
Gait Performance of Friction-Based Prosthetic Knee Joint Swing-Phase Controllers in Under-Resourced Settings

 , ,
, ,
Abstract
:1. Introduction
2. Methods
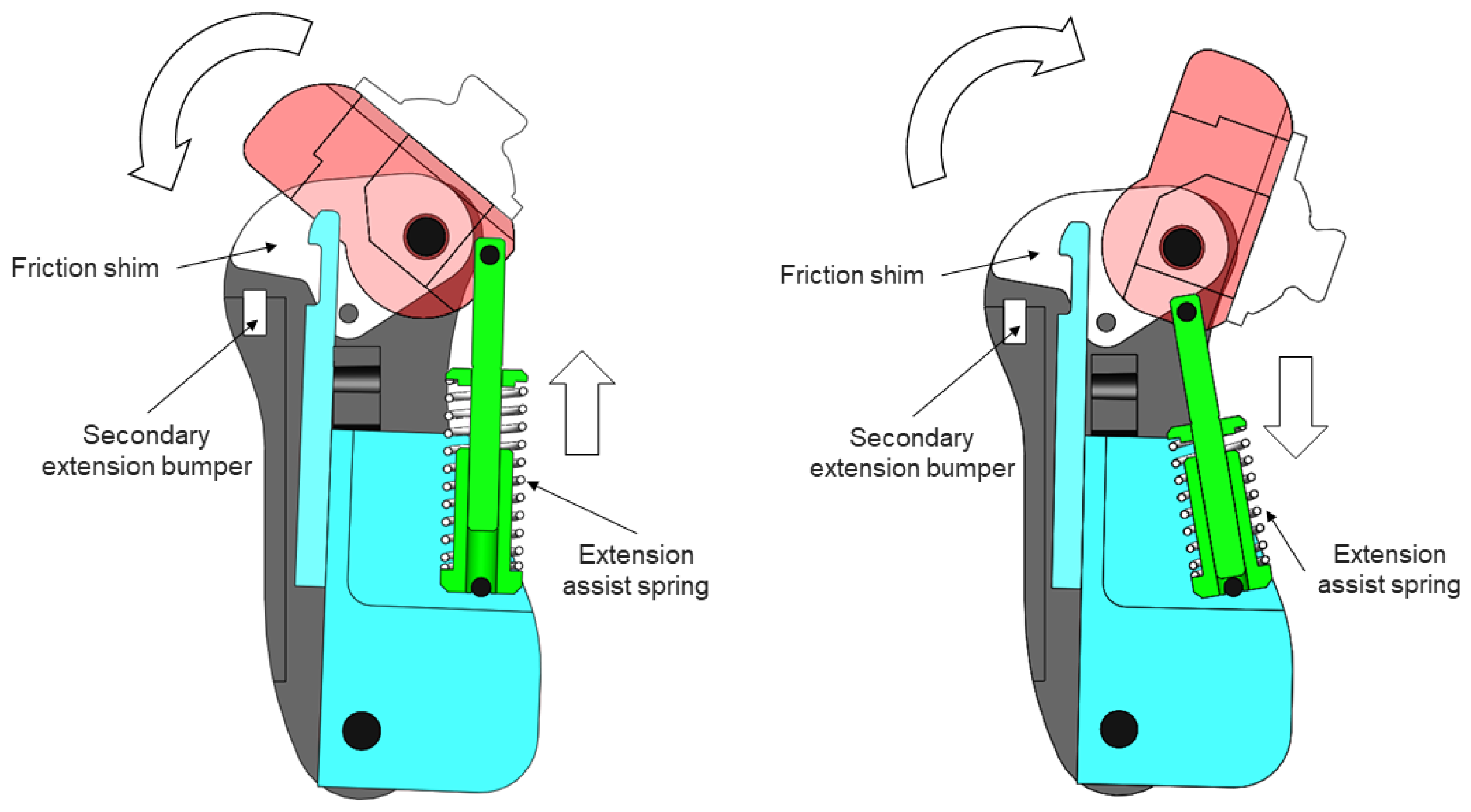
2.1. Prosthetic Knee Joints
2.2. Experimental Procedures
2.3. Recruitment
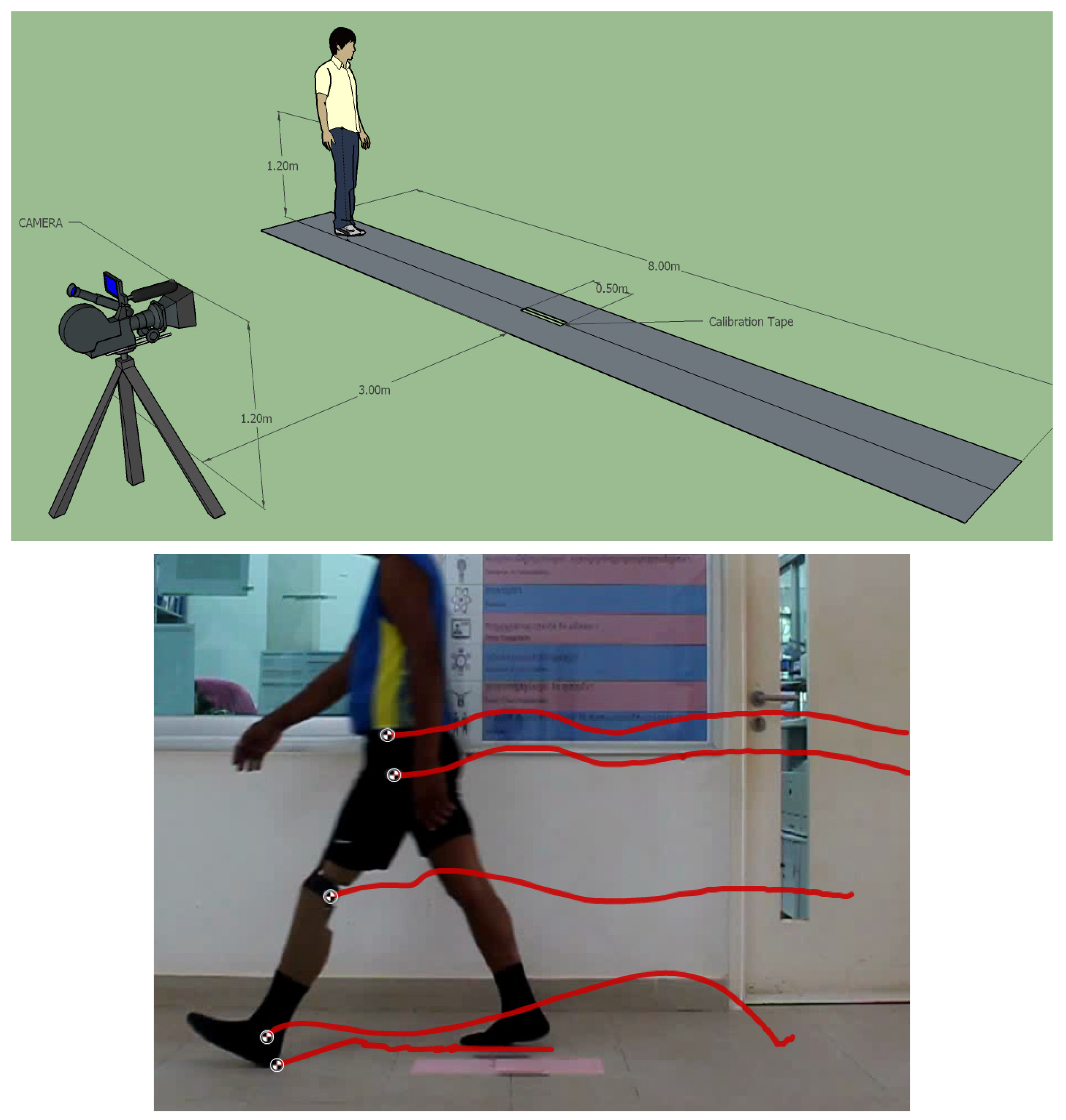
2.4. Data Collection
2.5. Gait Parameters
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eberly, V.J.; Mulroy, S.J.; Gronley, J.K.; Perry, J.; Yule, W.J.; Burnfield, J.M. Impact of a stance phase microprocessorcontrolled knee prosthesis on level walking in lower functioning individuals with a transfemoral amputation. Prosthet. Orthot. Int. 2014, 38, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Uchytil, J.; Jandacka, D.; Zahradnik, D.; Farana, R.; Janura, M. Temporal-spatial parameters of gait in transfemoral amputees: Comparison of bionic and mechanically passive knee joints. Prosthet. Orthot. Int. 2014, 38, 199–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genin, J.J.; Bastien, G.J.; Franck, B.; Detrembleur, C.; Willems, P.A. Effect of speed on the energy cost of walking in unilateral traumatic lower limb amputees. Eur. J. Appl. Physiol. 2008, 103, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Jarvis, H.L.; Bennett, A.N.; Twiste, M.; Phillip, R.D.; Etherington, J.; Baker, R. Temporal spatial and metabolic measures of walking in highly functional individuals with lower limb amputations. Arch. Phys. Med. Rehabil. 2017, 98, 1389–1399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gailey, R. Review of secondary physical conditions associated with lower-limb amputation and long-term prosthesis use. J. Rehabil. Res. Dev. 2008, 45, 15–30. [Google Scholar] [CrossRef] [PubMed]
- Ephraim, P.L.; Wegener, S.T.; MacKenzie, E.J.; Dillingham, T.R.; Pezzin, L.E. Phantom pain, residual limb pain, and back pain in amputees: Results of a national survey. Arch. Phys. Med. Rehabil. 2005, 86, 1910–1919. [Google Scholar] [CrossRef] [PubMed]
- Van Velzen, J.M.; Van Bennekom, C.A.M.M.; Polomski, W.; Slootman, J.R.; Van Der Woude, L.H.V.V.; Houdijk, H. Physical capacity and walking ability after lower limb amputation: A systematic review. Clin. Rehabil. 2006, 20, 999–1016. [Google Scholar] [CrossRef] [Green Version]
- Amtmann, D.; Morgan, S.J.; Kim, J.; Hafner, B.J. Health-Related Profiles of People with Lower Limb Loss. Arch. Phys. Med. Rehabil. 2015, 96, 1474–1483. [Google Scholar] [CrossRef] [Green Version]
- Jensen, J.S.; Raab, W. Clinical field testing of trans-femoral prosthetic technologies: Resin-wood and ICRC-polypropylene. Prosthet. Orthot. Int. 2004, 28, 141–151. [Google Scholar] [CrossRef] [Green Version]
- Furse, A.; Cleghorn, W.; Andrysek, J. Development of a low-technology prosthetic swing-phase mechanism. J. Med. Biol. Eng. 2011, 31, 145–150. [Google Scholar] [CrossRef]
- Andrysek, J. Lower-limb prosthetic technologies in the developing world: A review of literature from 1994–2010. Prosthet. Orthot. Int. 2010, 34, 378–398. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.S.; Mansour, J.M. Swing phase simulation and design of above knee prostheses. J. Biomech. Eng. 1986, 108, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Furse, A.; Cleghorn, W.; Andrysek, J. Improving the gait performance of nonfluid-based swing-phase control mechanisms in transfemoral prostheses. IEEE Trans. Biomed. Eng. 2011, 58, 2352–2359. [Google Scholar] [CrossRef] [PubMed]
- Variable Cadence Controller Demo. Available online: https://www.youtube.com/watch?v=bgGCPs5Trj8 (accessed on 10 August 2021).
- Andrysek, J.; Klejman, S.; Torres-Moreno, R.; Heim, W.; Steinnagel, B.; Glasford, S. Mobility function of a prosthetic knee joint with an automatic stance phase lock. Prosthet. Orthot. Int. 2011, 35, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Andrysek, J.; Wright, F.V.; Rotter, K.; Garcia, D.; Valdebenito, R.; Mitchell, C.A.; Rozbaczylo, C.; Cubillos, R. Long-term clinical evaluation of the automatic stance-phase lock-controlled prosthetic knee joint in young adults with unilateral above-knee amputation. Disabil. Rehabil. Assist. Technol. 2017, 12, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Andrysek, J.; García, D.; Rozbaczylo, C.; Alvarez-Mitchell, C.; Valdebenito, R.; Rotter, K.; Wright, F.V. Biomechanical responses of young adults with unilateral transfemoral amputation using two types of mechanical stance control prosthetic knee joints. Prosthet. Orthot. Int. 2020, 44, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Andrysek, J.; Michelini, A.; Eshraghi, A.; Kheng, S.; Heang, T.; Thor, P. Functional outcomes and user preferences of individuals with transfemoral amputations using two types of knee joints in under-resourced settings. Prosthet. Orthot. Int. 2021, 45, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Burke, B.; Andrysek, J. Variable Friction-Based Swing-Phase Controller with Artificial Joint. U.S. Patent No. 10,702,401, 8 April 2020. [Google Scholar]
- Fiedler, G.; Zhang, X. Quantifying accommodation to prosthesis interventions in persons with lower limb loss. Gait Posture 2016, 50, 14–16. [Google Scholar] [CrossRef]
- Fatone, S.; Stine, R. Capturing quality clinical videos for two-dimensional motion analysis. J. Prosthet. Orthot. 2015, 27, 27–32. [Google Scholar] [CrossRef]
- Michelini, A.; Eshraghi, A.; Andrysek, J. Two-dimensional video gait analysis: A systematic review of reliability, validity, and best practice considerations. Prosthet. Orthot. Int. 2020, 44, 245–262. [Google Scholar] [CrossRef] [PubMed]
- Robinson, R.O.; Herzog, W.; Nigg, B.M. Use of force platform variables to quantify the effects of chiropractic manipulation on gait symmetry. J. Manip. Physiol. Ther. 1987, 10, 172–176. [Google Scholar]
- Sagawa, Y.; Turcot, K.; Armand, S.; Thevenon, A.; Vuillerme, N.; Watelain, E. Biomechanics and physiological parameters during gait in lower-limb amputees: A systematic review. Gait Posture 2011, 33, 511–526. [Google Scholar] [CrossRef] [PubMed]
- Ugbolue, U.C.; Papi, E.; Kaliarntas, K.T.; Kerr, A.; Earl, L.; Pomeroy, V.M.; Rowe, P.J. The evaluation of an inexpensive, 2D, video based gait assessment system for clinical use. Gait Posture 2013, 38, 483–489. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant Descriptors | Mean ± SD, [Range] |
|---|---|
| Age (years) | 40.4 ± 14.0, (20–61) |
| Height (m) | 1.68 ± 0.07, (157–181) |
| Weight (kg) | 63.5 ± 12.4, (42–96) |
| Time since amputation (years) | 14.0 ± 9.8, (0.4–33) |
| Primary Parameters | ICRC (CF) | ATK (VCC) | % Change | p-Value |
|---|---|---|---|---|
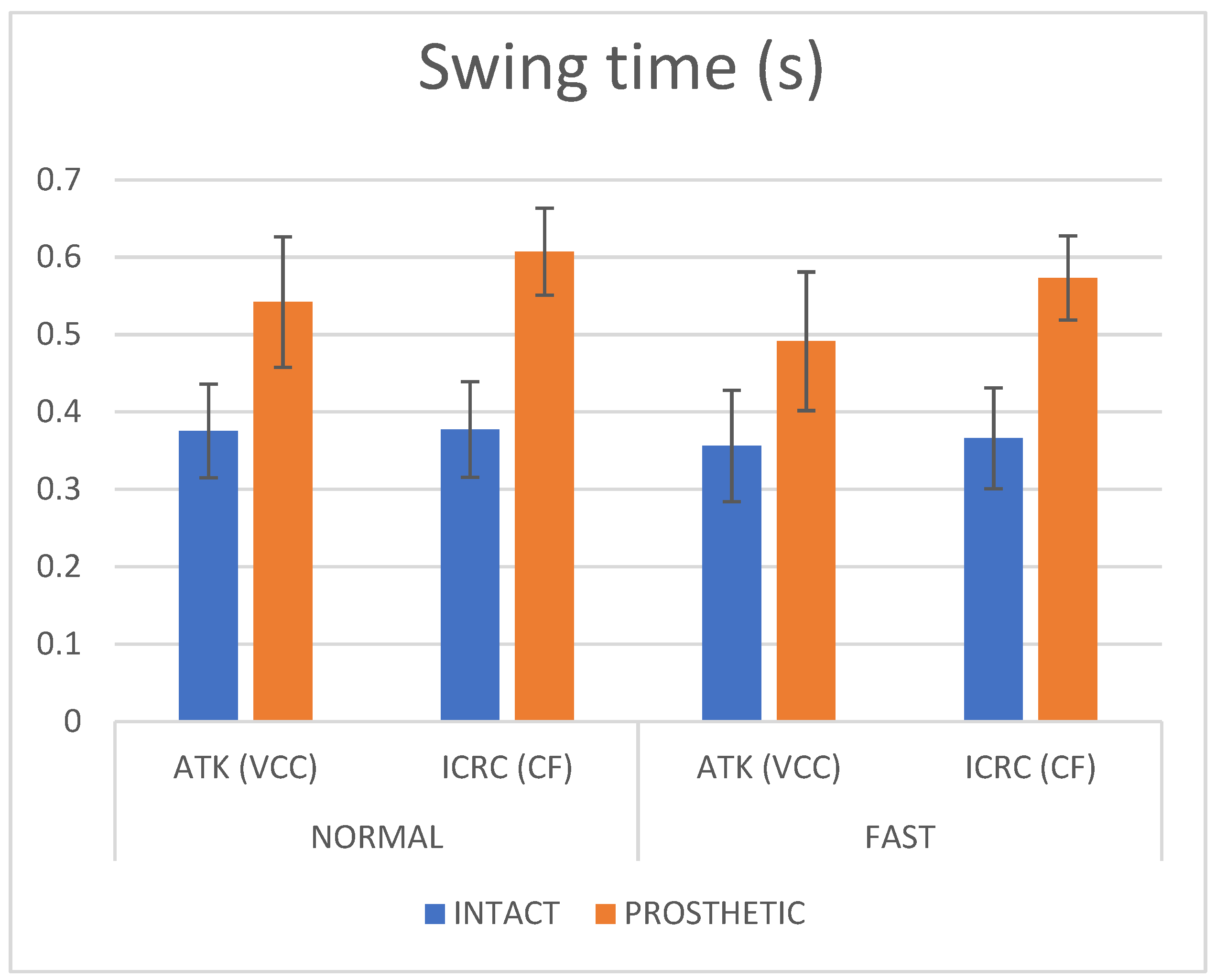
| Prosth Swing Time (s) | 0.607 ± 0.010, (0.587, 0.627) | 0.543 ± 0.084, (0.512, 0.571) | 11.1% | 0.000 |
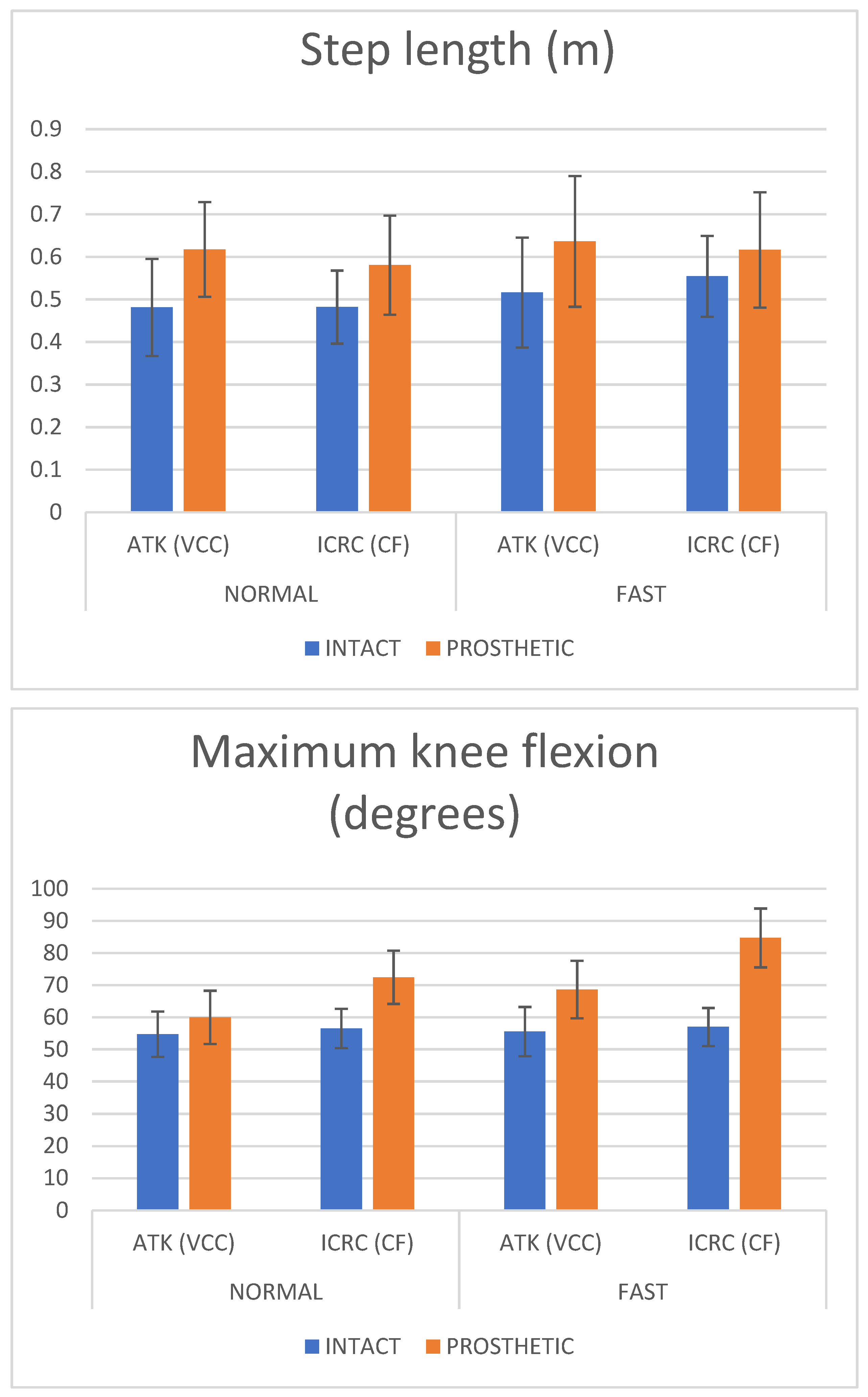
| Prosth Step length (m) | 0.581 ± 0.116, (0.540, 0.621) | 0.617 ± 0.111, (0.579, 0.656) | 6.0% | 0.094 |
| Prosth Knee flex (deg) | 72.4 ± 8.3, (68.2, 76.7) | 59.9 ± 8.3, (55.7, 64.2) | 18.9% | 0.000 |
| Swing time SI | 0.48 ± 0.14, (0.43, 0.52) | 0.36 ± 0.11, (0.32, 0.40) | 28.6% | 0.000 |
| Step length SI | 0.18 ± 0.22, (0.10, 0.26) | 0.26 ± 0.26, (0.17, 0.36) | 36.4% | 0.261 |
| Knee flex SI | 0.25 ± 0.14, (0.18, 0.32) | 0.09 ± 0.16, (0.01, 0.17) | 94.1% | 0.002 |
| Secondary Parameters | ||||
| Velocity (m/s) | 0.86 ± 0.09, (0.83, 0.89) | 0.99 ± 0.22, (0.91, 1.07) | 14.1% | 0.002 |
| Stride Length (m) | 1.13 ± 0.10, (1.09, 1.16) | 1.18 ± 0.13, (1.14, 1.23) | 4.3% | 0.066 |
| Cadence (steps/min) | 92 ± 7, (90, 95) | 101 ± 21, (94, 109) | 9.3% | 0.022 |
| Double Support (s) | 0.324 ± 0.073, (0.298, 0.349) | 0.302 ± 0.091, (0.270, 0.334) | 7.0% | 0.281 |
| Primary Parameters | ICRC (CF) | ATK (VCC) | % Change | p-Value |
|---|---|---|---|---|
| Prosth Swing Time (s) | 0.573 ± 0.054, (0.555, 0.592) | 0.491 ± 0.090, (0.460, 0.522) | 15.4% | 0.000 |
| Prosth. Step length (m) | 0.616 ± 0.135, (0.570, 0.663) | 0.636 ± 0.154, (0.583, 0.690) | 3.2% | 0.283 |
| Prosth Knee flex (deg) | 84.7 ± 9.1, (80.1, 89.2) | 68.6 ± 9.0, (64.0, 73.2) | 21.0% | 0.000 |
| Swing time SI | 0.45 ± 0.14, (0.40, 0.50) | 0.32 ± 0.15, (0.27, 0.37) | 33.8% | 0.000 |
| Step length SI | 0.09 ± 0.23, (0.01, 0.17) | 0.20 ± 0.27, (0.11, 0.30) | 75.9% | 0.022 |
| Knee flex SI | 0.39 ± 0.11, (0.26, 0.33) | 0.21 ± 0.186, (0.12, 0.30) | 60.0% | 0.001 |
| Secondary Parameters | ||||
| Velocity (m/s) | 1.07 ± 0.12, (1.03, 1.11) | 1.25 ± 0.32, (1.14, 1.36) | 15.5% | 0.002 |
| Stride Length (m) | 1.31 ± 0.14, (1.26, 1.35) | 1.36 ± 0.14, (1.31, 1.41) | 3.7% | 0.103 |
| Cadence (Steps/min) | 99.6 ± 6.4, (97.4, 101) | 112 ± 23.2, (104, 120) | 11.7% | 0.003 |
| Double Support (s) | 0.271 ± 0.077 (0.244, 0.297) | 0.253 ± 0.088 (0.222, 0.284) | 6.9% | 0.370 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrysek, J.; Michelini, A.; Eshraghi, A.; Kheng, S.; Heang, T.; Thor, P. Gait Performance of Friction-Based Prosthetic Knee Joint Swing-Phase Controllers in Under-Resourced Settings. Prosthesis 2022, 4, 125-135. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis4010013
Andrysek J, Michelini A, Eshraghi A, Kheng S, Heang T, Thor P. Gait Performance of Friction-Based Prosthetic Knee Joint Swing-Phase Controllers in Under-Resourced Settings. Prosthesis. 2022; 4(1):125-135. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis4010013
Chicago/Turabian StyleAndrysek, Jan, Alexandria Michelini, Arezoo Eshraghi, Sisary Kheng, Thearith Heang, and Phearsa Thor. 2022. "Gait Performance of Friction-Based Prosthetic Knee Joint Swing-Phase Controllers in Under-Resourced Settings" Prosthesis 4, no. 1: 125-135. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis4010013