
Follower-Centric Influences on Sexual Decision Making in a Pentecostal Church Faith Community

Abstract
:1. Introduction
2. Pentecostal Churches in Botswana
3. Interpretive Health Decisions
4. Goals of the Study
5. Method
5.1. Participants and Setting
5.2. Procedure and Data Collection
5.2.1. Brainstorming Workshop
“Think about an HIV/AIDS prevention message to prevent [you] from contracting HIV. As you think about these issues, please generate as many statements (short phrases or sentences) as you can and list them below.”
5.2.2. Sorting of the Statements
5.2.3. Rating of Statements
6. Data Analysis
7. Results
7.1. Religion Influences
7.2. Secular Influences
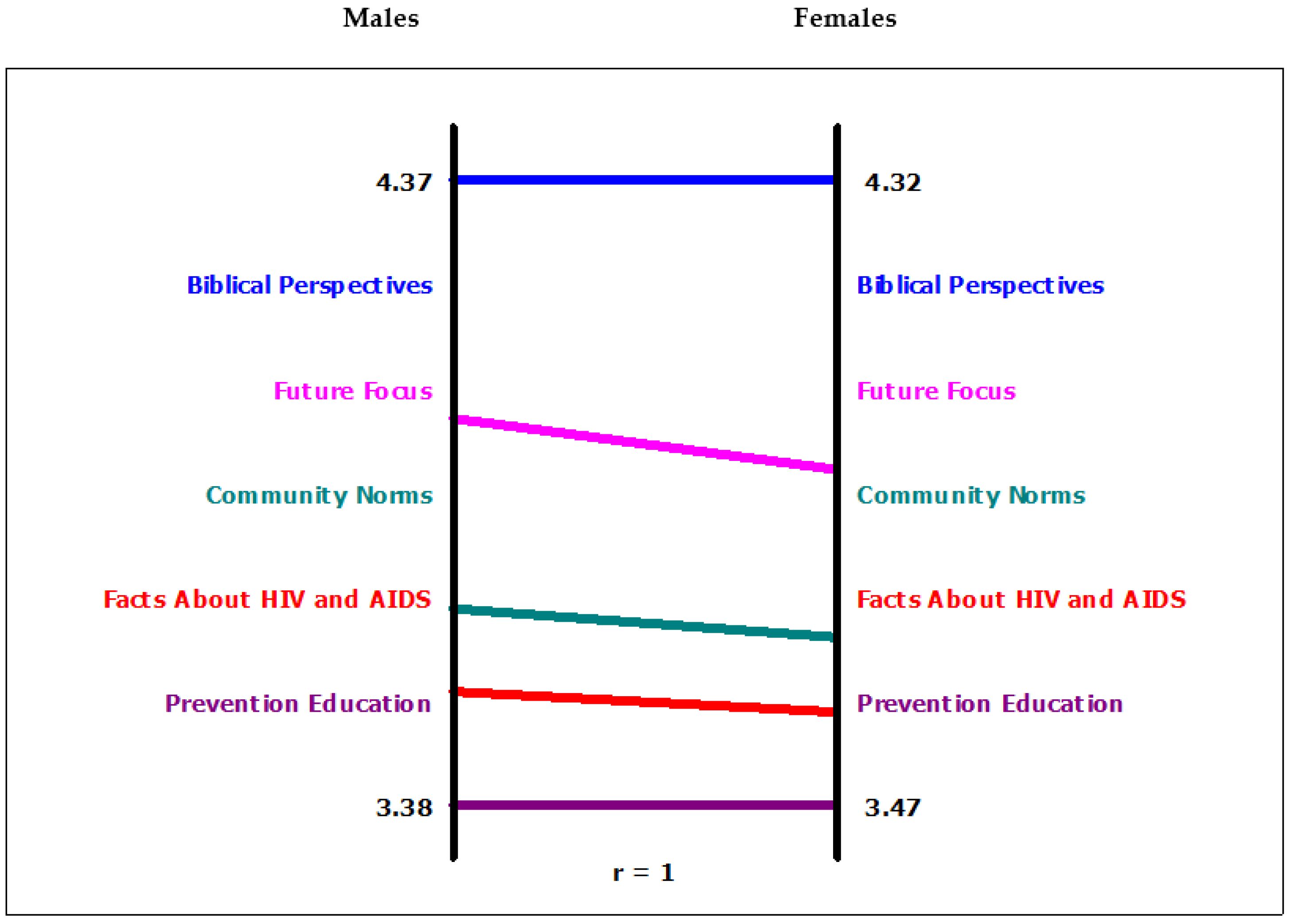
7.3. Sexual Decision Framing by Gender
8. Discussion
9. Conclusions
Acknowledgments
Conflicts of Interest
References
- Elva M. Arredondo, John P. Elder, Guadalupe X. Ayala, and Nadia R. Campbell. “Is Church attendance associated with Latinas’ Health practices and self-reported health? ” American Journal of Health Behavior 29 (2005): 502–11. [Google Scholar] [CrossRef] [PubMed]
- Laurie J. Bauman, and Rebecca Berman. “Adolescent relationships and condom use: Trust, love and commitment.” AIDS and Behavior 9 (2005): 211–22. [Google Scholar] [CrossRef] [PubMed]
- Brenda R. Jackson, and Cindy S. Bergeman. “How does religiosity enhance well-being? The role of perceived control.” Psychology of Religion and Spirituality 3 (2011): 149–61. [Google Scholar] [CrossRef] [PubMed]
- Monica M. McKenzie, Naomi M. Modeste, Helen Hopp Marshak, and Colwick Wilson. “Religious involvement and health-related behaviors among Black Seventh-Day Adventists in Canada.” Health Promotion Practice 16 (2014): 264–70. [Google Scholar] [CrossRef] [PubMed]
- Louis Brenner. Controlling Knowledge: Religion, Power and Schooling in a West African Muslim Society. Bloomington: Indiana University Press, 2001. [Google Scholar]
- Jesse Graham, and Jonathan Haidt. “Beyond beliefs: Religions bind individuals into moral communities.” Personality and Social Psychology Review 14 (2010): 140–50. [Google Scholar] [CrossRef] [PubMed]
- Stefan Huber, and Odilo W. Huber. “The Centrality of Religiosity Scale (CRS).” Religions 3 (2012): 710–24. [Google Scholar] [CrossRef] [Green Version]
- Ara Norenzayan, and Azim F. Shariff. “The origin and evolution of religious prosociality.” Science 332 (2008): 58–62. [Google Scholar] [CrossRef] [PubMed]
- Lacy G. McNamee. “Faith based organizational communication and its implications for member identity.” Journal of Applied Communication Research 39 (2011): 422–40. [Google Scholar] [CrossRef]
- Vassilis Saroglou. “Religiosity, bonding, behaving and belonging: The big four religious dimensions and cultural variation.” Journal of Cross-Cultural Psychology 42 (2011): 1320–40. [Google Scholar] [CrossRef]
- Christine Kim, and Robert Rector. “Evidence on the Effectiveness of Abstinence Education: An Update.” 2010. Available online: www.heritage.org/Research/Abstinence/bg2372.cfm (accessed on 4 November 2012).
- Elias Mpofu, Tinashe Moira Dune, Denise Dion Hallfors, John Mapfumo, Magen Mutepfa, and James January. “Apostolic faith organization contexts for health and wellbeing in women and children.” Ethnicity and Health 13 (2011): 1–16. [Google Scholar] [CrossRef] [PubMed]
- Elias Mpofu, Fidelis Nkomazana, Jabulani A. Muchado, Lovemore Togarasei, and Jeffrey B. Bingenheimer. “Faith and HIV prevention: The Conceptual framing of HIV prevention among Pentecostal Batswana Teenagers.” BMC Public Health 14 (2014): 225. [Google Scholar] [CrossRef] [PubMed]
- WHO/UNAIDS/UNICEF. Global AIDS Epidemic. Geneva: World Health Organization, 2011. [Google Scholar]
- Botswana Christian Council (BCC). Report: Adolescent Sexual Reproductive Health Survey. Gaborone: Botswana Christian Council, 2003. [Google Scholar]
- Musa W. Dube, ed. HIV/AIDS and the Curriculum: Methods of Integrating HIV/AIDS in Theological Programs. Geneva: World Council of Churches, 2003.
- Musa Dube. Africa Praying: A Handbook on HIV/AIDS Sensitive Sermon Guidelines and Liturgy. Geneva: World Council of Churches, 2003. [Google Scholar]
- Lovemore Togarasei, Sana K. Mmolai, and Fidelis Nkomazana. The Faith Sector and HIV/AIDS in Botswana: Responses and Challenges. Newcastle: Cambridge Scholars Publishing, 2011. [Google Scholar]
- Lovemore Togarasei. “The Pentecostal gospel of prosperity in African Contexts of poverty.” Exchange 40 (2011): 335–50. [Google Scholar] [CrossRef]
- John B. Jemmott III, Loretta S. Jemmott, and Goeffrey T. Fong. “Efficacy of a theory-based Abstinence-only intervention Over 24 Months.” Archives of Pediatrics and Adolescent Medicine 164 (2010): 152–59. [Google Scholar] [CrossRef] [PubMed]
- Jenn Anderson. “Vanity vs. Gluttony: Competing Christian discourses on personal health.” Journal of Applied Communication Research 39 (2011): 370–88. [Google Scholar] [CrossRef]
- Andrea D. Clements, and Anna V. Ermakova. “Surrender to God and stress: A possible link between religiosity and health.” Psychology of Religion and Spirituality 4 (2012): 93–107. [Google Scholar] [CrossRef]
- Christian Zwingmann, Constantin Klein, and Arndt Bussing. “Measuring religiosity/spirituality: Theoretical differentiations and categorization of instruments.” Religions 2 (2011): 345–57. [Google Scholar] [CrossRef]
- Elias Mpofu, Denise Dion Hallfors, Magen M. Mutepfa, and Tinashe M. Dune. “Sexual decision making as perceived by Zimbabwean orphan girl students.” Journal of Mixed Methods Research 8 (2014): 363–76. [Google Scholar] [CrossRef] [PubMed]
- Sue Aford, and Marilyn Keefe. “Abstinence only-until-marriage programs: Ineffective, unethical and poor public health.” 2007. Available online: www.advocatesyouth.org (accessed on 4 November 2012).
- Elias Mpofu, Magen Mhaka Mutepfa, and Denise Hallfors. “Mapping structural influences on sex and HIV education in church and secular schools in Zimbabwe.” Evaluation and the Health Professions 35 (2012): 346–59. [Google Scholar] [CrossRef] [PubMed]
- Beverly Haddad, ed. Religion and HIV and AIDS: Charting the Terrain. Pietermaritzburg: UKZN Press, 2011.
- Jenny Trinitapoli, and Alexander Weinreb. Religion and AIDS in Africa. Oxford and New York: Oxford University Press, 2012. [Google Scholar]
- Derek M. Griffith, Bettina Campbell, Julie Ober Allen, Kelvin J. Robinson, and Sarah Kretman Stewart. “YOUR blessed health: An HIV-prevention program bridging faith and public health communities.” Public Health Reports 125 (2010): 4–32. [Google Scholar] [PubMed]
- Concept Systems Incorporated. Concept Systems. Ithaca: Concept Systems Inc., 2012. [Google Scholar]
- Evan C. Carter, Michael E. McCullough, Jungmeen Kim-Spoon, Carolina Corrales, and Adam Blake. “Religious people discount the future less.” Evolution and Human Behavior 33 (2012): 224–31. [Google Scholar] [CrossRef]
- Christopher Ellison, and Daisy Fan. “Daily spiritual experiences and psychological well-being Among US Adults.” Social Indicators Research 8 (2008): 247–71. [Google Scholar] [CrossRef]
- Elias Mpofu, and Thomas Oakland. “Assessment of Value Change in Adults with Acquired Disabilities.” In Clinician’s Handbook of Adult Behavioral Assessment. Edited by Michel Hersen. New York: Elsevier Press, 2006, pp. 601–30. [Google Scholar]
- Steven J. Osterlind, Elias Mpofu, and Thomas Oakland. “Item response theory and computer adaptive testing.” In Rehabilitation and health assessment: Applying ICF guidelines. Edited by Elias Mpofu and Thomas Oakland. New York: Springer Publishing Company, 2010, pp. 95–119. [Google Scholar]
- Adriana Galvin. “Adolescent development of the reward system.” Frontiers in Human Neuroscience 4 (2010): 116–24. [Google Scholar] [CrossRef] [PubMed]
- Raymundo Baez-Mendoza, and Wolfram Schultz. “The role of the striatum in social behaviour.” Frontiers in Neuroscience 7 (2013): 1–14. [Google Scholar] [CrossRef] [PubMed]
- Ty A. Ridenour, Linda L. Caldwell, Douglas D. Coatsworth, and Melanie A. Gold. “Directionality between tolerance of deviance and deviant behaviour is age-moderated in chronically stressed youth.” Journal of Child Adolescnece Sunstance Abuse 2 (2011): 184–204. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Demographics | N (%) | Mean and Standard Deviation |
|---|---|---|
| Person variables | ||
| Gender | ||
| Female | 42 (62%) | |
| Male | 26 (38%) | |
| Tenure with church organization | ||
| Time with congregation (months) | 5.75 (3.42) | |
| Time with the Pentecostal Church (months) | 6.45 (4.09) | |
| Last sexual intercourse | ||
| Less than a day ago | 5 (7.4) | |
| Less than a day ago | 5 (7.4) | |
| Less than a week ago | (10.3) | |
| Less than a month ago | 12 (17.6) | |
| Several months ago | 44 (64.7) |
| Cluster 1: Biblical Perspectives (α = 0. 89) | ||
| Item # | Content | Importance (1–5) |
| 43 | Trust in God always. | 4.69 |
| 22 | Say no to sex before marriage. | 4.63 |
| 50 | Asking for partner from God and waiting for marriage | 4.56 |
| 15 | bstain from sex. | 4.54 |
| 38 | Protecting and valuing virginity. | 4.42 |
| 7 | Hold on to biblical faith and a good conscience. | 4.35 |
| 49 | Good moral character is important | 4.29 |
| 4 | Biblical perspective on HIV and AIDS. | 3.88 |
| 8 | Your spirit, soul and body should be blameless. | 3.60 |
| Count = 9; * Std. Dev.: 0.36; Average: | 4.33 | |
| Range | 3.60–4.60 | |
| Cluster 2: Future Focus (α = 0.92) | ||
| 31 | Importance of life targets and setting personal goals. | 4.39 |
| 34 | Being careful with your life style. | 4.37 |
| 16 | Resist negative peer pressure. | 4.28 |
| 47 | Aim for a career. | 4.18 |
| 19 | Taking responsibility for one’s future. | 4.12 |
| 27 | School first, sex after. | 4.08 |
| 44 | Choose friends wisely. | 3.93 |
| 32 | Self-pride or valuing one’s self. | 3.86 |
| 23 | Make informed decisions about personal relationships. | 3.79 |
| 25 | Managing new interpersonal relationships. | 3.54 |
| 48 | Books before boys or girls. | 3.47 |
| 40 | Learning use of leisure time. | 3.38 |
| Count = 12; Std. Dev.: 0.34; Average: | 3.94 | |
| Range | 3.38–4.39 | |
| Cluster 3: Community Norms (α = 0.87) | ||
| 10 | Healthy living. | 4.39 |
| 37 | Talk about HIV with peers, teachers and parents. | 4.26 |
| 33 | Listen to constructive advice. | 3.90 |
| 13 | Self help and community welfare for health. | 3.51 |
| 39 | Life consequences of unwanted pregnancies. | 3.42 |
| 36 | Share your sexual education needs with teacher. | 3.23 |
| 17 | The developmental stage of adolescence and puberty. | 3.00 |
| Count = 7; Std. Dev.: 0.52 Average | 3.67 | |
| Range | 3.51–4.36 | |
| Cluster 4: Facts About HIV and AIDS (α = 86) | ||
| 5 | Caring for the HIV and AIDS infected and affected. | 4.23 |
| 1 | Sexually transmitted infections. | 4.14 |
| 12 | Voluntary testing and counseling. | 4.01 |
| 3 | What are HIV and AIDS? | 3.79 |
| 9 | The impact of HIV and AIDS on community and national development. | 3.59 |
| 2 | Link between STD and HIV and AIDS. | 3.53 |
| 14 | Dealing with HIV and AIDS in the workplace. | 3.43 |
| 11 | Anti-retroviral therapy. | 3.28 |
| 18 | Living with the HIV virus. | 3.15 |
| 41 | Types of opportunistic infections with HIV and AIDS. | 3.12 |
| 28 | Substance use and HIV and AIDS. | 2.83 |
| 42 | Be open about your HIV status. | 2.72 |
| Count = 12; Std. Dev.: 0.49; Average: | 3.48 | |
| Range | 3.48–4.23 | |
| Cluster 5: Prevention Education (α = 81) | ||
| 21 | Avoid places with risk for bad abuse. | 4.23 |
| 24 | Risks from early involvement in love affairs while a minor. | 3.86 |
| 35 | Appropriate dressing and language. | 3.59 |
| 6 | Vulnerability of women and youth to HIV infection. | 3.54 |
| 20 | Family expectations for personal growth are important. | 3.39 |
| 30 | Risks from sex for money. | 3.18 |
| 26 | Proper use of contraceptives. | 3.13 |
| 45 | Cultural practices that promote the spread of HIV and AIDS. | 2.83 |
| 28 | Limits of condoms and contraceptives. | 2.25 |
| Count = 9; Std. Dev.: 0.58; Average: | 3.33 | |
| Range | 3.39–4.23 | |
© 2016 by the author; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mpofu, E. Follower-Centric Influences on Sexual Decision Making in a Pentecostal Church Faith Community. Religions 2016, 7, 66. https://0-doi-org.brum.beds.ac.uk/10.3390/rel7060066
Mpofu E. Follower-Centric Influences on Sexual Decision Making in a Pentecostal Church Faith Community. Religions. 2016; 7(6):66. https://0-doi-org.brum.beds.ac.uk/10.3390/rel7060066
Chicago/Turabian StyleMpofu, Elias. 2016. "Follower-Centric Influences on Sexual Decision Making in a Pentecostal Church Faith Community" Religions 7, no. 6: 66. https://0-doi-org.brum.beds.ac.uk/10.3390/rel7060066