Molecular Epidemiology of Rotavirus A Strains Pre- and Post-Vaccine (Rotarix®) Introduction in Mozambique, 2012–2019: Emergence of Genotypes G3P[4] and G3P[8]

 , , , , , , ,
, , , , , , ,  , and
, and
Abstract
:1. Introduction
2. Results
2.1. Comparison of Rotavirus G- and P-Types in Mozambique Pre- and Post-Vaccine Introduction
2.2. Comparison of G/P Genotype Combinations in Mozambique Pre- and Post-Vaccine Introduction
2.3. Yearly Distribution of Rotavirus Genotypes at the Mavalane General Hospital (HGM) and National Surveillance Sites
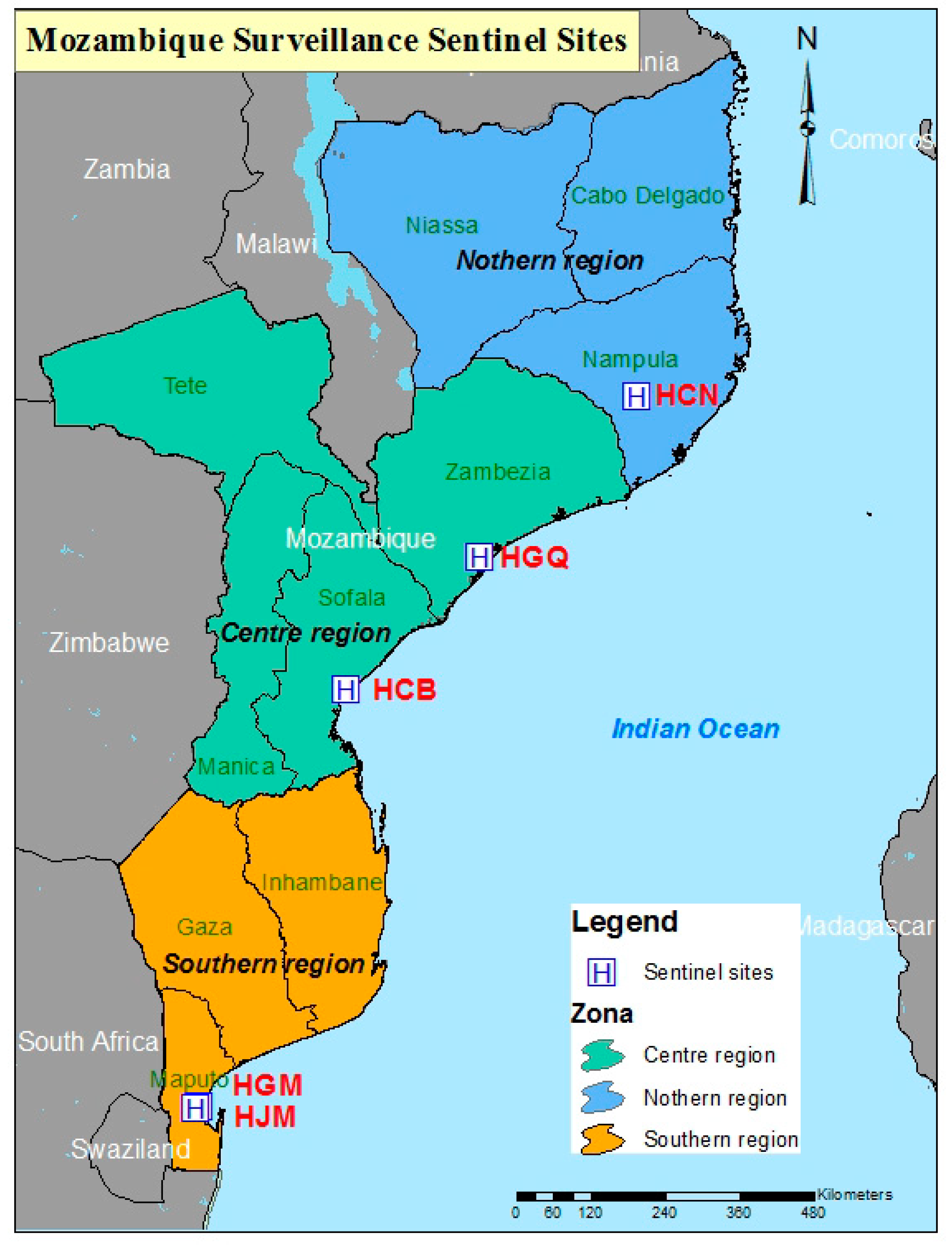
2.4. Geographical Distribution of Rotavirus Genotypes
3. Discussion
4. Materials and Methods
4.1. Study Population and Stool Samples Collection
4.2. Ethical Approval
4.3. Laboratory Testing
4.3.1. Rotavirus Detection and RNA Extraction
4.3.2. Reverse Transcriptase (RT) and G/P Typing PCR
4.4. Data Management and Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Troeger, C.; Khalil, I.A.; Rao, P.C.; Cao, S.; Blacker, B.F.; Ahmed, T.; Armah, G.; Bines, J.E.; Brewer, T.G.; Colombara, D.V.; et al. Rotavirus Vaccination and the Global Burden of Rotavirus Diarrhea Among Children Younger Than 5 Years. JAMA Pediatr. 2018, 172, 958–965. [Google Scholar] [CrossRef] [Green Version]
- Tate, J.E.; Burton, A.H.; Boschi-Pinto, C.; Parashar, U.D. Global, Regional, and National Estimates of Rotavirus Mortality in Children <5 Years of Age, 2000–2013. Clin. Infect. Dis. 2016, 62, S96–S105. [Google Scholar] [PubMed] [Green Version]
- GBD. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhoea in 195 countries: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1211–1228. [Google Scholar]
- Estes, M.K.; Cohen, J. Rotavirus gene structure and function. Microbiol. Rev. 1989, 53, 410–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crawford, S.E.; Ramani, S.; Tate, J.E.; Parashar, U.D.; Svensson, L.; Hagbom, M.; Francco, M.A.; Greenberg, H.B.; O’Ryan, M.; Kang, G.; et al. Rotavirus infection. Nat. Rev. Dis. Primers. 2017, 3, 17083. [Google Scholar] [CrossRef] [Green Version]
- Desselberger, U. Rotaviruses. Virus Res. 2014, 190, 75–96. [Google Scholar] [CrossRef] [Green Version]
- Matthijnssens, J.; Ciarlet, M.; McDonald, S.M.; Attoui, H.; Banyai, K.; Brister, J.R.; Buesa, J.; Esona, M.D.; Estes, M.K.; Gentsch, J.R.; et al. Uniformity of rotavirus strain nomenclature proposed by the Rotavirus Classification Working Group (RCWG). Arch. Virol. 2011, 156, 1397–1413. [Google Scholar] [CrossRef] [Green Version]
- Matthijnssens, J.; Ciarlet, M.; Heiman, E.; Arijs, I.; Delbeke, T.; McDonald, S.M.; Palombo, E.A.; Iturriza-Gómara, M.; Maes, P.; Patton, J.T.; et al. Full genome-based classification of rotaviruses reveals a common origin between human Wa-Like and porcine rotavirus strains and human DS-1-like and bovine rotavirus strains. J. Virol. 2008, 82, 3204–3219. [Google Scholar] [CrossRef] [Green Version]
- Virus Classification- Laboratory of Viral Metagenomics. Available online: https://rega.kuleuven.be/cev/viralmetagenomics/virus-classification/rcwg (accessed on 20 May 2020).
- Mwenda, J.M.; Tate, J.E.; Parashar, U.D.; Mihigo, R.; Agocs, M.; Serhan, F.; Nshimirimana, D. African rotavirus surveillance network: A brief overview. Pediatr. Infect. Dis. J. 2014, 33, S6–S8. [Google Scholar] [CrossRef]
- Banyai, K.; Laszlo, B.; Duque, J.; Steele, A.D.; Nelson, E.A.; Gentsch, J.R.; Parashar, U.D. Systematic review of regional and temporal trends in global rotavirus strain diversity in the pre rotavirus vaccine era: Insights for understanding the impact of rotavirus vaccination programs. Vaccine 2012, 30, A122–A130. [Google Scholar] [CrossRef]
- Gentsch, J.R.; Laird, A.R.; Bielfelt, B.; Griffin, D.D.; Banyai, K.; Ramachandran, M.; Jain, V.; Cunliffe, N.A.; Nakagomi, O.; Kirkwood, C.D.; et al. Serotype diversity and reassortment between human and animal rotavirus strains: Implications for rotavirus vaccine programs. J. Infect. Dis. 2005, 192, S146–S159. [Google Scholar] [CrossRef] [Green Version]
- Leshem, E.; Lopman, B.; Glass, R.; Gentsch, J.; Banyai, K.; Parashar, U.; Patel, M. Distribution of rotavirus strains and strain-specific effectiveness of the rotavirus vaccine after its introduction: A systematic review and meta-analysis. Lancet Infect. Dis. 2014, 14, 847–856. [Google Scholar] [CrossRef]
- Matthijnssens, J.; Bilcke, J.; Ciarlet, M.; Martella, V.; Banyai, K.; Rahman, M.; Zeller, M.; Beutels, P.; van Damme, P.; van Ranst, M. Rotavirus disease and vaccination: Impact on genotype diversity. Fut. Microbiol. 2009, 4, 1303–1316. [Google Scholar] [CrossRef]
- Todd, S.; Page, N.A.; Duncan Steele, A.; Peenze, I.; Cunliffe, N.A. Rotavirus strain types circulating in Africa: Review of studies published during 1997–2006. J. Infect. Dis. 2010, 202, S34–S42. [Google Scholar] [CrossRef] [Green Version]
- Seheri, L.M.; Magagula, N.B.; Peenze, I.; Rakau, K.; Ndadza, A.; Mwenda, J.M.; Weldegebriel, G.; Steele, A.D.; Mphahlele, M.J. Rotavirus strain diversity in Eastern and Southern African countries before and after vaccine introduction. Vaccine 2017, 36, 7222–7230. [Google Scholar] [CrossRef] [PubMed]
- Rotavirus vaccines. WHO position paper—January 2013. Wkly. Epidemiol. Rec. 2013, 88, 49–64. [Google Scholar]
- Langa, J.S.; Thompson, R.; Arnaldo, P.; Resque, H.R.; Rose, T.; Enosse, S.M.; Fialho, A.; Assis, R.M.S.; Silva, M.F.M.; Paulo, J.; et al. Epidemiology of Rotavirus A diarrhea in Chókwè, Southern Mozambique, from February to September, 2011. J. Med. Virol. 2016, 88, 1751–1758. [Google Scholar] [CrossRef]
- De Deus, N.; João, E.; Cuamba, A.; Cassocera, M.; Luís, L.; Acácio, S.; Mandomando, I.; Augusto, O.; Page, N. Epidemiology of Rotavirus Infection in Children from a Rural and Urban Area, in Maputo, Southern Mozambique, before Vaccine Introduction. J. Trop. Pediatr. 2018, 64, 141–145. [Google Scholar] [CrossRef]
- Kotloff, K.L.; Nataro, J.P.; Blackwelder, W.C.; Nasrin, D.; Farag, T.H.; Panchalingam, S.; Wu, Y.; O Sow, S.; Sur, D.; Breiman, R.F.; et al. Burden and aetiology of diarrhoeal disease in infants and young children in developing countries (the Global Enteric Multicenter Study, GEMS): A prospective, case-control study. Lancet 2013, 382, 209–222. [Google Scholar] [CrossRef]
- De Deus, N.; Chilaule, J.J.; Cassocera, M.; Bambo, M.; Langa, J.S.; Sitoe, E.; Chissaque, A.; Anapakala, E.; Sambo, J.; Lourenço Guimarães, E.; et al. Early impact of rotavirus vaccination in children less than five years of age in Mozambique. Vaccine 2018, 36, 7205–7209. [Google Scholar] [CrossRef]
- Matthijnssens, J.; de Grazia, S.; Piessens, J.; Heylen, E.; Zeller, M.; Giammanco, G.M.; Bányai, K.; Buonavoglia, C.; Ciarlet, M.; Martella, V.; et al. Multiple reassortment and interspecies transmission events contribute to the diversity of feline, canine and feline/canine-like human group A rotavirus strains. Infect. Genet. Evol. 2011, 11, 1396–1406. [Google Scholar] [CrossRef]
- Matthijnssens, J.; Taraporewala, Z.F.; Yang, H.; Rao, S.; Yuan, L.; Cao, D.; Hoshino, Y.; Mertens, P.P.C.; Carner, G.R.; McNeal, M.; et al. Simian rotaviruses possess divergent gene constellations that originated from interspecies transmission and reassortment. J. Virol. 2009, 84, 2013–2026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joao, E.D.; Strydom, A.; O’Neill, H.G.; Cuamba, A.; Cassocera, M.; Acacio, S.; Mandomando, I.; Motanyane, L.; Page, N.; de Deus, N. Rotavirus A strains obtained from children with acute gastroenteritis in Mozambique, 2012–2013: G and P genotypes and phylogenetic analysis of VP7 and partial VP4 genes. Arch. Virol. 2018, 163, 153–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, N.A.; Seheri, L.M.; Groome, M.J.; Moyes, J.; Walaza, S.; Mphahlele, J.; Kahn, K.; Kapongo, C.N.; Zar, H.J.; Tempia, S.; et al. Temporal association of rotavirus vaccination and genotype circulation in South Africa: Observations from 2002 to 2014. Vaccine 2017, 36, 7231–7237. [Google Scholar] [CrossRef]
- Lartey, B.L.; Damanka, S.; Dennis, F.E.; Enweronu-Laryea, C.C.; Addo-Yobo, E.; Ansong, D.; Kwarteng-Owusu, S.; Sagoe, K.W.; Mwenda, J.M.; Diamenu, S.K.; et al. Rotavirus strain distribution in Ghana pre- and post- rotavirus vaccine introduction. Vaccine 2018, 36, 7238–7242. [Google Scholar] [CrossRef]
- Bar-Zeev, N.; Jere, K.C.; Bennett, A.; Pollock, L.; Tate, J.E.; Nakagomi, O.; Iturriza-Gomara, M.; Costello, A.; Mwansambo, C.; Parashar, U.D.; et al. Population Impact and Effectiveness of Monovalent Rotavirus Vaccination in Urban Malawian Children 3 Years After Vaccine Introduction: Ecological and Case-Control Analyses. Clin. Infect. Dis. 2016, 62, S213–S219. [Google Scholar] [CrossRef]
- Hungerford, D.; Allen, D.J.; Nawaz, S.; Collins, S.; Ladhani, S.; Vivancos, R.; Iturriza-Gómara, M. Impact of rotavirus vaccination on rotavirus genotype distribution and diversity in England, September 2006 to August 2016. Eurosurveillance 2019, 24, 1700774. [Google Scholar]
- Matthijnssens, J.; Zeller, M.; Heylen, E.; de Coster, S.; Vercauteren, J.; Braeckman, T.; van Herck, K.; Meyer, N.; Pircon, J.-Y.; Soriano-Gabarro, M.; et al. Higher proportion of G2P[4] rotaviruses in vaccinated hospitalized cases compared with unvaccinated hospitalized cases, despite high vaccine effectiveness against heterotypic G2P[4] rotaviruses. Clin. Microbiol. Infect. 2014, 20, O702–O710. [Google Scholar] [CrossRef] [Green Version]
- Luchs, A.; Cilli, A.; Morillo, S.G.; de Cássia Compagnoli, C.R.; Timenetsky, M.C.S.T. Rotavirus Genotypes Circulating in Brazil, 2007-2012: Implications for the Vaccine Program. Rev. Inst. Med. Trop. 2015, 57, 305–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukhopadhya, I.; Murdoch, H.; Berry, S.; Hunt, A.; Iturriza-Gomara, M.; Smith-Palmer, A.; Cameron, J.C.; Hold, G.L. Changing molecular epidemiology of rotavirus infection after introduction of monovalent rotavirus vaccination in Scotland. Vaccine 2016, 35, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Cunliffe, N.A.; Ngwira, B.M.; Dove, W.; Thindwa, B.D.; Turner, A.M.; Broadhead, R.L.; Molyneux, M.E.; Hart, A.C. Epidemiology of rotavirus infection in children in Blantyre, Malawi, 1997–2007. J. Infect. Dis. 2010, 202, S168–S174. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.P.; Kaida, A.; Ono, A.; Kubo, H.; Iritani, N. Detection and characterization of a human G9P[4] rotavirus strain in Japan. J. Med. Virol. 2015, 87, 1311–1318. [Google Scholar] [CrossRef]
- Giri, S.; Nair, N.P.; Mathew, A.; Manohar, B.; Simon, A.; Singh, T.; Suresh Kumar, S.; Mathew, M.A.; Babji, S.; Arora, R.; et al. Rotavirus gastroenteritis in Indian children < 5 years hospitalized for diarrhoea, 2012 to 2016. BMC Public Health 2019, 19, 69. [Google Scholar]
- Cashman, O.; Collins, P.J.; Lennon, G.; Cryan, B.; Martella, V.; Fanning, S.; Staines, A.; O’Shea, H. Molecular characterization of group A rotaviruses detected in children with gastroenteritis in Ireland in 2006–2009. Epidemiol. Infect. 2011, 140, 247–259. [Google Scholar] [CrossRef]
- Collins, P.J.; Mulherin, E.; O’Shea, H.; Cashman, O.; Lennon, G.; Pidgeon, E.; Coughlan, S.; Hall, W.; Fanning, S. Changing patterns of rotavirus strains circulating in Ireland: Re-emergence of G2P[4] and identification of novel genotypes in Ireland. J. Med. Virol. 2015, 87, 764–773. [Google Scholar] [CrossRef]
- Lennon, G.; Reidy, N.; Cryan, B.; Fanning, S.; O’Shea, H. Changing profile of rotavirus in Ireland: Predominance of P[8] and emergence of P[6] and P[9] in mixed infections. J. Med. Virol. 2008, 80, 524–530. [Google Scholar] [CrossRef]
- Mokomane, M.; Esona, M.D.; Bowen, M.D.; Tate, J.E.; Steenhoff, A.P.; Lechiile, K.; Gaseitsiwe, S.; Seheri, L.M.; Magagula, N.B.; Weldegebriel, G.; et al. Diversity of Rotavirus Strains Circulating in Botswana before and after introduction of the Monovalent Rotavirus Vaccine. Vaccine 2019, 37, 6324–6328. [Google Scholar] [CrossRef]
- WHO-Botswana. Available online: https://www.afro.who.int/news/who-supports-botswana-respond-outbreak-diarrhoea-children-below-five-years-age. (accessed on 29 May 2020).
- Rakau, K.; Gededzha, M.; Peenze, I.; Seheri, M. Rotavirus strains detected in Dr George Mukhari academic hospital and Oukasie primary healthcare, Pretoria from 2015-2016. In Proceedings of the 12th African Rotavirus Symposium, Johannesburg, South Africa, 30 July–1 August 2019. [Google Scholar]
- Gugu, M.; Nomcebo, P.; Sindisiwe, D.; Susan, K.; Gilbert, M.; Goitom, W.; Lonkululeko, K.; Xolsile, D.; Getahun, T.; Michael, L.; et al. G3P[8] rotavirus strain causing diarrheal outbreak in the Kingdom of Eswatini, 2018. In Proceedings of the 12th African Rotavirus Symposium, Johannesburg, South Africa, 30 July–1 August 2019. [Google Scholar]
- Mhango, C.; Chinyama, E.; Mandolo, J.; Malamba, C.; Wachepa, R.; Kanjerwa, O.; Kamng’ona, A.W.; Shawa, I.T.; Jere, K.C. Changes in rotavirus strains circulating in Malawi before vaccine introduction and six years post vaccine era. In Proceedings of the 12th African Rotavirus Symposium, Johannesburg, South Africa, 30 July–1 August 2019. [Google Scholar]
- Carvalho-Costa, F.A.; de Assis, R.M.S.; Fialho, A.M.; Araujo, I.T.; Silva, M.F.; Gomez, M.M.; Andrade, J.S.; Rose, T.L.; Fumian, T.M.; Voloãto, E.M. The evolving epidemiology of rotavirus A infection in Brazil a decade after the introduction of universal vaccination with Rotarix(R). BMC Pediatr. 2019, 19, 42. [Google Scholar] [CrossRef]
- Roczo-Farkas, S.; Kirkwood, C.D.; Cowley, D.; Barnes, G.L.; Bishop, R.F.; Bogdanovic-Sakran, N.; Boniface, K.; Donato, C.M.; Bines, J.E. The Impact of Rotavirus Vaccines on Genotype Diversity: A Comprehensive Analysis of 2 Decades of Australian Surveillance Data. J. Infect. Dis. 2018, 218, 546–554. [Google Scholar] [CrossRef]
- Cowley, D.; Donato, C.M.; Roczo-Farkas, S.; Kirkwood, C.D. Emergence of a novel equine-like G3P[8] inter-genogroup reassortant rotavirus strain associated with gastroenteritis in Australian children. J. Gen. Virol. 2015, 97, 403–410. [Google Scholar] [CrossRef]
- Page, N.; Mapuroma, F.; Seheri, M.; Kruger, T.; Peenze, I.; Walaza, S.; Cohen, C.; Groome, M.; Madhi, S. Rotavirus surveillance report, South Africa, 2013. Commun Dis Surveill Bull. 2014, 12, 130–135. [Google Scholar]
- Jere, K.C.; Chaguza, C.; Bar-Zeev, N.; Lowe, J.; Peno, C.; Kumwenda, B.; Nakagomi, O.; Tate, J.E.; Parashar, U.D.; Heyderman, R.S.; et al. Emergence of Double- and Triple-Gene Reassortant G1P[8] Rotaviruses Possessing a DS-1-Like Backbone after Rotavirus Vaccine Introduction in Malawi. J. Virol. 2018, 92, e01246-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komoto, S.; Tacharoenmuang, R.; Guntapong, R.; Ide, T.; Haga, K.; Katayama, K.; Kato, T.; Ouchi, Y.; Kurahashi, H.; Tsjui, T.; et al. Emergence and Characterization of Unusual DS-1-Like G1P[8] Rotavirus Strains in Children with Diarrhea in Thailand. PLoS ONE 2015, 10, e0141739. [Google Scholar] [CrossRef] [PubMed]
- Mwangi, P.N.; Mogotsi, M.T.; Rasebotsa, S.P.; Seheri, M.L.; Mphahlele, M.J.; Ndze, V.N.; Dennis, F.E.; Jere, K.C.; Nyaga, M.M. Uncovering the First Atypical DS-1-like G1P[8] Rotavirus Strains That Circulated during Pre-Rotavirus Vaccine Introduction Era in South Africa. Pathogens 2020, 9, 391. [Google Scholar] [CrossRef]
- Gouvea, V.; Glass, R.I.; Woods, P.; Taniguchi, K.; Clark, H.F.; Forrester, B.; Fang, Z.Y. Polymerase chain reaction amplification and typing of rotavirus nucleic acid from stool specimens. J. Clin. Microbiol. 1990, 28, 276–282. [Google Scholar] [CrossRef] [Green Version]
- Iturriza Gomara, M.; Kang, G.; Mammen, A.; Jana, A.K.; Abraham, M.; Desselberger, U.; Brown, D.; Gray, J. Characterization of G10P[11] rotaviruses causing acute gastroenteritis in neonates and infants in Vellore, India. J. Clin. Microbiol. 2004, 42, 2541–2547. [Google Scholar] [CrossRef] [Green Version]
- Aladin, F.; Nawaz, S.; Iturriza-Gomara, M.; Gray, J. Identification of G8 rotavirus strains determined as G12 by rotavirus genotyping PCR: Updating the current genotyping methods. J. Clin. Virol. 2010, 47, 340–344. [Google Scholar] [CrossRef]
- Gentsch, J.R.; Glass, R.I.; Woods, P.; Gouvea, V.; Gorziglia, M.; Flores, J.; Das, B.K.; Bhan, M.K. Identification of group A rotavirus gene 4 types by polymerase chain reaction. J. Clin. Microbiol. 1992, 30, 1365–1373. [Google Scholar] [CrossRef] [Green Version]
- Iturriza-Gomara, M.; Green, J.; Brown, D.W.; Desselberger, U.; Gray, J.J. Diversity within the VP4 gene of rotavirus P [8] strains: Implications for reverse transcription-PCR genotyping. J. Clin. Microbiol. 2000, 38, 898–901. [Google Scholar] [CrossRef] [Green Version]
- Mphahlele, M.J.; Peenze, I.; Steele, A.D. Rotavirus strains bearing the VP4P[14] genotype recovered from South African children with diarrhoea. Arch. Virol. 1999, 144, 1027–1034. [Google Scholar] [CrossRef]


{kind=link}
| 1 G Type | Pre-Vaccine | Post-Vaccine | OR (95% CI) | p-Value | ||
|---|---|---|---|---|---|---|
| 5 2012–2015 | 2016–2019 | |||||
| n | % | n | % | |||
| G1 | 34 | 17.0 | 10 | 23.3 | 1.47 (0.59–3.44) | 0.330 |
| G12 | 37 | 18.5 | 1 | 2.3 | 0.10 (0.003–0.66) | 0.008 |
| G2 | 25 | 12.5 | 1 | 2.3 | 0.16 (0.004–1.08) | 0.054 |
| G3 | 0 | 0.0 | 21 | 48.8 | - | - |
| G8 | 6 | 3.0 | 1 | 2.3 | 0.76 (0.02–6.61) | 0.810 |
| G9 | 61 | 30.5 | 4 | 9.3 | 0.23 (0.01–0.69) | 0.004 |
| 2 Mix G | 10 | 5.0 | 1 | 2.3 | 0.45 (0.01–3.30) | 0.440 |
| 3 Gx | 27 | 13.5 | 4 | 9.3 | 0.65 (0.16–2.04) | 0.450 |
| Total | 200 | 100.0 | 43 | 100.0 | - | - |
| 1 P type | - | - | - | - | - | - |
| P[4] | 31 | 15.5 | 16 | 37.2 | 3.23 (1.44–7.04) | <0.001 |
| P[6] | 32 | 16.0 | 3 | 7.0 | 0.39 (0.07–1.36) | 0.120 |
| P[8] | 108 | 54.0 | 22 | 51.2 | 0.89 (0.43–1.83) | 0.740 |
| Mix P | 8 | 4.0 | 0 | 0.0 | - | - |
| 4 P[x] | 21 | 10.5 | 2 | 4.7 | 0.42 (0.05–0.82) | 0.230 |
| Total | 200 | 100.0 | 43 | 100.0 | - | - |
| 1 G Type | 5 Pre-Vaccine | Post-Vaccine | OR (95% CI) | p-Value | ||
|---|---|---|---|---|---|---|
| 2015 | 2016–2019 | |||||
| n | % | n | % | |||
| G1 | 67 | 31.5 | 42 | 21.6 | 0.60 (0.37–0.96) | 0.030 |
| G12 | 2 | 0.9 | 2 | 1.0 | 1.18 (0.08–15.29) | 0.930 |
| G2 | 10 | 4.7 | 11 | 5.7 | 1.22 (0.46–3.28) | 0.660 |
| G3 | 0 | 0 | 51 | 26.3 | - | - |
| G8 | 0 | 0 | 3 | 1.5 | - | - |
| G9 | 105 | 49.3 | 49 | 25.3 | 0.35 (0.22–0.54) | <0.001 |
| 2 Mix G | 0 | 0 | 12 | 6.2 | - | - |
| 3 Gx | 29 | 13.6 | 24 | 12.4 | 0.90 (0.48–1.66) | 0.710 |
| Total | 213 | 100.0 | 194 | 100.0 | - | - |
| 1 P type | - | - | - | - | - | - |
| P[4] | 1 | 0.5 | 71 | 36.6 | - | - |
| P[6] | 10 | 4.7 | 37 | 19.1 | 4.78 (2.23–11.10) | <0.001 |
| P[8] | 182 | 85.4 | 76 | 39.2 | 0.10 (0.06–0.16) | <0.001 |
| 4 P[x] | 20 | 9.4 | 10 | 5.2 | 0.57 (0.23–1.32) | 0.100 |
| Total | 213 | 100.0 | 194 | 100.0 | - | - |
| 1 G/P Genotype Combination | 5 Pre-Vaccine | Post-Vaccine | OR (95% CI) | p-Value | ||
|---|---|---|---|---|---|---|
| 2012–2015 | 2016–2019 | |||||
| n | % | n | % | |||
| G1P[8] | 34 | 17.0 | 9 | 20.9 | 1.29 (0.50–3.07) | 0.540 |
| G9P[8] | 57 | 28.5 | 1 | 2.3 | 0.06 (0.002–0.40) | < 0.001 |
| G12P[6] | 26 | 13.0 | 0 | 0.0 | - | - |
| G2P[4] | 20 | 10.0 | 1 | 2.3 | 0.21 (0.01–1.42) | 0.100 |
| G12P[8] | 6 | 3.0 | 0 | 0.0 | - | - |
| G3P[4] | 0 | 0.0 | 8 | 18.6 | - | - |
| G3P[8] | 0 | 0.0 | 11 | 25.6 | - | - |
| G8P[4] | 5 | 2.5 | 1 | 2.3 | 0.93 (0.02–8.61) | 0.950 |
| G9P[4] | 0 | 0.0 | 2 | 4.7 | - | - |
| G9P[6] | 0 | 0.0 | 2 | 4.7 | - | - |
| 2 Other genotypes | 5 | 2.5 | 3 | 7.0 | 2.93 (0.43–15.65) | 0.140 |
| 3 Mixed types | 13 | 6.5 | 1 | 2.3 | 0.34 (0.01–2.41) | 0.290 |
| 4 Partial G/P types | 20 | 10.0 | 2 | 4.7 | 0.44 (0.05–1.93) | 0.270 |
| Untypeables | 14 | 7.0 | 2 | 4.7 | 0.64 (0.07–3.00) | 0.570 |
| Total | 200 | 100.0 | 43 | 100.0 | - | - |
| 1 G/P Genotype Combination | 5 Pre-Vaccine | Post-Vaccine | OR (95% CI) | p-Value | ||
|---|---|---|---|---|---|---|
| 2015 | 2016–2019 | |||||
| n | % | n | % | |||
| G1P[8] | 66 | 31.0 | 40 | 20.6 | 0.58 (0.36–0.93) | 0.020 |
| G3P[4] | 0 | 0.0 | 28 | 14.4 | - | - |
| G3P[6] | 0 | 0.0 | 3 | 1.5 | - | - |
| G3P[8] | 0 | 0.0 | 19 | 9.8 | - | - |
| G8P[4] | 0 | 0.0 | 3 | 1.5 | - | - |
| G9P[4] | 0 | 0.0 | 24 | 12.4 | - | - |
| G9P[6] | 0 | 0.0 | 17 | 8.8 | - | - |
| G2P[4] | 1 | 0.5 | 3 | 1.5 | - | - |
| G2P[6] | 9 | 4.2 | 8 | 4.1 | 0.97 (0.32–2.91) | 0.959 |
| G9P[8] | 98 | 46.0 | 7 | 3.6 | 0.04 (0.02–0.10) | <0.001 |
| 2 Other genotypes | 3 | 1.4 | 4 | 2.1 | 1.47 (0.25–10.18) | 0.612 |
| 3 Mixed types | 0 | 0 | 12 | 6.2 | - | |
| 4 Partial G/P types | 23 | 10.8 | 18 | 9.3 | 0.84 (0.41–1.70) | 0.611 |
| Untypeables | 13 | 6.1 | 8 | 4.1 | 0.66 (0.23–1.77) | 0.370 |
| Total | 213 | 100.0 | 194 | 100.0 | - | - |
| G/P Genotype Combination | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | |
| G1P[8] | 2 | 3.0 | 0 | 0.0 | 28 | 84.8 | 4 | 5.3 | 6 | 66.7 | 3 | 18.8 | 0 | 0.0 | 0 | 0.0 |
| G9P[8] | 1 | 1.5 | 0 | 0.0 | 0 | 0.0 | 56 | 73.7 | 0 | 0.0 | 1 | 6.3 | 0 | 0.0 | 0 | 0.0 |
| G12P[6] | 26 | 38.8 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0 | 0 | 0.0 | 0 | 0.0 |
| G2P[4] | 5 | 7.5 | 16 | 66.7 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0 | 1 | 9.1 | 0 | 0.0 |
| G12P[8] | 5 | 7.5 | 0 | 0.0 | 0 | 0.0 | 1 | 1.3 | 0 | 0.0 | 0 | 0 | 0 | 0.0 | 0 | 0.0 |
| G3P[4] | 0 | 0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 11.1 | 4 | 25.0 | 3 | 27.3 | 0 | 0.0 |
| G3P[8] | 0 | 0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0 | 4 | 36.4 | 7 | 100.0 |
| G8P[4] | 5 | 7.5 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0 | 1 | 9.1 | 0 | 0.0 |
| G9P[4] | 0 | 0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 2 | 12.5 | 0 | 0.0 | 0 | 0.0 |
| G9P[6] | 0 | 0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0 | 0 | 0 | 2 | 18.2 | 0 | 0.0 |
| 1 Other genotypes | 3 | 4.5 | 0 | 0.0 | 0 | 0.0 | 2 | 2.6 | 1 | 11.1 | 2 | 12.5 | 0 | 0.0 | 0 | 0.0 |
| 2 Mixed types | 13 | 19.4 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 11.1 | 0 | 0 | 0 | 0.0 | 0 | 0.0 |
| 3 Partial G/P types | 5 | 7.5 | 4 | 16.7 | 4 | 12.1 | 7 | 9.2 | 0 | 0.0 | 2 | 12.5 | 0 | 0.0 | 0 | 0.0 |
| Untypeables | 2 | 3.0 | 4 | 16.7 | 1 | 3.0 | 6 | 7.9 | 0 | 0.0 | 2 | 12.5 | 0 | 0.0 | 0 | 0.0 |
| Total | 67 | 100.0 | 24 | 100.0 | 33 | 100.0 | 76 | 100.0 | 9 | 100.0 | 16 | 100.0 | 11 | 100.0 | 7 | 100.0 |
| G/P Genotype Combination | 2015 | 2016 | 2017 | 2018 | 2019 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | |
| G1P[8] | 66 | 31.0 | 17 | 43.6 | 20 | 19.2 | 0 | 0.0 | 3 | 15.0 |
| G3P[4] | 0 | 0.0 | 1 | 2.6 | 14 | 13.5 | 12 | 38.7 | 1 | 5.0 |
| G3P[6] | 0 | 0.0 | 0 | 0.0 | 2 | 1.9 | 1 | 3.2 | 0 | 0.0 |
| G3P[8] | 0 | 0.0 | 0 | 0.0 | 0 | 0 | 7 | 22.6 | 12 | 60.0 |
| G8P[4] | 0 | 0.0 | 0 | 0.0 | 1 | 1.0 | 2 | 6.5 | 0 | 0.0 |
| G9P[4] | 0 | 0.0 | 3 | 7.7 | 20 | 19.2 | 1 | 3.2 | 0 | 0.0 |
| G9P[6] | 0 | 0.0 | 5 | 12.8 | 9 | 8.7 | 3 | 9.7 | 0 | 0.0 |
| G2P[6] | 9 | 4.2 | 7 | 17.9 | 0 | 0 | 1 | 3.2 | 0 | 0.0 |
| G9P[8] | 98 | 46.0 | 0 | 0.0 | 6 | 5.8 | 1 | 3.2 | 0 | 0.0 |
| 1 Other genotypes | 4 | 1.9 | 3 | 7.7 | 3 | 2.9 | 1 | 3.2 | 0 | 0.0 |
| 2 Mixed types | 0 | 0.0 | 2 | 5.1 | 10 | 9.6 | 0 | 0.0 | 0 | 0.0 |
| 3 Partial G/P types | 23 | 10.8 | 0 | 0.0 | 14 | 13.5 | 2 | 6.5 | 2 | 10.0 |
| Untypeables | 13 | 6.1 | 1 | 2.6 | 5 | 4.8 | 0 | 0.0 | 2 | 10.0 |
| Total | 213 | 100.0 | 39 | 100.0 | 104 | 100.0 | 31 | 100.0 | 20 | 100.0 |
© 2020 World Health Organization; Licensee MDPI, Basel, Switzerland. This is an open access article distributed under the terms of the Creative Commons Attribution IGO License (http://creativecommons.org/licenses/by/3.0/igo/legalcode), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In any reproduction of this article there should not be any suggestion that WHO or this article endorse any specific organisation or products. The use of the WHO logo is not permitted.
Share and Cite
João, E.D.; Munlela, B.; Chissaque, A.; Chilaúle, J.; Langa, J.; Augusto, O.; Boene, S.S.; Anapakala, E.; Sambo, J.; Guimarães, E.; et al. Molecular Epidemiology of Rotavirus A Strains Pre- and Post-Vaccine (Rotarix®) Introduction in Mozambique, 2012–2019: Emergence of Genotypes G3P[4] and G3P[8]. Pathogens 2020, 9, 671. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens9090671
João ED, Munlela B, Chissaque A, Chilaúle J, Langa J, Augusto O, Boene SS, Anapakala E, Sambo J, Guimarães E, et al. Molecular Epidemiology of Rotavirus A Strains Pre- and Post-Vaccine (Rotarix®) Introduction in Mozambique, 2012–2019: Emergence of Genotypes G3P[4] and G3P[8]. Pathogens. 2020; 9(9):671. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens9090671
Chicago/Turabian StyleJoão, Eva D., Benilde Munlela, Assucênio Chissaque, Jorfélia Chilaúle, Jerónimo Langa, Orvalho Augusto, Simone S. Boene, Elda Anapakala, Júlia Sambo, Esperança Guimarães, and et al. 2020. "Molecular Epidemiology of Rotavirus A Strains Pre- and Post-Vaccine (Rotarix®) Introduction in Mozambique, 2012–2019: Emergence of Genotypes G3P[4] and G3P[8]" Pathogens 9, no. 9: 671. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens9090671