“Being in Control of My Asthma Myself” Patient Experience of Asthma Management: A Qualitative Interpretive Description


Abstract
:1. Introduction
- To identify how patients manage their asthma
- To describe what resources patients need to access for asthma management
- To understand how patients view and experience pharmacists’ roles in ongoing management of asthma.
2. Methods
2.1. Research Team and Reflexivity
2.2. Study Design
2.3. Recruitment and Sample
2.4. Data Collection
2.5. Data Analysis
2.6. Rigour
3. Results
3.1. Theme 1: Personalized Common Sense Approach to Asthma Management
3.1.1. Sub-Theme 1: Personalized Markers for Self-Monitoring
As soon as I start coughing, I know this is going to be a three-month adventure, trying to figure out why.(Patient 1)
So as soon as I start to get a tickle in my throat, and kind of that feeling that there’s feathers in there…then I make sure that I take my Advair® at night time as well,(Patient 6)
I know if I can’t make it up the stairs without wheezing, or a problem with my breath, that’s when I go to my primary care doc.(Patient 3)
3.1.2. Sub-Theme 2: Personalized Non-Medical Measures
So probably lifestyle wise is my biggest thing—like, you know, I try and exercise, get my cardiovascular as much as I can, make sure that my core is strong and strengthen everything around there.(Patient 4)
What I used to do was just to try to lay [sic] down, relax my muscles—there are a lot of times when you have an asthma attack, your core muscles are kind of working overtime to force air in and out of your lungs. Um, so, just the more relaxed I can make myself, the better.(Patient 2)
3.1.3. Sub-Theme 3: Personalized Access to Medication
Now, the fun part about prednisone is, for some insurance companies, it’s an indicator of disease severity—especially if you’ve taken it in the last six months and all that, and they won’t insure you for travel. So, like I said, I handle my asthma, and I know when I need to hit it hard and hit it quick. And, so, what you end up doing too is you have some patients—such as maybe myself—going down to Mexico, getting prednisone. Because they know that, number one, it’s an insurance flag if you take it.(Patient 3)
3.2. Theme 2: Patients Identify Their “Go-To” Health Care Provider
Would I have booked an appointment to come in, and sit down, and do this [asthma action plan] with them? Probably not. I think that’s probably—you know, that’s something again that I would reserve for my family doctor, but, (I) would appreciate that.(Patient 2)
When I go to [name of Asthma specialist] for the respiratory end of things, she’ll ask if I need any prescriptions.(Patient 9)
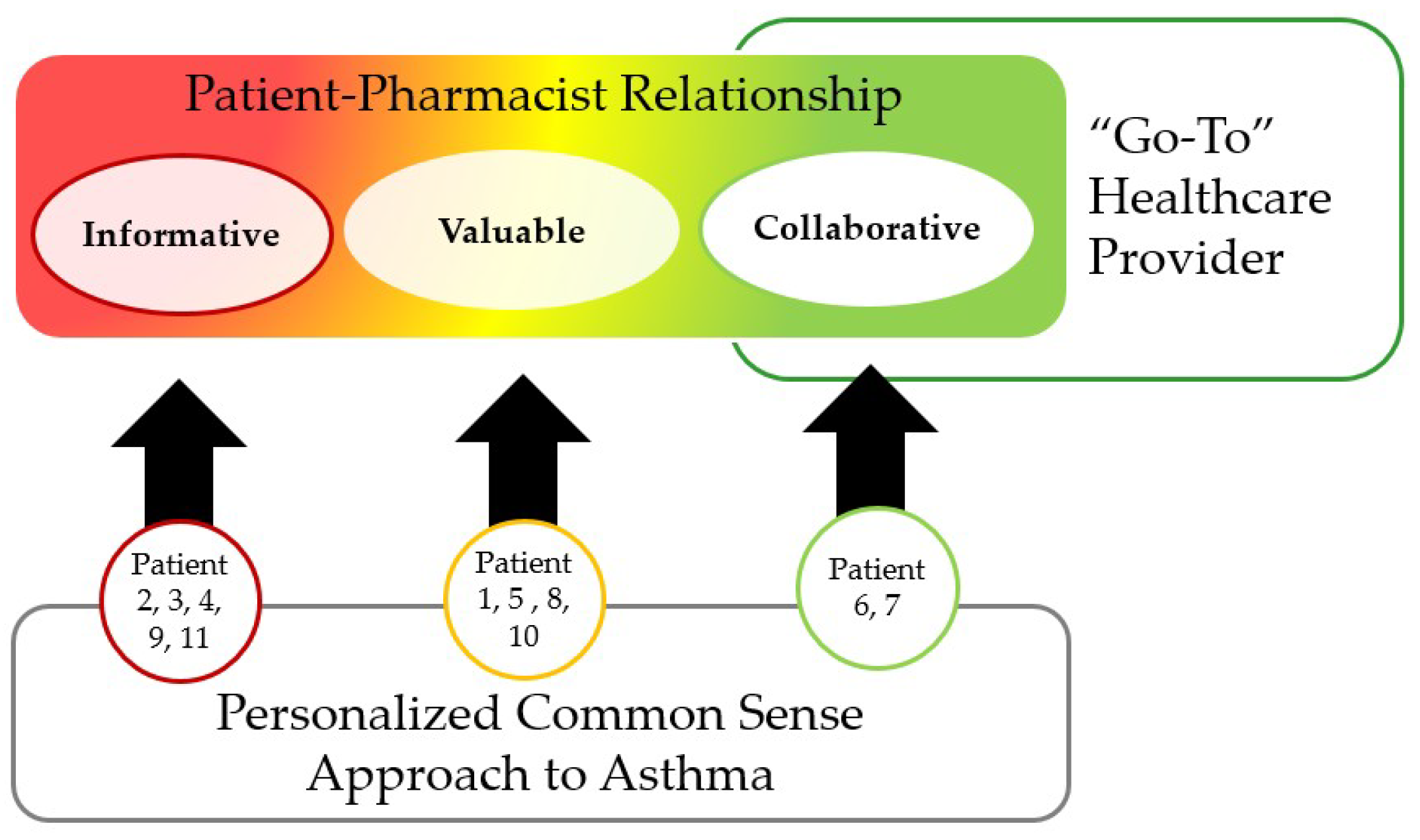
3.3. Theme 3: Patient–Pharmacist Relationship Comes First
I think it takes some time to build trust, that sometimes is built in that patient-physician, that’s important… But if you’re comfortable, I think a pharmacist is well within their scope of practice to help create an action plan, for sure.(Patient 4)
3.3.1. Sub-Theme 1: Information-Focused Relationship
It’s [the interaction] very brief. It’s just because I’ve had it for so long, that they know that I know what I’m doing with it. Um, but yeah, there’s no real discussion regarding the medication.(Patient 2)
The challenge is, it’s [role of pharmacist] only appropriate in what’s asked, right—I mean, nobody really wants anything forced on them, so, um… I imagine a pharmacist who is a certified respiratory educator would be a great thing, and [inaudible] lean on that background and work with them… But essentially in the end, I just want to know about the drug, interactions, possible side effects, and how to do it properly.(Patient 4)
Didn’t engage me on, yeah, “How well is he controlled? What is he doing about it? Does he know what he’s doing?” Right? I rarely get that question. But once again, I think that’s because in the last few years, I just… I just see that pharmacy as a dispensing outlet.(Patient 3)
“Well it’s a nightmare to be honest with you. I find that whenever I’ve gone to a pharmacy in [city name] I have either had a pharmacist try to tell me what my asthma medication should be or they try to ask you tons of questions because you have asthma, but they don’t know the whole picture. They only see the prescription that you’re bringing in, they don’t have your medical file, they don’t know how many doctors you’ve been to or what steps you’ve taken so far. They just assume that because you have asthma, it’s not under control and they can provide additional advice that is actually unsolicited. It’s really irritating to be honest with you”.(Patient 11)
3.3.2. Sub-Theme 2: Valuable Relationship
I do [use the AeroChamber®] yeah. Yeah I don’t even see that as a concern because I’ve always used it. It was actually a pharmacist who told me about that, not my family doctor. Which is part of why I wanted to participate in this because they play such an important role and that’s made such a difference for me.(Patient 8)
Or maybe even like when I get to a pharmacist, having an appointment with them when I go to pick it up, to go over things and maybe decide if this even going to help me, instead of spending three months trying to figure it out with my doctor, who maybe not as knowledgeable on that kind of stuff. So yeah, it’d be nice—I mean, I know they offer that kind of stuff, so maybe making it more known(Patient 1)
I understand that there might be insurance stuff involved in that but I do believe that I should not have to make an appointment with my doctor just to get medication refills. I think that is ridiculous and it’s a waste [of time]. There is legitimate sick people out there that really need to see the doctor and all that does is put stress on an already stressful system. So I really think the doctor should just be able to push a button to refill the prescriptions at the pharmacist or something. The pharmacy should be able to refill your medication without your doctor.(Patient 10)
3.3.3. Sub-Theme 3: Collaborative Relationship
Her [the CAE pharmacist’s] role is to advocate for being in control of my asthma myself, and making sure that the things she or my doctor are prescribing are actually benefitting me in the way they’re supposed to, because I have the right knowledge to use them properly”.(Patient 6)
You know, she’s really, really educated me on all aspects of asthma—it’s been a real eye opener. Because I’ve had it for so long, and for probably at least the first fifteen years or so, I was just… Kind of on my own. You know, I’d go to the doctor. “Oh hi, how you doing?” “Um yeah, kind of coughing.” You know, he was pretty good, but he didn’t help me understand why I was coughing, and why I was having these symptoms. Whereas she sits me down and says, “Okay, look. This is why you’re doing this, this, and this. And this is what you need to do. And you should not cough, period.” [laugh].(Patient 7)
And I’ve always wanted one. I would ask the doctor, and… They either didn’t know about it or didn’t have time. But she [the pharmacist] will sit down with me every month or two and go through it and do any changes…. So the action plan gives me specific things to do when my chest gets tight, when I get short of breath—then I can be flexible with the Symbicort. And I don’t have to be afraid to take more Ventolin, or take even less than, like, one an hour. If it gets bad, I can do more.(Patient 7)
[Speaking about pharmacist] “and be very caring and personable during the process”(Patient 6)
And [the pharmacist] is so good that way, she’s always encouraging me to, you know—by the time the next action plan comes up, ‘Oh yeah, I was supposed to do that, okay’. So she doesn’t judge, she doesn’t criticize, she just (says), ‘Okay, well let’s work on that’.(Patient 7)
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Patient Interview Guide
- How old are you? _______
- Gender: __Male __Female
- How long have you had asthma?
- What medications do you use for your asthma?
- Tell me about how you manage asthma. Who helps you with that?
- Tell me about your asthma medications
- Tell me about how you manage your asthma when you have a flare up/out of control?
- When thinking about your asthma and your life, what matters to you?
- Do you use an asthma action plan? (Show a copy). If so, please tell me how it was created?
- Who helps you manage your asthma?
- Family Physician, Asthma Clinic, Asthma Specialist, Nurse, Pharmacist?
- Tell me about a typical interaction with your pharmacist about your asthma medications.
- What is the pharmacist role in the interaction that occurs between pharmacists and patients?
- Has a pharmacist prescribed an inhaler for you? How did that happen?
- Have you had a med review or care plan session with your pharmacist? Has a pharmacist had a longer talk with you that concluded with signing a piece of paper? Please tell me about it.
- What is your role in the interaction that occurs between pharmacists and patients?
- Imagine that your pharmacist wants to do more for you. What could your pharmacist do to help with your asthma?
- Tell me about any negative experiences you have in the pharmacy.
- What would you think of creating an Asthma Action Plan with your pharmacist?
References
- Statistics Canada. Asthma, by Age Group. Available online: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310009608 (accessed on 24 August 2018).
- Papaioannou, A.I.; Kostikas, K.; Zervas, E.; Kolilekas, L.; Papiris, S.; Gaga, M. Control of asthma in real life: Still a valuable goal? Eur. Respir. Rev. 2015, 24, 361–369. [Google Scholar] [CrossRef] [PubMed]
- The Canadian Lung Association. Asthma Control in Canada Survey 2016. Available online: https://www.lung.ca/news/latest-news/survey-asthma-not-well-controlled-most-canadians (accessed on 24 August 2018).
- Sawicki, G.S.; Vilk, Y.; Schatz, M.; Kleinman, K.; Abrams, A.; Madden, J. Uncontrolled asthma in a commercially insured population from 2002 to 2007: Trends, predictors, and costs. J. Asthma 2010, 47, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Braido, F. Failure in asthma control: Reasons and consequences. Scientifica 2013, 2013, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Pinnock, H.; Parke, H.L.; Panagioti, M.; Daines, L.; Pearce, G.; Epiphaniou, E.; Bower, P.; Sheikh, A.; Griffiths, C.J.; Taylor, S.J.C.; et al. Systematic meta-review of supported self-management for asthma: A healthcare perspective. BMC Med. 2017, 15, 64. [Google Scholar] [CrossRef] [PubMed]
- Saini, B.; Krass, I.; Smith, L.; Bosnic-Anticevich, S.; Armour, C. Role of community pharmacists in asthma —Australian research highlighting pathways for future primary care models. Australas. Med. J. 2011, 4, 190–200. [Google Scholar] [CrossRef] [PubMed]
- Watkins, K.; Bourdin, A.; Trevenen, M.; Murray, K.; Kendall, P.A.; Schneider, C.R.; Clifford, R. Opportunities to develop the professional role of community pharmacists in the care of patients with asthma: A cross-sectional study. NPJ Prim. Care Respir. Med. 2016, 26, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Armour, C.L.; Lemay, K.; Saini, B.; Reddel, H.K.; Bosnic-Anticevich, S.Z.; Smith, L.D.; Burton, D.; Song, Y.J.; Alles, M.C.; Stewart, K.; et al. Using the community pharmacy to identify patients at risk of poor asthma control and factors which contribute to this poor control. J. Asthma 2011, 48, 914–922. [Google Scholar] [CrossRef] [PubMed]
- Apikoglu-Rabus, S.; Yesilyaprak, G.; Izzettin, F.V. Drug-related problems and pharmacist interventions in a cohort of patients with asthma and chronic obstructive pulmonary disease. Respir. Med. 2016, 120, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Saini, B.; Krass, I.; Armour, C. Development, Implementation, and Evaluation of a Community Pharmacy–Based Asthma Care Model. Ann. Pharmacother. 2004, 38, 1954–1960. [Google Scholar] [CrossRef] [PubMed]
- Manfrin, A.; Tinelli, M.; Thomas, T.; Krska, J. A cluster randomised control trial to evaluate the effectiveness and cost-effectiveness of the Italian medicines use review (I-MUR) for asthma patients. BMC Health Serv. Res. 2017, 17, 9. [Google Scholar] [CrossRef] [PubMed]
- Anum, P.O.; Anto, B.P.; Forson, A.G. Structured pharmaceutical care improves the health-related quality of life of patients with asthma. J. Pharm. Policy Pract. 2017, 10, 8. [Google Scholar] [CrossRef] [PubMed]
- Benavides, S.; Rodriguez, J.C.; Maniscalco-Feichtl, M. Pharmacist involvement in improving asthma outcomes in various healthcare settings: 1997 to present. Ann. Pharmacother. 2009, 43, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Armour, C.; Bosnic-Anticevich, S.; Brillant, M.; Burton, D.; Emmerton, L.; Krass, I.; Saini, B.; Smith, L.; Stewart, K. Pharmacy Asthma Care Program (PACP) improves outcomes for patients in the community. Thorax 2007, 62, 496. [Google Scholar] [CrossRef] [PubMed]
- Naik Panvelkar, P.; Armour, C.; Saini, B. Community Pharmacy-Based Asthma Services—What Do Patients Prefer? J. Asthma 2010, 47, 1085–1093. [Google Scholar] [CrossRef] [PubMed]
- Onda, M.; Sakurai, H.; Hayase, Y.; Sakamaki, H.; Arakawa, Y.; Yasukawa, F. Effects of patient-pharmacist communication in the treatment of asthma. Yakugaku Zasshi 2009, 129, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Street, R.L.; Mazor, K.M. Clinician–patient communication measures: Drilling down into assumptions, approaches, and analyses. Patient Educ. Couns. 2017, 100, 1612–1618. [Google Scholar] [CrossRef] [PubMed]
- Sapir, T.; Moreo, K.F.; Greene, L.S.; Simone, L.C.; Carter, J.D.; Mateka, J.J.L.; Hanania, N.A. Assessing Patient and Provider Perceptions of Factors Associated with Patient Engagement in Asthma Care. Ann. Am. Thorac. Soc. 2017, 14, 659–666. [Google Scholar] [CrossRef] [PubMed]
- Horne, R.; Price, D.; Cleland, J.; Costa, R.; Covey, D.; Gruffydd-Jones, K.; Haughney, J.; Henrichsen, S.H.; Kaplan, A.; Langhammer, A.; et al. Can asthma control be improved by understanding the patient’s perspective? BMC Pulm. Med. 2007, 7, 8. [Google Scholar] [CrossRef] [PubMed]
- Horne, R.; Weinman, J. Self-regulation and self-management in asthma: Exploring the role of illness perceptions and treatment beliefs in explaining non-adherence to preventer medication. Psychol. Health 2002, 17, 17–32. [Google Scholar] [CrossRef]
- Driesenaar, J.A.; De Smet, P.A.; van Hulten, R.; Noordman, J.; van Dulmen, S. Cue-Responding Behaviors During Pharmacy Counseling Sessions With Patients With Asthma About Inhaled Corticosteroids: Potential Relations With Medication Beliefs and Self-Reported Adherence. Health Commun. 2016, 31, 1266–1275. [Google Scholar] [CrossRef] [PubMed]
- Berry, T.M.; Prosser, T.R.; Wilson, K.; Castro, M. Asthma Friendly Pharmacies: A Model to Improve Communication and Collaboration among Pharmacists, Patients, and Healthcare Providers. J. Urban Health 2011, 88, 113–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, A.; Shaw, M.; Wright, H. How you can encourage medicines optimisation for patients with asthma. Pharm. J. 2014, 292, 125. [Google Scholar] [CrossRef]
- Canadian Pharmacists Association. Pharmacists’ Scope of Practice in Canada. Available online: https://www.pharmacists.ca/pharmacy-in-canada/scope-of-practice-canada (accessed on 20 September 2018).
- Morrison, J. Expanded pharmacy practice: Where are we, and where do we need to go? Can. Pharm. J. 2013, 146, 365–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thorne, S. Interpretive Description; Routledge: New York, NY, USA, 2016. [Google Scholar]
- Thorne, S.; Kirkham, S.R.; MacDonald-Emes, J. Interpretive description: A noncategorical qualitative alternative for developing nursing knowledge. Res. Nurs. Health 1997, 20, 169–177. [Google Scholar] [CrossRef] [Green Version]
- Hunt, M.R. Strengths and Challenges in the Use of Interpretive Description: Reflections Arising from a Study of the Moral Experience of Health Professionals in Humanitarian Work. Qual. Health Res. 2009, 19, 1284–1292. [Google Scholar] [CrossRef] [PubMed]
- Kahlke, R.M. Generic Qualitative Approaches: Pitfalls and Benefits of Methodological Mixology. Int. J. Qual. Meth. 2014, 13, 37–52. [Google Scholar] [CrossRef] [Green Version]
- Lau, S.R.; Traulsen, J.M. Are we ready to accept the challenge? Addressing the shortcomings of contemporary qualitative health research. Res. Soc. Adm. Pharm. 2017, 13, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Collins, C.S.; Stockton, C.M. The Central Role of Theory in Qualitative Research. Int. J. Qual. Meth. 2018, 17. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. What can “thematic analysis” offer health and wellbeing researchers? Int. J. Qual. Stud. Health 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Green, J.; Karen, W.; Emma, H.; Small, R.; Welch, N.; Lisa, G.; Daly, J. Generating best evidence from qualitative research: The role of data analysis. Aust. N. Z. J. Public Health 2007, 31, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Morse, J.M. Confusing categories and themes. Qual. Health Res. 2008, 18, 727–728. [Google Scholar] [CrossRef] [PubMed]
- Leventhal, H.; Phillips, L.A.; Burns, E. The Common—Sense Model of Self-Regulation (CSM): A dynamic framework for understanding illness self-management. J. Behav. Med. 2016, 39, 935–946. [Google Scholar] [CrossRef] [PubMed]
- Guirguis, L.M. Assessing the knowledge to practice gap: The asthma practices of community pharmacists. Can. Pharm. J. 2018, 151, 62–70. [Google Scholar] [CrossRef] [PubMed]
- McAndrew, L.M.; Musumeci-Szabo, T.J.; Mora, P.A.; Vileikyte, L.; Burns, E.; Halm, E.A.; Leventhal, E.A.; Leventhal, H. Using the common sense model to design interventions for the prevention and management of chronic illness threats: From description to process. Br. J. Health Psychol. 2008, 13, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Bodenheimer, T.; Lorig, K.; Holman, H.; Grumbach, K. Patient self-management of chronic disease in primary care. JAMA 2002, 288, 2469–2475. [Google Scholar] [CrossRef] [PubMed]
- Naughton, A.C. Patient-Centered Communication. Pharmacy 2018, 6, 1–8. [Google Scholar] [CrossRef] [PubMed]
- King, A.; Hoppe, R.B. “Best practice” for patient-centered communication: A narrative review. J. Grad. Med. Educ. 2013, 5, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Phillips, L.A.; Leventhal, H.; Leventhal, E.A. Physicians’ communication of the common-sense self-regulation model results in greater reported adherence than physicians’ use of interpersonal skills. Br. J. Health Psychol. 2012, 17, 244–257. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, D.R.; Shoemaker, S.J. Achieving Patient Centeredness in Pharmacy Practice: Openness and the Pharmacist’s Natural Attitude. J. Am. Pharm. Assoc. 2006, 46, 56–66. [Google Scholar] [CrossRef]
- Houben-Wilke, S.; Augustin, I.M.L.; Wouters, B.B.; Stevens, R.A.H.; Janssen, D.J.A.; Spruit, M.A.; Vanfleteren, L.E.G.W.; Franssen, F.M.E.; Wouters, E.F.M. The patient with a complex chronic respiratory disease: A specialist of his own life? Expert Rev. Respir. Med. 2017, 11, 919–924. [Google Scholar] [CrossRef] [PubMed]
- Cheong, L.H.; Armour, C.L.; Bosnic-Anticevich, S.Z. Patient asthma networks: Understanding who is important and why. Health Expect. 2015, 18, 2595–2605. [Google Scholar] [CrossRef] [PubMed]
- Gershon, A.S.; Macdonald, E.M.; Luo, J.; Austin, P.C.; Gupta, S.; Sivjee, K.; Upshur, R.; Aaron, S.D. Concomitant pulmonologist and primary care for chronic obstructive pulmonary disease: A population study. Fam. Pract. 2017, 34, 708–716. [Google Scholar] [CrossRef] [PubMed]
- Alberta Health. Pharmacy Services and Prescription Drugs. Available online: http://www.health.alberta.ca/services/pharmacy-services.html (accessed on 28 September 2018).
- Assa-Eley, M.; Kimberlin, C.L. Using interpersonal perception to characterize pharmacists’ and patients’ perceptions of the benefits of pharmaceutical care. Health Commun. 2005, 17, 41–56. [Google Scholar] [CrossRef] [PubMed]
- Tarn, D.M.; Paterniti, D.A.; Wenger, N.S.; Williams, B.R.; Chewning, B.A. Older patient, physician and pharmacist perspectives about community pharmacists’ roles. Int. J. Pharm. Pract. 2012, 20, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Guirguis, L.M.; Chewning, B.A. Role theory: Literature review and implications for patient-pharmacist interactions. Res. Soc. Adm. Pharm. 2005, 1, 483–507. [Google Scholar] [CrossRef] [PubMed]
- Shah, B.; Chewning, B. Conceptualizing and measuring pharmacist-patient communication: A review of published studies. Res. Soc. Adm. Pharm. 2006, 2, 153–185. [Google Scholar] [CrossRef] [PubMed]
- Worley, M.M.; Schommer, J.C.; Brown, L.M.; Hadsall, R.S.; Ranelli, P.L.; Stratton, T.P.; Uden, D.L. Pharmacists’ and patients’ roles in the pharmacist-patient relationship: Are pharmacists and patients reading from the same relationship script? Res. Soc. Adm. Pharm. 2007, 3, 47–69. [Google Scholar] [CrossRef] [PubMed]
- Antunes, L.P.; Gomes, J.J.; Cavaco, A.M. How pharmacist–patient communication determines pharmacy loyalty? Modeling relevant factors. Res. Soc. Adm. Pharm. 2015, 11, 560–570. [Google Scholar] [CrossRef] [PubMed]
- Mossialos, E.; Courtin, E.; Naci, H.; Benrimoj, S.; Bouvy, M.; Farris, K.; Noyce, P.; Sketris, I. From “retailers” to health care providers: Transforming the role of community pharmacists in chronic disease management. Health Policy 2015, 119, 628–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCullough, M.B.; Petrakis, B.A.; Gillespie, C.; Solomon, J.L.; Park, A.M.; Ourth, H.; Morreale, A.; Rose, A.J. Knowing the patient: A qualitative study on care-taking and the clinical pharmacist-patient relationship. Res. Soc. Adm. Pharm. 2016, 12, 78–90. [Google Scholar] [CrossRef] [PubMed]
- Schindel, T.J.; Yuksel, N.; Breault, R.; Daniels, J.; Varnhagen, S.; Hughes, C.A. Perceptions of pharmacists’ roles in the era of expanding scopes of practice. Res. Soc. Adm. Pharm. 2017, 13, 148–161. [Google Scholar] [CrossRef] [PubMed]
- Kelly, D.V.; Young, S.; Phillips, L.; Clark, D. Patient attitudes regarding the role of the pharmacist and interest in expanded pharmacist services. Can. Pharm. J. 2014, 147, 239–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mead, N.; Bower, P. Patient-centredness: A conceptual framework and review of the empirical literature. Soc. Sci. Med. 2000, 51, 1087–1110. [Google Scholar] [CrossRef]
- Tinelli, M.; Bond, C.; Blenkinsopp, A.; Jaffray, M.; Watson, M.; Hannaford, P. Patient Evaluation of a Community Pharmacy Medications Management Service. Ann. Pharmacother. 2007, 41, 1962–1970. [Google Scholar] [CrossRef] [PubMed]
- Greene, S.M.; Tuzzio, L.; Cherkin, D. A Framework for Making Patient-Centered Care Front and Center. Perm. J. 2012, 16, 49–53. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patient Identifier | Age | Gender | Recruitment Strategy | “Go-To” Healthcare Provider | Type of Pharmacist Relationship |
|---|---|---|---|---|---|
| Patient 1 | 24 | F | RSCN | Family physician | Valuable |
| Patient 2 | 43 | M | RSCN | Family physician | Information |
| Patient 3 | 41 | M | RSCN | Family physician | Information |
| Patient 4 | 51 | M | RSCN | Asthma specialist | Information |
| Patient 5 a | 45, 18, 14 | F, M, M | RSCN | Respiratory therapist | Valuable |
| Patient 6 b | 54 | F | Community Pharmacy | Pharmacist and Family physician | Collaboration |
| Patient 7 b | 56 | F | Community Pharmacy | Pharmacist and Asthma specialist | Collaboration |
| Patient 8 | 30 | F | Asthma Clinic | Family physician | Valuable |
| Patient 9 | 56 | F | Asthma Clinic | Asthma specialist | Information |
| Patient 10 | 30 | F | Asthma Clinic | Asthma specialist | Information |
| Patient 11 | 36 | F | Asthma Clinic | Asthma specialist | Information |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olufemi-Yusuf, D.T.; Gabriel, S.B.; Makhinova, T.; Guirguis, L.M. “Being in Control of My Asthma Myself” Patient Experience of Asthma Management: A Qualitative Interpretive Description. Pharmacy 2018, 6, 121. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy6040121
Olufemi-Yusuf DT, Gabriel SB, Makhinova T, Guirguis LM. “Being in Control of My Asthma Myself” Patient Experience of Asthma Management: A Qualitative Interpretive Description. Pharmacy. 2018; 6(4):121. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy6040121
Chicago/Turabian StyleOlufemi-Yusuf, Damilola T., Sophie Beaudoin Gabriel, Tatiana Makhinova, and Lisa M. Guirguis. 2018. "“Being in Control of My Asthma Myself” Patient Experience of Asthma Management: A Qualitative Interpretive Description" Pharmacy 6, no. 4: 121. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy6040121