
HA PEGylated Filler in Association with an Infrared Energy Device for the Treatment of Facial Skin Aging: 150 Day Follow-Up Data Report
 , , , ,
, , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Hyaluronic-Acid (HA)-Based Fillers
1.2. Infrared Radiation (IR) Device Used in the Study
2. Results
2.1. Hematoxylin and Eosin Staining
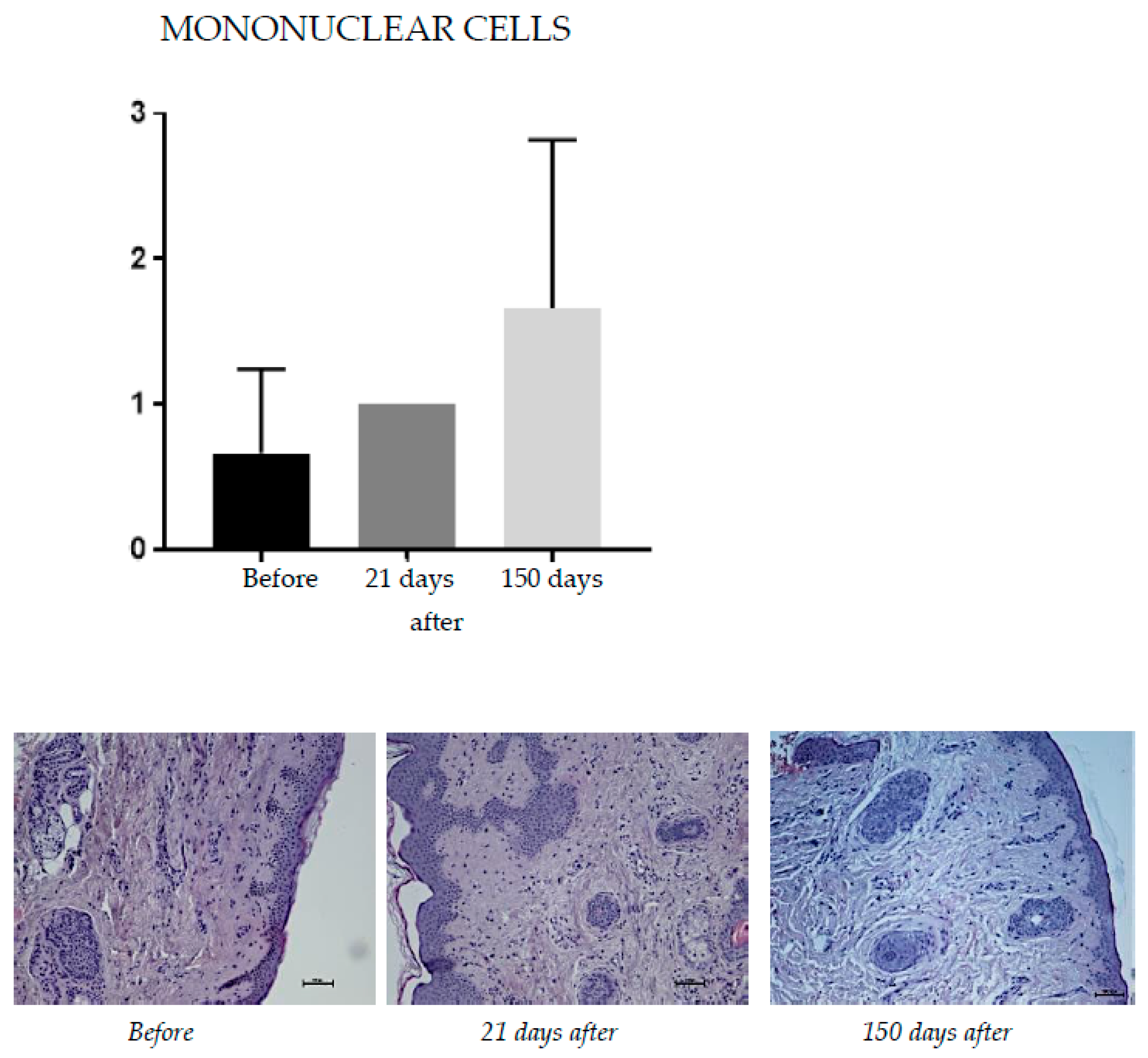
2.1.1. Mononuclear Cells
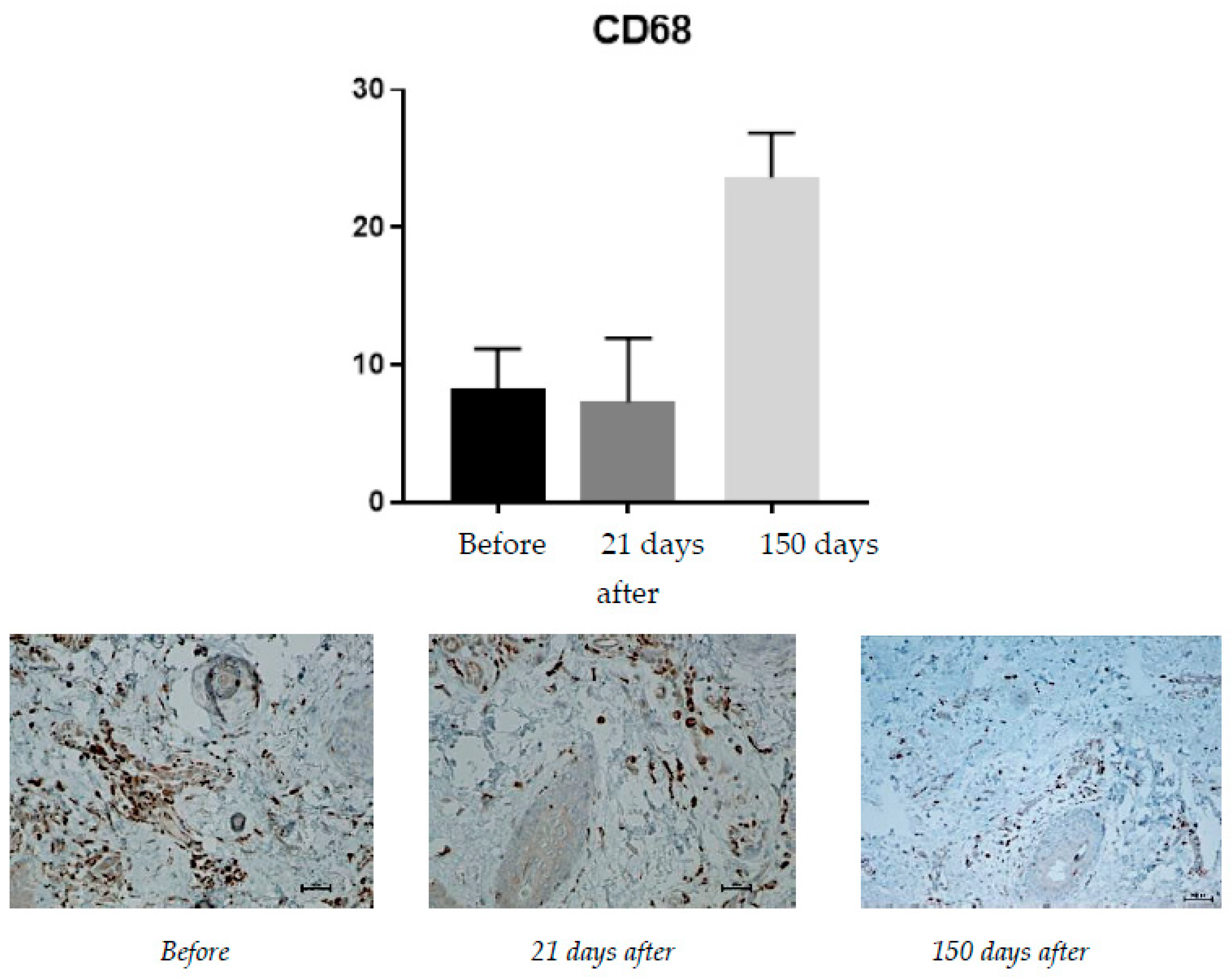
2.1.2. CD68 (Monocytes and Macrophages)
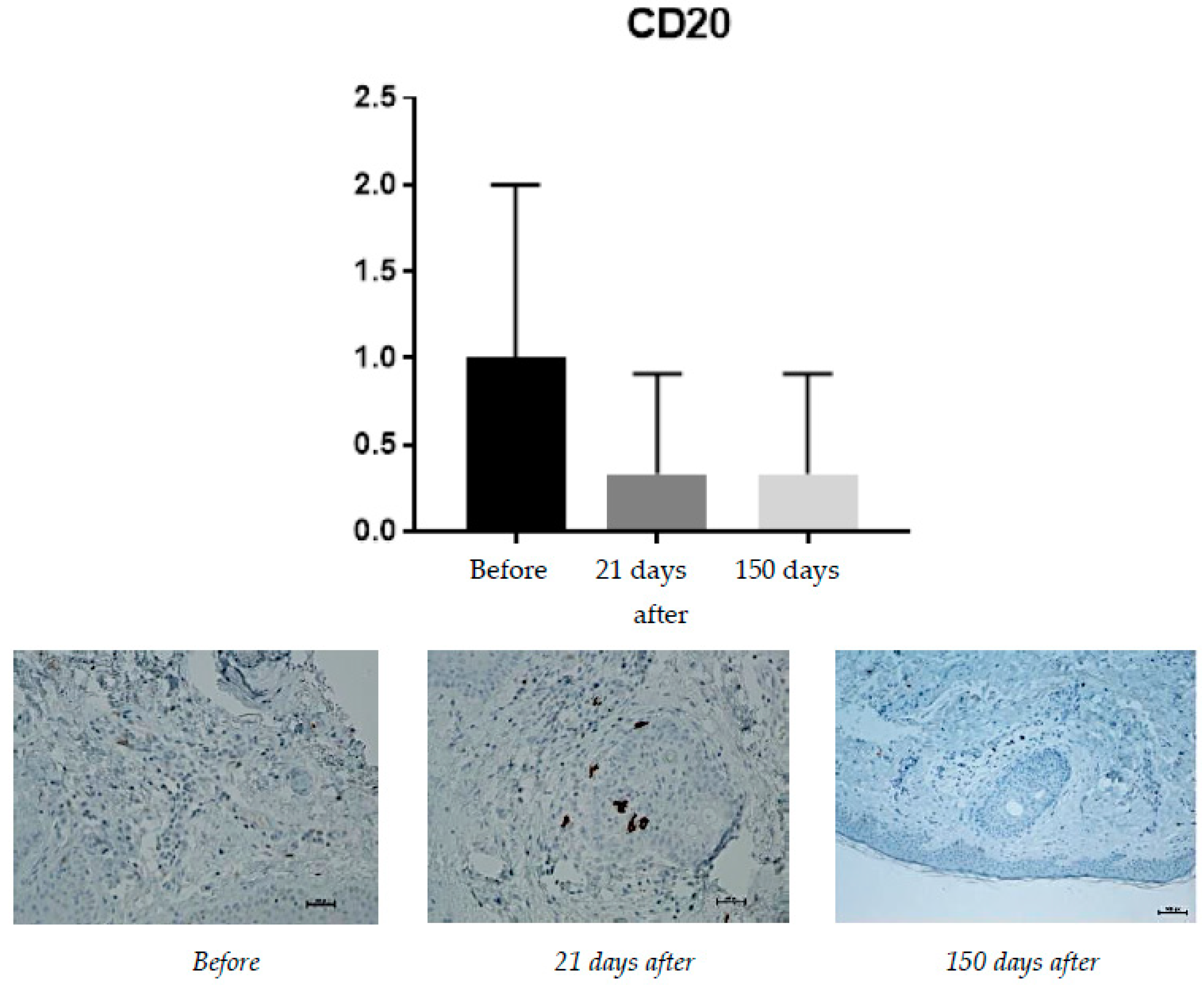
2.1.3. CD20 (B Lymphocytes)
2.1.4. CD8 (T Lymphocytes)
2.1.5. CD31 (PECAM-1)
2.1.6. Vimentin (Presence of Fibroblasts)
2.1.7. Masson’s Trichrome Staining
2.2. Cutometric Results
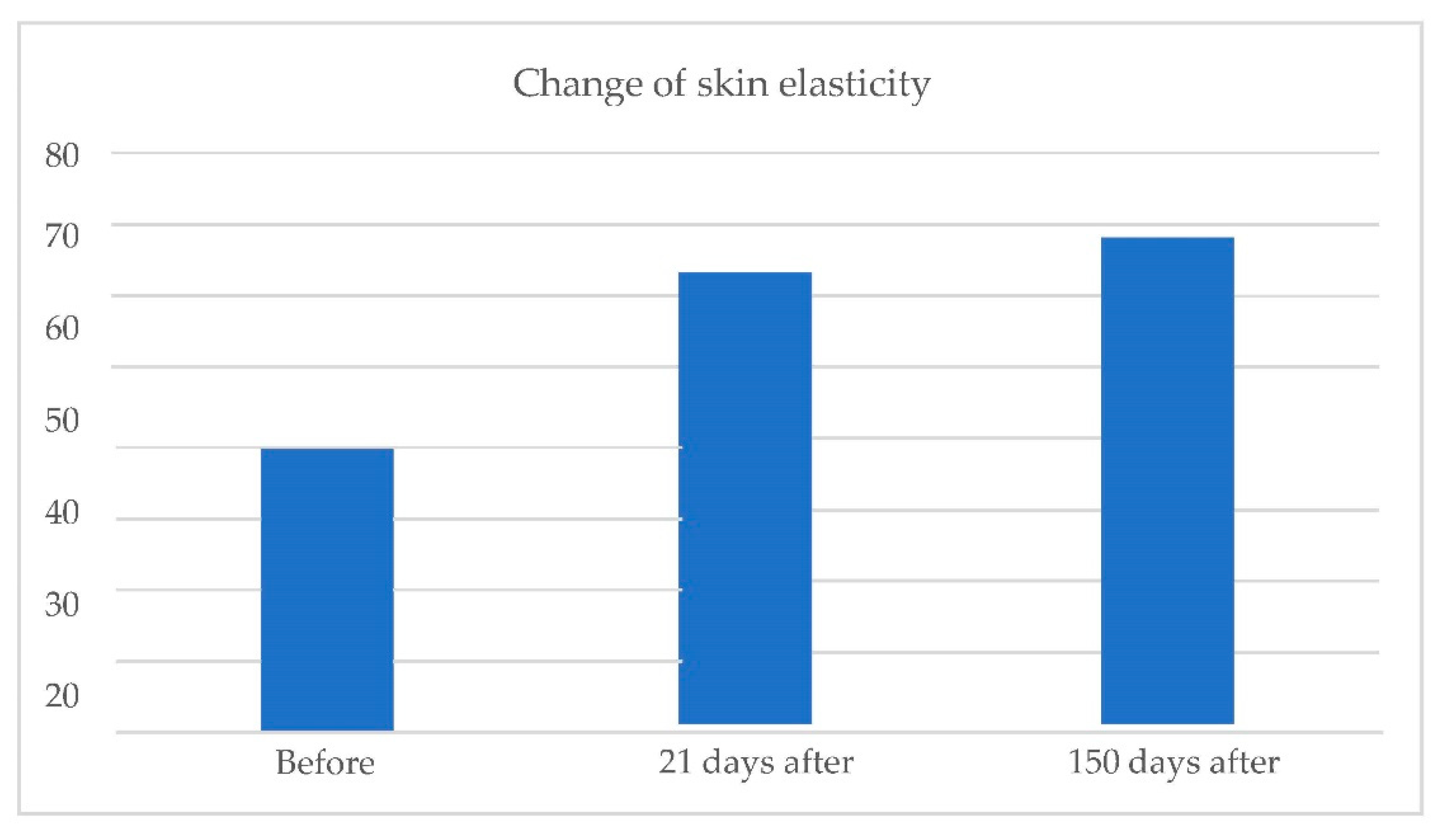
- Skin elasticity:
- Skin hydration:
3. Discussion
3.1. Immunohistochemical Staining Results
3.2. Cutometric Results
- Before the treatment, the average level of skin elasticity (on a scale of 0–100) was 57.70. It increased to 66.90 on day 21 and 59.030 at 150 days after the procedure.
- The average level of skin hydration (on a scale of 0–100) before the treatment was 56.10. After treatment, levels increased, achieving a level of 65.80 on day 21 and 67.07 at 150 days after the procedure.
- Before the treatment, the average level of skin elasticity (on a scale of 0–100) was 55.93. It increased to 69.83 on day 21 and 72.90 at 150 days after the procedure.
- An average level of skin hydration (on a scale of 0–100) before the treatment was 54.53. After treatment, levels increased, achieving a level of 56.83 on day 21 and 57.83 at 150 days after the procedure.
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cotofana, S.; Fratila, A.A.; Schenck, T.L.; Redka-Swoboda, W.; Zilinsky, I.; Pavicic, T. The Anatomy of the Aging Face: A Review. Facial Plast. Surg. 2016, 32, 253–260. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Liu, Y.; Zhao, Z.; Qiu, J. Oxidative stress in the skin: Impact and related protection. Int. J. Cosmet. Sci. 2021, 43, 495–509. [Google Scholar] [CrossRef]
- Landau, M.; Anand, C.V.; Besins, T.; Chao, Y.Y.Y.; Fabi, S.G.; Gout, U.; Kerscher, M.; Pavicic, T.; Peng, P.H.L.; Rzany, B.; et al. First consensus on primary prevention and early intervention in aesthetic medicine. J. Drugs Dermatol. 2017, 16, 846–854. [Google Scholar]
- Carruthers, J.; Burgess, C.; Day, D.; Fabi, S.G.; Goldie, K.; Kerscher, M.; Nikolis, A.; Pavicic, T.; Rho, N.K.; Rzany, B.; et al. Consensus recommendations for combined aesthetic interventions in the face using botulinum toxin, fillers, and energy-based devices. Dermatol. Surg. 2016, 42, 586–597. [Google Scholar] [CrossRef]
- Fabi, S.G.; Burgess, C.; Carruthers, A.; Carruthers, J.; Day, D.; Goldie, K.; Kerscher, M.; Nikolis, A.; Pavicic, T.; Rho, N.K.; et al. Consensus recommendations for combined aesthetic interventions using botulinum toxin, fillers, and microfocused ultrasound in the neck, décolletage, hands, and other areas of the body. Dermatol. Surg. 2016, 42, 1199–1208. [Google Scholar] [CrossRef]
- Fabi, S.; Pavicic, T.; Braz, A.; Green, J.B.; Seo, K.; van Loghem, J.A. Combined aesthetic interventions for prevention of facial ageing, and restoration and beautification of face and body. Clin. Cosmet. Investig. Dermatol. 2017, 10, 423–429. [Google Scholar] [CrossRef] [Green Version]
- Kapoor, K.M.; Saputra, D.I.; Porter, C.E.; Colucci, L.; Stone, C.; Brenninkmeijer, E.E.A.; Sloane, J.; Sayed, K.; Winaya, K.K.; Bertossi, D. Treating Aging Changes of Facial Anatomical Layers with Hyaluronic Acid Fillers. Clin. Cosmet. Investig. Dermatol. 2021, 14, 1105–1118. [Google Scholar] [CrossRef]
- Bass, L.S. Injectable Filler Techniques for Facial Rejuvenation, Volumization, and Augmentation. Facial Plast. Surg. Clin. N. Am. 2015, 23, 479–488. [Google Scholar] [CrossRef]
- Mehta-Ambalal, S.R. Neocollagenesis and Neoelastinogenesis: From the Laboratory to the Clinic. J. Cutan. Aesthet. Surg. 2016, 9, 145–151. [Google Scholar] [CrossRef]
- Solish, N.; Bertucci, V.; Percec, I.; Wagner, T.; Nogueira, A.; Mashburn, J. Dynamics of hyaluronic acid fillers formulated to maintain natural facial expression. J. Cosmet. Dermatol. 2019, 18, 738–746. [Google Scholar] [CrossRef]
- Bukhari, S.N.A.; Roswandi, N.L.; Waqas, M.; Habib, H.; Hussain, F.; Khan, S.; Sohail, M.; Ramli, N.A.; Thu, H.E.; Hussain, Z. Hyaluronic acid, a promising skin rejuvenating biomedicine: A review of recent updates and pre-clinical and clinical investigations on cosmetic and nutricosmetic effects. Int. J. Biol. Macromol. 2018, 120 Pt B, 1682–1695. [Google Scholar] [CrossRef]
- Barolet, D. Near-Infrared Light and Skin: Why Intensity Matters. Curr. Probl. Dermatol. 2021, 55, 374–384. [Google Scholar] [CrossRef]
- Iwayama, T.; Hashikawa, K.; Osaki, T.; Yamashiro, K.; Horita, N.; Fukumoto, T. Ultrasonography-guided Cannula Method for Hyaluronic Acid Filler Injection with Evaluation using Laser Speckle Flowgraphy. Plast. Reconstr. Surg. Glob. Open 2018, 6, e1776. [Google Scholar] [CrossRef] [PubMed]
- Koren, A.; Isman, G.; Cohen, S.; Bar Ilan, E.; Salameh, F.; Sprecher, E.; Artzi, O. Efficacy of a combination of diluted calcium hydroxylapatite-based filler and an energy-based device for the treatment of facial atrophic acne scars. Clin. Exp. Dermatol. 2019, 44, e171–e176. [Google Scholar] [CrossRef] [PubMed]
- Zerbinati, N.; D’Este, E.; Farina, A.; Rauso, R.; Cherubino, M.; Calligaro, A. Morphological evidence following pegylated filler treatment in human skin. J. Biol. Regul. Homeost. Agents 2017, 31 (Suppl. 2), 79–85. [Google Scholar]
- Zerbinati, N.; Haddad, R.G.; Bader, A.; Rauso, R.; D’Este, E.; Cipolla, G.; Calligaro, A.; Gonzalez, P.; Salvatore, S.; Serafin, D. A new hyaluronic acid polymer in the augmentation and restoration of labia majora. J. Biol. Regul. Homeost. Agents 2017, 31 (Suppl. 2), 153–161. [Google Scholar]
- Zerbinati, N.; Rauso, R.; Gonzalez, P.; Cherubino, M.; D’Este, E.; Calligaro, A.; Sommatis, S.; Maccario, C.; Mocchi, R. In vitro evaluation of collagen production on human fibroblasts treated with hyaluronic acid peg cross-linked with micromolecules of calcium hydroxyapatite in low concentration. J. Biol. Regul. Homeost. Agents 2017, 31 (Suppl. 2), 87–90. [Google Scholar]
- Knopf-Marques, H.; Pravda, M.; Wolfova, L.; Velebny, V.; Schaaf, P.; Vrana, N.E.; Lavalle, P. Hyaluronic Acid and Its Derivatives in Coating and Delivery Systems: Applications in Tissue Engineering, Regenerative Medicine and Immunomodulation. Adv. Healthc. Mater. 2016, 5, 2841–2855. [Google Scholar] [CrossRef]
- Firlar, I.; Altunbek, M.; McCarthy, C.; Ramalingam, M.; Camci-Unal, G. Functional Hydrogels for Treatment of Chronic Wounds. Gels 2022, 8, 127. [Google Scholar] [CrossRef]
- Baspeyras, M.; Rouvrais, C.; Liégard, L.; Delalleau, A.; Letellier, S.; Bacle, I.; Courrech, L.; Murat, P.; Mengeaud, V.; Schmitt, A.M. Clinical and biometrological efficacy of a hyaluronic acid-based mesotherapy product: A randomised controlled study. Arch. Dermatol. Res. 2013, 305, 673–682. [Google Scholar] [CrossRef] [Green Version]
- Heydenrych, I.; De Boulle, K.; Kapoor, K.M.; Bertossi, D. The 10-Point Plan 2021: Updated Concepts for Improved Procedural Safety During Facial Filler Treatments. Clin. Cosmet. Investig. Dermatol. 2021, 14, 779–814. [Google Scholar] [CrossRef] [PubMed]
- Jin, R.; Teixeira, L.M.; Krouwels, A.; Dijkstra, P.J.; Van Blitterswijk, C.A.; Karperien, M.; Feijen, J. Synthesis and characterization of hyaluronic acid-poly(ethylene glycol) hydrogels via Michael addition An injectable biomaterial for cartilage repair. Acta Biomater. 2010, 6, 1968–1977. [Google Scholar] [CrossRef] [PubMed]
- Zerbinati, N.; Rauso, R.; Protasoni, M.; D’Este, E.; Esposito, C.; Lotti, T.; Tirant, M.; Van Thuong, N.; Mocchi, R.; Zerbinati, U.; et al. Pegylated hyaluronic acid filler enriched with calcium hydroxyapatite treatment of human skin: Collagen renewal demonstrated through morphometric computerized analysis. J. Biol. Regul. Homeost. Agents 2019, 33, 1967–1971. [Google Scholar] [CrossRef] [PubMed]
- Leach, J.B.; Schmidt, C.E. Characterization of protein release from photocrosslinkable hyaluronic acid- polyethylene glycol hydrogel tissue engineering scaffolds. Biomaterials 2005, 26, 125–135. [Google Scholar] [CrossRef]
- Hassan, W.; Dong, Y.; Wang, W. Encapsulation and 3D culture of human adipose-derived stem cells in an in- situ cross-linked hybrid hydrogel composed of PEG-based hyperbranched copolymer and hyaluronic acid. Stem Cell Res. Ther. 2013, 4, 32–43. [Google Scholar] [CrossRef] [Green Version]
- Russo, M.; Grimaldi, A.M.; Bevilacqua, P.; Tammaro, O.; Netti, P.A.; Torino, E. PEGylated crosslinked hyaluronic acid nanoparticles designed through a microfluidic platform for nanomedicine. Nanomedicine 2017, 12, 2211–2222. [Google Scholar] [CrossRef]
- Zhang, Q.; Deng, C.; Fu, Y.; Sun, X.; Gong, T.; Zhang, Z. Repeated Administration of Hyaluronic Acid Coated Liposomes with Improved Pharmacokinetics and Reduced Immune Response. Mol. Pharm. 2016, 13, 1800–1808. [Google Scholar] [CrossRef]
- Bayer, I.S. Hyaluronic Acid and Controlled Release: A Review. Molecules 2020, 25, 2649. [Google Scholar] [CrossRef]
- Sabat, R.; Wolk, K.; Loyal, L.; Döcke, W.D.; Ghoreschi, K. T cell pathology in skin inflammation. Semin. Immunopathol. 2019, 41, 359–377. [Google Scholar] [CrossRef] [Green Version]
- Castillo-González, R.; Cibrian, D.; Fernández-Gallego, N.; Ramírez-Huesca, M.; Saiz, M.L.; Navarro, M.N.; Fresno, M.; de la Fuente, H.; Sánchez-Madrid, F. Galectin-1 Expression in CD8+ T Lymphocytes Controls Inflammation in Contact Hypersensitivity. J. Investig. Dermatol. 2021, 141, 1522–1532.e3. [Google Scholar] [CrossRef]
- Thorpe, R.B.; Gray, A.; Kumar, K.R.; Susa, J.S.; Chong, B.F. Site-Specific Analysis of Inflammatory Markers in Discoid Lupus Erythematosus Skin. Sci. World J. 2014, 2014, 925805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosello, S.; Angelucci, C.; Lama, G.; Alivernini, S.; Proietti, G.; Tolusso, B.; Sica, G.; Gremese, E.; Ferraccioli, G. Characterization of inflammatory cell infiltrate of scleroderma skin: B cells and skin score progression. Arthritis Res. Ther. 2018, 20, 75. [Google Scholar] [CrossRef] [PubMed]
- Tellechea, A.; Kafanas, A.; Leal, E.; Tecilazich, F.; Kuchibhotla, S.; Auster, M.E.; Kontoes, I.; Paolino, J.; Carvalho, E.; Nabzdyk, L.P.; et al. Increased skin inflammation and blood vessel density in human and experimental diabetes. Int. J. Low. Extrem. Wounds 2013, 12, 4–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sliogeryte, K.; Gavara, N. Vimentin Plays a Crucial Role in Fibroblast Ageing by Regulating Biophysical Properties and Cell Migration. Cells 2019, 8, 1164. [Google Scholar] [CrossRef] [PubMed]









Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kubik, P.; Jankau, J.; Rauso, R.; Galadari, H.; Protasoni, M.; Gruszczyński, W.; Grzanka, D.; Smolińska, M.; Antosik, P.; Piesiaków, M.-L.; et al. HA PEGylated Filler in Association with an Infrared Energy Device for the Treatment of Facial Skin Aging: 150 Day Follow-Up Data Report. Pharmaceuticals 2022, 15, 1355. https://0-doi-org.brum.beds.ac.uk/10.3390/ph15111355
Kubik P, Jankau J, Rauso R, Galadari H, Protasoni M, Gruszczyński W, Grzanka D, Smolińska M, Antosik P, Piesiaków M-L, et al. HA PEGylated Filler in Association with an Infrared Energy Device for the Treatment of Facial Skin Aging: 150 Day Follow-Up Data Report. Pharmaceuticals. 2022; 15(11):1355. https://0-doi-org.brum.beds.ac.uk/10.3390/ph15111355
Chicago/Turabian StyleKubik, Paweł, Jerzy Jankau, Raffaele Rauso, Hassan Galadari, Marina Protasoni, Wojciech Gruszczyński, Dariusz Grzanka, Marta Smolińska, Paulina Antosik, Maria-Luiza Piesiaków, and et al. 2022. "HA PEGylated Filler in Association with an Infrared Energy Device for the Treatment of Facial Skin Aging: 150 Day Follow-Up Data Report" Pharmaceuticals 15, no. 11: 1355. https://0-doi-org.brum.beds.ac.uk/10.3390/ph15111355