella michiganensis Outbreak in a Neonatal Unit. J. Clin. Microbiol. 2020, 58, e01980-19. [Google Scholar] [CrossRef]
- Dancer, S.J. Mopping up Hospital Infection. J. Hosp. Infect. 1999, 43, 85–100. [Google Scholar] [CrossRef] [Green Version]
- Rutala, W.A.; Weber, D.J. Disinfection and Sterilization in Health Care Facilities: An Overview and Current Issues. Clin. Infect. Dis. 2004, 39, 702–709. [Google Scholar] [CrossRef] [Green Version]
- Weber, D.J.; Rutala, W.A.; Sickbert-Bennett, E.E. Outbreaks Associated with Contaminated Antiseptics and Disinfectants. Antimicrob. Agents Chemother. 2007, 51, 4217–4224. [Google Scholar] [CrossRef] [Green Version]
- Weber, D.J.; Sickbert-Bennett, E.E.; Kanamori, H.; Rutala, W.A. New and Emerging Infectious Diseases (Ebola, Middle Eastern Respiratory Syndrome Coronavirus, Carbapenem-Resistant Enterobacteriaceae, Candida auris): Focus on Environmental Survival and Germicide Susceptibility. Am. J. Infect. Control 2019, 47, A29–A38. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Minimum Requirements for Infection Prevention and Control Programmes. Available online: https://www.who.int/publications-detail-redirect/9789241516945 (accessed on 28 April 2023).
- World Health Organization (WHO). Guidelines on Core Components of Infection Prevention and Control Programmes at the National and Acute Health Care Facility Level. Available online: https://www.who.int/teams/integrated-health-services/infection-prevention-control/core-components (accessed on 28 April 2023).
- World Bank. World Bank Country Classifications by Income Level. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 28 April 2023).
- Craven, D.E.; Moody, B.; Connoly, M.G.; Kollisch, N.R.; Stottmeier, K.D.; McCabe, W.R. Pseudobacteriemia Caused by Providone-Iodine Solution Contaminated by Pseudomonas cepacia. N. Engl. J. Med. 1981, 305, 621–623. [Google Scholar] [CrossRef]
- Kampf, G.; Degenhardt, S.; Lackner, S.; Jesse, K.; von Baum, H.; Kampf, G.; McDonald, C.O.C. Poorly Processed Reusable Surface Disinfection Tissue Dispensers May Be a Source of Infection. BMC Infect. Dis. 2014, 14, 37. [Google Scholar] [CrossRef] [Green Version]
- Assadian, O.; Kramer, A.; Christiansen, B.; Exner, M.; Martiny, H.; Sorger, A.; Suchomel, M. Recommendations and Requirements for Soap and Hand Rub Dispensers in Healthcare Facilities. GMS Krankenhhyg. Interdiszip. 2012, 7, Doc03. [Google Scholar] [CrossRef]
- Tomasienwicz, D.M.; Hotchkiss, D.K.; Reinbold, G.W.; Read, R.B.; Hartman, P.A. The Most Suitable Number of Colonies on Plates for Counting. J. Food Prot. 1980, 43, 282–286. [Google Scholar] [CrossRef]
- U.S. Food & Drug Administration, (FDA). BAM Chapter 3: Aerobic Plate Count. Available online: https://www.fda.gov/food/laboratory-methods-food/bam-chapter-3-aerobic-plate-count (accessed on 27 April 2023).
- Denis, F.; Ploy, M.-C.; Martin, C.; Cattoir, V. Acinetobacter. In Bactériologie Médicale—Techniques Usuelles; Elsevier: Amsterdam, The Netherlands, 2016; pp. 346–348. [Google Scholar]
- Clinical and Laboratory Standards Institute (CLSI). M100, 33rd ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2023; Available online: http://em100.edaptivedocs.net/GetDoc.aspx?doc=CLSI%20M100%20ED33:2023&scope=user (accessed on 28 April 2023).
- Clinical and Laboratory Standards Institute (CLSI). Methods for Antimicrobial Dilution and Disk Susceptibility Testing of Infrequently Isolated or Fastidious Bacteria, 3rd ed.; CLSI Guideline M45; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2016; Available online: http://em100.edaptivedocs.net/dashboard.aspx (accessed on 28 April 2023).
- Clinical and Laboratory Standards Institute (CLSI). Analysis and Presentation of Cumulative Antimicrobial Susceptibility Test Data, 5th ed.; M39; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2022; Available online: https://infostore.saiglobal.com/en-us/standards/clsi-m39-ed5-2022-1299841_saig_clsi_clsi_3143074/ (accessed on 6 October 2022).
- European Committee on Antimicrobial Susceptibility Testing, (EUCAST). Expected Resistant Phenotypes; EUCAST: Växjö, Sweden, 2023. [Google Scholar]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-Resistant, Extensively Drug-Resistant and Pandrug-Resistant Bacteria: An International Expert Proposal for Interim Standard Definitions for Acquired Resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [Green Version]
- Stone, S.P.; Cooper, B.S.; Kibbler, C.C.; Cookson, B.D.; Roberts, J.A.; Medley, G.F.; Duckworth, G.; Lai, R.; Ebrahim, S.; Brown, E.M.; et al. The ORION Statement: Guidelines for Transparent Reporting of Outbreak Reports and Intervention Studies of Nosocomial Infection. Lancet Infect. Dis. 2007, 7, 282–288. [Google Scholar] [CrossRef]
- Turner, P.; Fox-Lewis, A.; Shrestha, P.; Dance, D.A.B.; Wangrangsimakul, T.; Cusack, T.P.; Ling, C.L.; Hopkins, J.; Roberts, T.; Limmathurotsakul, D.; et al. Microbiology Investigation Criteria for Reporting Objectively (MICRO): A Framework for the Reporting and Interpretation of Clinical Microbiology Data. BMC Med. 2019, 17, 70. [Google Scholar] [CrossRef] [Green Version]
- Archibald, L.K.; Shah, B.; Schulte, M.; Arduino, M.J.; Aguero, S.; Fisher, D.J.; Stechenberg, B.W.; Banerjee, S.N.; Jarvis, W.R. Serratia marcescens Outbreak Associated with Extrinsic Contamination of 1% Chlorxylenol Soap. Infect. Control Hosp. Epidemiol. 1997, 18, 704–709. [Google Scholar] [CrossRef]
- Buffet-Bataillon, S.; Rabier, V.; Bétrémieux, P.; Beuchée, A.; Bauer, M.; Pladys, P.; Le Gall, E.; Cormier, M.; Jolivet-Gougeon, A. Outbreak of Serratia marcescens in a Neonatal Intensive Care Unit: Contaminated Unmedicated Liquid Soap and Risk Factors. J. Hosp. Infect. 2009, 72, 17–22. [Google Scholar] [CrossRef]
- Villari, P.; Crispino, M.; Salvadori, A.; Scarcella, A. Molecular Epidemiology of an Outbreak of Serratia marcescens in a Neonatal Intensive Care Unit. Infect. Control Hosp. Epidemiol. 2001, 22, 630–634. [Google Scholar] [CrossRef]
- Fanci, R.; Bartolozzi, B.; Sergi, S.; Casalone, E.; Pecile, P.; Cecconi, D.; Mannino, R.; Donnarumma, F.; Leon, A.G.; Guidi, S.; et al. Molecular Epidemiological Investigation of an Outbreak of Pseudomonas aeruginosa Infection in an SCT Unit. Bone Marrow Transplant. 2009, 43, 335–338. [Google Scholar] [CrossRef] [Green Version]
- Grohskopf, L.; Roth, V.; Feikin, D.; Arduino, M.; Carson, L.; JI, T.; Holt, S.; Jensen, B.; Hoffman, R.; Jarvis, W. Serratia liquefaciens Bloodstream Infections from Contamination of Epoetin Alfa at a Hemodialysis Center. N. Engl. J. Med. 2001, 344, 1491–1497. [Google Scholar] [CrossRef]
- Lanini, S.; D’Arezzo, S.; Puro, V.; Martini, L.; Imperi, F.; Piselli, P.; Montanaro, M.; Paoletti, S.; Visca, P.; Ippolito, G. Molecular Epidemiology of a Pseudomonas aeruginosa Hospital Outbreak Driven by a Contaminated Disinfectant-Soap Dispenser. PLoS ONE 2011, 6, e17064. [Google Scholar] [CrossRef]
- Oie, S.; Arakawa, J.; Furukawa, H.; Matsumoto, S.; Matsuda, N.; Wakamatsu, H. Microbial Contamination of a Disinfectant-Soaked Unwoven Cleaning Cloth. J. Hosp. Infect. 2012, 82, 61–63. [Google Scholar] [CrossRef]
- Rabier, V.; Bataillon, S.; Jolivet-Gougeon, A.; Chapplain, J.M.; Beuchée, A.; Bétrémieux, P. Hand Washing Soap as a Source of Neonatal Serratia marcescens Outbreak. Acta Paediatr. Int. J. Paediatr. 2008, 97, 1381–1385. [Google Scholar] [CrossRef]
- Sartor, C.; Jacomo, V.; Duvivier, C.; Tissot-Dupont, H.; Sambbuc, R.; Drancourt, M. Nosocomial Serratia marcescens Infections Associated with Extrinsic Contamination of a Liquid Nonmedicated Soap. Infect. Control Hosp. Epidemiol. 2000, 21, 196–199. [Google Scholar] [CrossRef]
- Süer, K.; Meryem, G.; Otlu, B.; Tunç, E. Outbreak of Burkholderia Cepacia Complex Associated with Contaminated Liquid Soap for Hospital Use: A Case Study. Afr. J. Microbiol. Res. 2016, 10, 791–795. [Google Scholar] [CrossRef]
- Takahashi, H.; Kramer, M.H.; Yasui, Y.; Fujii, H.; Nakase, K.; Ikeda, K.; Imai, T.; Okazawa, A.; Tanaka, T.; Ohyanna, T.; et al. Nosocomial Serratia marcescens Outbreak in Osaka, Japan, From 1999 to 2000. Infect. Control Hosp. Epidemiol. 2004, 25, 156–161. [Google Scholar] [CrossRef]
- Ben Saida, N.; Marzouk, M.; Ferjeni, A.; Boukadida, J. A Three-Year Surveillance of Nosocomial Infections by Methicillin-Resistant Staphylococcus haemolyticus in Newborns Reveals the Disinfectant as a Possible Reservoir. Pathol. Biol. 2009, 57, 29–36. [Google Scholar] [CrossRef]
- Khanna, A.; Khanna, M.; Aggarwal, A. Serratia marcescens—A Rare Opportunistic Nosocomial Pathogen and Measures to Limit Its Spread in Hospitalized Patients. J. Clin. Diagn. Res. 2013, 7, 243–246. [Google Scholar] [CrossRef]
- Parasakthi, N.; Vadivelu, J.; Ariffin, H.; Iyer, L.; Palasubramaniam, S.; Arasu, A. Epidemiology and Molecular Characterization of Nosocomially Transmitted Multidrug-Resistant Klebsiella pneumoniae. Int. J. Infect. Dis. 2000, 4, 123–128. [Google Scholar] [CrossRef] [Green Version]
- Stoesser, N.; Sheppard, A.E.; Shakya, M.; Sthapit, B.; Thorson, S.; Giess, A.; Kelly, D.; Pollard, A.J.; Peto, T.E.A.; Walker, A.S.; et al. Dynamics of MDR Enterobacter Cloacae Outbreaks in a Neonatal Unit in Nepal: Insights Using Wider Sampling Frames and next-Generation Sequencing. J. Antimicrob. Chemother. 2015, 70, 1008–1015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aktas, E.; Taspinar, E.; Alay, D.; Ögedey, E.D.K.; Külah, C.; Comert, F. Extrinsic Contamination of Liquid Soap with Various Gram-Negative Bacteria in a Hospital in Turkey. Infect. Control Hosp. Epidemiol. 2010, 31, 1199–1201. [Google Scholar] [CrossRef] [Green Version]
- Altaher, A.M.; Ghafoor, E.S.A.; Amudi, W.I.; Alderby, D.K. Comparative Identification of Bacterial Quality in Liquid Soap between Nasser and European Gaza Hospitals, Khanyounis Governorate. Asian J. Pharm. Nurs. Med. Sci. 2016, 4, 77–83. [Google Scholar]
- Biswal, M.; Prasad, A.; Dhaliwal, N.; Gupta, A.K.; Taneja, N. Increase in Hospital Purchase of Hand Hygiene Products: The Importance of Focusing on the Right Product. Am. J. Infect. Control 2015, 43, 765–766. [Google Scholar] [CrossRef] [PubMed]
- Salama, A.S.A. Microbiological Quality of Soaps and Efficacy of Antiseptics and Disinfectants Used in Hospitals in Gaza—Palestine. Master’s Thesis, Islamic University Gaza, Gaza, Palestine, 2016. [Google Scholar]
- Subbannayya, K.; Bhat, G.K.; Junu, V.G.; Shetty, S.; Jisho, M.G. Can Soaps Act as Fomites in Hospitals? J. Hosp. Infect. 2006, 62, 243–245. [Google Scholar] [CrossRef]
- Zeiny, S.M.H. Isolation of Some Microorganisms from Bar Soaps and Liquid Soaps in Hospital Environments. Iraqi. J. Pharm. Sci. 2009, 18, 28–32. [Google Scholar]
- Eiref, S.D.; Leitman, I.M.; Riley, W. Hand Sanitizer Dispensers and Associated Hospital-Acquired Infections: Friend or Fomite? Surg. Infect. 2012, 13, 137–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espinosa de los Monteros, L.E.; Silva-Sanchez, J.; Jiménez, L.V.; Rojas, T.; Garza-Ramos, U.; Valverde, V. Outbreak of Infection by Extended-Spectrum Beta-Lactamase SHV-5-Producing Serratia marcescens in a Mexican Hospital. J. Chemother. 2008, 20, 586–592. [Google Scholar] [CrossRef]
- Barry, M.A.; Craven, D.E.; Goularte, T.A.; Lichtenberg, D.A. Serratia marcescens Contamination of Antiseptic Soap Containing Triclosan: Implications for Nosocomial Infection. Infect. Control 1984, 5, 427–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarvis, J.D.; Wynne, C.D.; Enwright, L.; Williams, J.D. Handwashing and Antiseptic-Containing Hospital Soaps In. J. Clin. Pathol. 1979, 32, 732–737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McBride, M.E. Microbial Flora of In-Use Soap Products. Appl. Environ. Microbiol. 1984, 48, 338–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolan, S.A.; Littlehorn, C.; Glodé, M.P.; Dowell, E.; Xavier, K.; Nyquist, A.-C.; Todd, J.K. Association of Bacillus cereus Infection with Contaminated Alcohol Prep Pads. Infect. Control Hosp. Epidemiol. 2012, 33, 666–671. [Google Scholar] [CrossRef]
- Steinhauer, K.; Meyer, B.; Ostermeyer, C.; Rödger, H.-J.; Hintzpeter, M. Hygienic Safety of Alcohol-Based Hand Disinfectants and Skin Antiseptics. GMS Hyg. Infect. Control 2013, 8, Doc19. [Google Scholar] [CrossRef] [PubMed]
- Cisse, M.F.; Samb, A.; Mboup, S.; Gaye, A.; David, M.P.; Sow, H.D.; Sanokho, A. On a Nosocomial Transmission of Enterobacter cloacae in a Tropical Area Children Hospital. Méd. Mal. Infect. 1987, 5, 260–263. [Google Scholar] [CrossRef]
- Pinna, A.; Usai, D.; Sechi, L.A.; Zanetti, S.; Jesudasan, N.C.A.; Thomas, P.A.; Kaliamurthy, J. An Outbreak of Post-Cataract Surgery Endophthalmitis Caused by Pseudomonas aeruginosa. Ophthalmology 2009, 116, 2321–2326. [Google Scholar] [CrossRef]
- World Health Organization, (WHO). Prioritization of Pathogens to Guide Discovery, Research and Development of New Antibiotics for Drug-Resistant Bacterial Infections, Including Tuberculosis; WHO: Geneva, Switzerland, 2017; ISBN 978-92-4-002642-1.
- Ombelet, S.; Kpossou, G.; Kotchare, C.; Agbobli, E.; Sogbo, F.; Massou, F.; Lagrou, K.; Barbé, B.; Affolabi, D.; Jacobs, J. Blood Culture Surveillance in a Secondary Care Hospital in Benin: Epidemiology of Bloodstream Infection Pathogens and Antimicrobial Resistance. BMC Infect. Dis. 2022, 22, 119. [Google Scholar] [CrossRef]
- Kadri, S.S.; Adjemian, J.; Lai, Y.L.; Spaulding, A.B.; Ricotta, E.; Rebecca Prevots, D.; Palmore, T.N.; Rhee, C.; Klompas, M.; Dekker, J.P.; et al. Difficult-to-Treat Resistance in Gram-Negative Bacteremia at 173 US Hospitals: Retrospective Cohort Analysis of Prevalence, Predictors, and Outcome of Resistance to All First-Line Agents. Clin. Infect. Dis. 2018, 67, 1803–1814. [Google Scholar] [CrossRef] [Green Version]
- Yusuf, E.; Bax, H.I.; Verkaik, N.J.; van Westreenen, M. An Update on Eight “New” Antibiotics against Multidrug-Resistant Gram-Negative Bacteria. J. Clin. Med. 2021, 10, 1068. [Google Scholar] [CrossRef]
- Liu, S.; Xu, H.; Guo, X.; Li, S.; Wang, Q.; Li, Y.; Liu, R.; Gou, J. Emergence and Genetic Characterization of Plasmid-Encoded VIM-2-Producing Pseudomonas stutzeri with Novel Integron In1998 Isolated from Cerebrospinal Fluid. Infect. Drug Resist. 2021, 14, 3415–3424. [Google Scholar] [CrossRef]
- Bauer-Savage, J.; Pittet, D.; Kim, E.; Allegranzi, B. Local Production of WHO-Recommended Alcohol-Based Handrubs: Feasibility, Advantages, Barriers and Costs. Bull. World Health Organ. 2013, 91, 963–969. [Google Scholar] [CrossRef]
- Kohan, C.; Ligi, C.; Dumigan, D.G.; Boyce, J.M. The Importance of Evaluating Product Dispensers When Selecting Alcohol-Based Handrubs. Am. J. Infect. Control 2002, 30, 373–375. [Google Scholar] [CrossRef]
- Chattman, M. Occurrence of Heterotrophic and Coliform Bacteria in Liquid Hand Soaps from Bulk Refillable Dispensers in Public Facilities. J. Environ. Health 2011, 73, 26–29. [Google Scholar] [PubMed]
- Momeni, S.S.; Tomlin, N.; Ruby, J.D. Isolation of Raoultella planticola from Refillable Antimicrobial Liquid Soap Dispensers in a Dental Setting. J. Am. Dent. Assoc. 2015, 146, 241–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gräf, W.; Kersch, D.; Scherzer, G. Microbial Contamination of Wall-Attached, One-Way Dispensers of Fluid Soaps. Zbl. Bakt. Hyg. 1988, 186, 166–179. [Google Scholar]
- Otter, J.A.; Vickery, K.; Walker, J.T.; deLancey Pulcini, E.; Stoodley, P.; Goldenberg, S.D.; Salkeld, J.A.G.; Chewins, J.; Yezli, S.; Edgeworth, J.D. Surface-Attached Cells, Biofilms and Biocide Susceptibility: Implications for Hospital Cleaning Anddisinfection. J. Hosp. Infect. 2015, 89, 16–27. [Google Scholar] [CrossRef] [Green Version]
- Afolabi, B.A.; Oduyebo, O.O.; Ogunsola, F.T. Bacterial Flora of Commonly Used Soaps in Three Hospitals in Nigeria. East Afr. Med. J. 2007, 84, 489–495. [Google Scholar] [CrossRef] [Green Version]
- Danchaivijitr, S.; Dhiraputra, C.; Rongrungruang, Y.; Srihapol, N.; Pumsuwan, V. Microbial contamination of antiseptics and disinfectants. Microb. Contam. Antiseptics Disinfect. 2005, 88 (Suppl. S1), S133–S139. [Google Scholar]
- Gajadhar, T.; Lara, A.; Sealy, P.; Adesiyun, A.A. Microbial Contamination of Disinfectants and Antiseptics in Four Major Hospitals in Trinidad. Rev. Panam. Salud Publica/Pan Am. J. Public Health 2003, 14, 193–200. [Google Scholar] [CrossRef] [Green Version]
- Allegranzi, B.; Nejad, S.B.; Combescure, C.; Graafmans, W.; Attar, H.; Donaldson, L.; Pittet, D. Burden of Endemic Health-Care-Associated Infection in Developing Countries: Systematic Review and Meta-Analysis. Lancet 2011, 377, 228–241. [Google Scholar] [CrossRef]
- McNaughton, M.; Mazinke, N.; Thomas, E. Newborn Conjuctivitis Associated with Triclosan 0.5% Antiseptic Intrinsically Contaminated with Serratia marcescens. Can. J. Infect. Control 1995, 10, 7–8. [Google Scholar]
- Zapka, C.A.; Campbell, E.J.; Maxwell, S.L.; Gerba, C.P.; Dolan, M.J.; Arbogast, J.W.; Macinga, D.R. Bacterial Hand Contamination and Transfer after Use of Contaminated Bulk-Soap-Refillable Dispensers. Appl. Environ. Microbiol. 2011, 77, 2898–2904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanc, D.S.; Gomes Magalhaes, B.; Abdelbary, M.; Prod’hom, G.; Greub, G.; Wasserfallen, J.B.; Genoud, P.; Zanetti, G.; Senn, L. Hand Soap Contamination by Pseudomonas aeruginosa in a Tertiary Care Hospital: No Evidence of Impact on Patients. J. Hosp. Infect. 2016, 93, 63–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mapping Antimicrobial Resistance and Antimicrobial Use Partnership Measure Levels of Antimicrobial Resistance (AMR) and Antimicrobial Use (AMU) Based on Existing, Historical, Records, Assess the Relationship between the Two and Provide Policy Recommendations to Strengthen AMR and Antimicrobial Consumption (AMC) Surveilla. Available online: https://aslm.org/what-we-do/maap/ (accessed on 27 November 2022).
- Centers for Disease Control and Prevention, (CDC). Guideline for Hand Hygiene in Health-Care Settings Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Morb. Mortal. Wkly. Rep. Recomm. 2002, 51. [Google Scholar]
- Schaffner, D.W.; Jensen, D.; Gerba, C.P.; Shumaker, D.; Arbogast, J.W. Influence of Soap Characteristics and Food Service Facility Type on the Degree of Bacterial Contamination of Open, Refillable Bulk Soaps. J. Food Prot. 2018, 81, 218–225. [Google Scholar] [CrossRef]
- Caetano, J.A.; Lima, M.A.; Miranda, M.D.C.; Serufo, J.C.; Ponte, P.R.L. Identification of Bacterial Contamination in Liquid Soap for Hospital Use. Rev. Esc. Enferm. 2011, 45, 148–155. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Products Collected per Hospital Ward | Ethanol 70% (AS) | Ethanol 70% (HH) | Povidone Iodine | Alcohol-Based Handrub | Chlorhexidine | Dakin | Iodine Tincture | Chlorine | QUAT | PAPB | Liquid Soap | Bar Soap | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CHU-YO | 31 (2) | 1 | 14 | 8 (1) | 1 | - | - | 10 (2) | 1 (1) | 1 | 37 (24) | 16 (4) | 120 (34) |
| Surgery a | 3 (1) | - | 2 | 1 (1) | - | - | - | 1 | - | - | 9 (4) | 5 (2) | 21 (8) |
| Internal medicine | 3 (1) | - | - | - | - | - | - | 1 | - | - | 6 (6) | 3 | 13 (7) |
| Maternity | 6 | 1 | 4 | 1 | - | - | - | - | - | - | 6 (4) | - | 18 (4) |
| Neonatology | 3 | - | 1 | 3 | - | - | - | 3 | 1 | 3 (1) | 3 (2) | 17 (3) | |
| Dialysis | 3 | - | - | - | - | - | - | - | 1 (1) | - | 4 (4) | 1 | 9 (5) |
| Pediatrics b | 7 | - | 3 | 2 | - | - | - | 5 (2) | - | - | 6 (5) | 3 | 26 (7) |
| Others c | 6 | - | 4 | 1 | 1 | - | - | - | - | - | 3 | 1 | 16 |
| CNHU-HKM | 18 | 30 | 19 | 3 | 2 (1) | 14 | 1 | 2 | 1 | - | 32 (27) | 1 | 123 (28) |
| Internal medicine | 3 | - | 8 | - | - | 1 | - | - | - | - | 1 (1) | 1 | 14 (1) |
| Maternity | 7 | 1 | 10 | 1 | 1 (1) | 4 | 1 | - | - | - | 7 (6) | - | 32 (7) |
| Neonatology | 4 | 29 | 1 | 2 | 1 | 2 | - | 2 | 1 | - | 16 (16) | - | 58 (16) |
| Pediatrics b | 4 | - | - | - | - | 7 | - | - | - | - | 8 (4) | - | 19 (4) |
| Total | 49 (2) | 31 | 33 | 11 (1) | 3 (1) | 14 | 1 | 12 (2) | 2 (1) | 1 | 69 (51) | 17 (4) | 243 (62) |
| In-Use Products | Used as | Samples | Containers | Procurement and Supply | ||||
|---|---|---|---|---|---|---|---|---|
| CHU-YO | CNHU-HKM | Total | Aliquoted | Original | ||||
| Antiseptics/disinfectants * | 67 (6) | 90 (1) | 157 (7) | 110 | 47 | |||
| Ethanol 70% | AS/DI /HH | 32 (2) | 48 | 80 (2) | 79 | 1 | CHU-YO: | prepared by the hospital pharmacy (n = 32) branded product (n = 1) |
| CNHU-HKM: | prepared by the hospital pharmacy (n = 48) | |||||||
| Povidone iodine 4% and 10% | AS | 14 | 19 | 33 | 1 | 32 | CHU-YO: | branded product (n = 13) aliquoted product, origin not traceable (n = 1) |
| CNHU-HKM: | branded product (n = 19) | |||||||
| Dakin | AS/DI | - | 14 | 14 | 14 | - | CNHU-HKM: | prepared by the hospital pharmacy (n = 14) |
| Chlorhexidine 4% | AS | 1 | 2 (1) | 3 (1) | 1 | 2 | CHU-YO: | branded product (n = 1) |
| CNHU-HKM: | branded product (n = 1) branded product aliquoted in the ward (n = 1) | |||||||
| Iodine tincture | AS | - | 1 | 1 | 1 | - | CNHU-HKM: | prepared by the hospital pharmacy (n = 1) |
| Chlorine 0.5% | DI | 10 (2) | 2 | 12 (2) | 10 | 2 | CHU-YO: | branded product (n = 2) prepared by the hospital pharmacy (n = 10) |
| CNHU-HKM: | prepared by the hospital pharmacy (n = 2) | |||||||
| QUAT | DI | 1 (1) | 1 | 2 (1) | 1 | 1 | CHU-YO: | branded product (n = 1) |
| CNHU-HKM: | branded product aliquoted in the ward (n = 1) | |||||||
| PAPB | DI | 1 | - | 1 | - | 1 | CHU-YO: | branded product, polyaminopropyl biguanide 0.36% (n = 1) |
| Alcohol-based hand rub | HH | 8 (1) | 3 | 11 (1) | 3 | 8 | CHU-YO: | branded products (n = 6) aliquoted products, origin not traceable (n = 3) |
| CNHU-HKM: | branded products (n = 2) aliquoted products, origin not traceable (n = 1) | |||||||
| Soap products | 53 (28) | 33 (27) | 86 (55) | 69 | - | |||
| Liquid soap * | HH | 37 (24) | 32 (27) | 69 (51) | 69 | - | CHU-YO: | branded products (5 L containers), stored and aliquoted in the ward (n = 37) |
| CNHU-HKM: | artisanal small scale manufactured by private person (20–25 L containers) (n = 32) | |||||||
| Bar soap | HH | 16 (4) | 1 | 17 (4) | NA | NA | CHU-YO: | branded products, household grade soap (n = 12) home-made product, no brand name (n = 4) |
| CNHU-HKM: | home-made product, no brand name (n = 1) | |||||||
| Total | 120 (34) | 123 (28) | 243 (62) | 179 | 47 | - | - | |
| Container Type | PET Bottle | Table-Top with Pump Dispenser | Container with Screw Cap/ Dropper Nozzle | Other |
|---|---|---|---|---|
| CHU-YO (n = 37) | ||||
| Numbers | 2 (1) | 26 (19) | 2 (0) | 7 (4) |
| Examples | Soft drink and water bottles | Original ABHR Original scrub | Original povidone iodine Original Dakin Cooper | 3 x wall-mounted pump dispensers 4 x screw-cap container, all recycled |
| Clean/Dirty | Clean: 0 (0) Dirty: 2 (1) | Clean: 2 (1) Dirty: 24 (18) | Clean: 1 (0) Dirty: 1 (0) | Clean: 0 (0) Dirty: 7 (4) |
| Other observations | All of table-top containers with pump dispensers were overused (scratched surfaces); dispensers were missing in four containers and the dispensers of three containers were broken. Both PET bottles were overused, one had a perforated screw cap. | |||
| CNHU-HKM (n = 32) | ||||
| Numbers | 12 (9) | 15 (13) | 4 (4) | Total: 1 (1) |
| Examples | Soft drink and water bottles | Original ABHR Original antiseptic soap | Original povidone iodine | Non-identifiable uncapped container |
| Clean/Dirty | Clean: 11 (8) Dirty: 1 (1) | Clean: 15 (13) Dirty: 0 (0) | Clean:3 (3) Dirty: 1 (1) | Clean: 0 (0) Dirty: 1 (1) |
| Other observations | All table-top containers with pump dispensers had an intact dispenser. They were in use very recently before sampling and were recycled containers of ABHR diffused hospital-wide as part of a hand hygiene project. The original labels were still in place. Six PET bottles had their screw cap intact, four had a perforated cap and two were uncapped. | |||
| Species | No. of Affected Samples | Associated Total Colony Count (CFU/mL) | Hospital Wards |
|---|---|---|---|
| Enterobacterales, Aeromonas/Vibrio non-cholerae (n = 14) | |||
| Enterobacter bugandensis | 1 | >10,000 | CNHU-HKM Neonatology |
| Enterobacter cloacae complex | 3 | >10,000 | CNHU-HKM Neonatology (n = 2) |
| CNHU-HKM Maternity (n = 1) | |||
| Klebsiella oxytoca | 1 | >10,000 | CHU-YO Surgery |
| Klebsiella pneumoniae | 5 | >10,000 | CNHU-HKM Neonatology (n = 4) |
| CNHU-HKM Maternity (n = 1) | |||
| Aeromonas caviae | 2 | >10,000 | CNHU-HKM Maternity |
| CHU-YO Pediatric ward | |||
| Vibrio alginolyticus | 2 | >10,000 | CHU-YO Internal Medicine |
| CNHU-HKM Neonatology | |||
| Non-fermentative Gram-negative bacteria (n = 74) | |||
| Pseudomonas aeruginosa | 14 | >10,000 | CHU-YO Pediatric ward (n = 1) |
| CHU-YO Nephrology-Dialysis (n = 3) | |||
| CHU-YO Surgery (n = 1) | |||
| CNHU-HKM Neonatology (n = 9) | |||
| Pseudomonas spp. a | 21 | >10,000 (n = 19) 1001–2500 (n = 2) | CHU-YO Nephrology-Dialysis (n = 2) |
| CHU-YO Internal medicine (n = 4) | |||
| CHU-YO Pediatric wards (n = 2) | |||
| CHU-YO Maternity (n = 1) | |||
| CNHU-HKM Neonatology (n = 6) | |||
| CNHU-HKM Pediatric ward (n = 2) | |||
| CNHU-HKM Maternity (n = 3) | |||
| CNHU-HKM Internal medicine (n = 1) | |||
| Acinetobacter spp. b | 6 | >10,000 (n = 4) 2501–10,000 (n = 2) | CHU-YO Maternity (n = 1) |
| CHU-YO Surgery (n = 3) | |||
| CNHU-HKM Neonatology (n = 1) | |||
| CNHU-HKM Maternity (n = 1) | |||
| Alcaligenes faecalis | 1 | >10,000 | CHU-YO Neonatology |
| Halomonas spp. | 1 | >10,000 | CNHU-HKM Maternity |
| Pannonibacter phragmitetus | 1 | >10,000 | CNHU-HKM Neonatology |
| Shewanella spp. c | 2 | >10,000 | CHU-YO Pediatric ward |
| Other Non-fermentative Gram-negative bacteria | 28 | >10,000 (n = 20) 2501–10,000 (n = 1) 501–1000 (n = 4) <250 (n = 3) | CHU-YO Pediatric ward (n = 5) |
| CHU-YO Internal medicine (n = 4) | |||
| CHU-YO Surgery (n = 2) | |||
| CHU-YO Maternity (n = 3) | |||
| CHU-YO Nephrology-Dialysis (n = 1) | |||
| CNHU-HKM Neonatology (n = 3) | |||
| CNHU-HKM Pediatric ward (n = 6) | |||
| CNHU-HKM Maternity (n = 4) | |||
| Affected Product | Gram-Negative Bacterial Species | Total Colony Count (CFU/mL) | Hospital Wards | Comment |
| Liquid products (n = 7) | ||||
| Non-fermentative Gram-negative bacteria (n = 11) | ||||
| Chlorhexidine (n = 1) | Achromobacter xylosoxidans | 2501–10,000 | CNHU-HKM Maternity | Recycled container with screw-cap/dropper nozzle |
| Ethanol (n = 2) | Pseudomonas putida group | 250–500 | CHU-YO Surgery | |
| Pseudomonas putida group | <250 | CHU-YO Internal medicine | Recycled ABHR table-top dispenser | |
| Chlorine (n = 2) | Acinetobacter baumannii | >10,000 | CHU-YO Pediatric ward | Washing basin with a lid |
| Delftia acidovorans | Washing basin, no lid | |||
| Pseudomonas stutzeri | ||||
| QUAT (n = 1) | Acinetobacter indicus | CHU-YO Dialysis | Original container | |
| Acinetobacter spp. | ||||
| ABHR (n = 1) | Pseudomonas aeruginosa | CHU-YO Surgery | Recycled container, no label, no concentration mentioned | |
| NFGNB | ||||
| Bar soap products (n = 4) | ||||
| Enterobacterales (n = 4) | ||||
| Enterobacter cloacae complex (n = 2) | >10,000 | CHU-YO Neonatology | 1 on the bench 1 in a perforated container | |
| Enterobacter bugandensis (n = 1) | CHU-YO Neonatology | No receptacle, put directly on the bench | ||
| Klebsiella oxytoca (n = 1) | CHU-YO Surgery | No receptacle, put directly on the bench | ||
| Non-fermentative Gram-negative bacteria (n = 3) | ||||
| Acinetobacter haemolyticus | >10,000 | CHU-YO Surgery | No receptacle, put directly on the bench | |
| Wautersiella falsenii | CHU-YO Neonatology | No receptacle, put directly on the bench | ||
| Ochrobactrum intermedium | <250 | CHU-YO Surgery | No receptacle, put directly on the bench | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lompo, P.; Heroes, A.-S.; Agbobli, E.; Kazienga, A.; Peeters, M.; Tinto, H.; Lagrou, K.; Sangaré, L.; Affolabi, D.; Jacobs, J. Growth of Gram-Negative Bacteria in Antiseptics, Disinfectants and Hand Hygiene Products in Two Tertiary Care Hospitals in West Africa—A Cross-Sectional Survey. Pathogens 2023, 12, 917. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens12070917
Lompo P, Heroes A-S, Agbobli E, Kazienga A, Peeters M, Tinto H, Lagrou K, Sangaré L, Affolabi D, Jacobs J. Growth of Gram-Negative Bacteria in Antiseptics, Disinfectants and Hand Hygiene Products in Two Tertiary Care Hospitals in West Africa—A Cross-Sectional Survey. Pathogens. 2023; 12(7):917. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens12070917
Chicago/Turabian StyleLompo, Palpouguini, Anne-Sophie Heroes, Esenam Agbobli, Adama Kazienga, Marjan Peeters, Halidou Tinto, Katrien Lagrou, Lassana Sangaré, Dissou Affolabi, and Jan Jacobs. 2023. "Growth of Gram-Negative Bacteria in Antiseptics, Disinfectants and Hand Hygiene Products in Two Tertiary Care Hospitals in West Africa—A Cross-Sectional Survey" Pathogens 12, no. 7: 917. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens12070917