Fatal Rattlesnake Envenomation in Northernmost Brazilian Amazon: A Case Report and Literature Overview

 ,
,  , ,
, , 
Abstract
:1. Introduction
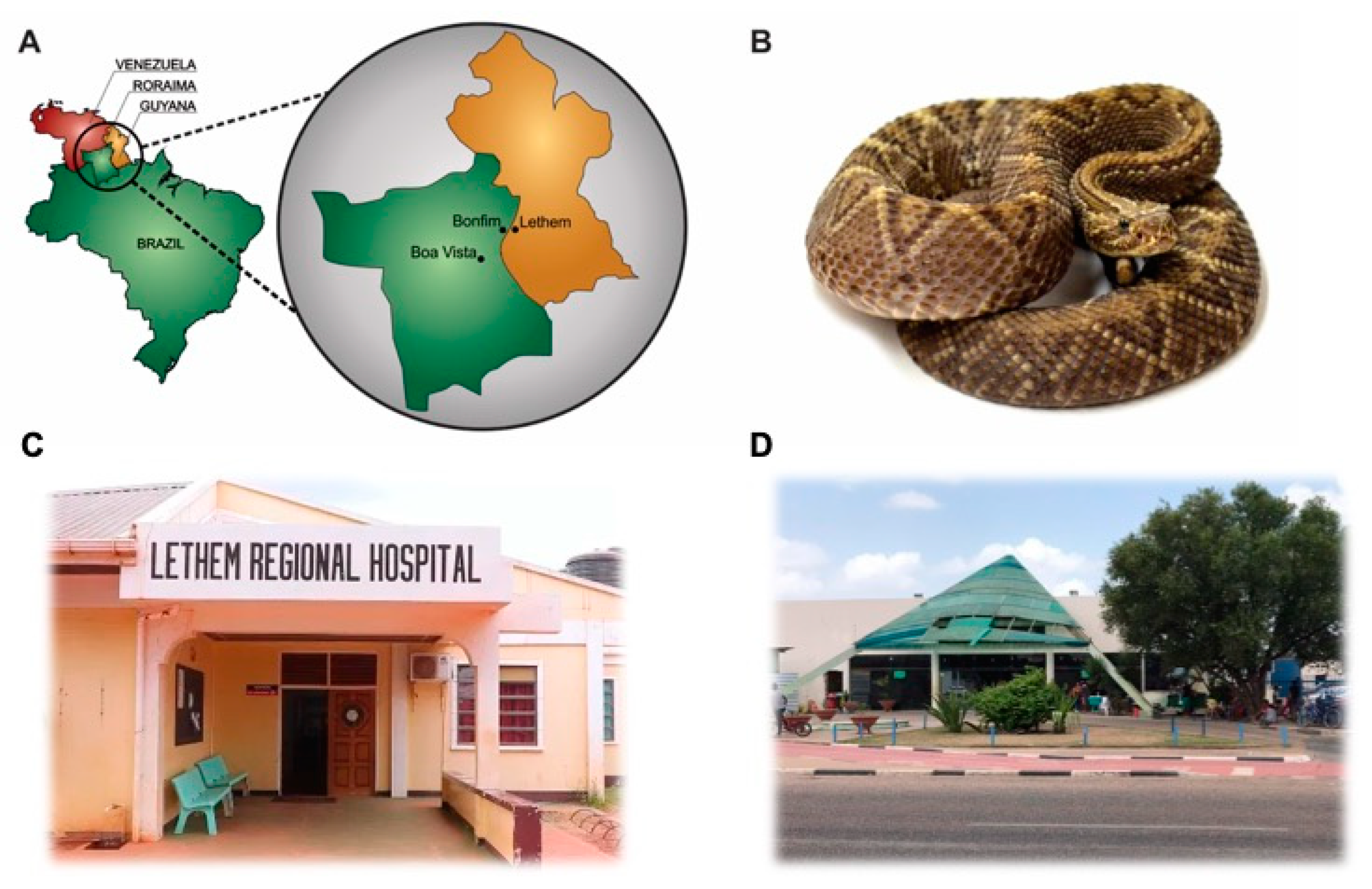
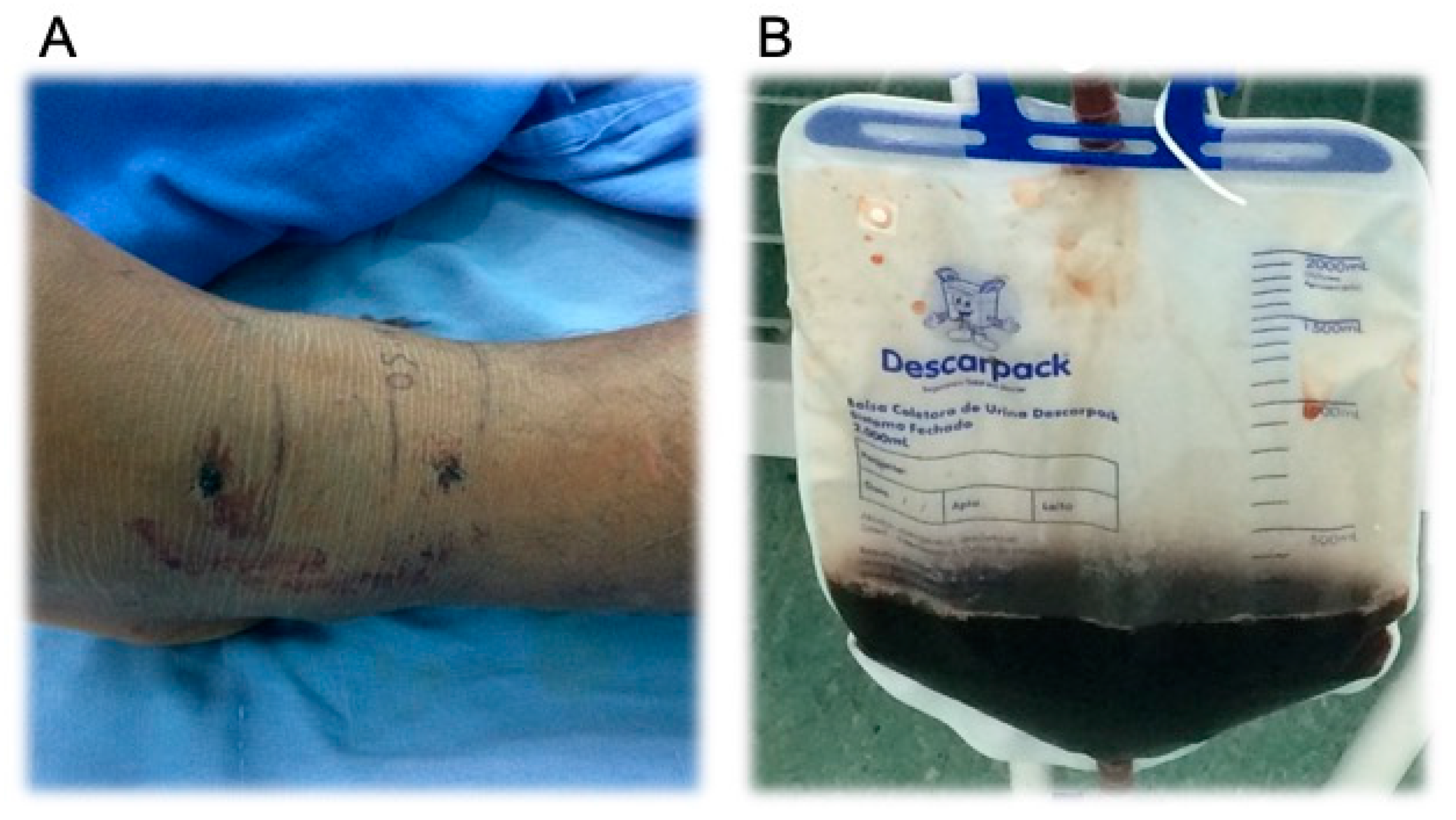
2. Case Presentation Section
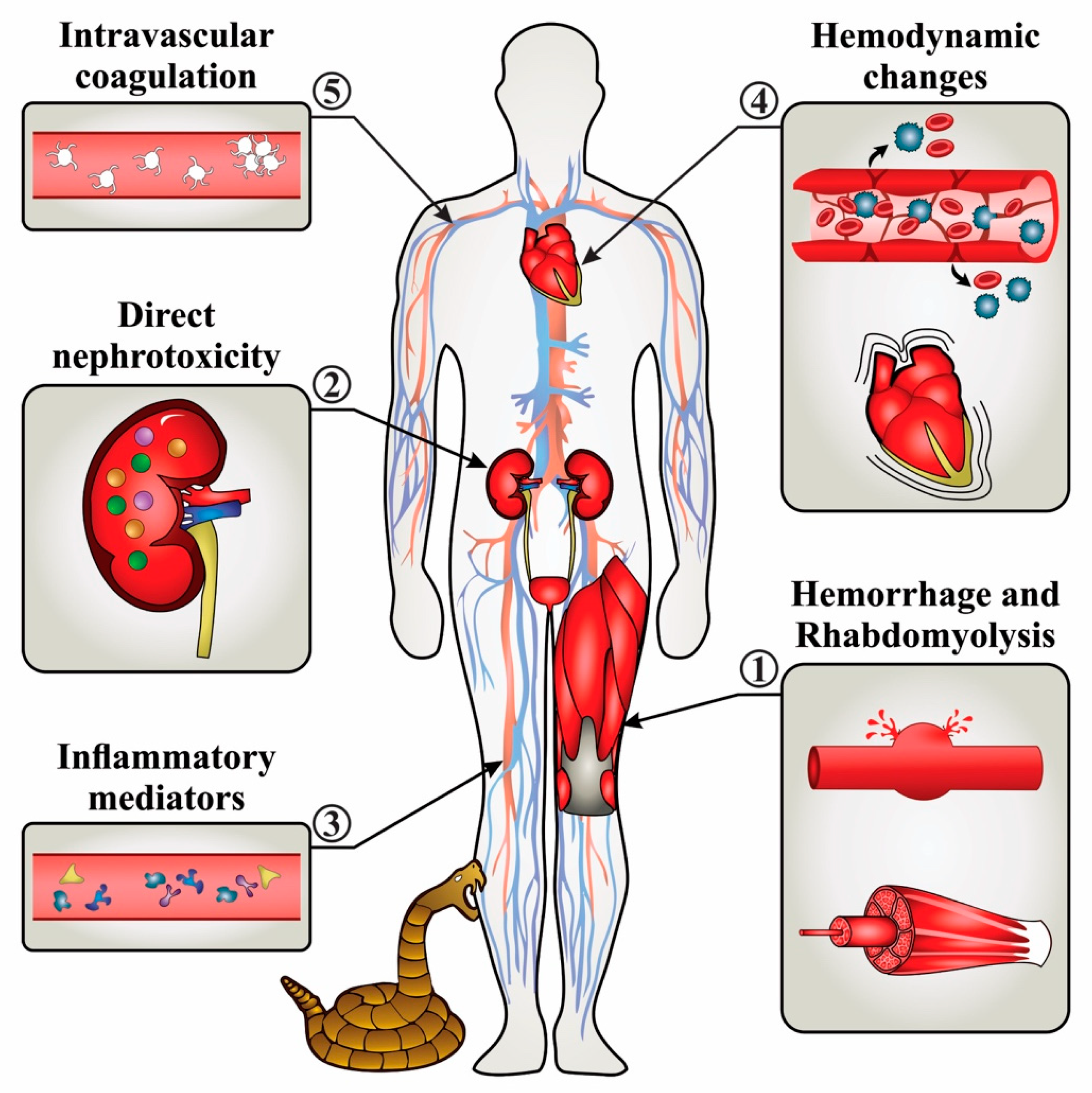
3. Discussion

Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Williams, D.J.; Faiz, M.A.; Abela-Ridder, B.; Ainsworth, S.; Bulfone, T.C.; Nickerson, A.D.; Habib, A.G.; Junghanss, T.; Fan, H.W.; Turner, M.; et al. Strategy for a globally coordinated response to a priority neglected tropical disease: Snakebite envenoming. PLoS Negl. Trop. Dis. 2019, 13, e0007059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutiérrez, J.M.; Williams, D.; Fan, H.W.; Warrell, D.A. Snakebite envenoming from a global perspective: Towards an integrated approach. Toxicon 2010, 56, 1223–1235. [Google Scholar] [CrossRef] [PubMed]
- Chippaux, J.-P. Snakebite envenomation turns again into a neglected tropical disease! J. Venom. Anim. Toxins Incl. Trop. Dis. 2017, 23, 38. [Google Scholar] [CrossRef] [PubMed]
- Costa, H.C.; Bérnils, R.S. Répteis do Brasil e suas Unidades Federativas: Lista de espécies. Herpetol. Bras. 2018, 7, 11–57. [Google Scholar]
- Cardoso, J.L.C.; França, F.O.S.; Wen, F.H.; Málaque, C.M.S.; Haddad, V., Jr. Animais peçonhentos no Brasil: Biologia, clínica e terapêutica dos acidentes. Rev. Inst. Med. Trop. São Paulo 2003, 45, 338. [Google Scholar] [CrossRef]
- Harris, H.S.; Simmons, R.S. A new subspecies of Crotalus durissus (serpentes: Crolalidae) from the Rupununisavanna of Southewestern Guyana. Memórias Inst. Butantan 1976, 40, 305–311. [Google Scholar]
- Souza, W.M.P.; Alexandre-Silva, G.; Cerni, F.A.; Oliveira, I.S.; Zottich, U.; Bassoli, B.K.; Pucca, M.B. Envenomings caused by venomous animals in Roraima: A neglected health problem in the Brazil’s Northernmost state. TCR 2019, 3, 1–8. [Google Scholar] [CrossRef]
- DATASUS TabNet Win32 3.0: Acidentes Por Animais Peçomentos. Notificações Registradas no Sistema de Informação de Agravos de Notificação, Brasil. Available online: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sinannet/cnv/animaisbr.def (accessed on 16 January 2020).
- Nascimento, S.P. do Aspectos epidemiológicos dos acidentes ofídicos ocorridos no Estado de Roraima, Brasil, entre 1992 e 1998. Cad. Saúde Pública 2000, 16, 271–276. [Google Scholar] [CrossRef] [Green Version]
- Alirol, E.; Lechevalier, P.; Zamatto, F.; Chappuis, F.; Alcoba, G.; Potet, J. Antivenoms for Snakebite Envenoming: What Is in the Research Pipeline? PLoS Negl. Trop. Dis. 2015, 9, e0003896. [Google Scholar] [CrossRef] [Green Version]
- Luna, W.F.; Ávila, B.T.; Brazão, C.F.F.; Freitas, F.P.D.P.; Cajado, L.C.D.S.; Bastos, L.O.D.A.; Luna, W.F. Project More Doctors for Brazil in remote areas of the state of Roraima: Relationship between doctors and the Special Supervision Group. Interface Comun. Saúde Educ. 2019, 23, e180029. [Google Scholar] [CrossRef]
- Wen, F.H.; Monteiro, W.M.; da Silva, A.M.M.; Tambourgi, D.V.; da Silva, I.M.; Sampaio, V.S.; dos Santos, M.C.; Sachett, J.; Ferreira, L.C.L.; Kalil, J.; et al. Snakebites and scorpion stings in the Brazilian Amazon: Identifying research priorities for a largely neglected problem. PLoS Negl. Trop. Dis. 2015, 9, e0003701. [Google Scholar]
- The Struggle of Venezuelan Migrants and Asylum Seekers in Northern Brazil|MSF. Available online: https://www.msf.org/struggle-venezuelan-migrants-and-asylum-seekers-northern-brazil (accessed on 30 March 2020).
- Magalhães, S.F.V.; Peixoto, H.M.; Moura, N.; Monteiro, W.M.; de Oliveira, M.R.F. Snakebite envenomation in the Brazilian Amazon: A descriptive study. Trans. R. Soc. Trop. Med. Hyg. 2019, 113, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Rübsamen, K.; Breithaupt, H.; Habermann, B. Biochemistry and pharmacology of the crotoxin complex. Naunyn Schmiedebergs Arch. Pharmak. 1971, 270, 274–288. [Google Scholar] [CrossRef]
- Hendon, R.A.; Fraenkel-Conrat, H. Biological roles of the two components of crotoxin. Proc. Natl. Acad. Sci. (USA) 1971, 68, 1560–1563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faure, G.; Bon, C. Several isoforms of crotoxin are present in individual venoms from the South American rattlesnake Crotalus durissus terrificus. Toxicon 1987, 25, 229–234. [Google Scholar] [CrossRef]
- Breithaupt, H. Enzymatic characteristics of Crotalus phospholipase A2 and the crotoxin complex. Toxicon 1976, 14, 221–233. [Google Scholar] [CrossRef]
- Calvete, J.J.; Sanz, L.; Cid, P.; de la Torre, P.; Flores-Díaz, M.; Dos Santos, M.C.; Borges, A.; Bremo, A.; Angulo, Y.; Lomonte, B.; et al. Snake venomics of the Central American rattlesnake Crotalus simus and the South American Crotalus durissus complex points to neurotoxicity as an adaptive paedomorphic trend along Crotalus dispersal in South America. J. Proteome Res. 2010, 9, 528–544. [Google Scholar] [CrossRef]
- de Carvalho, A.E.Z.; Giannotti, K.; Junior, E.L.; Matsubara, M.; Santos, M.C.D.; Fortes-Dias, C.L.; Teixeira, C. Crotalus durissus ruruima snake venom and a phospholipase A2 isolated from this venom elicit macrophages to form lipid droplets and synthesize inflammatory lipid mediators. J. Immunol. Res. 2019, 2019, 2745286. [Google Scholar] [CrossRef] [Green Version]
- Santos, M.C. dos Characterization of the biological activities of the Crotalus durissus ruruima yellow and white venoms compared with Crotalus durissus terrificus venom: Neutralizing effect of the antivenoms against Crotalus durissus terrificus venom. J. Venom. Anim. Toxins 1996, 2, 163. [Google Scholar] [CrossRef]
- Nascimento, S.P. Epidemiological characteristics of snake bites in the state of Roraima, Brazil, 1992–1998. Cad. Saude Publica 2000, 16, 271–276. [Google Scholar] [CrossRef] [Green Version]
- Frare, B.T.; Silva Resende, Y.K.; Dornelas, B.D.C.; Jorge, M.T.; Souza Ricarte, V.A.; Alves, L.M.; Izidoro, L.F.M. Clinical, laboratory, and therapeutic aspects of Crotalus durissus (South American rattlesnake) victims: A literature review. Biomed Res. Int. 2019, 2019, 1345923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pardal, P.P.D.O.; Silva, C.L.Q.D.; Hoshino, S.D.S.N.; Pinheiro, M.D.F.R. Acidente por cascavel (Crotalus sp) em Ponta de Pedras, Ilha do Marajó, Pará-Relato de caso. Rev. Para. Med. 2007, 21, 69–73. [Google Scholar] [CrossRef]
- WHO. Guidelines for the Production, Control and Regulation of Snake Antivenom Immunoglobulins. Available online: https://www.who.int/bloodproducts/snake_antivenoms/snakeantivenomguide/en/ (accessed on 22 January 2020).
- Azevedo-Marques, M.M.; Cupo, P.; Hering, S.E. Acidentes por animais peçonhentos: Serpentes peçonhentas. Medicina 2003, 36, 480–489. [Google Scholar] [CrossRef] [Green Version]
- Azevedo-Marques, M.M.; Hering, S.E.; Cupo, P. Evidence that Crotalus durissus terrificus (South American rattlesnake) envenomation in humans causes myolysis rather than hemolysis. Toxicon 1987, 25, 1163–1168. [Google Scholar] [CrossRef]
- Bucaretchi, F.; Capitani, E.M.D.; Hyslop, S.; Mello, S.M.; Fernandes, C.B.; Bergo, F.; Nascimento, F.B.P. Compartment syndrome after South American rattlesnake (Crotalus durissus terrificus) envenomation. Clin. Toxicol. 2014, 2, 639–641. [Google Scholar] [CrossRef]
- Pinho, F.M.O.; Pereira, I.D. Ofidismo. Rev. Assoc. Médica Bras. 2001, 47, 24–29. [Google Scholar] [CrossRef]
- Bucaretchi, F.; Herrera, S.R.F.; Hyslop, S.; Baracat, E.C.E.; Vieira, R.J. Snakebites by Crotalus durissus ssp in children in Campinas, São Paulo, Brazil. Rev. Inst. Med. Trop. Sao Paulo 2002, 44, 133–138. [Google Scholar] [CrossRef]
- Madey, J.J.; Price, A.B.; Dobson, J.V.; Stickler, D.E.; McSwain, S.D. Facial diplegia, pharyngeal paralysis, and ophthalmoplegia after a timber rattlesnake envenomation. Pediatr. Emerg. Care 2013, 29, 1213–1216. [Google Scholar] [CrossRef]
- Bush, S.P.; Jansen, P.W. Severe rattlesnake envenomation with anaphylaxis and rhabdomyolysis. Ann. Emerg. Med. 1995, 25, 845–848. [Google Scholar] [CrossRef]
- Jorge, M.T.; Ribeiro, L.A. Epidemiologia e quadro clínico do acidente por cascavel sul-americana (Crotalus durissus). Rev. Inst. Med. Trop. São Paulo 1992, 34, 347–354. [Google Scholar] [CrossRef]
- Pinho, F.M.O.; Zanetta, D.M.T.; Burdmann, E.A. Acute renal failure after Crotalus durissus snakebite: A prospective survey on 100 patients. Kidney Int. 2005, 67, 659–667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albuquerque, P.L.M.M.; Jacinto, C.N.; Silva, G.B.; Lima, J.B.; Veras, M.D.S.B.; Daher, E.F. Acute kidney injury caused by Crotalus and Bothrops snake venom: A review of epidemiology, clinical manifestations and treatment. Rev. Inst. Med. Trop. Sao Paulo 2013, 55, 295–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moysés-Neto, M.; Guimarães, F.M.; Ayoub, F.H.; Vieira-Neto, O.M.; Costa, J.A.C.; Dantas, M. Acute renal failure and hypercalcemia. Ren. Fail. 2006, 28, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Drews, R.E.; Weinberger, S.E. Thrombocytopenic disorders in critically Ill patients. Am. J. Respir. Crit. Care Med. 2000, 162, 347–351. [Google Scholar] [CrossRef] [Green Version]
- Kohli, H.S.; Sakhuja, V. Snake bites and acute renal failure. Saudi J. Kidney Dis. Transpl. 2003, 14, 165–176. [Google Scholar]
- Odeleye, A.A.; Presley, A.E.; Passwater, M.E.; Mintz, P.D. Rattlesnake venom-induced thrombocytopenia. Ann. Clin. Lab. Sci. 2004, 34, 467–470. [Google Scholar]
- Sano-Martins, I.S.; Tomy, S.C.; Campolina, D.; Dias, M.B.; de Castro, S.C.B.; de Sousa-e-Silva, M.C.C.; Amaral, C.F.S.; Rezende, N.A.; Kamiguti, A.S.; Warrell, D.A.; et al. Coagulopathy following lethal and non-lethal envenoming of humans by the South American rattlesnake (Crotalus durissus) in Brazil. QJM 2001, 94, 551–559. [Google Scholar] [CrossRef] [Green Version]
- Elbey, B.; Baykal, B.; Yazgan, Ü.C.; Zengin, Y. The prognostic value of the neutrophil/lymphocyte ratio in patients with snake bites for clinical outcomes and complications. Saudi J. Biol. Sci. 2017, 24, 362–366. [Google Scholar] [CrossRef] [Green Version]
- Claudet, I.; Grouteau, E.; Cordier, L.; Franchitto, N.; Bréhin, C. Hyperglycemia is a risk factor for high-grade envenomations after European viper bites (Vipera spp.) in children. Clin. Toxicol. 2016, 54, 34–39. [Google Scholar] [CrossRef]
- Gaballa, M.; Taher, T.; Brodin, L.A.; van der Linden, J.; O’Reilly, K.; Hui, W.; Brass, N.; Cheung, P.K.; Grip, L. Images in cardiovascular medicine. Myocardial infarction as a rare consequence of a snakebite: Diagnosis with novel echocardiographic tissue Doppler techniques. Circulation 2005, 112, e140–e142. [Google Scholar] [CrossRef]
- Johnston, M.A.; Fatovich, D.M.; Haig, A.D.; Daly, F.F.S. Successful resuscitation after cardiac arrest following massive brown snake envenomation. Med. J. Aust. 2002, 177, 646–649. [Google Scholar] [CrossRef]
- Dhaliwal, U. Cortical blindness: An unusual sequela of snake bite. Indian J. Ophthalmol. 1999, 47, 191. [Google Scholar] [PubMed]
- Gomes, R.A.F.; Cantarelli, F.L.; Vieira, F.A.; Macedo, A.R.A., Jr.; Gouveia, M.M.D.A.; Feitosa, A.D.D.M. Myocardial infarction after snake bite. Int. J. Cardiovasc. Sci. 2018, 31, 79–81. [Google Scholar] [CrossRef]
- Brown, R.; Dewar, H.A. Heart damage following Adder bite in England. Br. Heart J. 1965, 27, 144–147. [Google Scholar] [CrossRef] [Green Version]
- Upadhyaya, A.C.; Murthy, G.L.; Sahay, R.K.; Srinivasan, V.R.; Shantaram, V. Snake bite presenting as acute myocardial infarction, ischaemic cerebrovascular accident, acute renal failure and disseminated intravascular coagulopathy. J. Assoc. Physicians India 2000, 48, 1109–1110. [Google Scholar] [PubMed]
- Hifumi, T.; Sakai, A.; Kondo, Y.; Yamamoto, A.; Morine, N.; Ato, M.; Shibayama, K.; Umezawa, K.; Kiriu, N.; Kato, H.; et al. Venomous snake bites: Clinical diagnosis and treatment. J. Intensiv. Care 2015, 3, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kini, R.M. Anticoagulant proteins from snake venoms: Structure, function and mechanism. Biochem. J. 2006, 397, 377–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Oliveira, I.S.; Pucca, M.B.; Sampaio, S.V.; Arantes, E.C. Antivenomic approach of different Crotalus durissus collilineatus venoms. J. Venom. Anim. Toxins Incl. Trop. Dis. 2018, 24, 34. [Google Scholar] [CrossRef] [PubMed]
- Instituto Butantan Soro Anticrotalico Instituto Butantan. Available online: https://consultaremedios.com.br/ (accessed on 22 January 2020).
- Laustsen, A.H.; Gutiérrez, J.M.; Knudsen, C.; Johansen, K.H.; Bermúdez-Méndez, E.; Cerni, F.A.; Jürgensen, J.A.; Ledsgaard, L.; Martos-Esteban, A.; Øhlenschlæger, M.; et al. Pros and cons of different therapeutic antibody formats for recombinant antivenom development. Toxicon 2018, 146, 151–175. [Google Scholar] [CrossRef]
- Ponraj, D.; Gopalakrishnakone, P. Renal lesions in rhabdomyolysis caused by Pseudechis australis snake myotoxin. Kidney Int. 1997, 51, 1956–1969. [Google Scholar] [CrossRef] [Green Version]
- Tracz, M.J.; Alam, J.; Nath, K.A. Physiology and pathophysiology of heme: Implications for kidney disease. J. Am. Soc. Nephrol. 2007, 18, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Sitprija, V.; Sitprija, S. Renal effects and injury induced by animal toxins. Toxicon 2012, 60, 943–953. [Google Scholar] [CrossRef] [PubMed]
- Dineshkumar, T.; Dhanapriya, J.; Murugananth, S.; Surendar, D.; Sakthirajan, R.; Rajasekar, D.; Balasubramaniyan, T.; Gopalakrishnan, N. Snake envenomation-induced acute interstitial nephritis. J. Integr. Nephrol. 2018, 5, 14. [Google Scholar]
- Martins, A.M.C.; Monteiro, H.S.A.; Júnior, E.O.G.; Menezes, D.B.; Fonteles, M.C. Effects of Crotalus durissus cascavella venom in the isolated rat kidney. Toxicon 1998, 36, 1441–1450. [Google Scholar] [CrossRef]
- Voronov, E.; Apte, R.N.; Sofer, S. The systemic inflammatory response syndrome related to the release of cytokines following severe envenomation. J. Venom. Anim. Toxins 1999, 5, 5–33. [Google Scholar] [CrossRef]
- Kinsey, G.R.; Li, L.; Okusa, M.D. Inflammation in acute kidney injury. NEE 2008, 109, e102–e107. [Google Scholar] [CrossRef]
- Sakwiwatkul, K.; Chaiyabutr, N.; Sitprija, V. Renal function following sea snake venom (Lapemis hardwicki) administration in dogs treated with sodium bicarbonate solution. J. Nat. Toxins 2002, 11, 111–121. [Google Scholar]
- Isbister, G.K.; Little, M.; Cull, G.; McCoubrie, D.; Lawton, P.; Szabo, F.; Kennedy, J.; Trethewy, C.; Luxton, G.; Brown, S.G.A.; et al. Thrombotic microangiopathy from Australian brown snake (Pseudonaja) envenoming. Intern. Med. J. 2007, 37, 523–528. [Google Scholar] [CrossRef]
- Gutiérrez, J.M. Global availability of antivenoms: The relevance of public manufacturing laboratories. Toxins 2019, 11, 5. [Google Scholar] [CrossRef] [Green Version]
- Nishioka, S.D.A.; orge, M.T.; Silveira, P.V.; Ribeiro, L.A. South American rattlesnake bite and soft-tissue infection: Report of a case. Rev. Soc. Bras. Med. Trop. 2000, 33, 401–402. [Google Scholar] [CrossRef] [Green Version]
- Baum, R.A.; Bronner, J.; Akpunonu, P.D.S.; Plott, J.; Bailey, A.M.; Keyler, D.E. Crotalus durissus terrificus (viperidae; crotalinae) envenomation: Respiratory failure and treatment with antivipmyn TRI® antivenom. Toxicon 2019, 163, 32–35. [Google Scholar] [CrossRef]
- Isbister, G.K.; Duffull, S.B.; Brown, S.G.A. Failure of antivenom to improve recovery in Australian snakebite coagulopathy. QJM 2009, 102, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Kalantri, S.; Singh, A.; Joshi, R.; Malamba, S.; Ho, C.; Ezoua, J.; Morgan, M. Clinical predictors of in-hospital mortality in patients with snake bite: A retrospective study from a rural hospital in central India. Trop. Med. Int. Health 2006, 11, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Chugh, K.S.; Pal, Y.; Chakravarty, R.N.; Datta, B.N.; Mehta, R.; Sakhuja, V.; Mandal, A.K.; Sommers, S.C. Acute Renal Failure Following Poisonous Snakebite. Am. J. Kidney Dis. 1984, 4, 30–38. [Google Scholar] [CrossRef]
- Danzig, L.E.; Abels, G.H. Hemodialysis of Acute Renal Failure Following Rattlesnake Bite, with Recovery. JAMA 1961, 175, 136–137. [Google Scholar] [CrossRef]
- Makino, J.; Uchino, S.; Morimatsu, H.; Bellomo, R. A quantitative analysis of the acidosis of cardiac arrest: A prospective observational study. Crit. Care 2005, 9, R357–R362. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Analytes | Days | Reference Range & | |
|---|---|---|---|
| 0 | 1 | ||
| Hemoglobin | 16.3 * | 15.2 | 13.5–18.0 g/dL |
| Hematocrit | 46.7 | 45.7 | 40.0%–50.0% |
| Leucocytes | 16,810 * | 15,920 * | 4000–10,000 cells/µL |
| Neutrophils | - | 94.00 * | 50.0%–70.0% |
| Platelets | 158,000 | 16,000 * | 150,000–400,000/µL |
| PT | 14.2 * | 13.5 | 10.0–14.0 s |
| PTT | 32.2 | 36.1 | 25.0–39.0 s |
| Na+ | 139.0 | 133.0 * | 135.0–145.0 mmol/L |
| K+ | 4.0 | 3.8 | 3.5–5.1 mmol/L |
| Ca2+ | 0.68 * | 0.72 * | 1.17–1.32 mmol/L |
| Cl− | 100.0 | 107.0 | 98.0–107.0 mmol/L |
| Glucose | 133.26 * | - | 60.0–99.0 mg/dL |
| Urea | 58.71 * | - | 15–40 mg/dL |
| Creatinine | 1.65 * | - | 0.7–1.4 mg/dL |
| ALT | 466.6 * | - | 5.0–48.8 U/mL |
| AKP | 56.21 | - | 27.0–100.0 mg/dL |
| γGT | 20.5 | - | 12.0–45.0 U/L |
| LDH | 151.52 * | - | 200.0–480.0 U/L |
| CRP | 4.56 | - | 0.0–8.0 mg/L |
| Lactate | 35.53 * | - | 4.5–19.8 mg/dL |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Medeiros, J.M.; Oliveira, I.S.; Ferreira, I.G.; Alexandre-Silva, G.M.; Cerni, F.A.; Zottich, U.; B. Pucca, M. Fatal Rattlesnake Envenomation in Northernmost Brazilian Amazon: A Case Report and Literature Overview. Reports 2020, 3, 9. https://0-doi-org.brum.beds.ac.uk/10.3390/reports3020009
Medeiros JM, Oliveira IS, Ferreira IG, Alexandre-Silva GM, Cerni FA, Zottich U, B. Pucca M. Fatal Rattlesnake Envenomation in Northernmost Brazilian Amazon: A Case Report and Literature Overview. Reports. 2020; 3(2):9. https://0-doi-org.brum.beds.ac.uk/10.3390/reports3020009
Chicago/Turabian StyleMedeiros, Jilvando M., Isadora S. Oliveira, Isabela G. Ferreira, Gabriel Melo Alexandre-Silva, Felipe A. Cerni, Umberto Zottich, and Manuela B. Pucca. 2020. "Fatal Rattlesnake Envenomation in Northernmost Brazilian Amazon: A Case Report and Literature Overview" Reports 3, no. 2: 9. https://0-doi-org.brum.beds.ac.uk/10.3390/reports3020009