
High-Power LED Units Currently Available for Dental Resin-Based Materials—A Review

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Search Strategy
2.2.1. Sources of Information
2.2.2. Search Terms
2.2.3. Study Selection
2.2.4. Study Data
2.3. Quality Assessment
3. Results
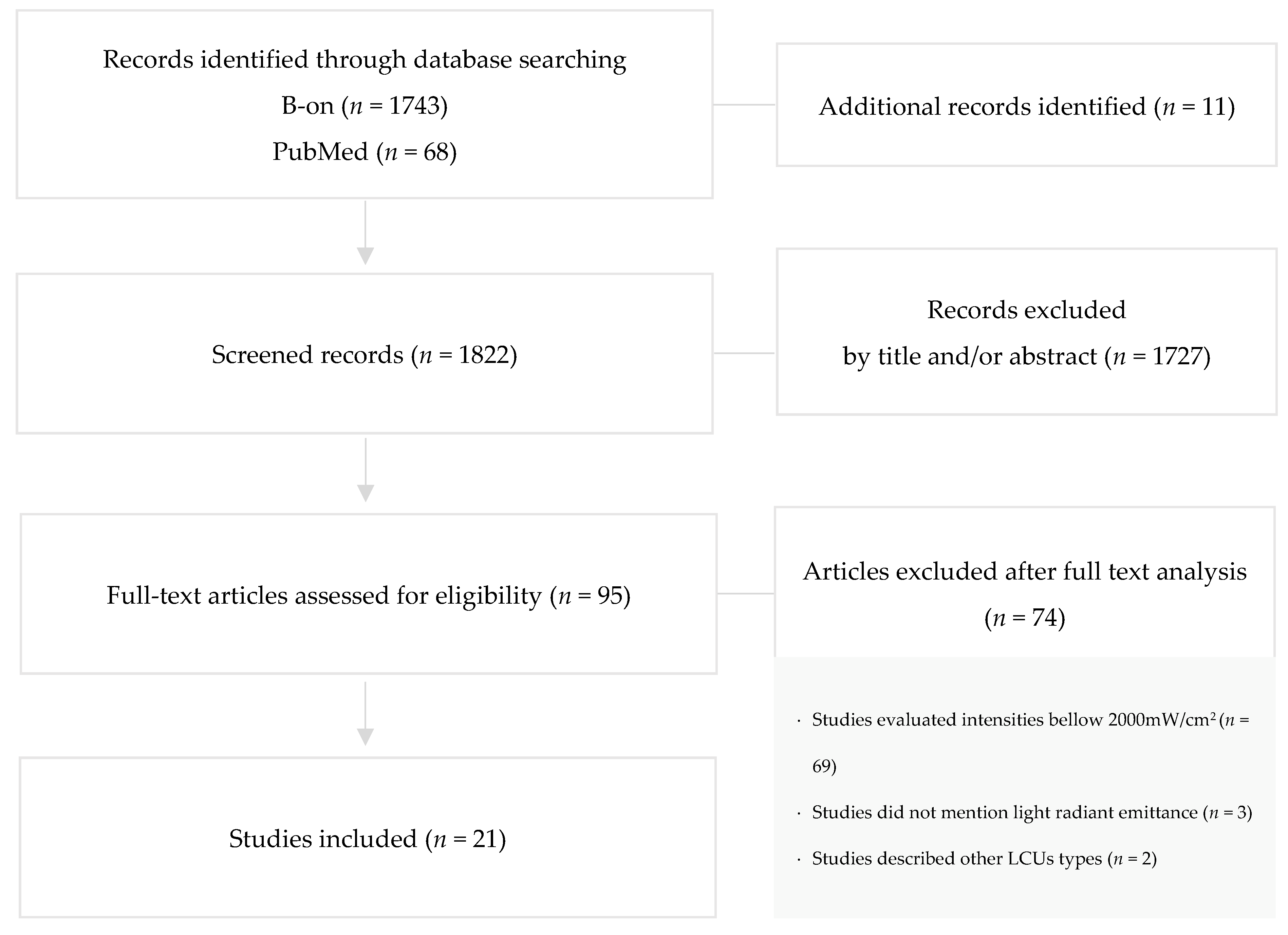
3.1. Study Selection and Flow Diagram
3.2. Study Characteristics
3.2.1. Study Design
3.2.2. Clinical Procedure
3.2.3. High-Power LED-LCUs
3.2.4. Control LCUs
3.2.5. Irradiation Technique

{kind=link}
| Author, Year | Study Design | Clinical/ Technical Procedure | High-Power LED-LCU (Manufacturer) | Radiant Emittance 1 (mW/cm2) | Exposure Time 1 (s) | Radiant Emittance Mean Value 2 (sd) (mW/cm2) | Control LCU (Manufacturer) | Radiant Emittance (mW/cm2) | Exposure Time (s) | Irradiation Technique |
|---|---|---|---|---|---|---|---|---|---|---|
| Park, Roulet and Heintze, 2010 [22] | In Vitro | Maxillary premolar exposed to light curing units | LEDexp2000 Prototype (Ivoclar Vivadent, Liechtenstein) LEDexp3000 Prototype (Ivoclar Vivadent, Liechtenstein) | 2000 3000 | 60 60 | Not reported | Astralis® 10 (Ivoclar Vivadent, Liechtenstein) Bluephase® 16i (Ivoclar Vivadent, Liechtenstein) | 1200 1600 | 30 60 | The unprepared tooth was light cured from the buccal side 1 mm from the buccal surface. |
| Flury et al., 2013 [10] | In Vitro | Light curing resin cements through glass ceramics | VALO® (Ultradent, Utah, USA) | 3200 | 18 | 3505 | Elipar™ Freelight 2 (3M ESPE, Seefeld, Germany) VALO® (Ultradent, Utah, USA) | 1200 1400 | 40 32 | Light curing was performed either directly or through ceramics discs of 1.5 or 3 mm. |
| Branchal et al., 2015 [31] | In Vitro | Light curing sealants | VALO® (Ultradent, Utah, USA) Fusion® (DentLight Inc., Texas, USA) SmartLite® Max (Dentsply International, York, PA, USA) | 3200 2700 2805 | 3, 6, 9 5, 10 10 | 3539 2773 2012 | 3M™ XL 3000 (3M ESPE, Minn, USA) | 450 | 40 | The light tip was placed directly in contact with the surface. |
| Gonulol, Ozer and Tunc, 2015 [16] | In Vitro | Polymerization of resin-based tooth-colored restorative materials | VALO® (Ultradent, MO, USA) | 3200 | 6 | Not reported | Elipar™ S10 (3M ESPE, MN, USA) VALO® (Ultradent, MO, USA) | 1200 1000 or 1400 | 10 20 or 12 | The light guide was in contact with the top surface. |
| Haenel et al., 2015 [17] | In Vitro | Light curing dental resins | Bluephase® 20i (Ivoclar Vivadent, Schaan, Liechtenstein) | 2200 | 5, 20, 80 | 2222 | Celalux® 2 (VOCO, Cuxhaven, Germany) Bluephase® 20i (Ivoclar Vivadent, Liechtenstein) | 1000–1500 3 650 | 5, 20, 80 5, 20, 80 | The light guide tips were placed directly over the center of the sample. |
| Runnacles et al., 2015 [32] | In Vivo | Human premolars exposed to a light curing unit | Bluephase® 20i (Ivoclar Vivadent, Schaan, Liechtenstein) | 2000 | 5 | 2204 (35) | Bluephase® 20i (Ivoclar Vivadent, Liechtenstein) | 650 1200 | 10 10, 60 | The LCU tip was placed against the buccal tooth surface with the lower edge of the light guide sheath just above the facial free gingiva. |
| Ward et al., 2015 [34] | In Vivo | Brackets cured with a high-intensity LED | VALO® Ortho (Ultradent, UT, USA) | 3200 | 6 | Not reported | VALO® Ortho (Ultradent, UT, USA) | 1200 | 20 | Not reported |
| Watanabe et al., 2015 [33] | In Vitro | Polymerization of dual-cured resin cement | PenCure 2000 (Morita, Tokyo, Japan) VALO® (Ultradent, Utah, USA) | 2000 3200 | 5, 10, 15, 20 5, 10, 15, 20 | Not reported | Jetlite 3000 (Morita, Tokyo, Japan) Demi™ (Kerr, CA, USA) | 400 1100 | 20, 40, 60, 80 20, 40, 60, 80 | The tip of the curing unit was placed on the top of the ceramic plate. |
| Armellin et al., 2016 [20] | In Vitro | Composite restorations in first molars | VALO® (Ultradent, Utah, USA) | 3200 | 3 | 1600 | VALO® (Ultradent, Utah, USA) Starlight PRO (Mectron, Carasco, Italy) | 1000 1000 | 20 20 | Not reported |
| Oz, Oz and Arici, 2016 [35] | In Vivo/ In Vitro | Metal brackets polymerized intraorally and, to extracted tooth | VALO® Ortho (Ultradent, Utah, USA) | 3200 | 3 | Not reported | Elipar™ S10 (3M Unitek, Monrovia, Calif) | 1600 | 10 | Not reported |
| Peutzfeldt, Lussi and Flury, 2016 [28] | In Vitro | Light curing resin cements | VALO® (Ultradent, UT, USA) | 3200 | 3 6 9 | 3162 (88.2) 3213 (110.9) 3299 (89.0) | VALO® (Ultradent, UT, USA) | 1000 1400 | 10, 20 8, 16 | The tip end of the LCUwas placed at a distance of 0 mm. |
| Bilgic et al., 2017 [27] | In Vitro | Curing of orthodontic adhesives | VALO® Ortho (Ultradent, Utah, USA) | 3200 | 3 | Not reported | VALO® (Ultradent, Utah, USA) | 1400 | 3 | According to the manufacturer’s instructions. |
| Shimokawa et al., 2017 [15] | In Vitro | Polymerization of resin-based composites | Single-peak high Prototype (Ultradent, UT, USA) Broad-spectrum high Prototype (Ultradent, UT, USA) | 3600 3600 | 5 5 | 3607 (16.6) 3612 (26.0) | Single-peak standard Prototype (Ultradent, UT, USA) Broad-spectrum standard Prototype (Ultradent, UT, USA) | 1200 1200 | 15 15 | Not reported |
| Udomthanaporn, Nisalak and Sawaengkit, 2017 [11] | In Vitro | Orthodontic brackets bonded to human premolars | VALO® (Ultradent, UT, USA) FlashMax™ P3 (CMS Dental, Copenhagen, Denmark) | 3200 4000–6000 | 6 3 | Not reported | Bluephase® (Ivoclar Vivadent Inc., Amherst, NY, USA) | 1200 | 20 | The tip of each curing unit was held about 1 mm away from the bracket-tooth interface. |
| Almeida, Martins and Martins, 2018 [18] | In Vitro | Bracket bonding to human premolars | VALO® Cordless (Ultradent, UT, USA) | 3200 | 3 | 2246 | VALO® Cordless (Ultradent, UT, USA) | 3200 | 6 | Not reported |
| Daugherty et al., 2018 [14] | In Vitro | Polymerization of bulk-fill composites | FlashMax™ P3 (CMS Dental, Copenhagen, Denmark) S.P.E.C.® 3 (Coltene, OH, USA) | 5000–6000 3000–3500 | 3, 9 3 | 2378 (22) 3001 (8) | Paradigm™ (3M ESPE, MN, USA) S.P.E.C.® 3 (Coltene, OH, USA) | 1200 1600 | 10, 20 20 | The LCU light tip was positioned concentrically to the mold opening and directly against the surface. |
| Nurlatifah, Eriwati and Indrani, 2018 [19] | In Vitro | Curing of packable composite resin | FlashMax™ P3 (Hexagon, Denmark) | 4000 | 1, 3 | 1200 | Ledmax™ 450 (Hilux, Benlioglu Dental Inc., Ankara, Turkey) | 450 | 20 | Not reported |
| Vinagre et al., 2019 [21] | In Vitro | Immediately extracted premolars submitted to light curing procedures | Bluephase® 20i (Ivoclar Vivadent, Schaan, Liechtenstein) S.P.E.C.® 3 (Coltene, OH, USA)VALO® (Ultradent, UT, USA) | 2000 3000 3200 | 5 3 3 | 1790 2420 2710 | Bluephase® 20i (Ivoclar Vivadent, Liechtenstein) S.P.E.C.® 3 (Coltene, OH, USA) VALO® (Ultradent, UT, USA) Demi Ultra™ (Kerr, Orange, CA, USA) | 1200 1600 1000 or 1400 4 1215 or 1100–1330 4 | 20 15 20 or 4 4 20 or 20 4 | The LCUs were placed in a support with the light guide touching the buccal surface of the teeth and four light emissions were made with 30 s intervals. |
| Gross et al., 2020 [29] | In Vivo | First premolars requiring extraction exposed to a Polywave LED LCU | Experimental LCU (Ivoclar Vivadent, Schaan, Liechtenstein) | 10,000 | 1,2 | 10,000 | Bluephase® 20i (Ivoclar Vivadent, Liechtenstein) | 1200 | 10, 20, 60 | LCU tip was placed against the buccal tooth surface, directly centered over the Class V preparation. |
| Sadeghyar, Watts and Schedle, 2020 [30] | In Vitro | Ultra-fast polimerization of bulk-fill resin-based composite RAFT-modified | Bluephase® Power Cure (Ivoclar Vivadent, Schaan, Liechtenstein) | 3000 | 3 | 3770.3 (±35.30) | Bluephase® Power Cure (Ivoclar Vivadent, Schaan, Liechtenstein) | 1200 | 10 | The LCU was placed perpendicular, directly on the top surface of the cylinder. |
| Rocha et al., 2021 [36] | In Vitro | Light-curing of a bulk fill composite | VALO® (Ultradent, UT, USA) | 3200 | 9 | 2244 | VALO® (Ultradent, UT, USA) | 1000 | 21 | Not reported |
3.3. Quality Assessment
3.4. Study Results
3.4.1. Degree of Conversion (DC) Analysis
3.4.2. Diametral Tensile Strength (DTS) Analysis
3.4.3. Elastic Modulus (EM) Analysis
3.4.4. Bond Strength (BS) Analysis
3.4.5. Temperature Changes in Pulp Tissue Analysis
3.4.6. High-Power LED-LCUs Commercially Available
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Santini, A. Current Status of Visible Light Activation Units and the Curing of Light-activated Resin-based Composite Materials. Dent. Update 2010, 37, 123. [Google Scholar] [CrossRef] [PubMed]
- Price, R.B.; Ferracane, J.L.; Shortall, A.C. Light-Curing Units: A Review of What We Need to Know. J. Dent Res. 2015, 94, 1179–1186. [Google Scholar] [CrossRef] [PubMed]
- Delgado, A.J.; Castellanos, E.M.; Coelho Sinhoreti, M.A.; de Oliveira, D.C.R.S.; Abdulhameed, N.; Geraldeli, S.; Sulaiman, T.A.; Roulet, J.-F. The use of different photoinitiator systems in photopolymerizing resin cements through ceramic veneers. Oper. Dent. 2019, 44, 396–404. [Google Scholar] [CrossRef]
- Brandt, W.C.; Schneider, L.F.J.; Frollini, E.; Correr-Sobrinho, L.; Sinhoreti, M.A.C. Effect of different photo-initiators and light curing units on degree of conversion of composites. Braz. Oral Res. 2010, 24, 263–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pratap, B.; Gupta, R.K.; Bhardwaj, B.; Nag, M. Resin based restorative dental materials: Characteristics and future perspectives. Jpn. Dent. Sci. Rev. 2019, 55, 126–138. [Google Scholar] [CrossRef]
- Rueggeberg, F.A.; Swift, E.J. Exposure times for Contemporary Composites. J. Esthet Restor Dent. 2013, 25, 82–84. [Google Scholar] [CrossRef]
- Yılmaz, B.; Bakkal, M.; Zengin Kurt, B. Structural and mechanical analysis of three orthodontic adhesive composites cured with different light units. J. Appl. Biomater. Funct. Mater. 2020, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jandt, K.D.; Mills, R.W. A brief history of LED photopolymerization. Dent. Mater. 2013, 29, 605–617. [Google Scholar] [CrossRef]
- Rahiotis, C.; Patsouri, K.; Silikas, N.; Kakaboura, A. Curing efficiency of high-intensity light-emitting diode (LED) devices. J. Oral Sci. 2010, 52, 187–195. [Google Scholar] [CrossRef]
- Flury, S.; Lussi, A.; Hickel, R.; Ilie, N. Light curing through glass ceramics with a second- and a third-generation LED curing unit: Effect of curing mode on the degree of conversion of dual-curing resin cements. Clin. Oral. Investig. 2013, 17, 2127–2137. [Google Scholar] [CrossRef] [Green Version]
- Udomthanaporn, B.; Nisalak, P.; Sawaengkit, P. Shear Bond Strength of Orthodontic Bonding Materials Polymerized by High-Intensity LEDs at Different Intensities and Curing Times. Key Eng. Mater. 2017, 723, 376–381. [Google Scholar] [CrossRef]
- Mohammed, A.; Ario, S. Resin-Based Composite and LCU-related Factors Affecting the Degree of Cure. A Literature Review: Part 2. Light Curing Units & Related Factors. Acta Med. Marisiensis 2015, 61, 255–260. [Google Scholar] [CrossRef] [Green Version]
- Shortall, A.C.; Palin, W.M.; Jacquot, B.; Pelissier, B. Advances in Light-Curing Units: Four Generations of LED Lights and Clinical Implications for Optimizing their Use: Part 2. From Present to Future. Dent. Update 2012, 39, 13–17; 20–22. [Google Scholar] [CrossRef]
- Daugherty, M.M.; Lien, W.; Mansell, M.R.; Risk, D.L.; Savett, D.A.; Vandewalle, K.S. Effect of high-intensity curing lights on the polymerization of bulk-fill composites. Dent. Mater. 2018, 34, 1531–1541. [Google Scholar] [CrossRef] [PubMed]
- Shimokawa, C.A.K.; Sullivan, B.; Turbino, M.L.; Soares, C.J.; Price, R.B. Influence of Emission Spectrum and Irradiance on Light Curing of Resin-Based Composites. Oper. Dent. 2017, 42, 537–547. [Google Scholar] [CrossRef] [PubMed]
- Gonulol, N.; Ozer, S.; Tunc, E.S. Effect of a third-generation LED LCU on microhardness of tooth-colored restorative materials. Int. J. Paediatr. Dent. 2015, 26, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Haenel, T.; Hausnerová, B.; Steinhaus, J.; Price, R.B.T.; Sullivan, B.; Moeginger, B. Effect of the irradiance distribution from light curing units on the local micro-hardness of the surface of dental resins. Dent. Mater. 2015, 31, 93–104. [Google Scholar] [CrossRef]
- Almeida, L.F.; Martins, L.P.; Martins, R.P. Effects of reducing light-curing time of a high-power LED device on shear bond strength of brackets. J. Orofac. Orthop. 2018, 79, 352–358. [Google Scholar] [CrossRef] [Green Version]
- Nurlatifah, A.; Eriwati, Y.K.; Indrani, D.J. The Effect of the Curing Time of an Ultra-High Intensity LED Curing Unit on Diametral Tensile Streght of Packable Composite Resin; IOP Publishing: Bristol, UK, 2018. [Google Scholar]
- Armellin, E.; Bovesecchi, G.; Coppa, P.; Pasquantonio, G.; Cerroni, L. LED Curing Lights and Temperature Changes in Different Tooth Sites. Biomed. Res. Int. 2016, 2016, 1894672. [Google Scholar] [CrossRef] [Green Version]
- Vinagre, A.; Ramos, J.C.; Rebelo, C.; Basto, J.F.; Messias, A.; Alberto, N.; Nogueira, R. Pulp Temperature Rise Induced by Light-Emitting Diode Light-Curing Units Using an Ex Vivo Model. Materials 2019, 12, 411. [Google Scholar] [CrossRef] [Green Version]
- Park, S.H.; Roulet, J.F.; Heintze, S.D. Parameters Influencing Increase in Pulp Chamber Temperature with Light-curing Devices: Curing Lights and Pulpal Flow Rates. Oper. Dent. 2010, 35, 353–361. [Google Scholar] [CrossRef]
- Rueggeberg, F.A.; Giannini, M.; Arrais, C.A.G.; Price, R.B.T. Light curing in dentistry and clinical implications: A literature review. Braz. Oral Res. 2017, 31, 64–91. [Google Scholar] [CrossRef] [Green Version]
- Alasiri, R.A.; Algarni, H.A.; Alasiri, R.A. Ocular hazards of curing light units used in dental practice—A systematic review. Saudi Dent. J. 2019, 31, 173–180. [Google Scholar] [CrossRef]
- Faggion, C.M. Guidelines for reporting pre-clinical in vitro studies on dental materials. J. Evid. Based Dent. Pract. 2012, 12, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. Notes Queries 1855, S1-XI, 64. [Google Scholar]
- Bilgic, F.; Altan, H.; Akinci Sözer Arslanoglu, Z.; Kale, E.; Özarslan, S. Effects of Third-generation LED LCU on Nanomechanical Properties of Orthodontic Adhesives. Acta Phys. Pol. A 2017, 132, 697–701. [Google Scholar] [CrossRef]
- Peutzfeldt, A.; Lussi, A.; Flury, S. Effect of High-Irradiance Light-Curing on Micromechanical Properties of Resin Cements. Biomed. Res. Int. 2016, 2016, 48994653. [Google Scholar] [CrossRef] [PubMed]
- Gross, D.J.; Dávila-Sánchez, A.; Runnacles, P.; Zarpellon, D.C.; Kiratcz, F.; Campagnoli, E.B.; Alegría-Acevedo, L.F.; Coelho, U.; Rueggeberg, F.; Arrais, C.A.G. In Vivo temperature rise and acute inflammatory response in anesthetized human pulp tissue of premolars having Class V preparations after exposure to Polywave® LED light curing units. Dent. Mater. 2020, 36, 1201–1213. [Google Scholar] [CrossRef] [PubMed]
- Sadeghyar, A.; Watts, D.C.; Schedle, A. Limited reciprocity in curing efficiency of bulk-fill resin-composites. Dent. Mater. 2020, 36, 997–1008. [Google Scholar] [CrossRef]
- Branchal, C.F.; Wells, M.H.; Tantbirojn, D.; Versluis, A. Can Increasing the Manufacturer’s Recommended Shortest Curing Time of High-intensity Light-emitting Diodes Adequately Cure Sealants? Pediatr. Dent. 2015, 37, E7–E13. [Google Scholar]
- Runnacles, P.; Augusto, C.; Arrais, G.; Thais, M.; André, F.; Coelho, U.; Rueggeberg, F.A.; Arrais, C.A.G. In Vivo temperature rise in anesthetized human pulp during exposure to a polywave LED light curing unit. Dent. Mater. 2015, 31, 505–513. [Google Scholar] [CrossRef]
- Watanabe, H.; Kazama, R.; Asai, T.; Kanaya, F.; Ishizaki, H.; Fukushima, M.; Okiji, T. Efficiency of Dual-Cured Resin Cement Polymerization Induced by High-Intensity LED Curing Cnits Through Ceramic Material. Oper. Dent. 2015, 40, 153–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward, J.D.; Wolf, B.J.; Leite, L.P.; Zhou, J. Clinical effect of reducing curing times with high-intensity LED lights. Angle Orthod. 2015, 85, 1064–1069. [Google Scholar] [CrossRef] [Green Version]
- Oz, A.A.; Oz, A.Z.; Arici, S. In-vitro bond strengths and clinical failure rates of metal brackets bonded with different light-emitting diode units and curing times. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 212–216. [Google Scholar] [CrossRef]
- Rocha, M.G.; Roulet, J.F.; Sinhoreti, M.A.C.; Correr, A.B.; Oliveira, D. Light transmittance and depth of cure of a bulk fill composite based on the Exposure Reciprocity Law. Braz. Dent. J. 2021, 32, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Eren, D.; Tutkan, F. Investigation of the Reliability of Light-Curing Units in Sivas City, Turkey. Niger. J. Clin. Pract. 2019, 22, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Santini, A.; Turner, S. General dental practitioners’ knowledge of polymerisation of resin-based composite restorations and light curing unit technology. Br. Dent. J. 2011, 211, E13. [Google Scholar] [CrossRef]
- Kopperud, S.E.; Rukke, H.V.; Kopperud, H.M.; Bruzell, E.M. Light curing procedures—performance, knowledge level and safety awareness among dentists. J. Dent. 2017, 58, 67–73. [Google Scholar] [CrossRef]
- Frazier, K.; Bedran-Russo, A.K.; Lawson, N.C.; Park, J.; Khajotia, S.; Urquhart, O. Dental light-curing units: An American Dental Association Clinical Evaluators Panel survey. J. Am. Dent. Assoc. 2020, 151, 544–545.e2. [Google Scholar] [CrossRef]
- Maghaireh, G.A.; Alzraikat, H.; Taha, N.A. Assessing the irradiance delivered from light-curing units in private dental offices in Jordan. J. Am. Dent. Assoc. 2013, 144, 922–927. [Google Scholar] [CrossRef]
- Al Shaafi, M.M.; Maawadh, A.M.; Al Qahtani, M.Q. Evaluation of Light Intensity Output of QTH and LED Curing Devices in Various Governmental Health Institutions. Oper. Dent. 2011, 36, 356–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ernst, C.P.; Callaway, A.; Masek, A.; Schwarm, H.; Rullmann, I.; Willershausen, B.; Ehlers, V. Visible Light Curing Devices—Irradiance and Use in 302 German Dental Offices. J. Adhes. Dent. 2018, 20, 41–55. [Google Scholar] [CrossRef] [PubMed]

| Search field 1 | (“LED dental curing-lights” OR “dental curing lights “ OR “curing lights dental” OR “high-power LED” OR “high intensity LED” |
| AND | |
| Search field 2 | (“resin-based composite resins” OR “dental resins” OR “dental materials”) |
| Modified CONSORT Checklist of Items for Reporting In Vitro Studies of Dental Materials | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2a | 2b | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
| Park, Roulet and Heintze, 2010 [22] | * | * | * | * | * | * | * | * | |||||||
| Flury et al., 2013 [10] | * | * | * | * | * | * | * | * | |||||||
| Branchal et al., 2015 [31] | * | * | * | * | * | * | * | * | |||||||
| Gonulol, Ozer and Tunc, 2015 [16] | * | * | * | * | * | * | * | ||||||||
| Haenel et al., 2015 [17] | * | * | * | * | * | * | * | * | |||||||
| Watanabe et al., 2015 [33] | * | * | * | * | * | * | * | ||||||||
| Armellin et al., 2016 [20] | * | * | * | * | * | * | * | ||||||||
| Oz, Oz and Arici, 2016 [35] | * | * | * | * | * | * | * | ||||||||
| Peutzfeldt, Lussi and Flury, 2016 [28] | * | * | * | * | * | * | * | * | |||||||
| Bilgic et al., 2017 [27] | * | * | * | * | * | * | * | ||||||||
| Shimokawa et al., 2017 [15] | * | * | * | * | * | * | * | * | |||||||
| Udomthanaporn, Nisalak and Sawaengkit, 2017 [11] | * | * | * | * | * | * | * | ||||||||
| Almeida, Martins and Martins, 2018 [18] | * | * | * | * | * | * | * | * | |||||||
| Daugherty et al., 2018 [14] | * | * | * | * | * | * | * | ||||||||
| Nurlatifah, Eriwati and Indrani, 2018 [19] | * | * | * | * | * | * | * | * | |||||||
| Vinagre et al., 2019 [21] | * | * | * | * | * | * | * | * | |||||||
| Sadeghyar, Watts and Schedle, 2020 [30] | * | * | * | * | * | * | * | ||||||||
| Rocha et al., 2021 [36] | * | * | * | * | * | * | * | * | |||||||
| CONSORT Checklist of Items for Reporting a Randomized Trial of Dental Materials | ||||
|---|---|---|---|---|
| Runnacles et al., 2015 [32] | Watanabe et al., 2015 [33] | Oz, Oz and Arici, 2016 [35] | Gross et al., 2020 [29] | |
| 1a | ||||
| 1b | * | * | * | * |
| 2a | * | * | * | * |
| 2b | * | * | * | * |
| 3a | * | * | * | |
| 3b | ||||
| 4a | * | * | * | * |
| 4b | * | * | * | * |
| 5 | * | * | * | * |
| 6a | * | * | * | * |
| 6b | ||||
| 7a | * | * | * | |
| 7b | ||||
| 8a | ||||
| 8b | ||||
| 9 | ||||
| 10 | ||||
| 11a | ||||
| 11b | ||||
| 12a | * | * | * | * |
| 12b | * | * | * | * |
| 13a | ||||
| 13b | ||||
| 14a | * | |||
| 14b | ||||
| 15 | ||||
| 16 | * | * | * | * |
| 17a | ||||
| 17b | ||||
| 18 | ||||
| 19 | ||||
| 20 | * | * | * | * |
| 21 | * | * | * | * |
| 22 | * | * | * | * |
| 23 | ||||
| 24 | ||||
| 25 | * | * | ||
| Author, Year | Dental Resin-Based Materials | Patients’ Oral Condition | |||
|---|---|---|---|---|---|
| Degree of Conversion | Diametral Tensile Strength | Elastic Modulus | Bond Strength | Temperature Changes in the Pulp | |
| Park, Roulet and Heintze, 2010 [22] | X | ||||
| Flury et al., 2013 [10] | X | ||||
| Branchal et al., 2015 [31] | X | ||||
| Gonulol, Ozer and Tunc, 2015 [16] | X | ||||
| Haenel et al., 2015 [17] | X | ||||
| Runnacles et al., 2015 [32] | X | ||||
| Ward et al., 2015 [34] | X | ||||
| Watanabe et al., 2015 [33] | X | ||||
| Armellin et al., 2016 [20] | X | ||||
| Oz, Oz and Arici, 2016 [35] | X | ||||
| Peutzfeldt, Lussi and Flury, 2016 [28] | X | ||||
| Bilgic et al., 2017 [27] | X | X | |||
| Shimokawa et al., 2017 [15] | X | ||||
| Udomthanaporn, Nisalak and Sawaengkit, 2017 [11] | X | ||||
| Almeida, Martins and Martins, 2018 [18] | X | ||||
| Daugherty et al., 2018 [14] | X | ||||
| Nurlatifah, Eriwati and Indrani, 2018 [19] | X | ||||
| Vinagre et al., 2019 [21] | X | ||||
| Gross et al., 2020 [29] | X | ||||
| Sadeghyar, Watts and Schedle, 2020 [30] | X | ||||
| Rocha et al., 2021 [36] | X | ||||
| Author, Year | Clinical Procedure | Tests Carried Out | Outcomes | |
|---|---|---|---|---|
| Degree of conversion | Flury et al., 2013 [10] | Light curing resin cements through glass ceramics | Directly examined through FT-IR | The higher irradiance emittance resulted in similar degree of conversion compared to standard irradiance values but with the advantage of shorter curing times. |
| Branchal et al., 2015 [31] | Light curing sealants | Indirectly examined through micro hardness values | Among the tested LED curing units, only VALO provided properly curing of opaque-filled and clear-filled sealants as specified by ISO 6874. | |
| Gonulol, Ozer and Tunc, 2015 [16] | Polymerization of resin-based tooth-colored restorative materials | Indirectly assessed through micro hardness values | VALO’s High-power mode can be recommended for clinical applications as it can shorten the time required to adequately polymerize resin-based restorative materials. | |
| Haenel et al., 2015 [17] | Light curing dental resins | Directly examined through FT-IR and indirectly through micro hardness values | The hardness distribution reflects the irradiance distribution of each LCU. Irradiance emittance values and exposure time do not affect the pattern of the hardness distribution, only the hardness level. | |
| Watanabe et al., 2015 [33] | Polymerization of dual-cured resin cement | Indirectly studied through micro hardness values | High-intensity LED units require a shorter irradiation period than halogen and standard LED curing units to obtain Knoop Hardness Numbers similar to those observed during direct irradiation. | |
| Peutzfeldt, Lussi and Flury, 2016 [28] | Light curing resin cements | Indirectly evaluated through micro hardness values | The irradiation protocol significantly influences micromechanical properties of dual curing resin cements due to variation of exposure time, indicating that high- irradiance light-curing has no detrimental effect on polymerization of resin cements. | |
| Shimokawa et al., 2017 [15] | Polymerization of resin-based composites | Directly examined through FT-IR and indirectly through micro hardness values | The irradiance level and emission spectrum affect the polymerization of resin-based composites. Equivalent or higher microhardness and degree of conversion values were achieved when standard irradiance values were used compared to high. | |
| Daugherty et al., 2018 [14] | Polymerization of bulk-fill composites | Directly examined through FT-IR and indirectly through depth of cure | High irradiance and short exposure time may not provide adequate depth of cure and degree of polymerization, which can lead to undesirable clinical properties on bulk-fill composites. | |
| Sadeghyar, Watts and Schedle, 2020 [30] | Light-curing of a bulk fill composite | Indirectly measured by micro hardness numbers | Irradiation with the standard LCU generally gave the highest KHN values for most materials however this difference was material-dependent. | |
| Rocha et al., 2021 [36] | Ultra-fast polymerization of bulk-fill resin-based composite RAFT-modified | Directly measured through FT-NIR and indirectly through depth of cure | No statistical difference in depth of cure and degree of conversion were found between the Standard and Xtra-Power mode, presenting both a lower depth of cure than the claimed by the manufacturer. | |
| Elastic modulus | Bilgic et al., 2017 [27] | Curing of orthodontic adhesives | Evaluated by nano-indentation tests | Orthodontics adhesives cured with 3200 mW/cm2 by VALO® had higher hardness and elastic modulus values than those cured with 1400 mW/cm2. |
| Diametral tensile strength | Nurlatifah, Eriwati and Indrani, 2018 [19] | Curing of packable composite resin | Calculated after loading test with a universal testing machine | The chosen irradiation protocol influences the diametral tensile strength of packable composite resin. |
| Bond strength | Ward et al., 2015 [34] | Brackets cured with a high-intensity LED | Determined by clinical bond failure rates | Both curing methods showed acceptable bond failure rates to be considered clinically valid. |
| Oz, Oz and Arici, 2016 [35] | Metal brackets polymerized intraorally and, to extracted tooth | Evaluated by clinical bond failure rates and shear bond strength values and the adhesive remnant index | Either 10 s of light-curing with Elipar LED or 3 s with a VALO LED can safely accomplish bracket bonding. | |
| Udomthanaporn, Nisalak and Sawaengkit, 2017 [11] | Orthodontic brackets bonded to human premolars | Determined evaluating shear bond strength values and the adhesive remnant index | The SBS generated by VALO curing at 6 s was not significantly different from Bluephase curing at 20 s while FlashMax™ P3 had significantly lowest mean SBS. | |
| Almeida, Martins and Martins, 2018 [18] | Bracket bonding to human premolars | Determined evaluating shear bond strength values and the adhesive remnant index | Reducing exposure time from lead to significantly lower mean values of SBS, even with the use of a high-power LED-LCU. Reduction in time did not affect the amount of adhesive remnant. | |
| Temperature changes in the pulp | Park, Roulet and Heintze, 2010 [22] | Maxillary premolar exposed to light curing units | Measured with a K-type thermocouple | Disparity in the intrapulpal peak temperature during the light-curing process and in the rate of temperature decrease in pulp after switching off the device between curing lights with different power densities was observed. |
| Runnacles et al., 2015 [29] | Human premolars exposed to a light curing unit | Measured with type T thermocouple | Exposing tooth to a polywave LED-LCU develops significant increase in pulp temperature. Most exposure modes led to variations in temperature lower than the potential damage threshold temperature increase of 5.5 °C, although some teeth exposed to high radiant exposures for 60 s exhibited pulp temperature rises above 5.5 °C. | |
| Armellin et al., 2016 [20] | Composite restorations in first molars | Measured with with a type J thermocouple | Intrapulpal temperature increase during composite photocuring is related to the exothermic polymerization reaction, the energy from the light unit and time of exposure. Longer exposure times resulted in higher increase of pulp tissue temperature, although radiant emittance was lower. | |
| Vinagre et al., 2019 [21] | Immediately extracted premolars submitted to light curing procedures | Measuredwith with an Optical Fibber Bragg grating sensor | A significant pulp temperature rise was detected when intact premolars were exposed to LED-LCUs. Curing modes emitting high energy densities produced pulp temperature variations around or above 5.5 °C and might be considered clinically relevant. | |
| Gross et al., 2020 [29] | First premolars requiring extraction exposed to a Polywave LED LCU | Measured with a type T thermocouple | Short exposure to high radiant emittance values were not different from those when teeth were exposed to longer exposure with lower radiant emittance values, given near-similar radiant exposure values. Also, increase values similar to or even higher than the threshold temperature increase of 5.5 °C caused no noticeable histological changes in the pulp tissue. |
| Manufacturer | LED-LCU (Ref. Number) | High-Power Curing Modes | Radiant Emittance (mW/cm2) | Exposure Time (s) | Wavelength Range (nm) | Light Meter Built in | DFU |
|---|---|---|---|---|---|---|---|
| ACTEON, France | MINILED STANDARD® (F02530) | Fast | 2000 | 6 or 12 | 420–480 | Yes | Available at <https://www.acteongroup.com/es/uploads/media/default/0001/01/444188825e19cff843cf686925b79f3efb247df5.pdf> (accessed on 19 February 2020) |
| MINILED SUPERCHARGED® (F05217) | Fast-Cure | 2000 (7.5 mm light tip) 3000 (5.5 mm light tip) | 3, 4, 5 or 10 | 420–480 | Yes | Available at <https://www.acteongroup.com/es/uploads/media/default/0001/01/45de84dd04184927973481ea27a32bd5b126e089.pdf/> (accessed on 19 February 2020) | |
| MINILED ORTHO 2® (F05220) | Fast Cure | 3000 | 4, 8, 12 or 32 | 420–480 | Yes | Available at <https://www.acteongroup.com/us/uploads/media/default/0001/01/d57b6f0c62b68188932a263f44a400fe9b383d76.pdf> (accessed on 19 February 2020) | |
| BA INTERNATIONAL, UK | ULTIMATE BASE290 (BA110200) | Power Level 3 Power Level 4 | 2000 3000 | 1, 3 or 5 1, 3 or 5 | 380–500 | No | Available at <https://www.bainternational.com/pub/media/kuki/download/50/BASE290-IFU-FINAL.pdf> (accessed on 20 February 2020). |
| BADER, Spain | BE LIGHT LED® (09070004) | NF1 | 2000 | 15 to 30 (adjustable) | 420–480 | Yes | Available at <http://www.bader.es/gb/index.php?controller=attachment&id_attachment=69> (accessed on 21 April 2020) |
| LED LIGHT CURING® (090770008) | NF1 | 2000 | 5 to 40 (adjustable) | 420–480 | No | Available at <http://www.bader.es/gb/index.php?controller=attachment&id_attachment=70> (accessed on 21 April 2020) | |
| ONE LED LIGHT® (09070088) | NF1 | 2300 | 1, 5 or 10 | 385–515 | No | NF http://www.bader.es/gb/clinic-equipment/1243-one-led-light-bader.html?search_query=one+light&results=35 (accessed on 21 April 2020) | |
| CLARBEN, Spain | LED CLEAR® (09–080) | Bright Light | 2000 | 5 to 40 (adjustable) | 420–480 | No | Available at <https://clarben.com/_files/200000330-3a62b3b5bd/FT-SGC15.01%20LAMPARA%20LED%20CLEAR.pdf> (accessed on 21 April 2020) |
| CMS DENTAL, Denmark | FLASHMAX™ P3 (100400) | Green Orange Red | 5000 to 6000 | 1 or 3 1 or 3 (two activations with 0.5 s pause) 1 or 3 (repetitive cycles with 0.5 s pause) | 440–480 | No | NF https://www.cmsdental.com/?id=422&c=Technic%20Flash&ulang=2 (accessed on 21 April 2020) |
| FLASHMAX™ P3 WIDE SPECTRUM (100403) | Green Orange Red | 5000 to 6000 | 2 or 4 2 or 4 (two activations with 0.5 s pause) 2 or 4 (repetitive cycles with 0.5 s pause) | 390–480 | No | NF https://www.cmsdental.com/?id=422&c=Technic%20Flash&ulang=2 (accessed on 21 April 2020) | |
| FLASHMAX™ P3 ORTHO (NF)1 | Green Orange Red | 5000 to 6000 | 1 or 3 1 or 3 (two activations with 0.5 s pause) 1 or 3 (repetitive cycles with 0.5 s pause) | 440–480 | No | NF https://www.cmsdental.com/?id=422&c=Technic%20Flash&ulang=2 (accessed on 21 April 2020) | |
| COLTENE, Spain | S.P.E.C.® 3 (60013942) | 3K Ortho | 3000 3000 | 1, 2 or 3 1, 2 or 3 | 430–490 | No | Available at <https://www.coltene.com/pim/DOC/IFU/docifu40001378g-spec3-ifu-multisallaindv1.pdf> (accessed on 18 November 2019) |
| DENTLIGHT, UK | FUSION 5™ (7800080) | Pulse Plasma | 2000 4000 | 3, 5, 10, 20 or 60 3 | 420–490 | No | Available at < http://www.dentlight.com//////////////wp-content/uploads/2019/07/FUSION5-Platform-IFU.pdf> (accessed on 22 April 2020) |
| FUSION GRAND™ (7830060) | Pulse Plasma | 2000 4000 | 3, 5, 10, 20 or 60 3 | 385–490 | No | Available at < http://www.dentlight.com//////////////wp-content/uploads/2019/07/FUSION5-Platform-IFU.pdf> (accessed on 22 April 2020) Available at < http://www.dentlight.com//////////////wp-content/uploads/2019/07/FUSION5-Platform-IFU.pdf> (accessed on 22 April 2020) | |
| FUSION PLUS™ (7820060) | Pulse Plasma | 2000 4000 | 3, 5, 10, 20 or 60 3 | 385–490 | No | NF http://www.diadenteurope.com/producten/small-equipment/d-luxplus-cordless-curing-light (accessed on 22 April 2020) Available at <http://downloads.ivoclarvivadent.com/zoolu-website/media/document/46806/Bluephase+PowerCure> (accessed on 20 November 2019) | |
| DIADENT, The Netherlands | D-LUX+® (4008–1110) | Max Power | 2400 | 1, 2 or 3 | 385–515 | Yes | Available at <http://downloads.ivoclarvivadent.com/zoolu-website/media/document/39483/Bluephase+Style+20i+-+en%2C+de%2C+fr%2C+it%2C+es%2C+pt> (accessed on 18 November 2019) |
| IVOCLAR VIVADENT, Liechtenstein | BLUEPHASE POWER CURE® (667092) | 3sCure Turbo | 3000 2000 | 3 5 | 385–515 | Yes | NF https://www.jmoritaeurope.de/en/products/handpieces-and-instruments/curing-light/pencure/ (accessed on 22 April 2020) |
| BLUEPHASE STYLE 20i® (682110) | Turbo | 2000 | 5 | 385–515 | No | NF https://www.myray.it/en/myray/ (accessed on 22 April 2020) NF https://www.premiumplusuk.com/product/c01-d-led-curing- (accessed on 22 April 2020) | |
| MORITA, Germany | PENCURE 2000 (NF) 1 | High Power | 2000 | 2 or 3 | 380–430 | No | light-with-fibre-optic-light-guide/ (accessed on 15 November 2019) NF https://www.premiumplusuk.com/product/c02-d-led-curing- (accessed on 15 November 2019) |
| MYRAY, Italy | T-LED (70140020) | Standard Quick | 2400 (5 mm light tip) 2200 (8 mm light tip) 3780 (5 mm light tip) | 1, 2 or 3 1, 2 or 3 | 430–490 | Yes | light-90-right-angle-direct-light-source-head/ (accessed on 15 November 2019) |
| PREMIUM PLUS, UK | C01-DUAL RANGE™ (NF) 1 | Turbo 3′ + 3′ | 2000 2000 | 4 3 (two activations with 1 s pause) | 390–480 | Yes | NF https://www.premiumplusuk.com/product/c01-s-led-curing-light-with-fibre-optic-light-guide/ (accessed on 15 November 2019) |
| C02-DUAL RANGE™ (NF) 1 | Turbo 3′ + 3′ | 2500 2000 | 3 3 (two activations with 1 s pause) | 390–480 | Yes | Available at <https://www.acteongroup.com/es/uploads/media/default/0001/01/444188825e19cff843cf686925b79f3efb247df5.pdf> (accessed on 19 February 2020) | |
| C01-SUPER POWER™ (NF)1 | Turbo 3′ + 3′ | 2000 2000 | 4 3 (two activations with 1 s pause) | 440–480 | Yes | Available at <https://www.acteongroup.com/es/uploads/media/default/0001/01/45de84dd04184927973481ea27a32bd5b126e089.pdf> (accessed on 19 February 2020) | |
| C02-SUPER POWER™ (NF) 1 | Turbo 3′ + 3′ | 2500 2000 | 3 3 (two activations with 1s pause) | 440–480 | Yes | Available at <https://www.acteongroup.com/us/uploads/media/default/0001/01/d57b6f0c62b68188932a263f44a400fe9b383d76.pdf> (accessed on 19 February 2020) | |
| ULTRADENT, USA | VALO® (5941) | Xtra Power | 3200 (8 mm light tip) | 3 | 395–480 | No | NF https://www.premiumplusuk.com/product/c02-s-led-curing-light-90-right-angle-direct-light-source-head/ (accessed on 15 November 2019) |
| VALO GRAND® (5972) | Xtra Power | 3200 (12 mm light tip) | 3 | 385–515 | No | NF https://www.ultradent.com/products/procedures/restorative/class-I-II-III-IV-composite-restoration/curing-lights/valo-cordless (accessed on 23 April 2020) | |
| VALO ORTHO® (5942) | Xtra Power Xtra Power Q | 3200 3200 | 1, 2 or 3 3 (five activations with 2 s pause) | 395–480 | No | NF http://www.glwoodpecker.com/index.php?m=content&c=index&a=show&catid=36&id=197 (accessed in 23 April 2020) | |
| WOODPECKER, China | B-CURE® (NF) 1 | Ortho | 2000 | 3 or 5 (ten activations with 1 s pause) | 385–515 | No | NF http://www.glwoodpecker.com/index.php?m=content&c=index&a=show&catid=36&id=195 (accessed on 23 April 2020) |
| B-CURE PLUS® (NF) 1 | Turbo | 2800 to 3000 | 1 or 3 | 385–515 | No | NF http://www.glwoodpecker.com/index.php?m=content&c=index&a=show&catid=36&id=44 (accessed on 23 April 2020) | |
| ILED® (NF) 1 | Turbo | 2300 to 2500 | 1 or 3 | 420–480 | No | NF http://www.glwoodpecker.com/index.php?m=content&c=index&a=show&catid=36&id=159 (accessed on 23 April 2020) | |
| ILED PLUS® (NF) 1 | Turbo | 2300 to 2500 | 1 or 3 | 385–515 | No | NF http://www.glwoodpecker.com/index.php?m=content&c=index&a=show&catid=36&id=45 (accessed on 23 April 2020) | |
| X-CURE® (NF) 1 | High | 2300 to 2500 | 1, 2 or 3 | 385–515 | No | NF https://www.premiumplusuk.com/product/c02-s-led-curing-light-90-right-angle-direct-light-source-head/ (accessed on 15 November 2019) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almeida, R.; Manarte-Monteiro, P.; Domingues, J.; Falcão, C.; Herrero-Climent, M.; Ríos-Carrasco, B.; Lemos, B.F. High-Power LED Units Currently Available for Dental Resin-Based Materials—A Review. Polymers 2021, 13, 2165. https://0-doi-org.brum.beds.ac.uk/10.3390/polym13132165
Almeida R, Manarte-Monteiro P, Domingues J, Falcão C, Herrero-Climent M, Ríos-Carrasco B, Lemos BF. High-Power LED Units Currently Available for Dental Resin-Based Materials—A Review. Polymers. 2021; 13(13):2165. https://0-doi-org.brum.beds.ac.uk/10.3390/polym13132165
Chicago/Turabian StyleAlmeida, Rita, Patricia Manarte-Monteiro, Joana Domingues, Carlos Falcão, Mariano Herrero-Climent, Blanca Ríos-Carrasco, and Bernardo Ferreira Lemos. 2021. "High-Power LED Units Currently Available for Dental Resin-Based Materials—A Review" Polymers 13, no. 13: 2165. https://0-doi-org.brum.beds.ac.uk/10.3390/polym13132165