Clinical Symptoms of Arboviruses in Mexico

 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Clinical Symptoms of Each Arbovirus by Age Group and Sex
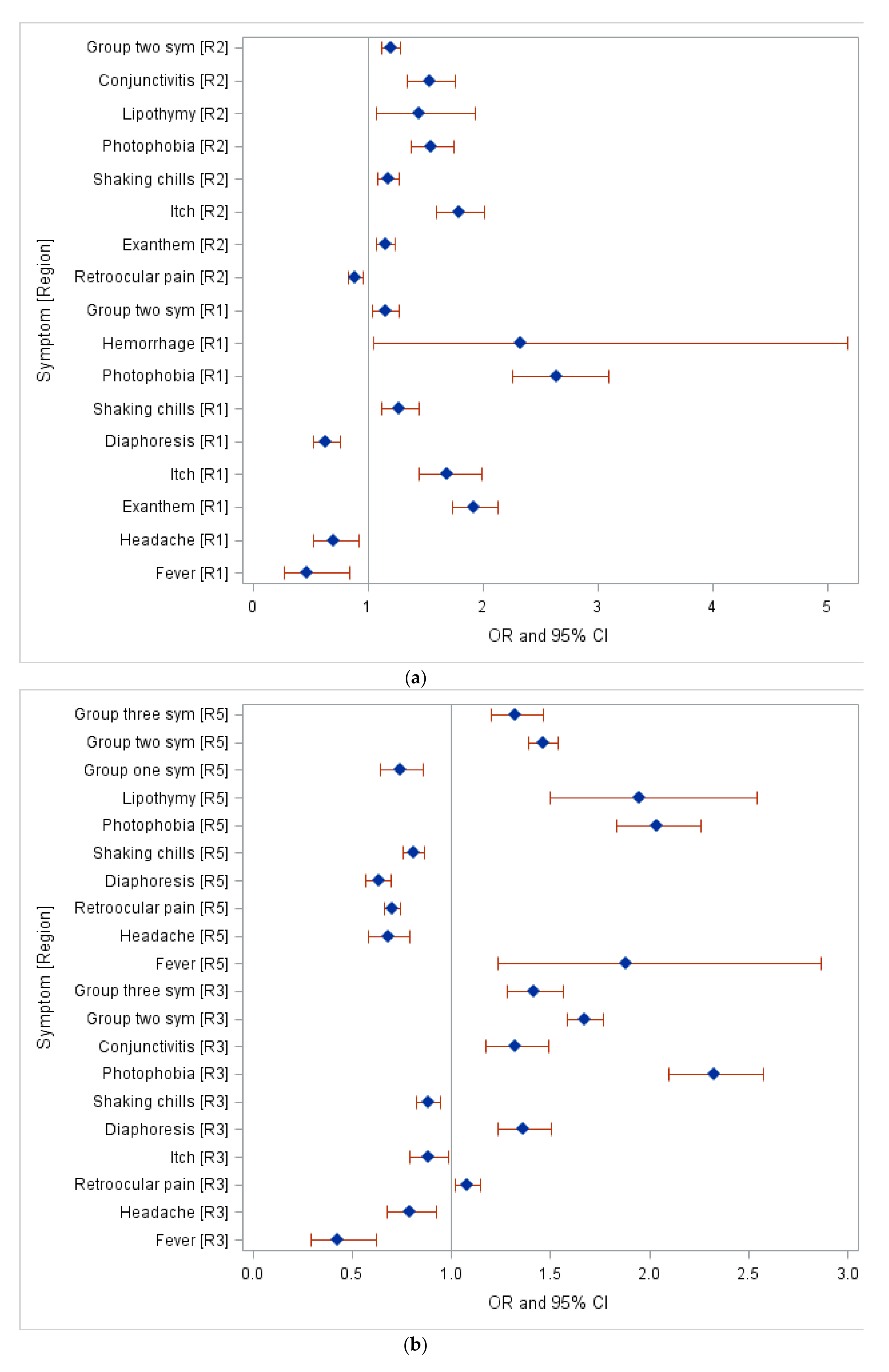
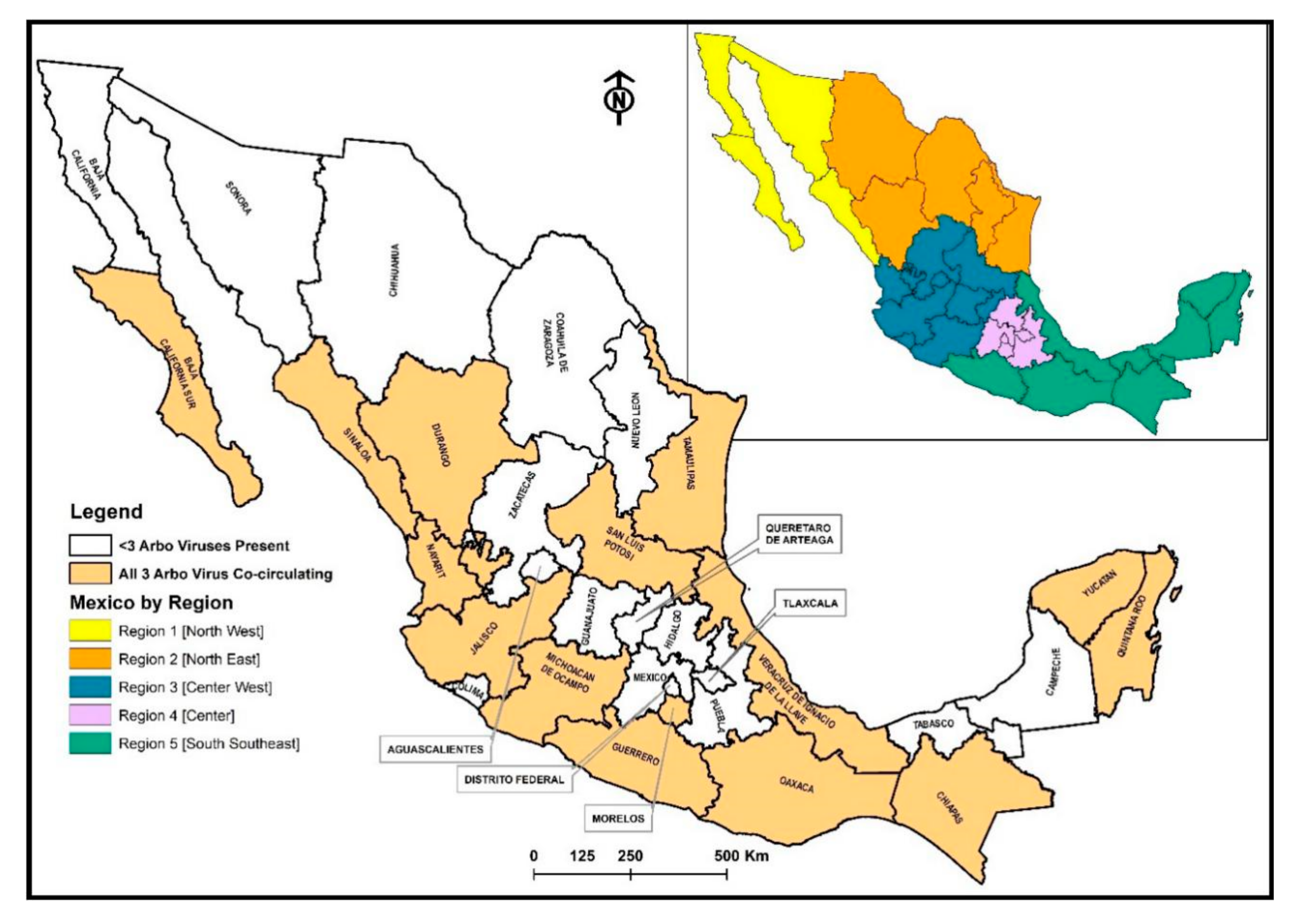
2.2. Clinical Symptoms of Each Arbovirus by Regions in Mexico
3. Discussion
4. Methodology
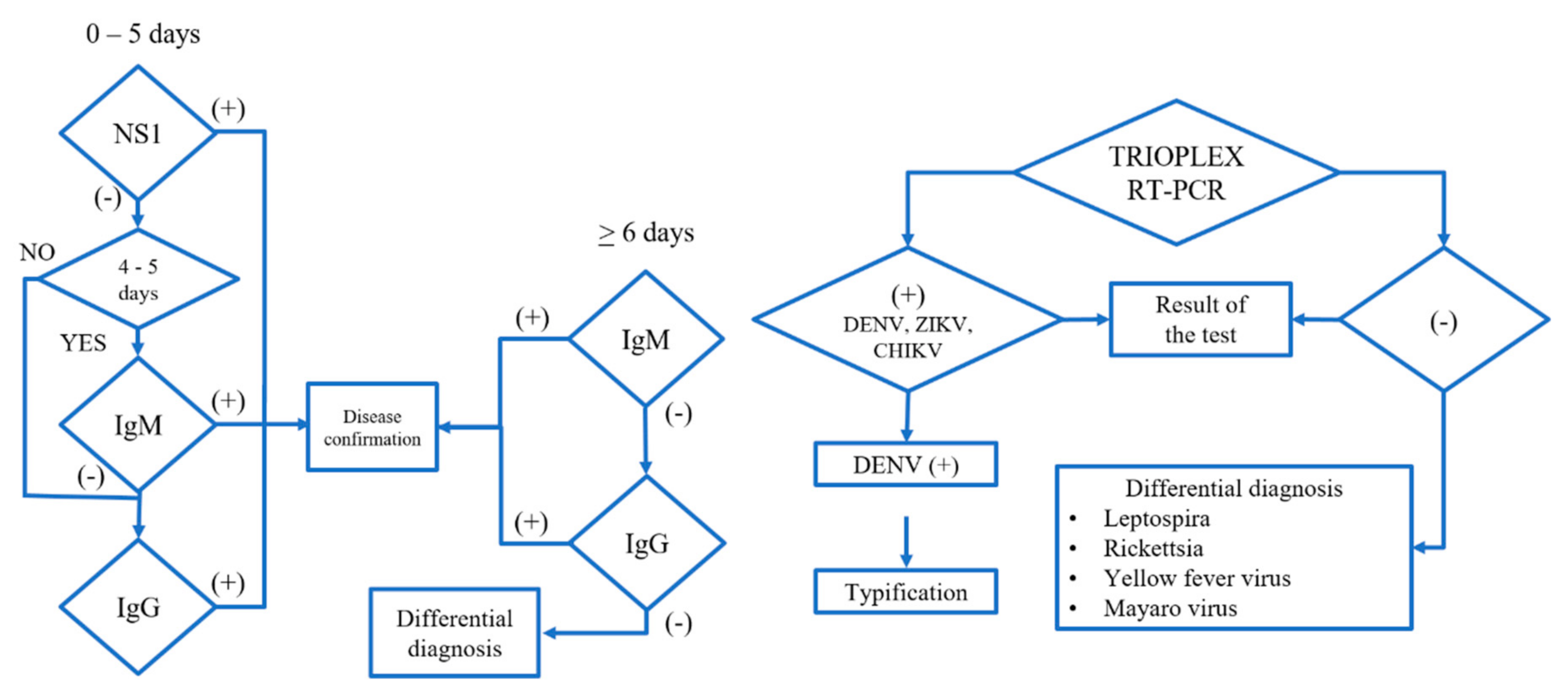
4.1. Arbovirus Cases and Diagnosis
4.2. Case Definition, Infection, and Diagnostic Tools
4.3. Statistical Analysis
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix: Tables A1–A8

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Symptoms | Total (N = 264,267) | Female (N = 145,878) | Male (N = 118,389) | p-Value * | |||
|---|---|---|---|---|---|---|---|
| Symptomatic Cases | Cases with Missing Symptoms | Symptomatic Cases | % | Symptomatic Cases | % | ||
| Fever | 263,837 | 10 | 145,611 | 55.19 | 118,227 | 44.81 | 0.003 |
| Myalgias | 244,636 | 397 | 135,666 | 55.46 | 108,971 | 44.54 | <0.0001 |
| Arthralgias | 231,277 | 407 | 128,508 | 55.56 | 102,769 | 44.44 | <0.0001 |
| Abdominal Pain | 32,430 | 57,649 | 18,413 | 56.78 | 14,017 | 43.22 | <0.0001 |
| Polyarthralgias | 27,315 | 155,201 | 16,137 | 59.08 | 11,179 | 40.92 | <0.0001 |
| Backache | 18,372 | 182,327 | 10,638 | 57.9 | 7734 | 42.1 | 0.0001 |
| Photophobia | 11,486 | 182,328 | 6825 | 59.42 | 4661 | 40.58 | <0.0001 |
| Diarrhea | 7442 | 182,321 | 3750 | 50.39 | 3692 | 49.61 | <0.0001 |
| Conjunctivitis | 5935 | 182,319 | 3169 | 53.4 | 2766 | 46.6 | <0.0001 |
| Cough | 4675 | 182324 | 2457 | 52.56 | 2218 | 47.44 | <0.0001 |
| Pharyngitis | 4956 | 182,323 | 2725 | 54.98 | 2231 | 45.02 | 0.014 |
| Sickness | 48,245 | 182,320 | 27,984 | 58 | 20,261 | 42 | <0.0001 |
| Headache | 253,725 | 366 | 140,751 | 55.47 | 112,975 | 44.53 | <0.0001 |
| Itch | 6396 | 224,855 | 3938 | 61.57 | 2458 | 38.42 | <0.0001 |
| Vomit | 42,869 | 76,174 | 24,289 | 56.66 | 18,580 | 43.34 | <0.0001 |
| Retroocular pain | 174,348 | 7044 | 96,723 | 55.48 | 77,625 | 44.52 | <0.0001 |
| Exanthem | 77,140 | 84 | 43,723 | 56.68 | 33,418 | 43.32 | <0.0001 |
| Symptoms | Cases with Missing Symptoms | Age Group (0–4) (N = 25,895) | Age Group (5–15) (N = 72,854) | Age Group (>15) (N = 165,523) | p-Value * | |||
|---|---|---|---|---|---|---|---|---|
| Symptomatic Cases | % | Symptomatic Cases | % | Symptomatic Cases | % | |||
| Fever | 10 | 25,765 | 9.77 | 72,676 | 27.55 | 165,396 | 62.69 | <0.0001 |
| Myalgias | 397 | 22,057 | 9.02 | 65,478 | 26.77 | 157,101 | 64.22 | <0.0001 |
| Arthralgias | 407 | 19,775 | 8.55 | 59,946 | 25.92 | 151,555 | 65.53 | <0.0001 |
| Abdominal Pain | 57,649 | 4270 | 13.17 | 10,564 | 32.57 | 17,596 | 54.26 | <0.0001 |
| Polyarthralgias | 155,201 | 2079 | 7.61 | 6098 | 22.32 | 19,138 | 70.06 | <0.0001 |
| Backache | 182,327 | 4215 | 22.94 | 6649 | 36.19 | 7508 | 40.87 | <0.0001 |
| Diaphoresis | 182,326 | 2559 | 26.23 | 3827 | 39.23 | 3369 | 34.54 | <0.0001 |
| Shaking chills | 182,321 | 5689 | 22.76 | 9532 | 38.13 | 9779 | 39.12 | <0.0001 |
| Photophobia | 182,328 | 2788 | 24.27 | 4460 | 38.83 | 4238 | 36.9 | <0.0001 |
| Diarrhea | 182,321 | 1896 | 25.48 | 2987 | 40.14 | 2559 | 34.39 | 0.0007 |
| Conjunctivitis | 182,319 | 1122 | 18.9 | 2071 | 34.89 | 2742 | 46.2 | <0.0001 |
| Nasal congestion | 182,323 | 719 | 22 | 1249 | 38.22 | 1249 | 39.78 | <0.0001 |
| Pharyngitis | 182,323 | 1122 | 22.64 | 1882 | 37.97 | 1952 | 39.39 | <0.0001 |
| Sickness | 182,320 | 11,870 | 24.6 | 20,318 | 42.11 | 16,057 | 33.28 | <0.0001 |
| Headache | 366 | 23,135 | 9.12 | 69,713 | 27.48 | 160,877 | 63.41 | <0.0001 |
| Itch | 224,855 | 220 | 3.44 | 1233 | 19.28 | 4943 | 77.28 | <0.0001 |
| Vomit | 76174 | 8004 | 18.67 | 16,372 | 38.19 | 18,493 | 43.14 | <0.0001 |
| Retroocular pain | 7044 | 15,868 | 9.1 | 47,189 | 27.07 | 111,291 | 63.83 | <0.0001 |
| Exanthem | 84 | 7660 | 9.93 | 21,512 | 27.89 | 47,968 | 62.18 | 0.0072 |
| Symptoms | Total (N = 305) | Female (N = 186) | Male (N = 119) | p-Value * | |||
|---|---|---|---|---|---|---|---|
| Symptomatic Cases | Cases with Missing Symptom | Symptomatic Cases | % | Symptomatic Cases | % | ||
| Polyarthralgias | 100 | 102 | 70 | 70 | 30 | 30 | 0.04 |
| Symptoms | Cases with Missing Symptoms | Age Group (0–4) (N = 8) | Age Group (5–15) (N = 52) | Age Group (>15) (N = 245) | p-Value * | |||
|---|---|---|---|---|---|---|---|---|
| Symptomatic Cases | % | Symptomatic Cases | % | Symptomatic Cases | % | |||
| Myalgias | 0 | 6 | 2.2 | 42 | 15.38 | 225 | 82.42 | 0.024 |
| Vomit | 9 | 1 | 2.56 | 12 | 30.77 | 26 | 66.67 | 0.037 |
| Shaking chills | 37 | 0 | 0 | 14 | 12.96 | 94 | 87.04 | 0.033 (F) |
| Cough | 37 | 2 | 7.41 | 1 | 3.7 | 24 | 88.89 | 0.049 (F) |
| Symptoms | Total (N = 10,319) | Female (N = 8745) | Male (N = 1574) | p-Value * | |||
|---|---|---|---|---|---|---|---|
| Symptomatic Cases | Cases with Missing Symptom | Symptomatic Cases | % | Symptomatic Cases | % | ||
| Fever | 7226 | 0 | 5810 | 80.4 | 1416 | 19.6 | <0.0001 |
| Myalgias | 7739 | 13 | 6417 | 82.92 | 1322 | 17.08 | <0.0001 |
| Arthralgias | 6659 | 25 | 5511 | 82.76 | 1148 | 17.24 | <0.0001 |
| Retroocular pain | 4967 | 40 | 4043 | 81.4 | 924 | 18.6 | <0.0001 |
| Exanthem | 9728 | 9 | 8333 | 85.66 | 1395 | 14.34 | <0.0001 |
| Abdominal Pain | 951 | 69 | 772 | 81.18 | 179 | 18.82 | 0.001 |
| Polyarthralgias | 674 | 63 | 516 | 76.56 | 158 | 23.44 | <0.0001 |
| Diaphoresis | 688 | 157 | 528 | 76.74 | 160 | 23.26 | <0.0001 |
| Shaking chills | 2145 | 57 | 1609 | 75.01 | 536 | 24.99 | <0.0001 |
| Photophobia | 1350 | 77 | 1103 | 81.7 | 247 | 18.3 | 0.0006 |
| Diarrhea | 700 | 70 | 536 | 76.57 | 164 | 23.43 | <0.0001 |
| Conjunctivitis | 5033 | 37 | 4230 | 84.05 | 803 | 15.95 | 0.043 |
| Nasal congestion | 602 | 75 | 485 | 80.56 | 117 | 19.44 | 0.003 |
| Cough | 498 | 68 | 391 | 78.51 | 107 | 21.49 | <0.0001 |
| Pharyngitis | 1096 | 70 | 862 | 78.65 | 234 | 21.35 | <0.0001 |
| Headache | 8408 | 10 | 7013 | 83.41 | 1395 | 16.59 | <0.0001 |
| Itch | 6751 | 42 | 5859 | 86.79 | 892 | 13.21 | <0.0001 |
| Symptoms | Cases with Missing Symptoms | Age Group (0–4) (N = 144) | Age Group (5–15) (N = 747) | Age Group (> 15) (N = 9428) | p-Value * | |||
|---|---|---|---|---|---|---|---|---|
| Symptomatic Cases | % | Symptomatic Cases | % | Symptomatic Cases | % | |||
| Fever | 0 | 126 | 1.74 | 606 | 8.39 | 6494 | 89.87 | <0.0001 |
| Myalgias | 13 | 74 | 0.96 | 558 | 7.21 | 7107 | 91.83 | <0.0001 |
| Arthralgias | 25 | 56 | 0.84 | 440 | 6.61 | 6163 | 92.55 | <0.0001 |
| Retroocular pain | 40 | 43 | 0.87 | 383 | 7.71 | 4541 | 91.42 | <0.0001 |
| Exanthem | 9 | 123 | 1.26 | 679 | 6.98 | 8926 | 91.76 | <0.0001 |
| Vomit | 68 | 24 | 2.37 | 86 | 8.48 | 904 | 89.15 | 0.004 |
| Backpain | 90 | 9 | 0.34 | 150 | 5.61 | 2516 | 94.06 | <0.0001 |
| Conjunctivitis | 37 | 60 | 1.19 | 310 | 6.16 | 4663 | 92.65 | <0.0001 |
| Sickness | 53 | 24 | 0.91 | 186 | 7.09 | 2415 | 92 | 0.05 |
| Headache | 10 | 86 | 1.02 | 656 | 7.8 | 7666 | 91.18 | <0.0001 |
| Itch | 42 | 72 | 1.07 | 435 | 6.44 | 6244 | 92.49 | <0.0001 |
| Clinical Symptom | Odds Ratio Estimate | Lower CL | Upper CL |
|---|---|---|---|
| Fever (R*1) | 0.47 | 0.27 | 0.84 |
| Headache (R1) | 0.70 | 0.53 | 0.92 |
| Exanthem (R1) | 1.93 | 1.74 | 2.14 |
| Itch (R1) | 1.69 | 1.44 | 1.99 |
| Diaphoresis (R1) | 0.63 | 0.53 | 0.75 |
| Shaking chills (R1) | 1.27 | 1.12 | 1.44 |
| Photophobia (R1) | 2.64 | 2.26 | 3.10 |
| Hemorrhage (R1) | 2.33 | 1.05 | 5.18 |
| Group two sym (R1) | 1.15 | 1.04 | 1.28 |
| Retroocular pain (R2) | 0.89 | 0.83 | 0.95 |
| Exanthem (R2) | 1.15 | 1.07 | 1.23 |
| Itch (R2) | 1.79 | 1.59 | 2.02 |
| Shaking chills (R2) | 1.17 | 1.08 | 1.27 |
| Photophobia (R2) | 1.55 | 1.38 | 1.74 |
| Lipothymy (R2) | 1.44 | 1.07 | 1.93 |
| Conjunctivitis (R2) | 1.54 | 1.35 | 1.76 |
| Group two sym (R2) | 1.20 | 1.12 | 1.28 |
| Fever (R3) | 0.42 | 0.29 | 0.62 |
| Headache (R3) | 0.79 | 0.67 | 0.93 |
| Retroocular pain (R3) | 1.08 | 1.02 | 1.15 |
| Itch (R3) | 0.88 | 0.79 | 0.99 |
| Diaphoresis (R3) | 1.36 | 1.23 | 1.50 |
| Shaking chills (R3) | 0.88 | 0.82 | 0.95 |
| Photophobia (R3) | 2.32 | 2.10 | 2.58 |
| Conjunctivitis (R3) | 1.32 | 1.17 | 1.49 |
| Group two sym (R3) | 1.67 | 1.58 | 1.76 |
| Group three sym (R3) | 1.42 | 1.28 | 1.57 |
| Fever (R5) | 1.88 | 1.24 | 2.87 |
| Headache (R5) | 0.68 | 0.58 | 0.79 |
| Retroocular pain (R5) | 0.70 | 0.66 | 0.75 |
| Diaphoresis (R5) | 0.63 | 0.57 | 0.70 |
| Shaking chills (R5) | 0.81 | 0.75 | 0.87 |
| Photophobia (R5) | 2.04 | 1.83 | 2.26 |
| Lipothymy (R5) | 1.95 | 1.5 | 2.54 |
| Group one sym (R5) | 0.75 | 0.64 | 0.86 |
| Group two sym (R5) | 1.46 | 1.39 | 1.54 |
| Group three sym (R5) | 1.33 | 1.20 | 1.47 |
| Clinical Symptom | Odds Ratio Estimate | Lower CL | Upper CL |
|---|---|---|---|
| Fever (R*1) | 2.22 | 1.33 | 3.71 |
| Itch (R1) | 0.38 | 0.25 | 0.58 |
| Conjunctivitis (R1) | 1.6 | 1.05 | 2.44 |
| Fever (R2) | 1.26 | 1.02 | 1.56 |
| Exanthem (R2) | 2.34 | 1.44 | 3.81 |
| Itch (R2) | 0.69 | 0.56 | 0.86 |
| Photophobia (R2) | 0.59 | 0.43 | 0.82 |
| Conjunctivitis (R2) | 0.51 | 0.42 | 0.63 |
| Fever (R4) | 1.73 | 1.36 | 2.2 |
| Exanthem (R4) | 2.1 | 1.26 | 3.48 |
| Itch (R4) | 0.32 | 0.25 | 0.4 |
| Photophobia (R4) | 0.66 | 0.47 | 0.92 |
| Conjunctivitis (R4) | 1.69 | 1.36 | 2.11 |
| Itch (R5) | 1.42 | 1.18 | 1.7 |
| Photophobia (R5) | 0.67 | 0.53 | 0.86 |
References
- Carrillo-Hernández, M.Y.; Ruiz-Saenz, J.; Villamizar, L.J.; Gómez-Rangel, S.Y.; Martínez-Gutierrez, M. Co-circulation and simultaneous co-infection of dengue, chikungunya, and zika viruses in patients with febrile syndrome at the Colombian-Venezuelan border. BMC Infect. Dis. 2018, 18, 61. [Google Scholar] [CrossRef]
- Kraemer, M.U.; Sinka, M.E.; Duda, K.A.; Mylne, A.Q.; Shearer, F.M.; Barker, C.M.; Moore, C.G.; Carvalho, R.G.; Coelho, G.E.; Van Bortel, W.; et al. The global distribution of the arbovirus vectors Aedes aegypti and Ae. albopictus. Elife 2015, 4, e08347. [Google Scholar] [CrossRef] [PubMed]
- Lubinda, J.; Trevino, C.J.; Walsh, M.R.; Moore, A.J.; Hanafi-Bojd, A.A.; Akgun, S.; Zhao, B.; Barro, A.S.; Begum, M.M.; Jamal, H.; et al. Environmental suitability for Aedes aegypti and Aedes albopictus and the spatial distribution of major arboviral infections in Mexico. Parasite Epidemiol. Control 2019, 6, e00116. [Google Scholar] [CrossRef] [PubMed]
- Monaghan, A.J.; Morin, C.W.; Steinhoff, D.F.; Wilhelmi, O.; Hayden, M.; Quattrochi, D.A.; Reiskind, M.; Lloyd, A.L.; Smith, K.; Schmidt, C.A.; et al. On the Seasonal Occurrence and Abundance of the Zika Virus Vector Mosquito Aedes aegypti in the Contiguous United States. PLoS Curr. 2016, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attaway, D.F.; Waters, N.M.; Geraghty, E.M.; Jacobsen, K.H. Zika virus: Endemic and epidemic ranges of Aedes mosquito transmission. J. Infect Public Health 2017, 10, 120–123. [Google Scholar] [CrossRef] [Green Version]
- Cabral-Castro, M.J.; Cavalcanti, M.G.; Peralta, R.H.S.; Peralta, J.M. Molecular and serological techniques to detect co-circulation of DENV, ZIKV and CHIKV in suspected dengue-like syndrome patients. J. Clin. Virol. 2016, 82, 108–111. [Google Scholar] [CrossRef]
- Estofolete, C.F.; Terzian, A.C.; Parreira, R.; Esteves, A.; Hardman, L.; Greque, G.V.; Rahal, P.; Nogueira, M.L. Clinical and laboratory profile of Zika virus infection in dengue suspected patients: A case series. J. Clin. Virol. 2016, 81, 25–30. [Google Scholar] [CrossRef] [Green Version]
- Acevedo, N.; Waggoner, J.; Rodriguez, M.; Rivera, L.; Landivar, J.; Pinsky, B.; Zambrano, H. Zika Virus, Chikungunya Virus, and Dengue Virus in Cerebrospinal Fluid from Adults with Neurological Manifestations, Guayaquil, Ecuador. Front. Microbiol. 2017, 8, 42. [Google Scholar] [CrossRef] [Green Version]
- Mackenzie, J.S.; Gubler, D.J.; Petersen, L.R. Emerging flaviviruses: The spread and resurgence of Japanese encephalitis, West Nile and dengue viruses. Nat. Med. 2004, 10, S98–S109. [Google Scholar] [CrossRef]
- Messina, J.P.; Brady, O.J.; Scott, T.W.; Zou, C.; Pigott, D.M.; Duda, K.A.; Bhatt, S.; Katzelnick, L.; Howes, R.E.; Battle, K.E.; et al. Global spread of dengue virus types: Mapping the 70 year history. Trends Microbiol. 2014, 22, 138–146. [Google Scholar] [CrossRef] [Green Version]
- Brathwaite Dick, O.; San Martin, J.L.; Montoya, R.H.; del Diego, J.; Zambrano, B.; Dayan, G.H. The history of dengue outbreaks in the Americas. Am. J. Trop Med. Hyg. 2012, 87, 584–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Treatment, Prevention and Control Global Strategy for Dengue Prevention and Control 2; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- WHO. Dengue Data Application; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Barclay, E. Is climate change affecting dengue in the Americas? Lancet 2008, 371, 973–974. [Google Scholar] [CrossRef]
- Chang, S.F.; Su, C.L.; Shu, P.Y.; Yang, C.F.; Liao, T.L.; Cheng, C.H.; Hu, H.C.; Huang, J.H. Concurrent isolation of chikungunya virus and dengue virus from a patient with coinfection resulting from a trip to Singapore. J. Clin. Microbiol. 2010, 48, 4586–4589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Messina, J.P.; Kraemer, M.U.; Brady, O.J.; Pigott, D.M.; Shearer, F.M.; Weiss, D.J.; Golding, N.; Ruktanonchai, C.W.; Gething, P.W.; Cohn, E.; et al. Mapping global environmental suitability for Zika virus. Elife 2016, 5, e15272. [Google Scholar] [CrossRef] [PubMed]
- Yanez-Arenas, C.; Rioja-Nieto, R.; Martin, G.A.; Dzul-Manzanilla, F.; Chiappa-Carrara, X.; Buenfil-Avila, A.; Manrique-Saide, P.; Correa-Morales, F.; Díaz-Quiñónez, J.A.; Pérez-Rentería, C.; et al. Characterizing environmental suitability of Aedes albopictus (Diptera: Culicidae) in Mexico based on regional and global niche models. J. Med. Entomol. 2018, 55, 69–77. [Google Scholar] [CrossRef]
- Machado-Machado, E.A. Empirical mapping of suitability to dengue fever in Mexico using species distribution modeling. Appl. Geogr. 2012, 33, 82–93. [Google Scholar] [CrossRef]
- Hernandez-Avila, J.E.; Rodriguez, M.H.; Santos-Luna, R.; Sanchez-Castaneda, V.; Roman-Perez, S.; Rios-Salgado, V.H.; Salas-Sarmiento, J.A. Nation-wide, web-based, geographic information system for the integrated surveillance and control of dengue fever in Mexico. PLoS ONE 2013, 8, e70231. [Google Scholar] [CrossRef] [Green Version]
- Hurtado-Diaz, M.; Riojas-Rodriguez, H.; Rothenberg, S.J.; Gomez-Dantes, H.; Cifuentes, E. Short communication: Impact of climate variability on the incidence of dengue in Mexico. Trop. Med. Int. Health 2007, 12, 1327–1337. [Google Scholar] [CrossRef]
- Manrique-Saide, P.; Coleman, P.; McCall, P.J.; Lenhart, A.; Vazquez-Prokopec, G.; Davies, C.R. Multi-scale analysis of the associations among egg, larval and pupal surveys and the presence and abundance of adult female Aedes aegypti (Stegomyia aegypti) in the city of Merida, Mexico. Med. Vet. Entomol. 2014, 28, 264–272. [Google Scholar] [CrossRef]
- Hunsberger, S.; Ortega-Villa, A.M.; Powers, J.H., 3rd; Rincon Leon, H.A.; Sosa, S.C.; Ruiz Hernandez, E.; Cancino, J.G.; Nason, M.; Lumbard, K.; Sepulveda, J.; et al. Patterns of signs, symptoms and laboratory values associated with Zika, dengue and undefined acute illnesses in a dengue endemic region: Secondary analysis of a prospective cohort study in southern Mexico. Int. J. Infect. Dis. 2020, 98, 241–248. [Google Scholar] [CrossRef]
- Haque, U.; Ball, J.D.; Zhang, W.; Khan, M.M.H.; Trevino, C.J. Clinical and spatial features of Zika virus in Mexico. Acta Trop. 2016, 162, 5–10. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Dengue and Severe Dengue; World Health Organization, Regional Office for the Eastern Mediterranean: Geneva, Switzerland, 2014. [Google Scholar]
- Beltrán-Silva, S.; Chacón-Hernández, S.; Moreno-Palacios, E.; Pereyra-Molina, J.A. Clinical and differential diagnosis: Dengue, chikungunya and Zika. Revista Médica del Hospital General de México 2018, 81, 146–153. [Google Scholar] [CrossRef]
- Tantawichien, T.J.P. Dengue fever and dengue haemorrhagic fever in adolescents and adults. Paediatr. Int. Child Health 2012, 32, 22–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srikiatkhachorn, A. Plasma leakage in dengue hemorrhagic fever. Thromb. Haemost. 2009, 102, 1042. [Google Scholar] [PubMed]
- Colombo, T.E.; Estofolete, C.F.; Reis, A.F.N.; da Silva, N.S.; Aguiar, M.L.; Cabrera, E.M.S.; Dos Santos, I.N.; Costa, F.R.; Cruz, L.E.; Rombola, P.L.; et al. Clinical, laboratory and virological data from suspected ZIKV patients in an endemic arbovirus area. J. Clin. Virol. 2017, 96, 20–25. [Google Scholar] [CrossRef]
- Garcell, H.G.; García, F.G.; Nodal, M.R.; Lozano, A.R.; Díaz, C.R.P.; Valdés, A.G.; Alvarez, L.G. Clinical relevance of Zika symptoms in the context of a Zika Dengue epidemic. J. Infect. Public Health 2020, 13, 173–176. [Google Scholar] [CrossRef]
- Dantés, H.G.; Farfán-Ale, J.A.; Sarti, E. Epidemiological trends of dengue disease in Mexico (2000–2011): A systematic literature search and analysis. PLoS Negl. Trop. Dis. 2014, 8, e3158. [Google Scholar] [CrossRef] [Green Version]
- Chakravarti, A.; Roy, P.; Malik, S.; Siddiqui, O.; Thakur, P. A study on gender-related differences in laboratory characteristics of dengue fever. Indian J. Med. Microbiol. 2016, 34, 82–84. [Google Scholar] [CrossRef]
- Kumar, M.; Verma, R.K.; Mishra, B. Prevalence of Dengue Fever in Western Uttar Pradesh, India: A Gender-Based Study. Int. J. Appl. Basic Med. Res. 2020, 10, 8–11. [Google Scholar]
- Jaenisch, T.; Tam, D.T.; Kieu, N.T.; Van Ngoc, T.; Nam, N.T.; Van Kinh, N.; Yacoub, S.; Chanpheaktra, N.; Kumar, V.; See, L.L.; et al. Clinical evaluation of dengue and identification of risk factors for severe disease: Protocol for a multicentre study in 8 countries. BMC Infect Dis. 2016, 16, 120. [Google Scholar] [CrossRef] [Green Version]
- Nava-Frías, M.; Searcy-Pavía, R.E.; Juárez-Contreras, C.A.; Valencia-Bautista, A. Enfermedad por virus de chikungunya: Actualidad en México. Boletín médico del Hospital Infantil de México 2016, 73, 67–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navarrete-Espinosa, J.; Acevedo-Vales, J.A.; Huerta-Hernández, E.; Torres-Barranca, J.; Gavaldón-Rosas, D. Prevalence of dengue and leptospira antibodies in the state of Veracruz, Mexico. Salud publica de Mexico 2006, 48, 220–228. [Google Scholar] [CrossRef] [Green Version]
- Ang, L.W.; Kam, Y.W.; Lin, C.; Krishnan, P.U.; Tay, J.; Ng, L.C.; James, L.; Lee, V.J.; Goh, K.T.; Ng, L.F.; et al. Seroprevalence of antibodies against chikungunya virus in Singapore resident adult population. PLoS Negl. Trop. Dis. 2017, 11, e0006163. [Google Scholar] [CrossRef] [PubMed]
- Levorato, C.D.; de Mello, L.M.; da Silva, A.S.; Nunes, A.A. Factors associated with the demand for health services from a gender-relational perspective. Cienc. Saude Coletiva 2014, 19, 1263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wenham, C.; Nunes, J.; Correa Matta, G.; de Oliveira Nogueira, C.; Aparecida Valente, P.; Pimenta, D. Gender mainstreaming as a pathway for sustainable arbovirus control in Latin America. PLoS Negl. Trop. Dis. 2020, 14, e0007954. [Google Scholar] [CrossRef]
- Tiguman, G.M.B.; Silva, M.T.; Souza, K.M.; Galvao, T. Prevalence of self-reported dengue infections in Manaus Metropolitan Region: A cross-sectional study. Rev. Soc. Bras. Med. Trop. 2019, 52. [Google Scholar] [CrossRef]
- Thai, K.T.; Nishiura, H.; Hoang, P.L.; Tran, N.T.; Phan, G.T.; Le, H.Q.; Tran, B.Q.; Van Nguyen, N.; de Vries, P.J. Age-specificity of clinical dengue during primary and secondary infections. PLoS Negl. Trop. Dis. 2011, 5, e1180. [Google Scholar] [CrossRef]
- Hammon, W.M. Dengue hemorrhagic fever--do we know its cause? Am. J. Trop. Med. Hyg. 1973, 22, 82–91. [Google Scholar] [CrossRef]
- Zambrana, J.V.; Carrillo, F.B.; Burger-Calderon, R.; Collado, D.; Sanchez, N.; Ojeda, S.; Monterrey, J.C.; Plazaola, M.; Lopez, B.; Arguello, S.; et al. Seroprevalence, risk factor, and spatial analyses of Zika virus infection after the 2016 epidemic in Managua, Nicaragua. Proc. Natl. Acad. Sci. USA 2018, 115, 9294–9299. [Google Scholar] [CrossRef] [Green Version]
- Halstead, S.B. Global epidemiology of dengue hemorrhagic fever. Southeast Asian J. Trop. Med. Public Health 1990, 21, 636–641. [Google Scholar]
- Rosen, L. The Emperor’s New Clothes revisited, or reflections on the pathogenesis of dengue hemorrhagic fever. Am. J. Trop. Med. Hyg. 1977, 26, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Halstead, S.B. Pathogenesis of dengue: Challenges to molecular biology. Science 1988, 239, 476–481. [Google Scholar] [CrossRef] [PubMed]
- Grajales-Muñiz, C.; Borja-Aburto, V.H.; Cabrera-Gaytán, D.A.; Rojas-Mendoza, T.; Arriaga-Nieto, L.; Vallejos-Parás, A. Zika virus: Epidemiological surveillance of the Mexican Institute of Social Security. PLoS ONE 2019, 14, e0212114. [Google Scholar] [CrossRef]
- Menchaca-Armenta, I.; Ocampo-Torres, M.; Hernández-Gómez, A.; Zamora-Cerritos, K. Risk perception and level of knowledge of diseases transmitted by Aedes aegypti. Rev. Inst. Med. Trop. São Paulo 2018, 60, e10. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.S.; Karamehic-Muratovic, A.; Baghbanzadeh, M.; Amrin, M.; Zafar, S.; Rahman, N.N.; Shirina, S.U.; Haque, U. Climate change and dengue fever knowledge, attitudes and practices in Bangladesh: A social media–based cross-sectional survey. Trans. R. Soc. Trop. Med. Hyg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Jimenez Corona, M.E.; De la Garza Barroso, A.L.; Rodriguez Martinez, J.C.; Luna Guzman, N.I.; Ruiz Matus, C.; Diaz Quinonez, J.A. Clinical and Epidemiological Characterization of Laboratory-Confirmed Autochthonous Cases of Zika Virus Disease in Mexico. PLoS Curr. 2016, 8. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadística y Geografía [INEGI] (2020). México en Cifras. Available online: https://www.inegi.org.mx/app/areasgeograficas/?ag=00 (accessed on 15 July 2020).
- SSA-InDRE. Lineamientos Para la Vigilancia por Laboratorio del Dengue y Otras Arbovirosis. 2019. Available online: https://www.gob.mx/salud/documentos/lineamientos-vigentes-red-nacional-de-laboratorios-de-salud-publica (accessed on 1 September 2020).
- Cabanas, M.; Nuño, J.P. A Mexican Flower Cluster: Strategy and Industrial Engineering. Proceedings 2013, 2013, 2065–2073. [Google Scholar]
- Delgado-Enciso, I.; López-Lemus, U.A.; Valcarcel-Gamiño, J.A.; Rodriguez-Sanchez, I.P.; Valle-Reyes, S.; Martinez-Fierro, M.L.; Melnikov, V.; Guzmán-Esquivel, J.; Vaca-Paniagua, F.; Valdez-Velazquez, L.L.; et al. Dengue virus-1 NS5 genetic variant associated with a severe clinical infection: Possible reduction of the innate immune response by inhibition of interferon type 1 and the Janus kinase-signal transducer and activator of transcription signaling pathway. Int. J. Mol. Med. 2018, 41, 2263–2269. [Google Scholar] [CrossRef]
- Perez-Ramirez, G.; Diaz-Badillo, A.; Camacho-Nuez, M.; Cisneros, A.; de Lourdes Munoz, M. Multiple recombinants in two dengue virus, serotype-2 isolates from patients from Oaxaca, Mexico. BMC Microbiol. 2009, 9, 260. [Google Scholar] [CrossRef] [Green Version]
- Espinoza-Gómez, F.; Delgado-Enciso, I.; Valle-Reyes, S.; Vásquez, C.; López-Lemus, U. Dual infection with dengue virus serotype 1 and 2 in a patient in Western Mexico. J. Glob. Infect. Dis. 2017, 9, 164–165. [Google Scholar]
- De Figueiredo, R.M.; Naveca, F.G.; Oliveira, C.M.; Bastos, M.d.S.; Mourão, M.P.G.; Viana, S.d.S.; Melo, M.D.; Itapirema, E.F.; Saatkamp, C.J.; Farias, I.P. Co-infection of Dengue virus by serotypes 3 and 4 in patients from Amazonas, Brazil. Rev. Inst. Med. Trop. São Paulo 2011, 53, 321–323. [Google Scholar] [CrossRef]




| Dengue (N = 264,273) | Chikungunya (N = 305) | Zika (N = 10,319) | |
|---|---|---|---|
| Sex N (%) | |||
| Female | 145,878 (55) | 186 (61) | 154,809 (56) |
| Male | 118,389 (45) | 119 (39) | 120,082 (44) |
| Age in years Mean (SD) | 26 (18.7) | 33 (19.1) | 28 (12.4) |
| Pregnancy N (%) | |||
| Yes | 5696 (13.30) | 10 (13.5) | 5476 (67) |
| No | 37,137 (86.7) | 64 (86.5) | 2691 (33) |
| Region N (%) | |||
| 1 (North west) | 26,921 (10) | 26 (9) | 710 (7) |
| 2 (North east) | 28,894 (11) | 7 (2) [Ref] * | 1215 (12) |
| 3 (Center west) | 50,779 (20) | 23 (8) | 639 (6) [Ref] * |
| 4 (Center) | 22,324 (9) [Ref] * | 11 (4) | 2110 (21) |
| 5 (South east) | 129,976 (50) | 235 (78) | 5481 (54) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ananth, S.; Shrestha, N.; Treviño C., J.A.; Nguyen, U.-s.; Haque, U.; Angulo-Molina, A.; Lopez-Lemus, U.A.; Lubinda, J.; Sharif, R.M.; Zaki, R.A.; et al. Clinical Symptoms of Arboviruses in Mexico. Pathogens 2020, 9, 964. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens9110964
Ananth S, Shrestha N, Treviño C. JA, Nguyen U-s, Haque U, Angulo-Molina A, Lopez-Lemus UA, Lubinda J, Sharif RM, Zaki RA, et al. Clinical Symptoms of Arboviruses in Mexico. Pathogens. 2020; 9(11):964. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens9110964
Chicago/Turabian StyleAnanth, Sushmitha, Nistha Shrestha, Jesús A. Treviño C., Uyen-sa Nguyen, Ubydul Haque, Aracely Angulo-Molina, Uriel A. Lopez-Lemus, Jailos Lubinda, Rashed Md. Sharif, Rafdzah Ahmad Zaki, and et al. 2020. "Clinical Symptoms of Arboviruses in Mexico" Pathogens 9, no. 11: 964. https://0-doi-org.brum.beds.ac.uk/10.3390/pathogens9110964