
Ondansetron Reduces the Incidence of Hypotension after Spinal Anaesthesia: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Methods
2.1. Systematic Literature Search
2.2. Criteria for Selection
2.3. Extraction of Data and Outcomes
2.4. Evaluation of the Quality and the Risk of Bias
2.5. Statistical Analysis
3. Results and Discussion
3.1. Search Results
3.2. Study Characteristics
3.3. Assessment of Bias
3.4. The Incidence of Hypotension
3.5. The Incidence of Bradycardia
3.6. Rescue of Vasopressor Administration
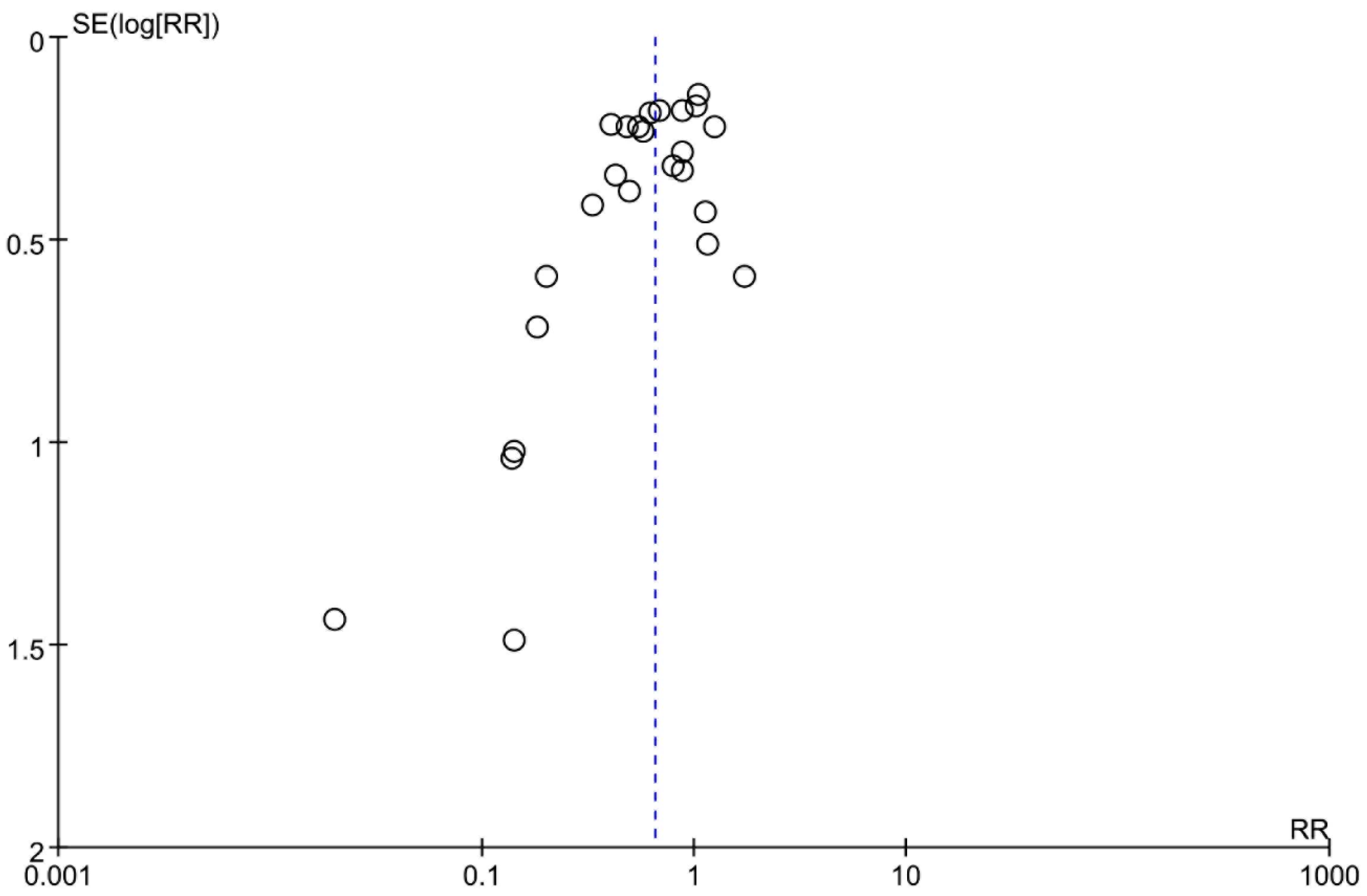
3.7. Publication Bias and Sensitivity Analysis
3.8. Trial Sequential Analysis
3.9. Grade Evaluation
3.10. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pereira, I.D.F.; Grando, M.M.; Vianna, P.T.; Braz, J.R.; Castiglia, Y.M.; Vane, L.A.; Módolo, N.S.P., Jr.; do Nascimento, P., Jr.; Amorim, R.B.; Rolim Rodrigues, G., Jr.; et al. Retrospective analysis of risk factors and predictors of intraoperative complications in neuraxial blocks at Faculdade de Medicina de Botucatu-UNESP. Rev. Bras. Anestesiol. 2011, 61, 844–866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marashi, S.M.; Soltani-Omid, S.; Soltani Mohammadi, S.; Aghajani, Y.; Movafegh, A. Comparing Two Different Doses of Intravenous Ondansetron with Placebo on Attenuation of Spinal-induced Hypotension and Shivering. Anesthesiol. Pain Med. 2014, 4, e12055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinsella, S.M.; Tuckey, J.P. Perioperative bradycardia and asystole: Relationship to vasovagal syncope and the Bezold-Jarisch reflex. Br. J. Anaesth. 2001, 86, 859–868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinek, R.M. Witnessed asystole during spinal anesthesia treated with atropine and ondansetron: A case report. Can. J. Anaesth. J. Can. D’anesthesie 2004, 51, 226–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, C.M.; Chow, M.S.; Fan, C.; Kluger, J.; Bazunga, M. Efficacy of intravenous granisetron in suppressing the bradycardia and hypotension associated with a rabbit model of the Bezold-Jarisch reflex. J. Clin. Pharmacol. 1998, 38, 172–177. [Google Scholar] [CrossRef]
- Kannan, M.H.; Heggeri, V.M.; Kumaran, R.M. Ondansetron Attenuates Hypotension Due to Subarachnoid Block-A Randomised Double Blind, Placebo-Controlled Study. J. Res. Med. Dent. Sci. 2022, 10, 414–420. [Google Scholar]
- Xiao, F.; Wei, C.; Chang, X.; Zhang, Y.; Xue, L.; Shen, H.; Ngan, K.; Warwick, D.; Chen, X. A Prospective, Randomized, Double-Blinded Study of the Effect of Intravenous Ondansetron on the Effective Dose in 50% of Subjects of Prophylactic Phenylephrine Infusions for Preventing Spinal Anesthesia-Induced Hypotension During Cesarean Delivery. Anesth. Analg. 2020, 131, 564–569. [Google Scholar] [CrossRef]
- Attri, A.; Sharma, N.; Singh, M.R.; Bansal, K.; Singh, S. Effect of intravenous ondansetron on maternal hemodynamics during elective caesarean section under subarachnoid block. J. Obstet. Anaesth. Crit. Care 2019, 9, 94. [Google Scholar]
- Heesen, M.; Klimek, M.; Hoeks, S.E.; Rossaint, R. Prevention of Spinal Anesthesia-Induced Hypotension During Cesarean Delivery by 5-Hydroxytryptamine-3 Receptor Antagonists: A Systematic Review and Meta-analysis and Meta-regression. Anesth. Analg. 2016, 123, 977–988. [Google Scholar] [CrossRef] [Green Version]
- Tubog, D.T.; Bramble, R.S. Ondansetron reduces the incidence of hypotension after spinal anaesthesia in non-caesarean delivery: A systematic review and meta-analysis. J. Perioper. Pract. 2022, 32, 29–40. [Google Scholar] [CrossRef]
- Mohamed, S.; Befkadu, A.; Mohammed, A.; Neme, D.; Ahmed, S.; Yimer, Y.; Girma, T. Effectiveness of prophylactic ondansetron in preventing spinal anesthesia induced hypotension and bradycardia in pregnant mother undergoing elective cesarean delivery: A double blinded randomized control trial, 2021. Int. J. Surg. Open 2021, 35, 100401. [Google Scholar] [CrossRef]
- Mendonça, F.T.; Crepaldi, L.C., Jr.; Gersanti, R.C.; de Araújo, K.C. Effect of ondansetron on spinal anesthesia-induced hypotension in non-obstetric surgeries: A randomised, double-blind and placebo-controlled trial. Braz. J. Anesthesiol. 2021, 71, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Bhiwal, A.K.; Chauhan, K.; Choudhary, S.; Bhatt, H.A.; Gupta, S. Intravenous Ondansetron to Prevent Hypotension During Cesarean Section Under Spinal Anaesthesia. J. Obstet. Anaesth. Crit. Care 2021, 11, 15–19. [Google Scholar] [CrossRef]
- Patel, P.C.; Parmar, D.; Patel, U.; Shah, R.S. Comparison of Injection Granisetron versus Injection Ondansetron for Control of Intraoperative Nausea and Vomiting and Post-Operative Nausea and Vomiting among the Women Undergoing Lower Segment Caesarean Section under Spinal Anaesthesia. Adv. Hum. Biol. 2021, 11, 172–175. [Google Scholar]
- Wetterslev, J.; Jakobsen, J.C.; Gluud, C. Trial Sequential Analysis in systematic reviews with meta-analysis. BMC Med. Res. Methodol. 2017, 17, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogah, J.; Otegbeye, A.U. Attenuating Spinal-Induced Hypotension with Ondansetron in Parturients Undergoing Casarean Section. Anesth. Analg. 2021, 132, 596. [Google Scholar]
- Brahim, A.; Ben Lamine, F.; Abdelmoula, H.; Ben Jazia, K. Ondansetron, dexamethasone and their combination compared for the prevention of nausea and vomiting during a caesarean section under spinal anesthesia. Anesth. Analg. 2021, 133, 1030. [Google Scholar]
- Uerpairojkit, K.; Chesoh, A.; Budcharoentong, D. Ondansetron for Prophylaxis of Spinal Morphine Induced Nausea during Early Rooming in Breastfeeding: A Randomized Placebo Controlled Trial. Anesth. Analg. 2016, 123, 286–287. [Google Scholar] [CrossRef]
- Samarah, W.K.; Alghanem, S.M.; Bsisu, I.K.; Rahman, Z.A.; Guzu, H.A.; Abufares, B.N. The effect of ondansetron administration 20 minutes prior to spinal anaesthesia on haemodynamic status in patients undergoing elective caesarean section: A comparison between two different doses. Indian J. Anaesth. 2020, 64, 954–959. [Google Scholar]
- Moro, E.T.; Teixeira Ferreira, M.A.; dos Santos Goncalves, R.; Vargas, R.C.; Calil, S.J.; Soranz, M.A.; Bloomstone, J. The Quality of Recovery after Dexamethasone, Ondansetron, or Placebo Administration in Patients Undergoing Lower Limbs Orthopedic Surgery under Spinal Anesthesia Using Intrathecal Morphine. A Randomized Controlled Trial. Anesthesiol. Res. Pract. 2020, 2020, 9265698. [Google Scholar] [CrossRef]
- Hulchafo, A.; Abiy, S.; Shifa, S.; Yemam, D. Effectiveness of prophylactic intravenous ondasetron to reduce fentanyl induced pruritus among elective cesarean section patients in Worabe Comprehensive Specialized Hospital, Southern Ethiopia, 2020, randomized clinical trial. Int. J. Surg. Open 2020, 24, 52–56. [Google Scholar] [CrossRef]
- Rasooli, S.; Moslemi, F.; Gogazadeh, M. Preventing Nausea and Vomiting Using Ondansetron and Metoclopramide-Phenylephrine in Cesarean Section Using Spinal Anesthesia. Crescent J. Med. Biol. Sci. 2019, 6, 61–65. [Google Scholar]
- Oliveira Campos, G.; de Jesus Martins, M.; Jesus, G.N.; Rios de Oliveira, P.R.; Lessa, C.N.; Macedo Fernandes de Oliveira, J.C., Jr.; de Castro Alves, L.J.S.; Alves, R.L.; Módolo, N.S.P. Palonosetron versus ondansetron for prevention of nausea and vomiting after total abdominal hysterectomy under spinal anesthesia with intrathecal morphine: A double-blind, randomized controlled trial. BMC Anesthesiol. 2019, 19, 159. [Google Scholar]
- Shokrpour, M.; Homayuni, S.; Kamali, A.; Pazuki, S. Comparing the prophylactic effect of ondansetron and dexamethasone in controlling headaches caused by spinal anesthesia among women candidated for caesarean A randomized controlled trial. Electron. J. Gen. Med. 2018, 15, 6. [Google Scholar]
- Suman, B.R.; Umesh, R.; Rohan, B. A Comparative Study of Intravenous Ondansetron, Granisetron and Ramosetron for Prevention of Postoperative Nausea and Vomiting in Patients Undergoing Caesarean Section. J. Evol. Med. Dent. Sci.-JEMDS 2017, 6, 575–580. [Google Scholar] [CrossRef]
- Ghanei, M.; Damshenas, M.H.; Radmehr, M.; Kalani, N.; Rastgarian, A. Comparison of the Effects of Pethidine and Ondansetron in Prevention of Shivering after Spinal Anesthesia for Cesarean Section: A Double-Blind Clinical Trial. J. Fundam. Appl. Sci. 2017, 9, 1134–1142. [Google Scholar]
- Badawy, A.A.; Mokhtar, A.M. The role of ondansetron in prevention of post-spinal shivering (PSS) in obstetric patients: A double-blind randomized controlled trial. Egypt. J. Anaesth. 2017, 33, 29–33. [Google Scholar] [CrossRef] [Green Version]
- Rai, S.; Verma, S.; Pandey, H.P.; Yadav, P.; Patel, A. Role of butorphanol and ondansetron premedication in reducing postoperative shivering after general and spinal anesthesia: A randomized comparative study from North India. Anesth. Essays Res. 2016, 10, 319–323. [Google Scholar] [CrossRef] [Green Version]
- Moustafa, A.A.; Baaror, A.S.; Abdelazim, I.A. Comparative study between nalbuphine and ondansetron in prevention of intrathecal morphine-induced pruritus in women undergoing cesarean section. Anesth. Essays Res. 2016, 10, 238–244. [Google Scholar]
- Bommala, S.; Mukkara, M.; Samantaray, A.; Pasupuleti, H.; Reddycogu, D.M.; Pudotha, S.S.; Shravani, P.; Sathish. Effects of Intravenous Odansetron and Granisetron on Haemodynamic Changes during Spinal Anaesthesia in Non-obstetric Population: A Randomised Double Blind Study. J. Clin. Diagn. Res. 2019, 13, UC01–UC4. [Google Scholar]
- Haroon, M. Effectiveness of Prophylactic Venous Management of Ondansetron for Anticipation of Backbone Anesthesia Encouraged Hypotension in Aged Respondents. Indo Am. J. Pharm. Sci. 2019, 6, 11855–11858. [Google Scholar]
- Kelsaka, E.; Baris, S.; Karakaya, D.; Sarihasan, B. Comparison of ondansetron and meperidine for prevention of shivering in patients undergoing spinal anesthesia. Reg. Anesth. Pain Med. 2006, 31, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Marciniak, A.; Owczuk, R.; Wujtewicz, M.; Preis, K.; Majdyło, K. The influence of intravenous ondansetron on maternal blood haemodynamics after spinal anaesthesia for caesarean section: A double-blind, placebo-controlled study. Ginekol. Pol. 2015, 86, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, S.A.; Hussam, A.M.; Abdallah, S.A.; Sarhan, K.A.; Shaban, A.M. Ondansetron Is an Effective Alternative to Decrease the Incidence of Postspinal Hypotension in Healthy Subjects Undergoing Infra-Umbilical Surgeries Compared to Combined Volume Loading and Vasoconstrictors: Randomized Controlled Trial. Open Access Maced. J. Med. Sci. 2018, 6, 2363–2368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohammadzadeh Jouryabi, A.; Sharami, S.H.; Mansour Ghanaie, M.; Sedighinejad, A.; Imantalab, V.; Rafiee Sorouri, Z.; Biazar, G.; Nobijari, T.Z. Comparing the Effects of Low Dose of Ketamine, Tramadol, and Ondansetron in Prevention of Post Spinal Anesthesia Shivering in Cesarean Section. Anesthesiol. Pain Med. 2021, 11, e116429. [Google Scholar] [CrossRef] [PubMed]
- Nallam, S.R.; Cherukuru, K.; Sateesh, G. Efficacy of Intravenous Ondansetron for Prevention of Postspinal Shivering during Lower Segment Cesarean Section: A Double-Blinded Randomized Trial. Anesth. Essays Res. 2017, 11, 508–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortiz-Gómez, J.R.; Palacio-Abizanda, F.J.; Morillas-Ramirez, F.; Fornet-Ruiz, I.; Lorenzo-Jiménez, A.; Bermejo-Albares, M.L. The effect of intravenous ondansetron on maternal haemodynamics during elective caesarean delivery under spinal anaesthesia: A double-blind, randomised, placebo-controlled trial. Int. J. Obstet. Anesth. 2014, 23, 138–143. [Google Scholar] [CrossRef]
- Owczuk, R.; Wenski, W.; Polak-Krzeminska, A.; Twardowski, P.; Arszułowicz, R.; Dylczyk-Sommer, A.; Wujtewicz, M.A.; Sawicka, W.; Morzuch, E.; Smietanski, M.; et al. Ondansetron given intravenously attenuates arterial blood pressure drop due to spinal anesthesia: A double-blind, placebo-controlled study. Reg. Anesth. Pain Med. 2008, 33, 332–339. [Google Scholar]
- Owczuk, R.; Wenski, W.; Twardowski, P.; Dylczyk-Sommer, A.; Sawicka, W.; Wujtewicz, M.A.; Marciniak, A.; Polak-Krzemińska, A.; Jasiński, T.; Wujtewicz, M. Ondansetron attenuates the decrease in blood pressure due to spinal anesthesia in the elderly: A double blind, placebo-controlled study. Minerva Anestesiol. 2015, 81, 598–607. [Google Scholar]
- Pirat, A.; Tuncay, Ş.F.; Torgay, A.; Candan, S.; Arslan, G. Ondansetron, orally disintegrating tablets versus intravenous injection for prevention of intrathecal morphine-induced nausea, vomiting, and pruritus in young males. Anesth. Analg. 2005, 101, 1330–1336. [Google Scholar] [CrossRef]
- Ramon Ortiz-Gomez, J.; Javier Palacio-Abizanda, F.; Morillas-Ramirez, F.; Fornet-Ruiz, I.; Lorenzo-Jimenez, A.; Lourdes Bermejo-Albares, M. Reducing by 50% the incidence of maternal hypotension during elective caesarean delivery under spinal anesthesia: Effect of prophylactic ondansetron and/or continuous infusion of phenylephrine—A double-blind, randomized, placebo controlled trial. Saudi J. Anaesth. 2017, 11, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Rashad, M.M.; Farmawy, M.S. Effects of intravenous ondansetron and granisetron on hemodynamic changes and motor and sensory blockade induced by spinal anesthesia in parturients undergoing cesarean section. Egypt. J. Anaesth. 2013, 29, 369–374. [Google Scholar] [CrossRef]
- Safavi, M.; Honarmand, A.; Negahban, M.; Attari, M. Prophylactic effects of intrathecal Meperidine and intravenous Ondansetron on shivering in patients undergoing lower extremity orthopedic surgery under spinal anesthesia. J. Res. Pharm. Pract. 2014, 3, 94–99. [Google Scholar] [PubMed]
- Sahoo, T.; SenDasgupta, C.; Goswami, A.; Hazra, A. Reduction in spinal-induced hypotension with ondansetron in parturients undergoing caesarean section: A double-blind randomised, placebo-controlled study. Int. J. Obstet. Anesth. 2012, 21, 24–28. [Google Scholar] [CrossRef]
- Shakya, S.; Chaturvedi, A.; Sah, B.P. Prophylactic low dose ketamine and ondansetron for prevention of shivering during spinal anaesthesia. J. Anaesthesiol. Clin. Pharmacol. 2010, 26, 465–469. [Google Scholar]
- Tatikonda, C.M.; Rajappa, G.C.; Rath, P.; Abbas, M.; Madhapura, V.S.; Gopal, N.V. Effect of Intravenous Ondansetron on Spinal Anesthesia-Induced Hypotension and Bradycardia: A Randomized Controlled Double-Blinded Study. Anesth. Essays Res. 2019, 13, 340–346. [Google Scholar] [CrossRef]
- Terkawi, A.S.; Tiouririne, M.; Mehta, S.H.; Hackworth, J.M.; Tsang, S.; Durieux, M.E. Ondansetron Does Not Attenuate Hemodynamic Changes in Patients Undergoing Elective Cesarean Delivery Using Subarachnoid Anesthesia: A Double-Blind, Placebo-Controlled, Randomized Trial. Reg. Anesth. Pain Med. 2015, 40, 344–348. [Google Scholar] [CrossRef]
- Trabelsi, W.; Romdhani, C.; Elaskri, H.; Sammoud, W.; Bensalah, M.; Labbene, I.; Ferjani, M. Effect of Ondansetron on the Occurrence of Hypotension and on Neonatal Parameters during Spinal Anesthesia for Elective Caesarean Section: A Prospective, Randomized, Controlled, Double-Blind Study. Anesthesiol. Res. Pract. 2015, 2015, 158061. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.; Zhuo, L.; Wang, Q.; Shen, M.K.; Yu, Y.Y.; Yu, J.J.; Wang, Z.-P. Efficacy of prophylactic intravenous ondansetron on the prevention of hypotension during cesarean delivery: A dose-dependent study. Int. J. Clin. Exp. Med. 2014, 7, 5210–5216. [Google Scholar]
- Wang, Q.; Zhuo, L.; Shen, M.K.; Yu, Y.Y.; Yu, J.J.; Wang, M. Ondansetron preloading with crystalloid infusion reduces maternal hypotension during cesarean delivery. Am. J. Perinatol. 2014, 31, 913–922. [Google Scholar] [CrossRef]
- Chooi, C.; Cox, J.J.; Lumb, R.S.; Middleton, P.; Chemali, M.; Emmett, R.S.; Middleton, P.; Simmons, S.W. Techniques for preventing hypotension during spinal anaesthesia for caesarean section. Cochrane Database Syst. Rev. 2020, 7, Cd002251. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, J.P.; Fedoruk, K.A.; Jadin, S.M.; Carvalho, B.; Halpern, S.H. Prevention of hypotension after spinal anaesthesia for caesarean section: A systematic review and network meta-analysis of randomised controlled trials. Anaesthesia 2020, 75, 109–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eldaba, A.A.; Amr, Y.M. Intravenous granisetron attenuates hypotension during spinal anesthesia in cesarean delivery: A double-blind, prospective randomized controlled study. J. Anaesthesiol. Clin. Pharmacol. 2015, 31, 329–332. [Google Scholar]
- Tubog, T.D.; Kane, T.D.; Pugh, M.A. Effects of Ondansetron on Attenuating Spinal Anesthesia–Induced Hypotension and Bradycardia in Obstetric and Nonobstetric Subjects: A Systematic Review and Meta-Analysis. AANA J. 2017, 85, 113–122. [Google Scholar] [PubMed]
- Gao, L.; Zheng, G.; Han, J.; Wang, Y.; Zheng, J. Effects of prophylactic ondansetron on spinal anesthesia-induced hypotension: A meta-analysis. Int. J. Obstet. Anesth. 2015, 24, 335–343. [Google Scholar] [CrossRef]
- Heesen, M.; Stewart, A.; Fernando, R. Vasopressors for the treatment of maternal hypotension following spinal anaesthesia for elective caesarean section: Past, present and future. Anaesthesia 2015, 70, 252–257. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Sample Size | Type of Surgery | Patients | Blinded Method | Spinal Anaesthesia | Dosage of Ondansetron | Definition of Hypotension |
|---|---|---|---|---|---|---|---|
| Bhiwal 2021 [13] | O (4 mg): 48 | Caesarean section | ASA: I–II | Double-blinded | Position: left lateral | Ondansetron 4 mg or 8 mg before spinal anaesthesia | Reduction in SBP by > 20% from the baseline value. |
| O (8 mg): 50 | Age range: 18–40 | Local anaesthetic: 2 mL 0.5% hyperbaric bupivacaine at L 3–4 or L 4–5 | |||||
| Control: 50 | |||||||
| Bommala 2019 [30] | O (4 mg): 30 | Nonobstetric surgery | ASA: I–II | Double-blinded | Position: lateral decubitus | Ondansetron 4 mg before spinal anaesthesia | Reduction in SBP by > 30% from the baseline value or SBP < 90 mmHg. |
| Control: 30 | Age range: 18–60 | Local anaesthetic: 3 mL 0.5% hyperbaric bupivacaine at L 3–4 | |||||
| Haroon 2019 [31] | O (9 mg): 55 | NR | ASA: I–III | Double-blinded | Position: Sitting | Ondansetron 9 mg before spinal anaesthesia | Reduction in SBP by > 21% from the baseline value or SBP < 91 mmHg. |
| Control: 55 | Age range: 51–81 | Local anaesthetic: 17 mg 0.76% bupivacaine at L 4–5 | |||||
| Kelsaka 2006 [32] | O (8 mg): 25 | Orthopaedic surgery | ASA: I–II | Double-blinded | Position: lateral | Ondansetron 8 mg before spinal anaesthesia | Reduction in SBP by > 20% from the baseline value. |
| Control: 25 | Age range: 20–60 | Local anaesthetic: 2.5 mL 0.5% hyperbaric bupivacaine at L 3–4 | |||||
| Marashi 2014 [2] | O (6 mg):70 | Urologic, orthopaedic or gynaecologic surgeries | ASA: I–II | Double-blinded | Position: lateral | Ondansetron 6 mg or 12 mg before spinal anaesthesia | Reduction in MAP by > 20% from the baseline value or MAP < 80 mm Hg. |
| O (12 mg):70 | Age range: 20–50 | Local anaesthetic: 15 mg of 0.5% hypertonic bupivacaine at L 3–4 or L 4–5 | |||||
| Control: 70 | |||||||
| Rashad 2013 [42] | O (4 mg):20 | Caesarean section | ASA: I–II | Investigator-blinded | Position: Sitting | Ondansetron 4 mg before spinal anaesthesia | Reduction in MAP by > 20% from the baseline value. |
| Control: 20 | Age range: 20–40 | Local anaesthetic: 2 mL 0.5% hyperbaric bupivacaine at L 3–4 or L 4–5 | |||||
| Marciniak 2015 [33] | O (8 mg): 36 | Caesarean section | ASA: I–II | Double-blinded | Position: Sitting | Ondansetron 8 mg before spinal anaesthesia | Reduction in SBP by > 20% from the baseline value or SBP < 90 mmHg. |
| Control: 34 | Age range: NR | Local anaesthetic: 0.5% hypertonic bupivacaine at L 3–4 or L 4–5 | |||||
| Mendonça 2021 [12] | O (8 mg): 72 | Nonobstetric surgery | ASA: I–II | Double-blinded | Position: Sitting | Ondansetron 8 mg before spinal anaesthesia | Reduction in SBP by > 20% from the baseline value or SBP < 90 mmHg. |
| Control: 72 | Age range: ≥18 | Local anaesthetic: hyperbaric bupivacaine (15 mg or more) | |||||
| Mohamed 2021 [11] | O (10 mg): 38 | Caesarean section | ASA: I–II | Double-blinded | Position: Sitting | Ondansetron 10 mg before spinal anaesthesia | Reduction in MAP by > 20% from the baseline value. |
| Control: 38 | Age range: NR | Local anaesthetic: 12.5 mL 0.5% isobaric bupivacaine. at L 3–4 | |||||
| Mohamed 2018 [34] | O (4 mg): 45 | NR | ASA: I | Patient-blinded | Position: Sitting | Ondansetron 4 mg before spinal anaesthesia | Reduction in MAP by > 20% from the baseline value or MAP < 70 mm Hg. |
| Control: 45 | Age range: 18–45 | Local anaesthetic: 2.5–3 mL 0.5% hyperbaric bupivacaine at L 3–4 | |||||
| Mohammadzadeh 2021 [35] | O (4 mg): 127 | Caesarean section | ASA: II | Double-blinded | Position: Sitting | Ondansetron 4 mg after spinal anaesthesia | Reduction in BP by > 20% from the baseline value or BP < 100 mm Hg. |
| Control: 127 | Age range: 18–40 | Local anaesthetic: 12.5 mg isobar bupivacaine at L 3–4 or L 4–5 | |||||
| Nallam 2017 [36] | O (8 mg): 40 | Caesarean section | ASA: I–II | Double-blinded | Position: Sitting | Ondansetron 8 mg before spinal anaesthesia | Reduction in BP by > 20% from the baseline value or MAP below 60 mmHg. |
| Control: 40 | Age range: 22–32 | Local anaesthetic: 12.5 mg 0.5% hyperbaric bupivacaine L 3–4 or L 4–5 | |||||
| Ortiz-Gómez 2014 [37] | O (2 mg):32 | Caesarean section | ASA: I | Double-blinded | Position: Sitting | Ondansetron (2, 4 or 8 mg) before spinal anaesthesia | Reduction in SBP by > 25% from the baseline value. |
| O (4 mg):32 | Age range: 20–45 | ||||||
| O (8 mg):32 | Local anaesthetic: 0.5% hyperbaric bupivacaine L 3–4 or L 4–5 | ||||||
| Control: 32 | |||||||
| Owczuk 2008 [38] | O (8 mg): 36 | NR | ASA: I–II | Double-blinded | Position: Sitting | Ondansetron 8 mg before spinal anaesthesia | SBP < 90 mmHg. |
| Control: 35 | Age range: 20–70 | Local anaesthetic: 4 mL 0.5% hyperbaric bupivacaine L 3–4 or L 4–5 | |||||
| Owczuk 2015 [39] | O (8 mg): 26 | NR | ASA: I–III | Double-blinded | Position: Sitting | Ondansetron 8 mg before spinal anaesthesia | Reduction in SBP by > 20% from the baseline value or SBP < 90 mmHg. |
| Control: 27 | Age range: >70 | Local anaesthetic: 2.5 to 3 mL 0.5% hyperbaric bupivacaine at L 2–3 or L 3–4 or L 4–5 | |||||
| Pirat 2005 [40] | O (4 mg): 50 | Inguinal hernia, cord hydrocele, and pilonidal sinus | ASA: NR | Double-blinded | Position: Sitting | Ondansetron 4 mg before spinal anaesthesia | Reduction in SBP by > 15% from the baseline value. |
| Control: 50 | Age range: NR | Local anaesthetic: 12.5 mg or 15 mg 0.5% hyperbaric bupivacaine at L 2–3 or L 3–4 | |||||
| Ramon 2017 [41] | O (8 mg): 65 | Caesarean section | ASA: I | Double-blinded | Position: Sitting | Ondansetron 8 mg before spinal anaesthesia | Reduction in SBP by > 25% from the baseline value. |
| Control: 65 | Age range: 20–45 | Local anaesthetic: 0.5% hyperbaric bupivacaine at L 3–4 or L 4–5 | |||||
| Safavi 2014 [43] | O (8 mg): 40 | Orthopaedic surgery | ASA: I–II | Double-blinded | Position: Sitting | Ondansetron 8 mg before spinal anaesthesia | Reduction in SBP by > 20% from the baseline value. |
| Control: 40 | Age range: 16–65 | Local anaesthetic: 0.5% hyperbaric bupivacaine at L 3–4 | |||||
| Sahoo 2012 [44] | O (4 mg): 26 | Caesarean section | ASA: I | Double-blinded | Position: Sitting | Ondansetron 4 mg before spinal anaesthesia | SBP < 90 mmHg or DBP < 60 mmHg. |
| Control: 26 | Age range: 20–40 | Local anaesthetic: 2 mL 0.5% hyperbaric bupivacaine at L 3–4 or L 4–5 | |||||
| Shakya 2010 [45] | O (4 mg): 40 | General and gynaecological surgery | ASA: I | Double-blinded | Position: NR | Ondansetron 4 mg after spinal anaesthesia | NR. |
| Control: 40 | Age range: NR | Local anaesthetic: 3 mL 0.5% hyperbaric bupivacaine at L 3–4 or L 4–5 | |||||
| Tatikonda 2019 [46] | O (4 mg): 70 | Orthopaedic, gynaecological, and general surgical procedures | ASA: I–II | Double-blinded | Position: Sitting | Ondansetron 4 mg before spinal anaesthesia | Reduction in MAP by > 20% from the baseline value. |
| Control: 70 | Age range: 20–60 | Local anaesthetic: 3 mL 0.5% hyperbaric bupivacaine at L 3–4 or L 4–5 | |||||
| Terkawi 2015 [47] | O (8 mg): 44 | Caesarean section | ASA: I | Double-blinded | Position: recumbent | Ondansetron 8 mg before spinal anaesthesia | SBP < 90 mmHg. |
| Control: 42 | Age range: NR | Local anaesthetic: 15 mg 0.75% bupivacaine at L 3–4 or L 4–5 | |||||
| Trabelsi 2015 [48] | O (4 mg): 40 | Caesarean section | ASA: NR | Double-blinded | Position: sitting | Ondansetron 4 mg before spinal anaesthesia | Reduction in SBP by > 20% from the baseline value or SBP < 80 mmHg. |
| Control: 40 | Age range: NR | Local anaesthetic: 2 mL hyperbaric bupivacaine at L 2–3 or L 3–4 | |||||
| Wang M 2014 [49] | O (2 mg): 29 | Caesarean section | ASA: I–II | Double-blinded | Position: NR | Ondansetron (2, 4, 6, or 8 mg) before spinal anaesthesia | Reduction in SBP by > 20% from the baseline value. |
| O (4 mg): 30 | Age range: 18–35 | Local anaesthetic: 2 mL 0.5% hyperbaric bupivacaine | |||||
| O (6 mg): 29 | |||||||
| O (8 mg): 30 | |||||||
| Control: 30 | |||||||
| Wang Q 2014 [50] | O (4 mg): 33 | Caesarean section | ASA: I–II | Double-blinded | Position: NR | Ondansetron 4 mg before spinal anaesthesia | Reduction in SBP by > 20% from the baseline value. |
| Control: 32 | Age range: 18–35 | Local anaesthetic: 2 mL 0.5% hyperbaric bupivacaine |
| Outcome | MD/RR (95% CI) | Level of Certainty | Reasons |
|---|---|---|---|
| Incidence of hypotension | 0.65 (0.53, 0.80) | ⨁⨁⨁◯ MODERATE | Inconsistency was “serious”. |
| Incidence of bradycardia | 0.56 (0.38, 0.83) | ⨁⨁⨁⨁ HIGH | None. |
| Rescue of vasopressor administration | 0.50 (0.38, 0.67) | ⨁⨁⨁⨁ HIGH | None. |
| Administration of ephedrine | −2.81 (−4.72, −0.89) | ⨁⨁⨁◯ MODERATE | Inconsistency was “serious”. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hou, X.-M.; Chen, Y.-J.; Lai, L.; Liu, K.; Shen, Q.-H. Ondansetron Reduces the Incidence of Hypotension after Spinal Anaesthesia: A Systematic Review and Meta-Analysis. Pharmaceuticals 2022, 15, 1588. https://0-doi-org.brum.beds.ac.uk/10.3390/ph15121588
Hou X-M, Chen Y-J, Lai L, Liu K, Shen Q-H. Ondansetron Reduces the Incidence of Hypotension after Spinal Anaesthesia: A Systematic Review and Meta-Analysis. Pharmaceuticals. 2022; 15(12):1588. https://0-doi-org.brum.beds.ac.uk/10.3390/ph15121588
Chicago/Turabian StyleHou, Xiao-Min, Yan-Jun Chen, Lan Lai, Ke Liu, and Qi-Hong Shen. 2022. "Ondansetron Reduces the Incidence of Hypotension after Spinal Anaesthesia: A Systematic Review and Meta-Analysis" Pharmaceuticals 15, no. 12: 1588. https://0-doi-org.brum.beds.ac.uk/10.3390/ph15121588