
Polymeric Denture Base Materials: A Review

 , , ,
, , ,  ,
,  and
and 
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Evolution/History of DBMs
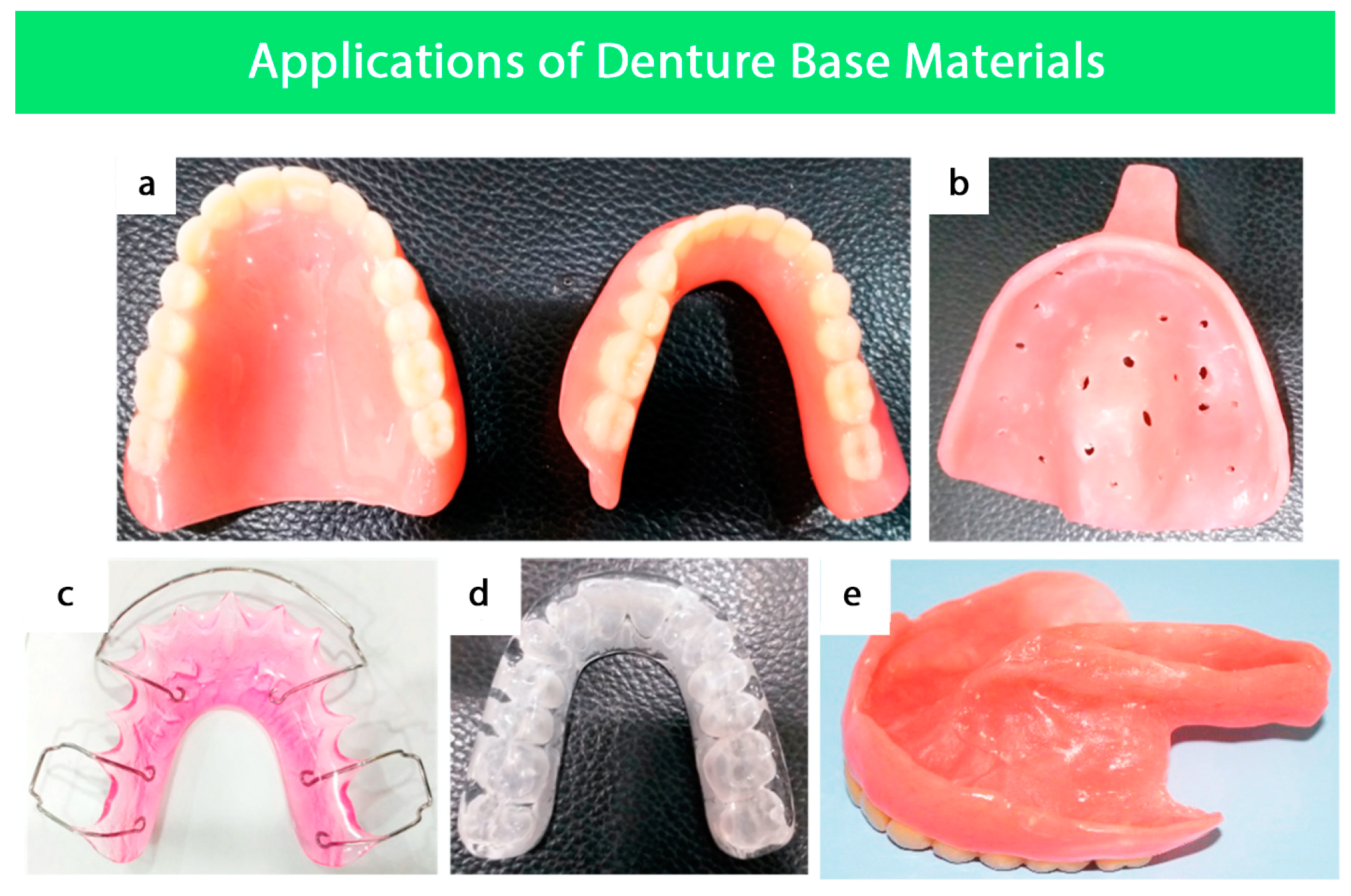
4. Applications of Denture Base Materials
4.1. Fabrication of Removable Partial and Complete Dentures
4.2. Surgical Splints
4.3. Secondary Impression Trays
4.4. Orthodontics
4.5. Obturators
5. Desired Properties of DBMs
5.1. Physical Properties
5.1.1. Sorption and Solubility
5.1.2. Thermal Conductivity
5.1.3. Color Stability
5.1.4. Polymerization Shrinkage
5.1.5. Radiopacity
5.2. Mechanical Properties
5.2.1. Flexural Strength
5.2.2. Fracture Toughness
5.2.3. Impact Strength
5.2.4. Surface Hardness
5.3. Biological Properties
5.3.1. Biocompatibility of Acrylic Resins
Consequences of Biodegradation
Release of Compounds from Acrylic-Based Resins
Biological Effects of the Release
Inner Properties of PMMA
5.3.2. Antimicrobial Modification of PMMA
6. Classification of DBMs
6.1. Polymeric DBMs
6.1.1. Historical Polymeric DBMs
Polycarbonates
Acetal
Polystyrene
6.1.2. Acrylic Resins
Heat-Activated Denture Base Resins
Chemically Activated Denture Base Resin
Pour Type Denture Base Resin
High-Impact Strength Materials
Injection Molding Denture Base Resin
Light-Cured Denture Base Resin
Microwavable Resins
6.1.3. Thermoplastic Resins
Thermoplastic Acetal
Thermoplastic Polycarbonate
Thermoplastic Nylon
Thermoplastic Acrylic Resin “Versacryl”
6.1.4. Modified PMMA
Fiber Reinforcement
Glass Fibers
Polyamides
Polyethylene and Polypropylene
Filler Reinforcement
Metal Oxides Alumina (Al2O3)
6.1.5. Other Polymeric Materials
PEEK
Nylon
6.2. Base Metal Alloys (BMA)
7. Method of Construction
7.1. Conventional Method
7.1.1. Resin Denture Base
7.1.2. Metal Denture Base
7.2. Computer-Aided Design and Manufacturing (CAD/CAM) and Rapid Prototyping
7.2.1. Complete Denture
7.2.2. Partial Denture
Milled Titanium Framework for RPDs
Additive Manufacturing of Titanium Framework for RPDs
8. Comparison of Polymeric and Casting Alloys DBMs
9. Conclusions and Future Aspects
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Hassan, M.; Asghar, M.; Din, S.U.; Zafar, M.S. Thermoset polymethacrylate-based materials for dental applications. In Materials for Biomedical Engineering; Elsevier: Amsterdam, The Netherlands, 2019; pp. 273–308. [Google Scholar]
- Zafar, M.S. Prosthodontic Applications of Polymethyl Methacrylate (PMMA): An Update. Polymers 2020, 12, 2299. [Google Scholar] [CrossRef]
- Anusavice, K.J.; Shen, C.; Rawls, H.R. Phillips’ Science of Dental Materials; Elsevier Health Sciences: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Rickman, L.J.; Padipatvuthikul, P.; Satterthwaite, J.D.; McCord, J.F.; Grey, N.J.; Winstanley, R.B.; Johnson, A.; George, G.S.; Hussain, S.; Welfare, R.; et al. Contemporary denture base resins: Part 1. Dent. Updat. 2012, 39, 25–30. [Google Scholar] [CrossRef] [Green Version]
- Van Noort, R.; Barbour, M. Introduction to Dental Materials-e-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Khan, A.A.; Fareed, M.A.; Alshehri, A.H.; Aldegheishem, A.; Alharthi, R.; Saadaldin, S.A.; Zafar, M.S. Mechanical Properties of the Modified Denture Base Materials and Polymerization Methods: A Systematic Review. Int. J. Mol. Sci. 2022, 23, 5737. [Google Scholar] [CrossRef]
- Cohen, R.A. Methods and Materials Used for Artificial Teeth [Abridged]; SAGE Publications: New York, NY, USA, 1959. [Google Scholar]
- Sheejith, M.; Swapna, C.; Roshy, S.N.G. Evolution of denture base material: From past to new era. IOSR J. Dent. Medic. Sci. 2018, 17, 23–27. [Google Scholar]
- Sheng, T.; Shafee, M.; Ariffin, Z.; Jaafar, M. Review on poly-methyl methacrylate as denture base materials. Malays. J. Microsc. 2018, 14, 1–16. [Google Scholar]
- Jadhav, S.S.; Mahajan, N.; Sethuraman, R. Comparative evaluation of the amount of the residual monomer in conventional and deep-frozen heat cure polymethylmethacrylate acrylic resin: An in vitro study. J. Indian Prosthodont. Soc. 2018, 18, 147–153. [Google Scholar] [PubMed]
- Singh, R.D.; Gautam, R.; Siddhartha, R.; Singh, B.P.; Chand, P.; Sharma, V.P.; Jurel, S.K. High Performance Liquid Chromatographic Determination of Residual Monomer Released from Heat-Cured Acrylic Resin. An In Vivo Study. J. Prosthodont. 2013, 22, 358–361. [Google Scholar] [CrossRef] [PubMed]
- Baemmert, R.J.; Lang, B.R.; Barco, M.T.; Billy, E.J. Effects of denture teeth on the dimensional accuracy of acrylic resin denture bases. Int. J. Prosthodont. 1990, 3, 528–537. [Google Scholar]
- International Organization for Standardization. Dentistry–Base Polymers–Part 1: Denture Base Polymers; International Organization of Standardization (ISO): Geneva, Switzerland, 2013. [Google Scholar]
- Tuna, S.H.; Keyf, F.; Gumus, H.O.; Uzun, C. The Evaluation of Water Sorption/Solubility on Various Acrylic Resins. Eur. J. Dent. 2008, 2, 191–197. [Google Scholar] [CrossRef] [Green Version]
- Kotian, R.; Saini, R.; Madhyastha, P.; Srikant, N. Comparative study of sorption and solubility of heat-cure and self-cure acrylic resins in different solutions. Indian J. Dent. Res. 2016, 27, 288–294. [Google Scholar] [CrossRef]
- Kopperud, H.M.; Kleven, I.S.; Wellendorf, H. Identification and quantification of leachable substances from polymer-based orthodontic base-plate materials. Eur. J. Orthod. 2011, 33, 26–31. [Google Scholar] [CrossRef] [Green Version]
- LLang, A.; Mattie, P.A.; Rawis, H.R. The effect of triphenylbismuth on the radiopacity and performance properties of com-pression-and injection-molded denture resins. J. Prosthodont. 2000, 9, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, D.B.; de Souza, R.F.; Pero, A.C.; Marra, J.; Compagnoni, M.A. Flexural strength of acrylic resins polymerized by different cycles. J. Appl. Oral Sci. 2007, 15, 424–428. [Google Scholar] [CrossRef] [PubMed]
- Stafford, G.; Huggett, R.; Causton, B. Fracture toughness of denture base acrylics. J. Biomed. Mater. Res. 1980, 14, 359–371. [Google Scholar] [CrossRef]
- Robinson, J.; McCabe, J. Impact strength of acrylic resin denture base materials with surface defects. Dent. Mater. 1993, 9, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Zafar, M.S.; Ahmed, N. Nanoindentation and surface roughness profilometry of poly methyl methacrylate denture base ma-terials. Technol. Health Care 2014, 22, 573–581. [Google Scholar] [CrossRef]
- Ibrahim, S.A.; Lafta, S.H.; Hussain, W.A. Effect of Reinforcing PMMA Denture Base Material by Stainless Steel 316L Wires on Flexural Strength. J. Appl. Sci. Nanotechnol. 2023, 3, 51–58. [Google Scholar] [CrossRef]
- Potewiratnanond, P.; Ekrojanakul, C.; Harikul, T.; Kositvanich, R. Wear effects between polymethyl methacrylate occlusal splints and opposing dentin surfaces during bruxism mimicking events. BDJ Open 2023, 9, 21. [Google Scholar] [CrossRef]
- León, B.L.T.; Cury, A.A.D.B.; Garcia, R.C.M.R. Loss of residual monomer from resilient lining materials processed by different methods. Rev. Odonto Ciência 2008, 23, 215–219. [Google Scholar]
- Faltermeier, A.; Rosentritt, M.; Müssig, D. Acrylic removable appliances: Comparative evaluation of different postpolymerization methods. Am. J. Orthod. Dentofac. Orthop. 2007, 131, 301.e16–301.e22. [Google Scholar] [CrossRef]
- Kawahara, T.; Nomura, Y.; Tanaka, N.; Teshima, W.; Okazaki, M.; Shintani, H. Leachability of plasticizer and residual monomer from commercial temporary restorative resins. J. Dent. 2004, 32, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Ferracane, J.L. Hygroscopic and hydrolytic effects in dental polymer networks. Dent. Mater. 2006, 22, 211–222. [Google Scholar] [CrossRef] [PubMed]
- Santerre, J.; Shajii, L.; Leung, B. Relation of Dental Composite Formulations to Their Degradation and the Release of Hydrolyzed Polymeric-Resin-Derived Products. Crit. Rev. Oral Biol. Med. 2001, 12, 136–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santerre, J.; Shajii, L.; Tsang, H. Biodegradation of commercial dental composites by cholesterol esterase. J. Dent. Res. 1999, 78, 1459–1468. [Google Scholar] [CrossRef]
- Finer, Y.; Santerre, J. Salivary Esterase Activity and Its Association with the Biodegradation of Dental Composites. J. Dent. Res. 2004, 83, 22–26. [Google Scholar] [CrossRef]
- Jaffer, F.; Finer, Y.; Santerre, J. Interactions between resin monomers and commercial composite resins with human saliva derived esterases. Biomaterials 2002, 23, 1707–1719. [Google Scholar] [CrossRef]
- Lin, B.A.; Jaffer, F.; Duff, M.D.; Tang, Y.W.; Santerre, J.P. Identifying enzyme activities within human saliva which are relevant to dental resin composite biodegradation. Biomaterials 2005, 26, 4259–4264. [Google Scholar] [CrossRef]
- Yourtee, D.; Smith, R.; Russo, K.; Burmaster, S.; Cannon, J.; Eick, J.; Kostoryz, E. The stability of methacrylate biomaterials when enzyme challenged: Kinetic and systematic evaluations. J. Biomed. Mater. Res. 2001, 57, 522–531. [Google Scholar] [CrossRef]
- Larsen, I.B.; Munksgaard, E.G. Effect of human saliva on surface degradation of composite resins. Eur. J. Oral Sci. 1991, 99, 254–261. [Google Scholar] [CrossRef]
- Larsen, I.; Freund, M.; Munksgaard, E. Change in Surface Hardness of BisGMA/TEGDMA Polymer due to Enzymatic Action. J. Dent. Res. 1992, 71, 1851–1853. [Google Scholar] [CrossRef]
- Iqbal, Z.; Zafar, M.S. Role of antifungal medicaments added to tissue conditioners: A systematic review. J. Prosthodont. Res. 2016, 60, 231–239. [Google Scholar] [CrossRef]
- Shaikh, M.S.; Alnazzawi, A.; Habib, S.R.; Lone, M.A.; Zafar, M.S. Therapeutic Role of Nystatin Added to Tissue Conditioners for Treating Denture-Induced Stomatitis: A Systematic Review. Prosthesis 2021, 3, 61–74. [Google Scholar] [CrossRef]
- D’Ambrosio, F.; Santella, B.; Di Palo, M.P.; Giordano, F.; Giudice, R.L. Characterization of the Oral Microbiome in Wearers of Fixed and Removable Implant or Non-Implant-Supported Prostheses in Healthy and Pathological Oral Conditions: A Narrative Review. Microorganisms 2023, 11, 1041. [Google Scholar] [CrossRef] [PubMed]
- Chladek, G.; Nowak, M.; Pakieła, W.; Mertas, A. Effect of Candida albicans Suspension on the Mechanical Properties of Denture Base Acrylic Resin. Materials 2022, 15, 3841. [Google Scholar] [CrossRef] [PubMed]
- Gligorijević, N.; Mihajlov-Krstev, T.; Kostić, M.; Nikolić, L.; Stanković, N.; Nikolić, V.; Dinić, A.; Igić, M.; Bernstein, N. Antimicrobial properties of silver-modified denture base resins. Nanomaterials 2022, 12, 2453. [Google Scholar] [CrossRef] [PubMed]
- Farid, D.A.M.; Zahari, N.A.H.; Said, Z.; Ghazali, M.I.M.; Hao-Ern, L.; Zol, S.M.; Aldhuwayhi, S.; Alauddin, M.S. Modification of Polymer Based Dentures on Biological Properties: Current Update, Status, and Findings. Int. J. Mol. Sci. 2022, 23, 10426. [Google Scholar] [CrossRef]
- Willershausen, B.; Callaway, A.; Ernst, C.P.; Stender, E. The influence of oral bacteria on the surfaces of resin-based dental re-storative materials-an in vitro study. Int. Dent. J. 1999, 49, 231–239. [Google Scholar] [CrossRef]
- Bettencourt, A.F.; Neves, C.B.; de Almeida, M.S.; Pinheiro, L.M.; e Oliveira, S.A.; Lopes, L.P.; Castro, M.F. Biodegradation of acrylic based resins: A review. Dent. Mater. 2010, 26, e171–e180. [Google Scholar] [CrossRef]
- Ebadian, B.; Razavi, M.; Soleimanpour, S.; Mosharraf, R. Evaluation of Tissue Reaction to Some Denture-base Materials: An Animal Study. J. Contemp. Dent. Pract. 2008, 9, 67–74. [Google Scholar] [CrossRef]
- Boeckler, A.F.; Morton, D.; Poser, S.; Dette, K.-E. Release of dibenzoyl peroxide from polymethyl methacrylate denture base resins: An in vitro evaluation. Dent. Mater. 2008, 24, 1602–1607. [Google Scholar] [CrossRef]
- Munksgaard, E.C. Plasticizers in denture soft-lining materials: Leaching and biodegradation. Eur. J. Oral Sci. 2005, 113, 166–169. [Google Scholar] [CrossRef] [PubMed]
- Graham, B.; Jones, D.; Sutow, E. An in vivo and in vitro Study of the Loss of Plasticizer from Soft Polymer-gel Materials. J. Dent. Res. 1991, 70, 870–873. [Google Scholar] [CrossRef] [PubMed]
- Zissis, A.; Yannikakis, S.; Polyzois, G.; Harrison, A. A long term study on residual monomer release from denture materials. Eur. J. Prosthodont. Restor. Dent. 2008, 16, 81. [Google Scholar] [PubMed]
- Kawaguchi, M.; Takahashi, Y.; Fukushima, T.; Habu, T. Effect of light-exposure duration on the amount of leachable monomers from light-activated reline material. J. Prosthet. Dent. 1996, 75, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.L.; Chen, Y.T.; Lee, S.Y.; Shieh, T.M.; Hung, S.L. Cytotoxic effects of dental resin liquids on primary gingival fibroblasts and periodontal ligament cells in vitro. J. Oral Rehabil. 2004, 31, 1165–1172. [Google Scholar] [CrossRef]
- Sofou, A.; Tsoupi, I.; Karayannis, M.; Owall, B. Determination of residual monomers released from soft lining materials with the use of HPLC. Pak. J. Anal. Environ. Chem. 2007, 8, 10. [Google Scholar]
- Brożek, R.; Rogalewicz, R.; Koczorowski, R.; Voelkel, A. The influence of denture cleansers on the release of organic compounds from soft lining materials. J. Environ. Monit. 2008, 10, 770–774. [Google Scholar]
- Gonçalves, T.S.; de Menezes, L.M.; Silva, L.E.A. Residual monomer of autopolymerized acrylic resin according to different ma-nipulation and polishing methods: An in situ evaluation. Angle Orthod. 2008, 78, 722–727. [Google Scholar] [CrossRef]
- Urban, V.M.; Machado, A.L.; Vergani, C.E.; Giampaolo, E.T.; Pavarina, A.C.; de Almeida, F.G.; Cass, Q.B. Effect of water-bath post-polymerization on the mechanical properties, degree of conversion, and leaching of residual compounds of hard chairside reline resins. Dent. Mater. 2009, 25, 662–671. [Google Scholar] [CrossRef]
- Koda, T.; Tsuchiya, H.; Yamauchi, M.; Ohtani, S.; Takagi, N.; Kawano, J. Leachability of denture-base acrylic resins in artificial saliva. Dent. Mater. 1990, 6, 13–16. [Google Scholar] [CrossRef]
- Kedjarune, U.; Charoenworaluk, N.; Koontongkaew, S. Release of methyl methacrylate from heat-curved and autopolymerized resins: Cytotoxicity testing related to residual monomer. Aust. Dent. J. 1999, 44, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Baker, S.; Brooks, S.; Walker, D. The Release of Residual Monomeric Methyl Methacrylate from Acrylic Appliances in the Human Mouth: An Assay for Monomer in Saliva. J. Dent. Res. 1988, 67, 1295–1299. [Google Scholar]
- Azzarri, M.; Cortizo, M.; Alessandrini, J. Effect of the curing conditions on the properties of an acrylic denture base resin mi-crowave-polymerised. J. Dent. 2003, 31, 463–468. [Google Scholar]
- Çelebi, N.; Yüzügüllü, B.; Canay, Ş.; Yücel, Ü. Effect of polymerization methods on the residual monomer level of acrylic resin denture base polymers. Polym. Adv. Technol. 2008, 19, 201–206. [Google Scholar] [CrossRef]
- Lygre, H.; Solheim, E.; Gjerdet, N.R.; Berg, E. Leaching of organic additives from dentures in vivo. Acta Odontol. Scand. 1993, 51, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Lygre, H.; Klepp, K.N.; Solheim, E.; Gjerdet, N.R. Leaching of additives and degradation products from cold-cured orthodontic resins. Acta Odontol. Scand. 1994, 52, 150–156. [Google Scholar] [PubMed]
- Tsuchiya, H.; Hoshino, Y.; Tajima, K.; Takagi, N. Leaching and cytotoxicity of formaldehyde and methyl methacrylate from acrylic resin denture base materials. J. Prosthet. Dent. 1994, 71, 618–624. [Google Scholar] [CrossRef]
- Hauser, R.; Calafat, A. Phthalates and human health. Occup. Environ. Med. 2005, 62, 806–818. [Google Scholar] [CrossRef] [Green Version]
- Pielichowski, K.; Njuguna, J.; Majka, T.M. Thermal Degradation of Polymeric Materials; Elsevier: Amsterdam, The Netherlands, 2022. [Google Scholar]
- Sadamori, S.; Kotani, H.; Hamada, T. The usage period of dentures and their residual monomer contents. J. Prosthet. Dent. 1992, 68, 374–376. [Google Scholar] [CrossRef]
- Sofou, A.; Tsoupi, I.; Emmanouil, J.; Karayannis, M. HPLC determination of residual monomers released from heat-cured acrylic resins. Anal. Bioanal. Chem. 2005, 381, 1336–1346. [Google Scholar] [CrossRef]
- de Mello, J.A.N.; Braun, K.O.; Rached, R.N.; Cury, A.A.D.B. Reducing the negative effects of chemical polishing in acrylic resins by use of an additional cycle of polymerization. J. Prosthet. Dent. 2003, 89, 598–602. [Google Scholar] [CrossRef]
- Lefebvre, C.A.; Schuster, G.S.; Marr, J.C.; Knoernschild, K.L. The effect of pH on the cytotoxicity of eluates from denture base resins. Int. J. Prosthodont. 1995, 8, 122–128. [Google Scholar] [PubMed]
- Tsuchiya, H.; Hoshino, Y.; Kato, H.; Takagi, N. Flow injection analysis of formaldehyde leached from denture-base acrylic resins. J. Dent. 1993, 21, 240–243. [Google Scholar] [CrossRef] [PubMed]
- Keyf, F.; Keyf, A.I. Harmful effects of methylmethacrylate and formaldehyde from acrylic resin denture base materials. Saudi Dent. J. 1998, 10, 23–28. [Google Scholar]
- Hashimoto, Y.; Kawaguchi, M.; Miyazaki, K.; Nakamura, M. Estrogenic activity of tissue conditioners in vitro. Dent. Mater. 2003, 19, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Jorge, J.H.; Giampaolo, E.T.; Machado, A.L.; Vergani, C.E. Cytotoxicity of denture base acrylic resins: A literature review. J. Prosthet. Dent. 2003, 90, 190–193. [Google Scholar] [CrossRef]
- Golbidi, F.; Asghari, G. The level of residual monomer in acrylic denture base materials. Res. J. Biol. Sci. 2009, 4, 244–249. [Google Scholar]
- Giunta, J.; Zablotsky, N. Allergic stomatitis caused by self-polymerizing resin. Oral Surg. Oral Med. Oral Pathol. 1976, 41, 631–637. [Google Scholar] [CrossRef]
- Huang, F.-M.; Tai, K.-W.; Hu, C.-C.; Chang, Y.-C. Cytotoxic effects of denture base materials on a permanent human oral epi-thelial cell line and on primary human oral fibroblasts in vitro. Int. J. Prosthodont. 2001, 14, 439–443. [Google Scholar]
- Schuster, G.S.; Lefebvre, C.A.; Dirksen, T.R.; Knoernschild, K.L.; Caughman, G.B. Relationships between denture base resin cytotoxicity and cell lipid metabolism. Int. J. Prosthodont. 1995, 8, 580–586. [Google Scholar]
- Yang, H.-W.; Chou, L.S.-S.; Chou, M.-Y.; Chang, Y.-C. Assessment of genetic damage by methyl methacrylate employing in vitro mammalian test system. Biomaterials 2003, 24, 2909–2914. [Google Scholar] [CrossRef]
- Jorge, J.H.; Giampaolo, E.T.; Vergani, C.E.; Machado, A.L.; Pavarina, A.C.; Carlos, I.Z. Effect of post-polymerization heat treat-ments on the cytotoxicity of two denture base acrylic resins. J. Appl. Oral Sci. 2006, 14, 203–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schweikl, H.; Schmalz, G.; Spruss, T. The induction of micronuclei in vitro by unpolymerized resin monomers. J. Dent. Res. 2001, 80, 1615–1620. [Google Scholar] [CrossRef]
- Schweikl, H.; Spagnuolo, G.; Schmalz, G. Genetic and Cellular Toxicology of Dental Resin Monomers. J. Dent. Res. 2006, 85, 870–877. [Google Scholar] [CrossRef] [PubMed]
- Dixon, D.L.; Breeding, L.C.; Ekstrand, K.G. Linear dimensional variability of three denture base resins after processing and in water storage. J. Prosthet. Dent. 1992, 68, 196–200. [Google Scholar] [CrossRef]
- Cucci, A.L.M.; Rached, R.N.; Giampaolo, E.T.; Vergani, C.E. Tensile bond strengths of hard chairside reline resins as influenced by water storage. J. Oral Rehabil. 1999, 26, 631–634. [Google Scholar] [CrossRef] [PubMed]
- Anusavice, K.J. Philip’s Science of Dental Materials, 11th ed.; Elsevier Science: St. Louis, MO, USA, 2003; p. 96. [Google Scholar]
- Mese, A.; Guzel, K.G. Effect of storage duration on the hardness and tensile bond strength of silicone- and acrylic resin-based resilient denture liners to a processed denture base acrylic resin. J. Prosthet. Dent. 2008, 99, 153–159. [Google Scholar] [CrossRef]
- Dixon, D.L.; Ekstrand, K.G.; Breeding, L.C. The transverse strengths of three denture base resins. J. Prosthet. Dent. 1991, 66, 510–513. [Google Scholar] [CrossRef]
- Takahashi, Y.; Chai, J.; Kawaguchi, M. Equilibrium strengths of denture polymers subjected to long-term water immersion. Int. J. Prosthodont. 1999, 12, 348–352. [Google Scholar]
- Craig, R. Scope and History of Restorative Materials, Restorative Dental Materials, 11th ed.; Mosby, Inc.: St. Louis, MO, USA, 2002; pp. 1–18. [Google Scholar]
- Muraoka, G.; Takahashi, H.; Hayakawa, I. Effects of cyclic loading on viscoelastic properties of soft lining materials. Dent. Mater. J. 2003, 22, 251–261. [Google Scholar] [CrossRef] [Green Version]
- Jepson, N.J.; McGill, J.T.; McCabe, J.F. Influence of dietary simulating solvents on the viscoelasticity of temporary soft lining materials. J. Prosthet. Dent. 2000, 83, 25–31. [Google Scholar] [CrossRef]
- Ferracane, J.; Berge, H. Fracture Toughness of Experimental Dental Composites Aged in Ethanol. J. Dent. Res. 1995, 74, 1418–1423. [Google Scholar] [CrossRef] [PubMed]
- Al-Bakri, I.; Harty, D.; Al-Omari, W.; Swain, M.; Chrzanowski, W.; Ellakwa, A. Surface characteristics and microbial adherence ability of modified polymethylmethacrylate by fluoridated glass fillers. Aust. Dent. J. 2014, 59, 482–489. [Google Scholar] [CrossRef]
- Tsutsumi, C.; Takakuda, K.; Wakabayashi, N. Reduction of Candida biofilm adhesion by incorporation of prereacted glass ionomer filler in denture base resin. J. Dent. 2016, 44, 37–43. [Google Scholar] [CrossRef]
- Sawada, T.; Sawada, T.; Kumasaka, T.; Hamada, N.; Shibata, T.; Nonami, T.; Kimoto, K. Self-cleaning elects of acrylic F. Gerodontology 2014, 31, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Shibata, T.; Hamada, N.; Kimoto, K.; Sawada, T.; Sawada, T.; Kumada, H.; Umemoto, T.; Toyoda, M. Antifungal e_ect of acrylic resin containing apatite-coated TiO2 photocatalyst. Dent. Mater. J. 2007, 26, 437–444. [Google Scholar] [CrossRef] [Green Version]
- Akihiro Yoshihara, D.; Sakuma, P.S.; Kobayashi, P.S.; Miyazaki, P.H. Antimicrobial effect of fluoride mouthrinse on mutans streptococci and lactobacilli in saliva. Pediatr. Dent. 2001, 23, 113–117. [Google Scholar] [PubMed]
- Casemiro, L.A.; Martins, C.H.G.; Pires-De-Souza, F.d.C.P.; Panzeri, H. Antimicrobial and mechanical properties of acrylic resins with incorporated silver-zinc zeolite—Part I. Gerodontology 2008, 25, 187–194. [Google Scholar] [CrossRef]
- Flores, J.C.; Garcia, R.; Villanueva, G.; Acosta-Torres, L. Antimicrobial poly (methyl methacrylate) with silver nanoparticles for dentistry: A systematic review. Appl. Sci. 2020, 10, 4007. [Google Scholar]
- Kurt, A.; Erkose-Genc, G.; Uzun, M.; Emrence, Z.; Ustek, D.; Isik-Ozkol, G. The antifungal activity and cytotoxicity of silver containing denture base material. Niger. J. Clin. Pract. 2017, 20, 290–295. [Google Scholar] [CrossRef] [Green Version]
- Acosta-Torres, L.S.; Mendieta, I.; Nunez-Anita, R.E.; Cajero-Juarez, M.; Castano, V.M. Cytocompatible antifungal acrylic resin containing silver nanoparticles for dentures. Int. J. Nanomed. 2012, 7, 4777–4786. [Google Scholar]
- Monteiro, D.R.; Gorup, L.F.; Takamiya, A.S.; de Camargo, E.R.; Filho, A.C.R.; Barbosa, D.B. Silver Distribution and Release from an Antimicrobial Denture Base Resin Containing Silver Colloidal Nanoparticles. J. Prosthodont. 2012, 21, 7–15. [Google Scholar] [CrossRef]
- Mangal, U.; Kim, J.-Y.; Seo, J.-Y.; Kwon, J.-S.; Choi, S.-H. Novel Poly(Methyl Methacrylate) Containing Nanodiamond to Improve the Mechanical Properties and Fungal Resistance. Materials 2019, 12, 3438. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.-H.; El-Fiqi, A.; Jo, J.-K.; Kim, D.-A.; Kim, S.-C.; Jun, S.-K.; Kim, H.-W.; Lee, H.-H. Development of long-term antimicrobial poly(methyl methacrylate) by incorporating mesoporous silica nanocarriers. Dent. Mater. 2016, 32, 1564–1574. [Google Scholar] [CrossRef] [PubMed]
- Gad, M.M.; Al-Thobity, A.M.; Fouda, S.M.; Näpänkangas, R.; Raustia, A. Flexural and Surface Properties of PMMA Denture Base Material Modified with Thymoquinone as an Antifungal Agent. J. Prosthodont. 2020, 29, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Makvandi, P.; Jamaledin, R.; Jabbari, M.; Nikfarjam, N.; Borzacchiello, A. Antibacterial quaternary ammonium compounds in dental materials: A systematic review. Dent. Mater. 2018, 34, 851–867. [Google Scholar] [CrossRef] [PubMed]
- Makvandi, P.; Ghaemy, M.; Mohseni, M. Synthesis and characterization of photo-curable bis-quaternary ammonium di-methacrylate with antimicrobial activity for dental restoration materials. Eur. Polym. J. 2016, 74, 81–90. [Google Scholar] [CrossRef]
- Makvandi, P.; Ghaemy, M.; Ghadiri, A.; Mohseni, M. Photocurable, antimicrobial quaternary ammonium–modified nano-silica. J. Dent. Res. 2015, 94, 1401–1407. [Google Scholar] [CrossRef]
- Pesci-Bardon, C.; Fosse, T.; Serre, D.; Madinier, I. In vitro antiseptic properties of an ammonium compound combined with denture base acrylic resin. Gerodontology 2006, 23, 111–116. [Google Scholar] [CrossRef]
- Pesci-Bardon, C.; Fosse, T.; Madinier, I.; Serre, D. Flores denture acrylic resin. Lett. Appl. Microbiol. 2004, 39, 226–231. [Google Scholar] [CrossRef]
- Delfi, M.; Ghomi, M.; Zarrabi, A.; Mohammadinejad, R.; Taraghdari, Z.B.; Ashrafizadeh, M.; Zare, E.N.; Agarwal, T.; Padil, V.V.T.; Mokhtari, B.; et al. Functionalization of Polymers and Nanomaterials for Biomedical Applications: Antimicrobial Platforms and Drug Carriers. Prosthesis 2020, 2, 117–139. [Google Scholar] [CrossRef]
- Mai, H.-N.; Kim, D.-Y.; Hyun, D.C.; Park, J.H.; Lee, S.M.; Lee, D. A New Antibacterial Agent-Releasing Polydimethylsiloxane Coating for Polymethyl Methacrylate Dental Restorations. J. Clin. Med. 2019, 8, 1831. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.-H.; Jo, J.-K.; Kim, D.-A.; Patel, K.D.; Kim, H.-W.; Lee, H.-H. Nano-graphene oxide incorporated into PMMA resin to prevent microbial adhesion. Dent. Mater. 2018, 34, e63–e72. [Google Scholar] [CrossRef] [PubMed]
- Ratanajanchai, M.; Kanchanavasita, W.; Suputtamongkol, K.; Wonglamsam, A.; Thamapipol, S.; Sae-Khow, O. Heat-cured poly(methyl methacrylate) resin incorporated with di_erent food preservatives as an anti-microbial denture base material. J. Dent. Sci. 2020, 6, 706–712. [Google Scholar]
- Lassila, L.; Vallittu, P. Denture base polymer Alldent Sinomer®: Mechanical properties, water sorption and release of residual compounds. J. Oral Rehabil. 2001, 28, 607–613. [Google Scholar] [CrossRef]
- Najeeb, S.; Zafar, M.S.; Khurshid, Z.; Siddiqui, F. Applications of polyetheretherketone (PEEK) in oral implantology and pros-thodontics. J. Prosthodont. Res. 2016, 60, 12–19. [Google Scholar] [CrossRef]
- Zol, S.M.; Alauddin, M.S.; Said, Z.; Ghazali, M.I.M.; Hao-Ern, L.; Farid, D.A.M.; Zahari, N.A.F.H.; Al-Khadim, A.H.A.; Aziz, A.H.A. Description of Poly (aryl-ether-ketone) Materials (PAEKs), Polyetheretherketone (PEEK) and Polyetherketon-eketone (PEKK) for Application as a Dental Material: A Materials Science Review. Polymers 2023, 15, 2170. [Google Scholar] [CrossRef]
- Silva, L.S.; Bento, V.A.A.; Brunetto, J.L.; Pesqueira, A.A. Polyetheretherketone materials for removable partial denture frameworks: An integrative review. Gen. Dent. 2023, 71, 58–62. [Google Scholar]
- Alqurashi, H.; Khurshid, Z.; Syed, A.U.Y.; Habib, S.R.; Rokaya, D.; Zafar, M.S. Polyetherketoneketone (PEKK): An emerging biomaterial for oral implants and dental prostheses. J. Adv. Res. 2021, 28, 87–95. [Google Scholar] [CrossRef]
- Consani, R.L.X.; Domitti, S.S.; Barbosa, C.M.R.; Consani, S. Effect of commercial acrylic resins on dimensional accuracy of the maxillary denture base. Braz. Dent. J. 2002, 13, 57–60. [Google Scholar]
- Cruzeiro, M.T.R.; Moraes, F.A.; Kaizer, M.R.; Moreira, M.L.; Zhang, Y.; Moraes, R.R.; Cava, S.S. Functionalized pink Al2O3: Mn pigments applied in prosthetic dentistry. J. Prosthet. Dent. 2017, 118, 771–777. [Google Scholar] [CrossRef] [Green Version]
- Alrahlah, A.; Fouad, H.; Hashem, M.; Niazy, A.A.; AlBadah, A. Titanium oxide (TiO2)/polymethylmethacrylate (PMMA) denture base nanocomposites: Mechanical, vis-coelastic and antibacterial behavior. Materials 2018, 11, 1096. [Google Scholar] [CrossRef] [Green Version]
- Alamgir; Mallick, A.; Nayak, G.C.; Tiwari, S.K. Development of PMMA/TiO2 nanocomposites as excellent dental materials. J. Mech. Sci. Technol. 2019, 33, 4755–4760. [Google Scholar] [CrossRef]
- Grant, A.; Atkinson, H. Comparison between dimensional accuracy of dentures produced with pour-type resin and with heat-processed materials. J. Prosthet. Dent. 1971, 26, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Nogueira, S.S.; Ogle, R.E.; Davis, E.L. Comparison of accuracy between compression- and injection-molded complete dentures. J. Prosthet. Dent. 1999, 82, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Tandon, R.; Gupta, S.; Agarwal, S.K. Denture base materials: From past to future. Indian J. Dent. Sci. 2010, 2, 33–39. [Google Scholar]
- Sakaguchi, R.L.; Powers, J.M. Craig’s Restorative Dental Materials-e-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Phoenix, R.D.; Mansueto, M.A.; Ackerman, N.A.; Jones, R.E. Evaluation of Mechanical and Thermal Properties of Commonly Used Denture Base Resins. J. Prosthodont. 2004, 13, 17–27. [Google Scholar] [CrossRef]
- Kj, A. Phillips’ Science of Dental Materials; WB Saunders: St. Louis, MO, USA, 2003; Volume 596, pp. 41–43. [Google Scholar]
- John, J.; Gangadhar, S.A.; Shah, I. Flexural strength of heat-polymerized polymethyl methacrylate denture resin reinforced with glass, aramid, or nylon fibers. J. Prosthet. Dent. 2001, 86, 424–427. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.-J.; Bok, S.-B.; Bae, J.-Y.; Lee, H.-H. Comparative adaptation accuracy of acrylic denture bases evaluated by two different methods. Dent. Mater. J. 2010, 29, 411–417. [Google Scholar] [CrossRef]
- Becker, C.M.; Smith, D.E.; Nicholls, J.I. The comparison of denture-base processing techniques. Part II. Dimensional changes due to processing. J. Prosthet. Dent. 1977, 37, 450–459. [Google Scholar] [CrossRef]
- Fujisawa, M.; Adachi, K.; Tsuruta, S.; Ishibashi, K. A procedure for fitting a fixed partial denture to an existing removable partial denture. J. Prosthet. Dent. 2004, 91, 392–394. [Google Scholar] [CrossRef]
- Garfunkel, E. Evaluation of dimensional changes in complete dentures processed by injection-pressing and the pack-and-press technique. J. Prosthet. Dent. 1983, 50, 757–761. [Google Scholar] [CrossRef] [PubMed]
- Keenan, P.L.; Radford, D.R.; Clark, R.K. Dimensional change in complete dentures fabricated by injection molding and mi-crowave processing. J. Prosthet. Dent. 2003, 89, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Huggett, R.; Zissis, A.; Harrison, A.; Dennis, A. Dimensional accuracy and stability of acrylic resin denture bases. J. Prosthet. Dent. 1992, 68, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Consani, R.L.X.; Domitti, S.S.; Mesquita, M.F.; Consani, S. Effect of packing types on the dimensional accuracy of denture base resin cured by the conventional cycle in relation to post-pressing times. Braz. Dent. J. 2004, 15, 63–67. [Google Scholar] [CrossRef]
- Memon, M.S.; Yunus, N.; Razak, A.A.A.; Memon, M.; Yunus, N.; Razak, A. Some mechanical properties of a highly cross-linked, microwave-polymerized, injection-molded denture base polymer. Int. J. Prosthodont. 2001, 14, 214–218. [Google Scholar]
- Strohaver, R.A. Comparison of changes in vertical dimension between compression and injection molded complete dentures. J. Prosthet. Dent. 1989, 62, 716–718. [Google Scholar] [CrossRef]
- Polat, T.N.; Karacaer, Ö.; Tezvergil, A.; Lassila, L.V.J.; Vallittu, P.K. Water Sorption, Solubility and Dimensional Changes of Denture Base Polymers Reinforced with Short Glass Fibers. J. Biomater. Appl. 2003, 17, 321–335. [Google Scholar] [CrossRef]
- Young, B.C. A Comparison of Polymeric Denture Base Materials; University of Glasgow: Glasgow, UK, 2010. [Google Scholar]
- Donovan, T.E.; Cho, G.C. Esthetic considerations with removable partial dentures. J. Calif. Dent. Assoc. 2003, 31, 551–557. [Google Scholar] [CrossRef]
- Ono, T.; Kita, S.; Nokubi, T. Dimensional accuracy of acrylic resin maxillary denture base polymerized by a new injection pressing method. Dent. Mater. J. 2004, 23, 348–352. [Google Scholar] [CrossRef] [Green Version]
- Rejab, L.T. The Effect of the Thermopress Curing Technique on the Water Sorption and Solubility of the Cold and Heat–Cured Acrylic Resins. Al-Rafidain Dent. J. 2008, 8, 11–17. [Google Scholar] [CrossRef] [Green Version]
- Parvizi, A.; Lindquist, T.; Schneider, R.; Williamson, D.; Boyer, D.; Dawson, D.V. Comparison of the dimensional accuracy of injection-molded denture base materials to that of conventional pressure-pack acrylic resin. J. Prosthodont. Implant. Esthet. Reconstr. Dent. 2004, 13, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Wataha, J.C.; Messer, R.L. Casting alloys. Dent. Clin. 2004, 48, 499–512. [Google Scholar] [CrossRef] [PubMed]
- Gad, M.M.; Fouda, S.M.; Al-Harbi, F.A.; Näpänkangas, R.; Raustia, A. PMMA denture base material enhancement: A review of fiber, filler, and nanofiller addition. Int. J. Nanomed. 2017, 12, 3801. [Google Scholar] [CrossRef] [Green Version]
- Garcia, A.A.M.N.; Sugio, C.Y.C.; de Azevedo-Silva, L.J.; Gomes, A.C.G.; Batista, A.U.D.; Porto, V.C.; Soares, S.; Neppelenbroek, K.H. Nanoparticle-modified PMMA to prevent denture stomatitis: A systematic review. Arch. Microbiol. 2021, 204, 75. [Google Scholar] [CrossRef]
- Fouda, S.M.; Gad, M.M.; Ellakany, P.; Al Ghamdi, M.A.; Khan, S.Q.; Akhtar, S.; Ali, M.S.; Al-Harbi, F.A. Flexural Properties, Impact Strength, and Hardness of Nanodiamond-Modified PMMA Denture Base Resin. Int. J. Biomater. 2022, 2022, 6583084. [Google Scholar] [CrossRef]
- An, J.; Ding, N.; Zhang, Z. Mechanical and antibacterial properties of polymethyl methacrylate modified with zinc dimethacrylate. J. Prosthet. Dent. 2022, 128, 100.e1–100.e8. [Google Scholar] [CrossRef]
- Correa, S.; Matamala, L.; González, J.P.; de la Fuente, M.; Miranda, H.; Olivares, B.; Maureira, M.; Agüero, A.; Gómez, L.; Lee, X.; et al. Development of novel antimicrobial acrylic denture modified with copper nanoparticles. J. Prosthodont. Res. 2023, JPR_D_22_00227. [Google Scholar] [CrossRef]
- Tomar, P.; Gope, P. Impact Strength Enhancement of PMMA base Denture Material by Fibre Addition. Int. J. Mater. Manuf. Sustain. Technol. 2023, 2, 49–57. [Google Scholar] [CrossRef]
- Elmwafy, D.; Abdelghany, A. Evaluation of flexural strength, microhardness and color stability of polyamide and heat cured acrylic resins modified with titania nanorods. Egypt. Dent. J. 2022, 68, 1665–1673. [Google Scholar] [CrossRef]
- Kowalski, R.; Kozak, M.; Sobolewska, E. Contemporary hybrid acrylic materials and modern thermoplastics in the manufacture of dental prostheses. Pomeranian J. Life Sci. 2023, 69, 39–45. [Google Scholar]
- Nabhan, A.; Taha, M.; Ghazaly, N.M. Filler loading effect of Al2O3/TiO2 nanoparticles on physical and mechanical characteristics of dental base composite (PMMA). Polym. Test. 2023, 117, 107848. [Google Scholar] [CrossRef]
- Díez-Pascual, A.M. PMMA-Based Nanocomposites for Odontology Applications: A State-of-the-Art. Int. J. Mol. Sci. 2022, 23, 10288. [Google Scholar] [CrossRef]
- Safi, I.N. Evaluation the effect of nano-fillers (TiO2, Al2O3, SiO2) addition on glass transition temperature, E-Moudulus and coefficient of thermal expansion of acrylic denture base material. J. Baghdad Coll. Dent. 2014, 325, 1–10. [Google Scholar] [CrossRef]
- Abdulkareem, M.M.; Hatim, N.A. Evaluation the biological effect of adding aluminum oxide, silver nanoparticles into micro-wave treated PMMA powder. Int. J. Enhanc. Res. Sci. Technol. Eng. 2015, 4, 172–178. [Google Scholar]
- Alla, R.; Raghavendra, K.; Vyas, R.; Konakanchi, A. Conventional and contemporary polymers for the fabrication of denture prosthesis: Part I–overview, composition and properties. Int. J. Appl. Dent. Sci. 2015, 1, 82–89. [Google Scholar]
- Engelmeier, R.L. The history and development of posterior denture teeth—Introduction, part I. J. Prosthodont. 2003, 12, 219–226. [Google Scholar] [CrossRef]
- Bathala, L.; Majeti, V.; Rachuri, N.; Singh, N.; Gedela, S. The Role of Polyether Ether Ketone (Peek) in Dentistry—A Review. J. Med. Life 2019, 12, 5–9. [Google Scholar] [CrossRef]
- Muhsin, S.A.; Hatton, P.V.; Johnson, A.; Sereno, N.; Wood, D.J. Determination of Polyetheretherketone (PEEK) mechanical properties as a denture material. Saudi Dent. J. 2019, 31, 382–391. [Google Scholar] [CrossRef]
- Silva, J.W.J.; Sousa, L.L.; Nakazato, R.Z.; Codaro, E.N.; de Felipe, H. Electrochemical and Microstructural Study of Ni-Cr-Mo Alloys Used in Dental Prostheses. Mater. Sci. Appl. 2011, 2, 42–48. [Google Scholar] [CrossRef]
- Wataha, J.C. Biocompatibility of dental casting alloys: A review. J. Prosthet. Dent. 2000, 83, 223–234. [Google Scholar] [CrossRef] [PubMed]
- Wataha, J.C.; O’Dell, N.L.; Singh, B.B.; Ghazi, M.; Whitford, G.M.; Lockwood, P.E. Relating nickel-induced tissue inflammation to nickel release in vivo. J. Biomed. Mater. Res. 2001, 58, 537–544. [Google Scholar] [CrossRef]
- Rokaya, D.; Bohara, S.; Srimaneepong, V.; Kongkiatkamon, S.; Khurshid, Z.; Heboyan, A.; Zafar, M.S.; Sapkota, J. Metallic bio-Materials for Medical and Dental Prosthetic Applications, Functional Biomaterials: Drug Delivery and Biomedical Applications; Springer: Berlin/Heidelberg, Germany, 2022; pp. 503–522. [Google Scholar]
- Özen, J.; Ural, A.U.; Dalkiz, M.; Beydemir, B. Influence of dental alloys and an all-ceramic material on cell viability and interleu-kin-1beta release in a three-dimensional cell culture model. Turk. J. Med. Sci. 2005, 35, 203–208. [Google Scholar]
- Alqutaibi, A.Y.; Alharbi, A.F.; Alharbi, A.M.; Karbouji, G.A.; Dagharire, E.Y.; Aboalrejal, A. Pretreatment expectations and posttreatment satisfaction with different prosthodontic treatments in a Saudi population. Saudi J. Oral Sci. 2022, 9, 63. [Google Scholar]
- Alqutaibi, A.Y. A within-subject comparison of the conventional clasp-retained with attachment-retained removable partial dentures. J. Taibah Univ. Med. Sci. 2020, 15, 305–311. [Google Scholar] [CrossRef]
- Wulfes, H. Precision Milling and Partial Denture Constructions; Academia-Dental: Bremen, Germany, 2004. [Google Scholar]
- Craig, O.B. Dental Materials: Properties and Manipulation; Mosby Year Book: Maryland Heights, MI, USA, 1992; pp. 45–56. [Google Scholar]
- Reclaru, L.; Lüthy, H.; Eschler, P.-Y.; Blatter, A.; Susz, C. Corrosion behaviour of cobalt–chromium dental alloys doped with precious metals. Biomaterials 2005, 26, 4358–4365. [Google Scholar] [CrossRef]
- Wataha, J.C. Alloys for prosthodontic restorations. J. Prosthet. Dent. 2002, 87, 351–363. [Google Scholar] [CrossRef]
- Iacoban, S.; Bolat, G.; Munteanu, C.; Cailean, D.; Trinca, L.; Mareci, D. A comparative study on the corrosion behaviour of CoCr and NiCr dental alloys in saline medium. Rev. Roum. Chim. 2015, 60, 949–955. [Google Scholar]
- Bilgin, M.S.; Baytaroğlu, E.N.; Erdem, A.; Dilber, E. A review of computer-aided design/computer-aided manufacture techniques for removable denture fabrication. Eur. J. Dent. 2016, 10, 286–291. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, N.; Abbasi, M.S.; Haider, S.; Ahmed, N.; Habib, S.R.; Altamash, S.; Zafar, M.S.; Alam, M.K. Fit Accuracy of Removable Partial Denture Frameworks Fabricated with CAD/CAM, Rapid Prototyping, and Conventional Techniques: A Systematic Review. BioMed Res. Int. 2021, 2021, 3194433. [Google Scholar] [CrossRef]
- Steinmassl, P.-A.; Klaunzer, F.; Steinmassl, O.; Dumfahrt, H.; Grunert, I. Evaluation of Currently Available CAD/CAM Denture Systems. Int. J. Prosthodont. 2017, 30, 116–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Limírio, J.P.J.D.O.; Gomes, J.M.D.L.; Rezende, M.C.R.A.; Lemos, C.A.A.; Rosa, C.D.D.R.D.; Pellizzer, E.P. Mechanical properties of polymethyl methacrylate as a denture base: Conventional versus CAD-CAM resin—A systematic review and meta-analysis of in vitro studies. J. Prosthet. Dent. 2021, 128, 1221–1229. [Google Scholar] [CrossRef] [PubMed]
- Inokoshi, M.; Kanazawa, M.; Minakuchi, S. Evaluation of a complete denture trial method applying rapid prototyping. Dent. Mater. J. 2012, 31, 40–46. [Google Scholar] [CrossRef] [Green Version]
- Bezzon, O.L.; Pedrazzi, H.; Zaniquelli, O.; da Silva, T.B.C. Effect of casting technique on surface roughness and consequent mass loss after polishing of NiCr and CoCr base metal alloys: A comparative study with titanium. J. Prosthet. Dent. 2004, 92, 274–277. [Google Scholar] [CrossRef]
- Dobrzański, L. Influence of Cr and Co on hardness and corrosion resistance CoCrMo alloys used on dentures. J. Achiev. Mater. Manuf. Eng. 2011, 49, 193–199. [Google Scholar]
- Eliaz, N. Corrosion of Metallic Biomaterials: A Review. Materials 2019, 12, 407. [Google Scholar] [CrossRef] [Green Version]
- Joias, R.M.; Tango, R.N.; de Araujo, J.E.J.; de Araujo, M.A.J.; Saavedra, G.D.S.F.A.; de Arruda Paes-Junior, T.J.; Kimpara, E.T. Shear bond strength of a ceramic to Co-Cr alloys. J. Prosthet. Dent. 2008, 99, 54–59. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alqutaibi, A.Y.; Baik, A.; Almuzaini, S.A.; Farghal, A.E.; Alnazzawi, A.A.; Borzangy, S.; Aboalrejal, A.N.; AbdElaziz, M.H.; Mahmoud, I.I.; Zafar, M.S. Polymeric Denture Base Materials: A Review. Polymers 2023, 15, 3258. https://0-doi-org.brum.beds.ac.uk/10.3390/polym15153258
Alqutaibi AY, Baik A, Almuzaini SA, Farghal AE, Alnazzawi AA, Borzangy S, Aboalrejal AN, AbdElaziz MH, Mahmoud II, Zafar MS. Polymeric Denture Base Materials: A Review. Polymers. 2023; 15(15):3258. https://0-doi-org.brum.beds.ac.uk/10.3390/polym15153258
Chicago/Turabian StyleAlqutaibi, Ahmed Yaseen, Abdulmajeed Baik, Sarah A. Almuzaini, Ahmed E. Farghal, Ahmad Abdulkareem Alnazzawi, Sary Borzangy, Afaf Noman Aboalrejal, Mohammed Hosny AbdElaziz, Ihab Ismail Mahmoud, and Muhammad Sohail Zafar. 2023. "Polymeric Denture Base Materials: A Review" Polymers 15, no. 15: 3258. https://0-doi-org.brum.beds.ac.uk/10.3390/polym15153258