Key Enabling Technologies for Point-of-Care Diagnostics

 , , ,
, , , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
- Quick reliable response: A tests should last less than 1 h and the procedure should be as simple as possible, with few steps, and in compliance with the basic rules of good laboratory practice.
- Accuracy: sensitivity/specificity and detection limits should meet the legal limits needed for the specific application, improving or at least equaling the performances of traditional tests in order to enable medical decisions without further expensive tests so reducing impact on the public health costs. In this respect, nanotech-based approaches exploiting novel nanomaterials can provide new amplification methods for signal transduction with significant improvement in sensitivity. These include the use of metallic nanoparticles (NPs) or nanostructured metal layers for enhanced SPR or SERS analysis or as electrocatalytic labels as well as the use of nanowires, nanotubes and graphene [2,3].
- Ease of use: the test should be easily performed by unskilled people after minimal training, and the results should be clear and easy to understand.
- Self-containment: users should only be required to collect and deliver samples into the device. Reagent handling, analysis, data interpretation and storing of waste products should limit the intervention of users and their exposure to biohazard as much as possible.
- Portability and robustness: the tests should be carried out in the field, if needed, implying that they should be portable, resist the transport, and have a long shelf life. In the best cases, they should not even require electricity to work, neither cold storage.
- Low-cost: the platforms should be affordable for public healthcare systems, as well as for users and patients. The tests should be cheaper than standard, and should reduce the costs for the patient—for example in low-resource settings, where even the cost of travelling to healthcare structures could be discouraging.
- Multiplexing capacity: Multiplexed point-of-care testing (xPOCT), able to perform more than one analysis simultaneously [4], could enable a full characterization of a biological sample and a improvement in clinical diagnostics [5]—for example obtaining a complete molecular fingerprint of a patient allowing precision medicine approaches [5,6].
2. POC Technologies in Low-Resource Settings and Developed World
3. POC Tools for Personalized Medicine
3.1. POC Tools for Cells Identification
- Biochemical methods. Usually CTCs are distinguished from haematological cells using antigens expressed on epithelial cells only (e.g., EpCAM in the immunomagnetic Veridex CellSearch® system for breast, colon, and prostate cancer). These methods are limited by CTC’s heterogeneity and the lack of universally approved tumour markers for affinity capture. Moreover, they are intrinsically biased by the positive selection induced by the capture system. There will be some cells, such as those undergoing epithelial to mesenchymal transition (EMT) (the most phenotypically aggressive), which will remain out of the analysis. In addition, the binding of antibodies to CTCs surface could induce phenotypical alterations, resulting in a misleading subsequent molecular studies.
- Physical methods are label-free and based on differences in physical properties such as size, shape, plasticity and electrical polarizability. In this case, no specific surface biomarkers are needed with a significant advantage. However, the physical properties of CTCs can overlap with those of residential blood cells and accurate techniques for CTC isolation are required.
3.2. POC Tools for Protein Analysis
3.3. POC Tools for Nucleic Acids Detection
4. Innovative Sensing Elements for POC Applications
4.1. Molecularly Imprinted Polymers
4.2. Lyophilized Reagents
4.3. Hydrogels
5. Smartphone-Based Platforms
6. From Chip in a Lab to Lab-on-a-Chip—A Case Study
7. Market Challenges
8. Conclusions
Funding
Conflicts of Interest
References
- Yager, P.; Domingo, G.J.; Gerdes, J. Point-of-care diagnostics for global health. Annu. Rev. Biomed. Eng. 2008, 10, 107–144. [Google Scholar] [CrossRef] [PubMed]
- Syedmoradi, L.; Daneshpour, M.; Alvandipour, M.; Gomez, F.A.; Hajghassem, H.; Omidfar, K. Point of care testing: The impact of nanotechnology. Biosens. Bioelectr. 2017, 87, 373–387. [Google Scholar] [CrossRef] [PubMed]
- Quesada-González, D.; Merkoçi, A. Nanomaterial-based devices for point-of-care diagnostic applications. Chem. Soc. Rev. 2018, 47, 4697–4709. [Google Scholar] [CrossRef] [PubMed]
- Kling, A.; Chatelle, C.; Armbrecht, L.; Qelibari, E.; Kieninger, J.; Dincer, C.; Weber, W.; Urban, G. Multianalyte Antibiotic Detection on an Electrochemical Microfluidic Platform. Anal. Chem. 2016, 88, 10036–10043. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Macdonald, J. Multiplexed lateral flow biosensors: Technological advances for radically improving point-of-care diagnoses. Biosens. Bioelectron. 2016, 83, 177–192. [Google Scholar] [CrossRef] [PubMed]
- Dincer, C.; Bruch, R.; Kling, A.; Dittrich, P.S.; Urban, G.A. Multiplexed Point-of-Care Testing—xPOCT. Trends Biotechnol. 2017, 35, 728–742. [Google Scholar] [CrossRef] [PubMed]
- Chan, M. Ebola Virus Disease in West Africa—No Early End to the Outbreak. N. Eng. J. Med. 2014, 371, 1183–1185. [Google Scholar] [CrossRef] [PubMed]
- Pollock, N.R.; Colby, D.; Rolland, J.P. A point-of-care paper-based fingerstick transaminase test: Toward low-cost “lab-on-a-chip” technology for the developing world. Clin. Gastroenterol. Hepatol. 2013, 11, 478–482. [Google Scholar] [CrossRef] [PubMed]
- Becquart, P.; Mahlakoiv, T.; Nkoghe, D.; Leroy, E.M. Identification of Continuous Human B-Cell Epitopes in the VP35, VP40, Nucleoprotein and Glycoprotein of Ebola Virus. PLoS ONE 2014, 9, e96360. [Google Scholar] [CrossRef] [PubMed]
- Euler, M.; Wang, Y.J.; Heidenreich, D.; Patel, P.; Strohmeier, O.; Hakenberg, S.; Niedrig, M.; Hufert, F.T.; Weidmann, M. Development of a Panel of Recombinase Polymerase Amplification Assays for Detection of Biothreat Agents. J. Clin. Microbiol. 2013, 51, 1110–1117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armah, G.E.; Sow, S.O.; Breiman, R.F.; Dallas, M.J.; Tapia, M.D.; Feikin, D.R.; Binka, F.N.; Steele, A.D.; Laserson, K.F.; Ansah, N.A.; et al. Efficacy of pentavalent rotavirus vaccine against severe rotavirus gastroenteritis in infants in developing countries in sub-Saharan Africa: A randomised, double-blind, placebo-controlled trial. Lancet 2010, 376, 606–614. [Google Scholar] [CrossRef]
- Researchers Seek Crucial Tool: A Fast, Finger-Prick Ebola Test. Available online: http://www.nytimes.com/2014/11/05/business/ebola-researchers-rush-to-find-a-fast-diagnostic-test.html?_r=0 (accessed on 19 October 2018).
- Boschi-Pinto, C.; Velebit, L.; Shibuya, K. Estimating child mortality due to diarrhoea in developing countries. Bull. World Health Organ. 2008, 86, 710–717. [Google Scholar] [CrossRef] [PubMed]
- Chiriaco, M.S.; Primiceri, E.; D’Amone, E.; Ionescu, R.E.; Rinaldi, R.; Maruccio, G. EIS microfluidic chips for flow immunoassay and ultrasensitive cholera toxin detection. Lab Chip 2011, 11, 658–663. [Google Scholar] [CrossRef] [PubMed]
- Irenge, L.M.; Gala, J.L. Rapid detection methods for Bacillus anthracis in environmental samples: A review. Appl. Microbiol. Biotechnol. 2012, 93, 1411–1422. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Hachamovitch, R.; Menon, V. Current Trial-Associated Outcomes with Warfarin in Prevention of Stroke in Patients with Nonvalvular Atrial Fibrillation A Meta-analysis. Arch. Intern. Med. 2012, 172, 623–631. [Google Scholar] [PubMed]
- Heneghan, C.; Ward, A.; Perera, R.; Bankhead, C.; Fuller, A.; Stevens, R.; Bradford, K.; Tyndel, S.; Alonso-Coello, P.; Ansell, J.; et al. Self-monitoring of oral anticoagulation: Systematic review and meta-analysis of individual patient data. Lancet 2012, 379, 322–334. [Google Scholar] [CrossRef]
- Sunderji, R.; Gin, K.; Shalansky, K.; Carter, C.; Chambers, K.; Davies, C.; Schwartz, L.; Fung, A. A randomized trial of patient self-managed versus physician-managed oral anticoagulation. Can. J. Cardiol. 2004, 20, 1117–1123. [Google Scholar] [PubMed]
- Riegel, B.; Hanlon, A.L.; McKinley, S.; Moser, D.K.; Meischke, H.; Doering, L.V.; Davidson, P.; Pelter, M.M.; Dracup, K. Differences in mortality in acute coronary syndrome symptom clusters. Am. Heart J. 2010, 159, 392–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noncommunicable Diseases. Available online: http://www.who.int/en/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 19 October 2018).
- Cancer Diagnostics Market (Tumor Biomarker Tests, Imaging, Endoscopy and Biopsy)—Global Industry Analysis, Size, Share, Growth, Trends and Forecast, 2014–2020. Available online: http://www.transparencymarketresearch.com/cancer-diagnostics-market.html (accessed on 19 October 2018).
- Barry, M.J. Screening for Prostate Cancer—The Controversy That Refuses to Die. N. Eng. J. Med. 2009, 360, 1351–1354. [Google Scholar] [CrossRef] [PubMed]
- Thompson, I.M.; Ankerst, D.P.; Tangen, C.M. Prostate-Specific Antigen, Risk Factors, and Prostate Cancer: Confounders Nestled in an Enigma. J. Natl. Cancer Inst. 2010, 102, 1299–1301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finne, P.; Auvinen, A.; Aro, J.; Juusela, H.; Maattanen, L.; Rannikko, S.; Hakama, M.; Tammela, T.L.; Stenman, U.H. Estimation of prostate cancer risk on the basis of total and free prostate-specific antigen, prostate volume and digital rectal examination. Eur. Urol. 2002, 41, 619–626. [Google Scholar] [CrossRef]
- Chiriacò, M.S.; Primiceri, E.; Montanaro, A.; de Feo, F.; Leone, L.; Rinaldi, R.; Maruccio, G. On-chip screening for prostate cancer: An EIS microfluidic platform for contemporary detection of free and total PSA. Analyst 2013, 138, 5404–5410. [Google Scholar] [CrossRef] [PubMed]
- Yetisen, A.K.; Martinez-Hurtado, J.L.; Uenal, B.; Khademhosseini, A.; Butt, H. Wearables in Medicine. Adv. Mater. 2018, 30, 26. [Google Scholar] [CrossRef] [PubMed]
- Salvatore, G.A.; Sulzle, J.; Dalla Valle, F.; Cantarella, G.; Robotti, F.; Jokic, P.; Knobelspies, S.; Daus, A.; Buthe, L.; Petti, L.; et al. Biodegradable and Highly Deformable Temperature Sensors for the Internet of Things. Adv. Funct. Mater. 2017, 27, 10. [Google Scholar] [CrossRef]
- Dehennis, A.; Mortellaro, M.A.; Ioacara, S. Multisite Study of an Implanted Continuous Glucose Sensor Over 90 Days in Patients with Diabetes Mellitus. J. Diabetes Sci. Technol. 2015, 9, 951–956. [Google Scholar] [CrossRef] [PubMed]
- Rose, D.P.; Ratterman, M.E.; Griffin, D.K.; Hou, L.L.; Kelley-Loughnane, N.; Naik, R.R. Adhesive RFID Sensor Patch for Monitoring of Sweat Electrolytes. IEEE Trans. Biomed. Eng. 2015, 62, 1457–1465. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Valdes-Ramirez, G.; Bandodkar, A.J.; Jia, W.Z.; Martinez, A.G.; Ramirez, J.; Mercier, P.; Wang, J. Non-invasive mouthguard biosensor for continuous salivary monitoring of metabolites. Analyst 2014, 139, 1632–1636. [Google Scholar] [CrossRef] [PubMed]
- Ascaso, F.J.; Huerva, V. Noninvasive Continuous Monitoring of Tear Glucose Using Glucose-Sensing Contact Lenses. Opt. Vis. Sci. 2016, 93, 426–434. [Google Scholar] [CrossRef] [PubMed]
- Hood, L.; Friend, S.H. Predictive, personalized, preventive, participatory (P4) cancer medicine. Nat. Rev. Clin. Oncol. 2011, 8, 184–187. [Google Scholar] [CrossRef] [PubMed]
- Tian, Q.; Price, N.D.; Hood, L. Systems cancer medicine: Towards realization of predictive, preventive, personalized and participatory (P4) medicine. J. Intern. Med. 2012, 271, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Schneiderhan-Marra, N.; Joos, T.O. Protein microarrays for personalized medicine. Biochim. Clin. 2011, 35, 491–502. [Google Scholar] [CrossRef] [PubMed]
- Hood, L.; Flores, M. A personal view on systems medicine and the emergence of proactive P4 medicine: Predictive, preventive, personalized and participatory. New Biotechnol. 2012, 29, 613–624. [Google Scholar] [CrossRef] [PubMed]
- Schneider, L.; Stoeckel, D.; Kehl, T.; Gerasch, A.; Ludwig, N.; Leidinger, P.; Huwer, H.; Tenzer, S.; Kohlbacher, O.; Hildebrandt, A.; et al. DrugTargetInspector: An assistance tool for patient treatment stratification. Int. J. Cancer 2016, 138, 1765–1776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerlinger, M.; Rowan, A.J.; Horswell, S.; Larkin, J.; Endesfelder, D.; Gronroos, E.; Martinez, P.; Matthews, N.; Stewart, A.; Tarpey, P.; et al. Intratumor Heterogeneity and Branched Evolution Revealed by Multiregion Sequencing. N. Eng. J. Med. 2012, 366, 883–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, L.-J.; Pan, Y.-D.; Pei, X.-Y.; Chen, H.; Nguyen, S.; Kashyap, A.; Liu, J.; Wu, J. Capturing circulating tumor cells of hepatocellular carcinoma. Cancer Lett. 2012, 326, 17–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rana, A.; Zhang, Y.; Esfandiari, L. Advancements in microfluidic technologies for isolation and early detection of circulating cancer-related biomarkers. Analyst 2018, 143, 2971–2991. [Google Scholar] [CrossRef] [PubMed]
- Hematology Testing & White Blood Cell Count (WBC). Available online: https://www.hemocue.com/en/solutions/hematology (accessed on 19 October 2018).
- Evaluation of Chempaq XBC. Available online: https://www.skup.org/GetFile.ashx?fileid=312 (accessed on 19 October 2018).
- Allard, W.J.; Matera, J.; Miller, M.C.; Repollet, M.; Connelly, M.C.; Rao, C.; Tibbe, A.G.J.; Uhr, J.W.; Terstappen, L. Tumor cells circulate in the peripheral blood of all major carcinomas but not in healthy subjects or patients with nonmalignant diseases. Clin. Cancer Res. 2004, 10, 6897–6904. [Google Scholar] [CrossRef] [PubMed]
- Steeg, P.S. Tumor metastasis: Mechanistic insights and clinical challenges. Nat. Med. 2006, 12, 895–904. [Google Scholar] [CrossRef] [PubMed]
- Bidard, F.C.; Peeters, D.J.; Fehm, T.; Nole, F.; Gisbert-Criado, R.; Mavroudis, D.; Grisanti, S.; Generali, D.; Garcia-Saenz, J.A.; Stebbing, J.; et al. Clinical validity of circulating tumour cells in patients with metastatic breast cancer: A pooled analysis of individual patient data. Lancet Oncol. 2014, 15, 406–414. [Google Scholar] [CrossRef]
- Alberter, B.; Klein, C.A.; Polzer, B. Single-cell analysis of CTCs with diagnostic precision: Opportunities and challenges for personalized medicine. Expert Rev. Mol. Diagn. 2016, 16, 25–38. [Google Scholar] [CrossRef] [PubMed]
- Lyberopoulou, A.; Aravantinos, G.; Efstathopoulos, E.P.; Nikiteas, N.; Bouziotis, P.; Isaakidou, A.; Papalois, A.; Marinos, E.; Gazouli, M. Mutational Analysis of Circulating Tumor Cells from Colorectal Cancer Patients and Correlation with Primary Tumor Tissue. PLoS ONE 2015, 10, e0123902. [Google Scholar] [CrossRef] [PubMed]
- Alix-Panabieres, C.; Pantel, K. Circulating Tumor Cells: Liquid Biopsy of Cancer. Clin. Chem. 2013, 59, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Van de Stolpe, A.; Pantel, K.; Sleijfer, S.; Terstappen, L.W.; den Toonder, J.M.J. Circulating Tumor Cell Isolation and Diagnostics: Toward Routine Clinical Use. Cancer Res. 2011, 71, 5955–5960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurkuri, M.D.; Al-Ejeh, F.; Shi, J.Y.; Palms, D.; Prestidge, C.; Griesser, H.J.; Brown, M.P.; Thierry, B. Plasma functionalized PDMS microfluidic chips: Towards point-of-care capture of circulating tumor cells. J. Mater. Chem. 2011, 21, 8841–8848. [Google Scholar] [CrossRef]
- Autebert, J.; Coudert, B.; Champ, J.; Saias, L.; Guneri, E.T.; Lebofsky, R.; Bidard, F.-C.; Pierga, J.-Y.; Farace, F.; Descroix, S.; et al. High purity microfluidic sorting and analysis of circulating tumor cells: Towards routine mutation detection. Lab Chip 2015, 15, 2090–2101. [Google Scholar] [CrossRef] [PubMed]
- Sarioglu, A.F.; Aceto, N.; Kojic, N.; Donaldson, M.C.; Zeinali, M.; Hamza, B.; Engstrom, A.; Zhu, H.; Sundaresan, T.K.; Miyamoto, D.T.; et al. A microfluidic device for label-free, physical capture of circulating tumor cell clusters. Nat. Methods 2015, 12, 685. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Huang, D.; Tang, W.; Jiang, D.; Chen, K.; Yi, H.; Xiang, N.; Ni, Z. A low cost and quasi-commercial polymer film chip for high-throughput inertial cell isolation. RSC Adv. 2016, 6, 9734–9742. [Google Scholar] [CrossRef]
- Sollier, E.; Go, D.E.; Che, J.; Gossett, D.R.; O’Byrne, S.; Weaver, W.M.; Kummer, N.; Rettig, M.; Goldman, J.; Nickols, N.; et al. Size-selective collection of circulating tumor cells using Vortex technology. Lab Chip 2014, 14, 63–77. [Google Scholar] [CrossRef] [PubMed]
- Alazzam, A.; Stiharu, I.; Bhat, R.; Meguerditchian, A.-N. Interdigitated comb-like electrodes for continuous separation of malignant cells from blood using dielectrophoresis. Electrophoresis 2011, 32, 1327–1336. [Google Scholar] [CrossRef] [PubMed]
- Antfolk, M.; Magnusson, C.; Augustsson, P.; Lija, H.; Laurell, T. Acoustofluidic, Label-Free Separation and Simultaneous Concentration of Rare Tumor Cells from White Blood Cells. Anal. Chem. 2015, 87, 9322–9328. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Mao, Z.; Peng, Z.; Zhou, L.; Chen, Y.; Huang, P.-H.; Truica, C.I.; Drabick, J.J.; El-Deiry, W.S.; Dao, M.; et al. Acoustic separation of circulating tumor cells. Proc. Natl. Acad. Sci. USA 2015, 112, 4970–4975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sano, M.B.; Caldwell, J.L.; Davalos, R.V. Modeling and development of a low frequency contactless dielectrophoresis (cDEP) platform to sort cancer cells from dilute whole blood samples. Biosens. Bioelectron. 2011, 30, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Mok, J.; Mindrinos, M.N.; Davis, R.W.; Javanmard, M. Digital microfluidic assay for protein detection. Proc. Natl. Acad. Sci. USA 2014, 111, 2110–2115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gogoi, P.; Sepehri, S.; Zhou, Y.; Gorin, M.A.; Paolillo, C.; Capoluongo, E.; Gleason, K.; Payne, A.; Boniface, B.; Cristofanilli, M.; et al. Development of an Automated and Sensitive Microfluidic Device for Capturing and Characterizing Circulating Tumor Cells (CTCs) from Clinical Blood Samples. PLoS ONE 2016, 11, e0147400. [Google Scholar] [CrossRef] [PubMed]
- Peng, W.K.; Chen, L.; Han, J. Development of miniaturized, portable magnetic resonance relaxometry system for point-of-care medical diagnosis. Rev. Sci. Instrum. 2012, 83, 095115. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Sun, E.; Ham, D.; Weissleder, R. Chip-NMR biosensor for detection and molecular analysis of cells. Nat. Med. 2008, 14, 869–874. [Google Scholar] [CrossRef] [PubMed]
- Chiriaco, M.S.; Primiceri, E.; De Feo, F.; Montanaro, A.; Monteduro, A.G.; Tinelli, A.; Megha, M.; Carati, D.; Maruccio, G. Simultaneous detection of multiple lower genital tract pathogens by an impedimetric immunochip. Biosens. Bioelectron. 2016, 79, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Quesada-Gonzalez, D.; Merkoci, A. Nanoparticle-based lateral flow biosensors. Biosens. Bioelectron. 2015, 73, 47–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Posthuma-Trumpie, G.A.; Korf, J.; van Amerongen, A. Lateral flow (immuno) assay: Its strengths, weaknesses, opportunities and threats. A literature survey. Anal. Bioanal. Chem. 2009, 393, 569–582. [Google Scholar] [CrossRef] [PubMed]
- Ang, S.H.; Rambeli, M.; Thevarajah, T.M.; Alias, Y.B.; Khor, S.M. Quantitative, single-step dual measurement of hemoglobin A1c and total hemoglobin in human whole blood using a gold sandwich immunochromatographic assay for personalized medicine. Biosens. Bioelectron. 2016, 78, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Jia, Q.; Yang, C.; Qiao, R.; Jing, L.; Wang, L.; Xu, C.; Gao, M. Lateral Flow Immunochromatographic Assay for Sensitive Pesticide Detection by Using Fe3O4 Nanoparticle Aggregates as Color Reagents. Anal. Chem. 2011, 83, 6778–6784. [Google Scholar] [CrossRef] [PubMed]
- Anfossi, L.; Di Nardo, F.; Giovannoli, C.; Passini, C.; Baggiani, C. Increased sensitivity of lateral flow immunoassay for ochratoxin A through silver enhancement. Anal. Bioanal. Chem. 2013, 405, 9859–9867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, H.; Chen, J.; Birrenkott, J.; Zhao, J.X.; Takalkar, S.; Baryeh, K.; Liu, G. Gold-Nanoparticle-Decorated Silica Nanorods for Sensitive Visual Detection of Proteins. Anal. Chem. 2014, 86, 7351–7359. [Google Scholar] [CrossRef] [PubMed]
- Yetisen, A.K.; Akram, M.S.; Lowe, C.R. Paper-based microfluidic point-of-care diagnostic devices. Lab Chip 2013, 13, 2210–2251. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.; Si, J.; Li, Z. Fabrication techniques for microfluidic paper-based analytical devices and their applications for biological testing: A review. Biosens. Bioelectron. 2016, 77, 774–789. [Google Scholar] [CrossRef] [PubMed]
- Rivas, L.; Medina-Sanchez, M.; de la Escosura-Muniz, A.; Merkoci, A. Improving sensitivity of gold nanoparticle-based lateral flow assays by using wax-printed pillars as delay barriers of microfluidics. Lab Chip 2014, 14, 4406–4414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sofia Fluorescent Immunoassay Analyzer. Available online: https://www.quidel.com/immunoassays/sofia-tests-kits/sofia-analyzer (accessed on 19 October 2018).
- ESEQuant Lateral Flow Reader. Available online: https://www.qiagen.com/kr/products/custom-solutions/automation/ese-instruments/esequant-lateral-flow-reader/ (accessed on 19 October 2018).
- Wang, Y.; Qin, Z.; Boulware, D.R.; Pritt, B.S.; Sloan, L.M.; González, I.J.; Bell, D.; Rees-Channer, R.R.; Chiodini, P.; Chan, W.C.W.; et al. Thermal Contrast Amplification Reader Yielding 8-Fold Analytical Improvement for Disease Detection with Lateral Flow Assays. Anal. Chem. 2016, 88, 11774–11782. [Google Scholar] [CrossRef] [PubMed]
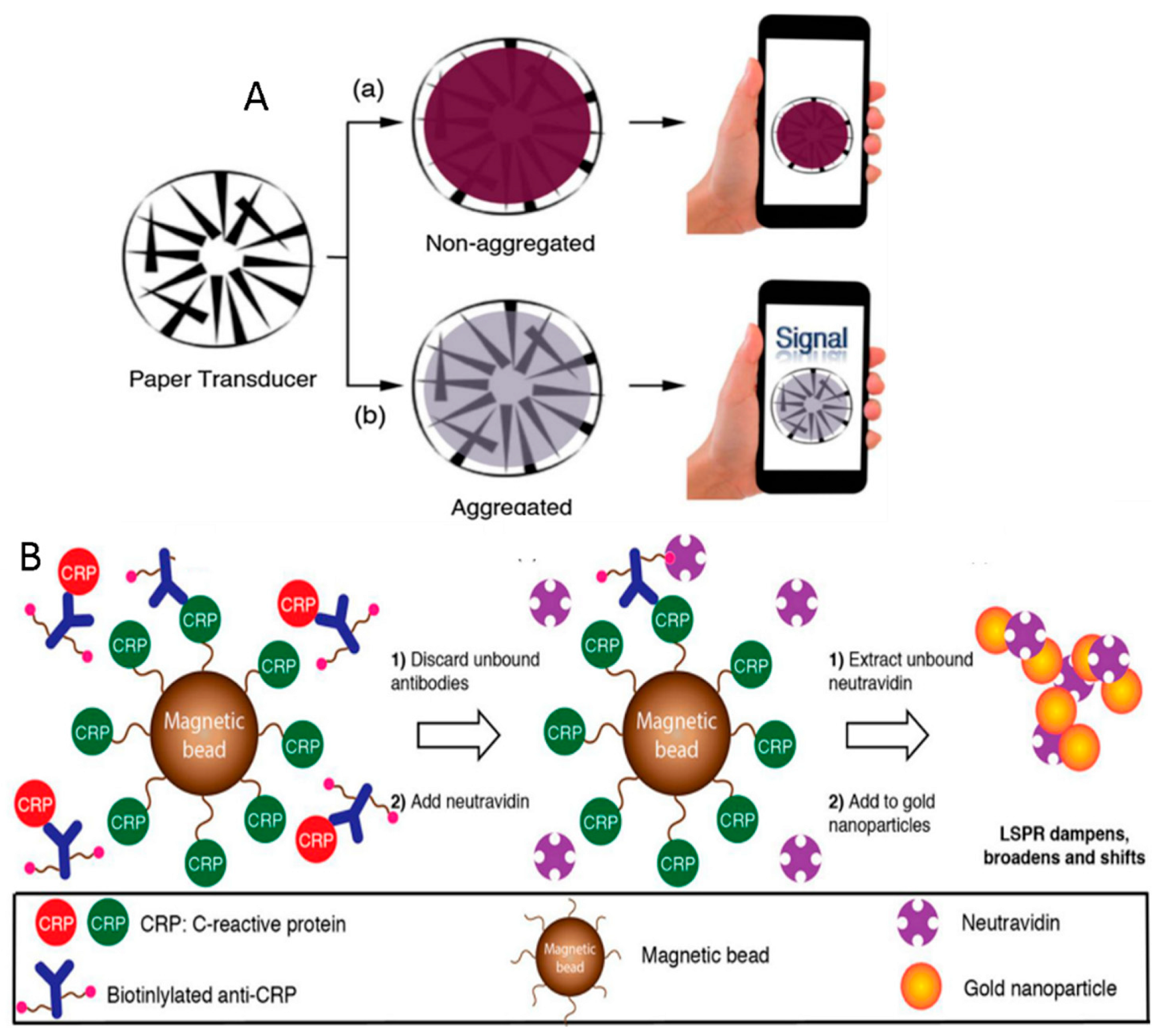
- Russell, S.M.; de la Rica, R. Paper transducers to detect plasmon variations in colorimetric nanoparticle biosensors. Sens. Actuator B-Chem. 2018, 270, 327–332. [Google Scholar] [CrossRef]
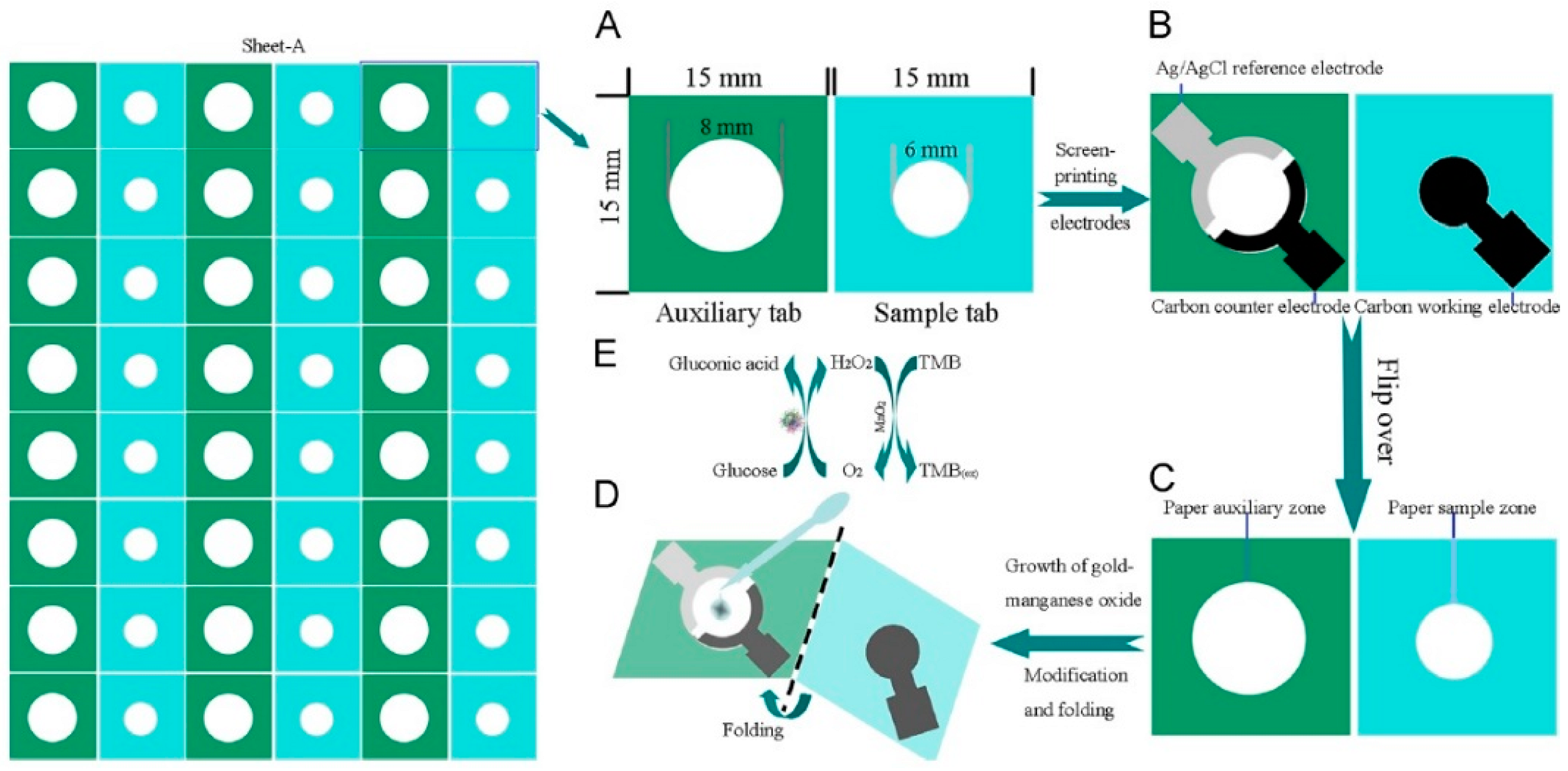
- Li, L.; Xu, J.; Zheng, X.; Ma, C.; Song, X.; Ge, S.; Yu, J.; Yan, M. Growth of gold-manganese oxide nanostructures on a 3D origami device for glucose-oxidase label based electrochemical immunosensor. Biosens. Bioelectron. 2014, 61, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Primiceri, E.; Chiriacò, M.S.; de Feo, F.; Santovito, E.; Fusco, V.; Maruccio, G. A multipurpose biochip for food pathogen detection. Anal. Methods 2016, 8, 3055–3060. [Google Scholar] [CrossRef]
- Chiriaco, M.S.; Primiceri, E.; Monteduro, A.G.; Bove, A.; Leporatti, S.; Capello, M.; Ferri-Borgogno, S.; Rinaldi, R.; Novelli, F.; Maruccio, G. Towards pancreatic cancer diagnosis using EIS biochips. Lab Chip 2013, 13, 730–734. [Google Scholar] [CrossRef] [PubMed]
- Chiriaco, M.S.; de Feo, F.; Primiceri, E.; Monteduro, A.G.; de Benedetto, G.E.; Pennetta, A.; Rinaldi, R.; Maruccio, G. Portable gliadin-immunochip for contamination control on the food production chain. Talanta 2015, 142, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Primiceri, E.; Chiriacò, M.S.; Ionescu, R.E.; D’Amone, E.; Cingolani, R.; Rinaldi, R.; Maruccio, G. Development of EIS cell chips and their application for cell analysis. Microelectron. Eng. 2009, 86, 1477–1480. [Google Scholar] [CrossRef]
- Primiceri, E.; Chiriacò, M.S.; D’Amone, E.; Urso, E.; Ionescu, R.E.; Rizzello, A.; Maffia, M.; Cingolani, R.; Rinaldi, R.; Maruccio, G. Real-time monitoring of copper ions-induced cytotoxicity by EIS cell chips. Biosens. Bioelectron. 2010, 25, 2711–2716. [Google Scholar] [CrossRef] [PubMed]
- Primiceri, E.; Chiriacò, M.S.; Dioguardi, F.; Monteduro, A.G.; D’Amone, E.; Rinaldi, R.; Giannelli, G.; Maruccio, G. Automatic transwell assay by an EIS cell chip to monitor cell migration. Lab Chip 2011, 11, 4081–4086. [Google Scholar] [CrossRef] [PubMed]
- Choi, G.; Prince, T.; Miao, J.; Cui, L.W.; Guan, W.H. Sample-to-answer palm-sized nucleic acid testing device towards low-cost malaria mass screening. Biosens. Bioelectron. 2018, 115, 83–90. [Google Scholar] [CrossRef] [PubMed]
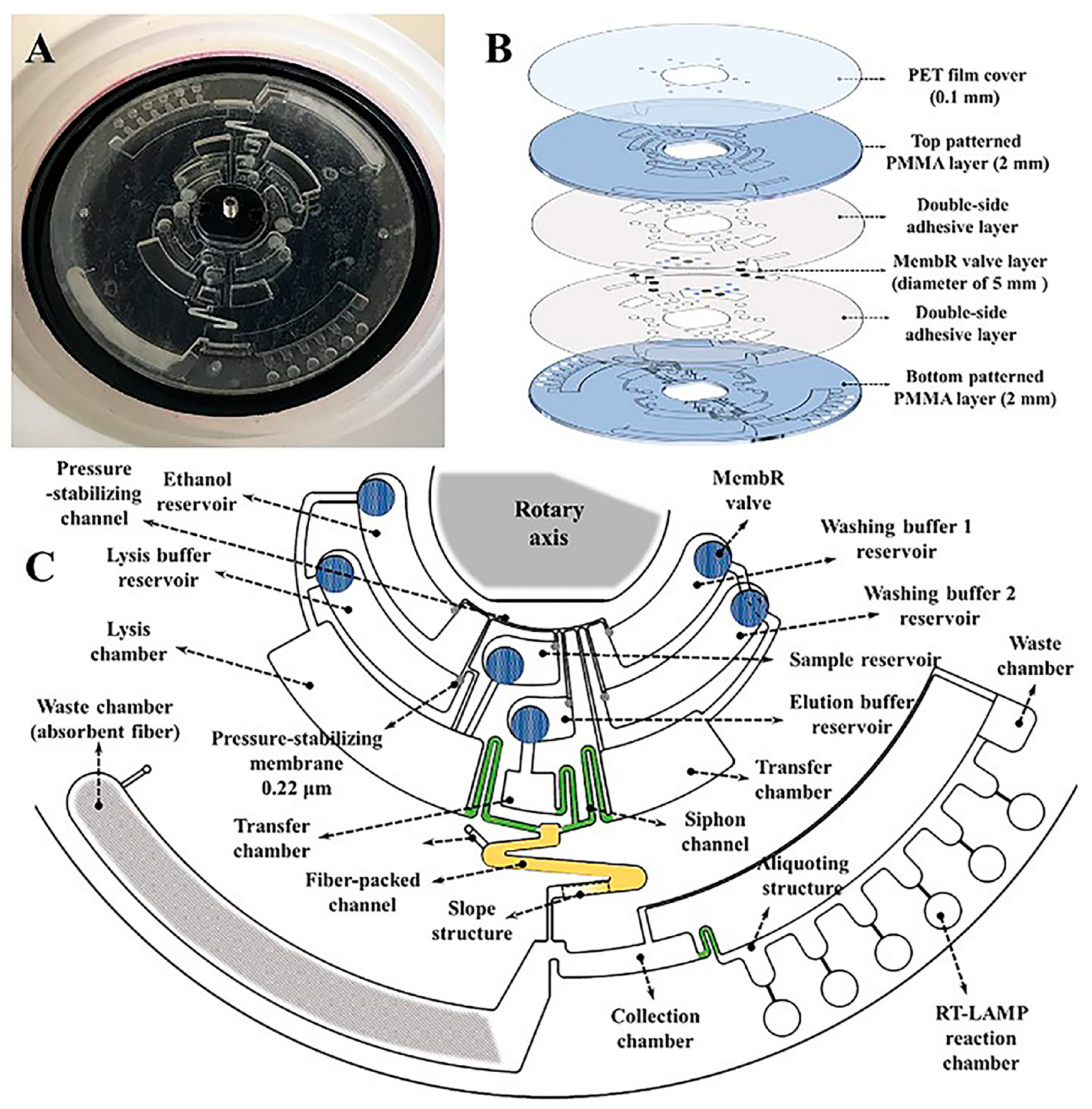
- Liu, Q.; Zhang, X.L.; Chen, L.P.; Yao, Y.H.; Ke, S.R.; Zhao, W.; Yang, Z.F.; Sui, G.D. A sample-to-answer labdisc platform integrated novel membrane-resistance valves for detection of highly pathogenic avian influenza viruses. Sens. Actuator B-Chem. 2018, 270, 371–381. [Google Scholar] [CrossRef]
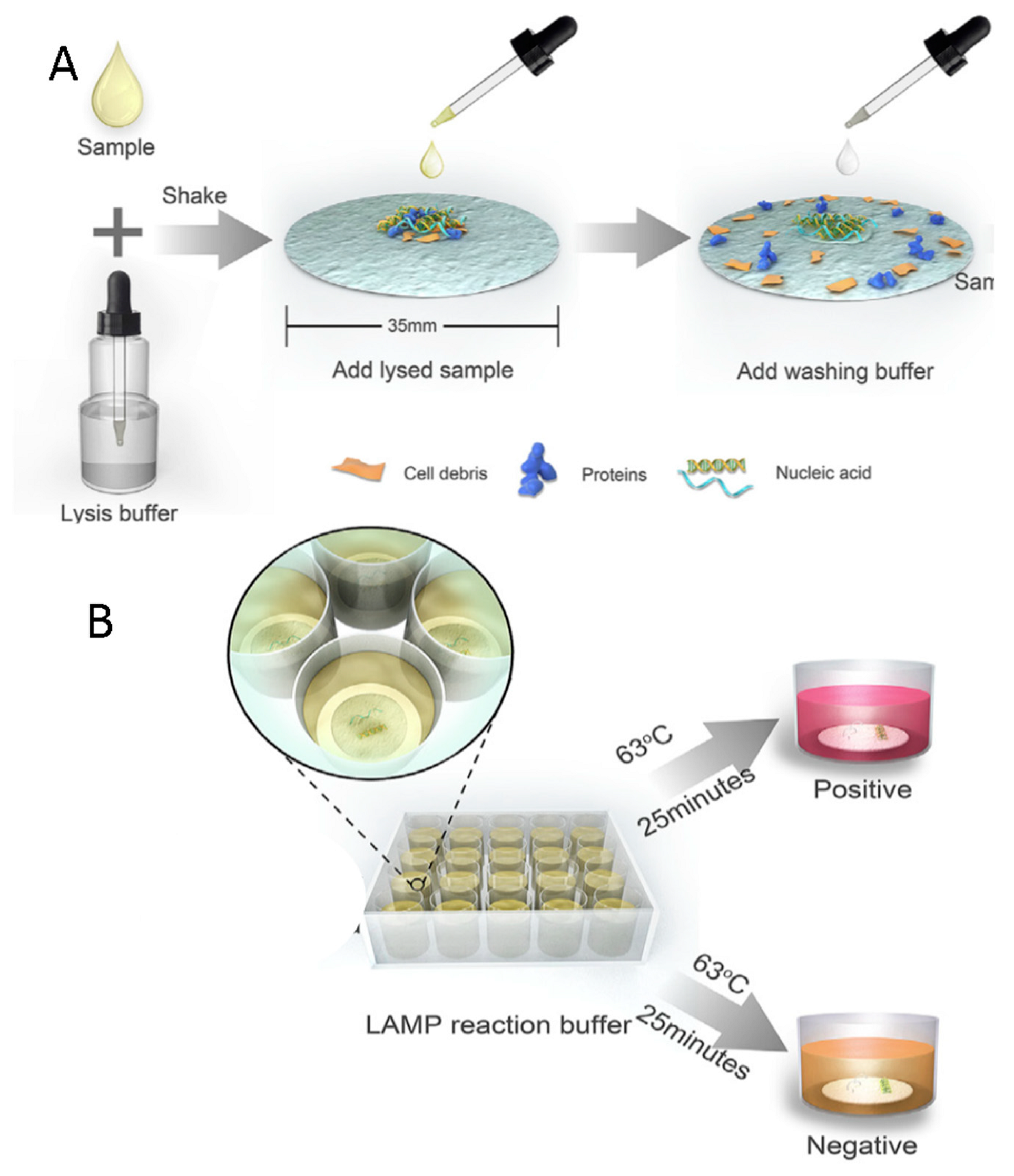
- Ye, X.; Xu, J.; Lu, L.J.; Li, X.X.; Fang, X.E.; Kong, J.L. Equipment-free nucleic acid extraction and amplification on a simple paper disc for point-of-care diagnosis of rotavirus A. Anal. Chim. Acta 2018, 1018, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Peng, F.; Zhang, Y.; Wang, R.; Zhou, W.; Zhao, Z.; Liang, H.; Qi, L.; Zhao, W.; Wang, H.; Wang, C.; et al. Identification of differentially expressed miRNAs in individual breast cancer patient and application in personalized medicine. Oncogenesis 2016, 5, e194. [Google Scholar] [CrossRef] [PubMed]
- Dehghanzadeh, R.; Jadidi-Niaragh, F.; Gharibi, T.; Yousefi, M. MicroRNA-induced drug resistance in gastric cancer. Biomed. Pharmacother. 2015, 74, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Potrich, C.; Vaghi, V.; Lunelli, L.; Pasquardini, L.; Santini, G.C.; Ottone, C.; Quaglio, M.; Cocuzza, M.; Pirri, C.F.; Ferracin, M.; et al. OncomiR detection in circulating body fluids: A PDMS microdevice perspective. Lab Chip 2014, 14, 4067–4075. [Google Scholar] [CrossRef] [PubMed]
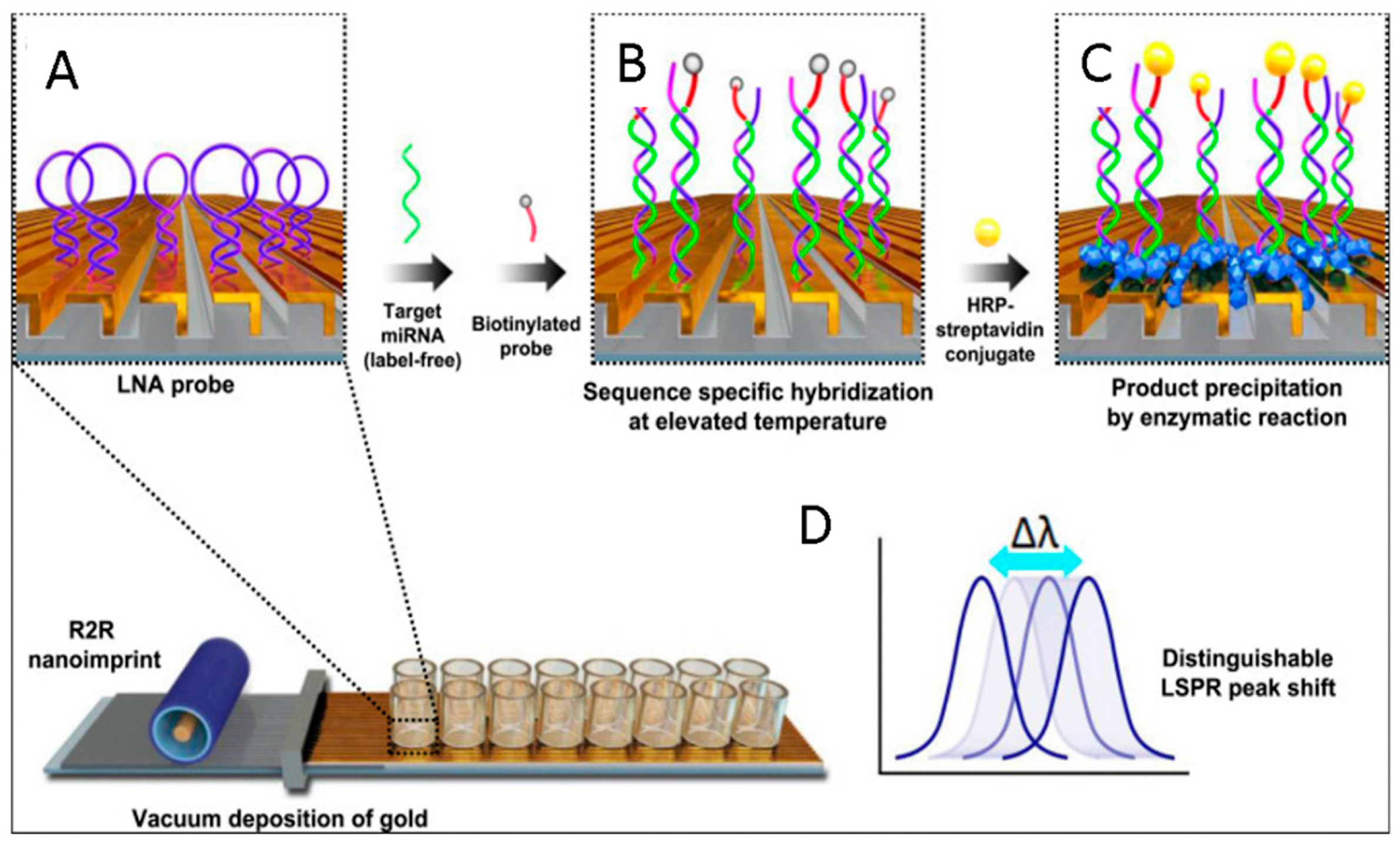
- Na, H.K.; Wi, J.S.; Son, H.Y.; Ok, J.G.; Huh, Y.M.; Lee, T.G. Discrimination of single nucleotide mismatches using a scalable, flexible, and transparent three-dimensional nanostructure-based plasmonic miRNA sensor with high sensitivity. Biosens. Bioelectron. 2018, 113, 39–45. [Google Scholar] [CrossRef] [PubMed]
- GeneXpert I. Available online: http://www.cepheid.com/us/cepheid-solutions/systems/genexpert-systems/genexpert-i (accessed on 31 August 2018).
- Hillemann, D.; Rüsch-Gerdes, S.; Boehme, C.; Richter, E. Rapid Molecular Detection of Extrapulmonary Tuberculosis by the Automated GeneXpert MTB/RIF System. J. Clin. Microbiol. 2011, 49, 1202–1205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaydos, C.A.; Van Der Pol, B.; Jett-Goheen, M.; Barnes, M.; Quinn, N.; Clark, C.; Daniel, G.E.; Dixon, P.B.; Hook, E.W. Performance of the Cepheid CT/NG Xpert Rapid PCR Test for Detection of Chlamydia trachomatis and Neisseria gonorrhoeae. J. Clin. Microbiol. 2013, 51, 1666–1672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Available online: http://www.cepheid.com/administrator/components/com_productcatalog/library-files/cb5f713dd5d8cb48dc618f0e42285d70-CEP-Corp-Overview-0320-13.pdf (accessed on 19 October 2018).
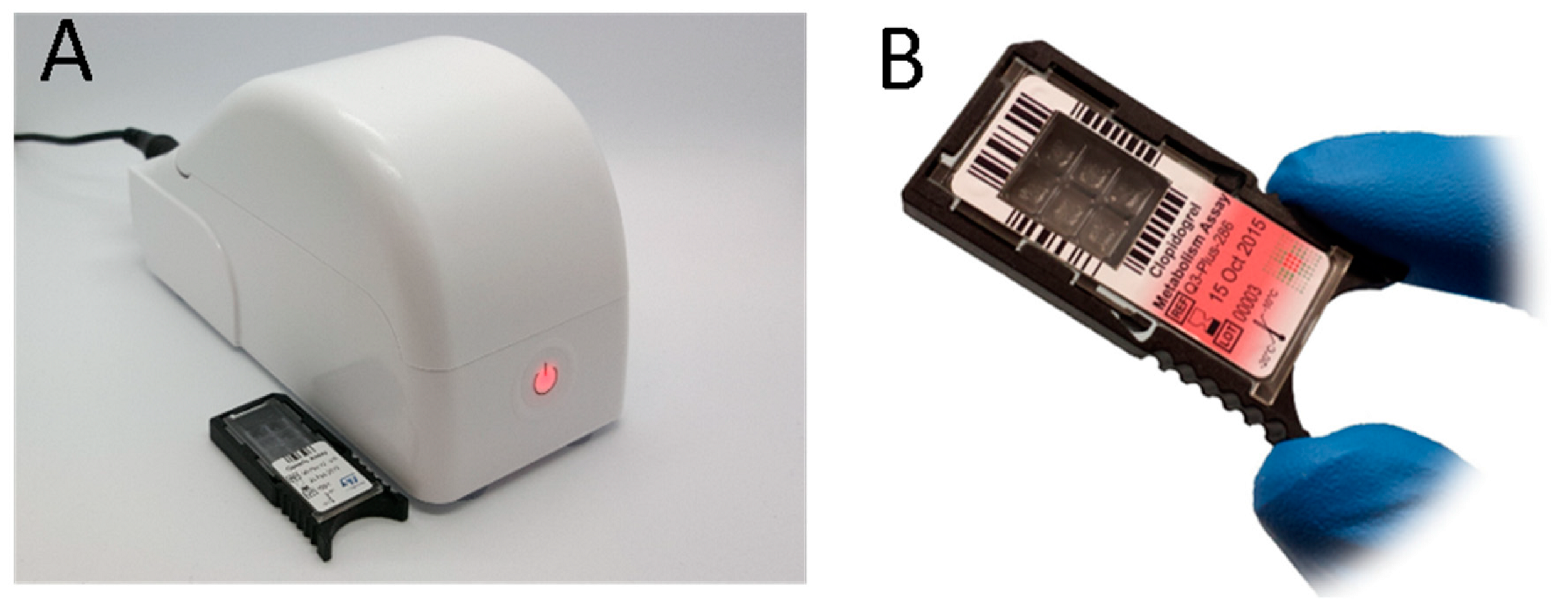
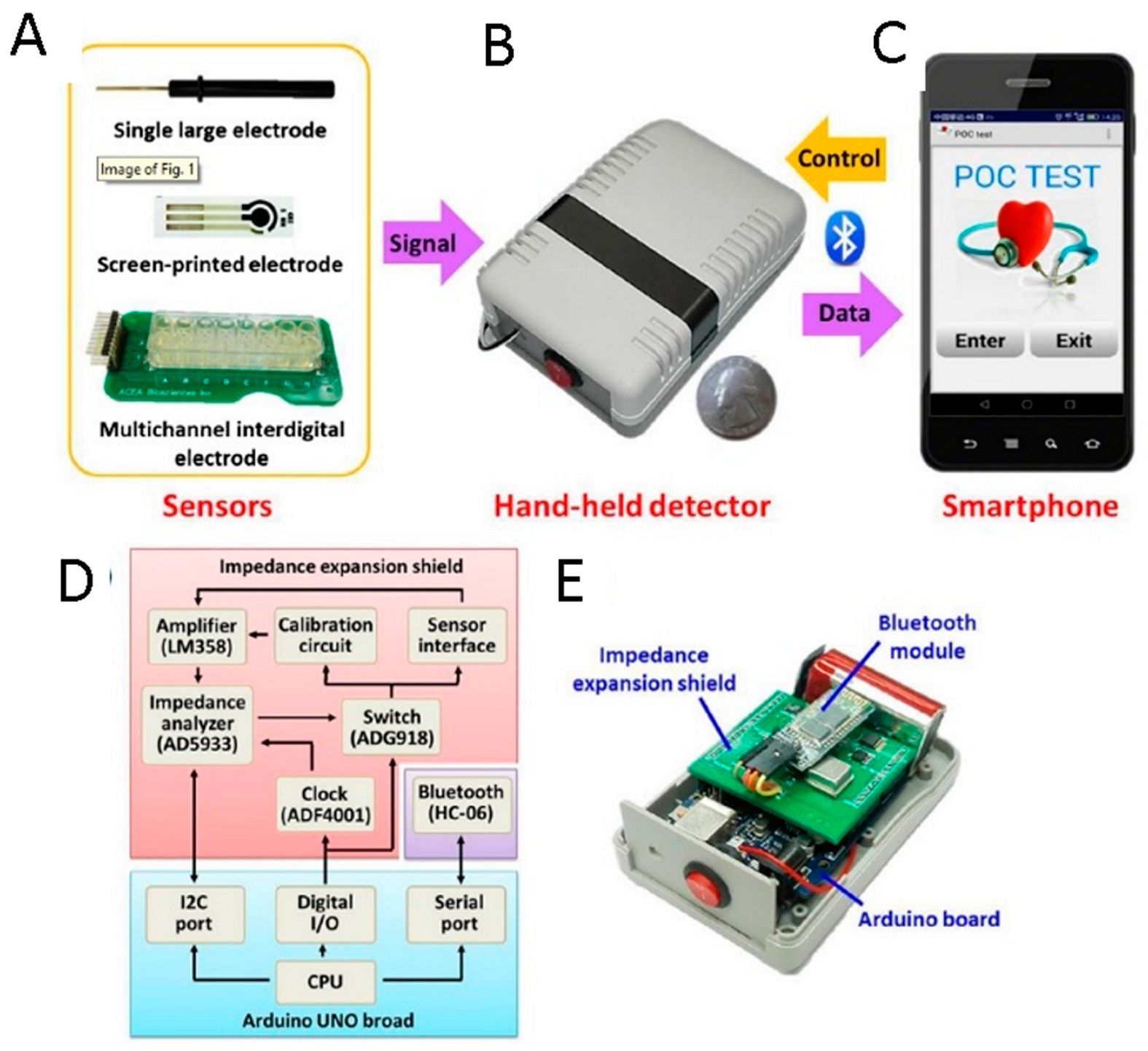
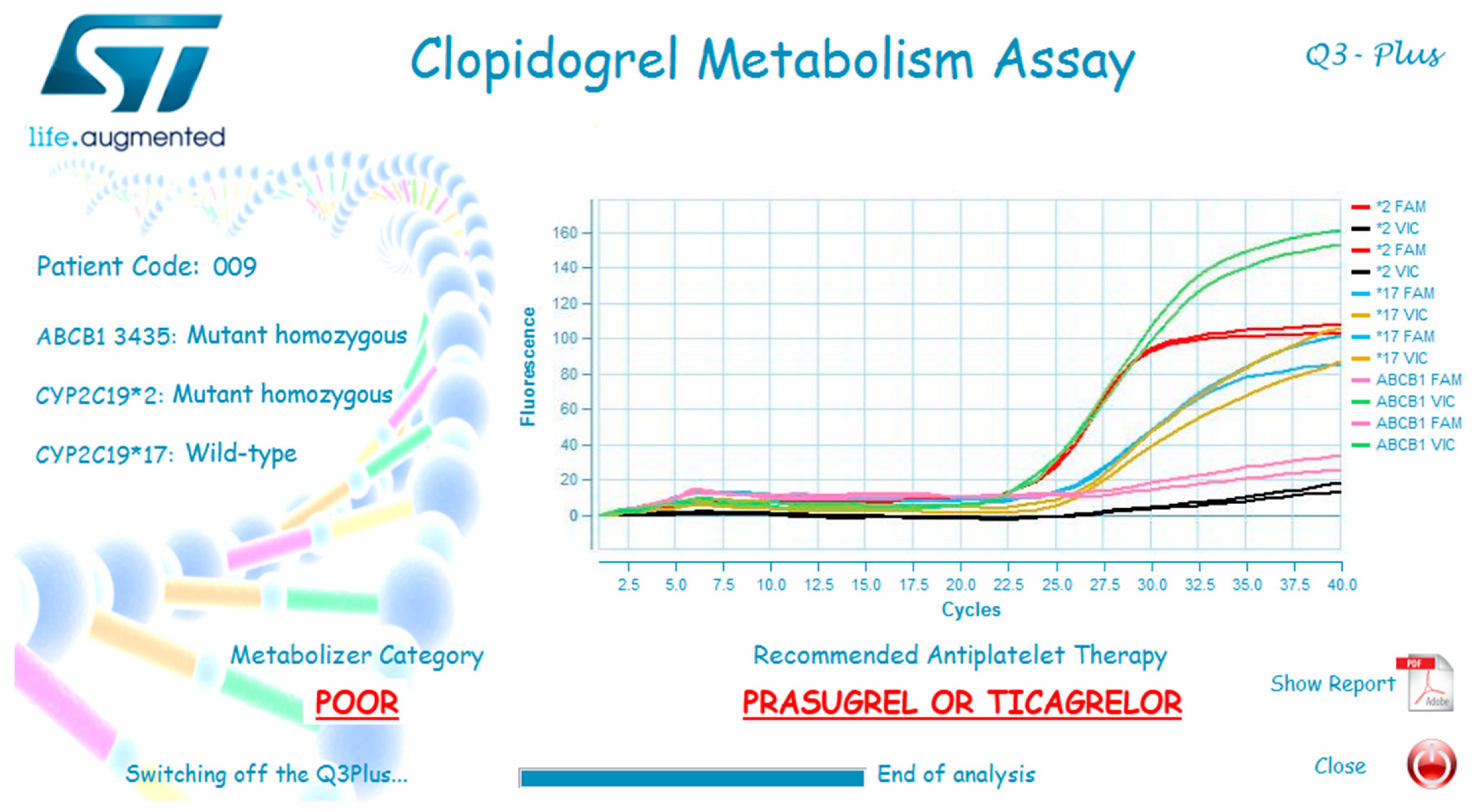
- Marziliano, N.; Notarangelo, M.F.; Cereda, M.; Caporale, V.; Coppini, L.; Demola, M.A.; Guidorossi, A.; Crocamo, A.; Pigazzani, F.; Boffetti, F.; et al. Rapid and portable, lab-on-chip, point-of-care genotyping for evaluating clopidogrel metabolism. Clin. Chim. Acta 2015, 451, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Cereda, M.; Cocci, A.; Cucchi, D.; Raia, L.; Pirola, D.; Bruno, L.; Ferrari, P.; Pavanati, V.; Calisti, G.; Ferrara, F.; et al. Q3: A Compact Device for Quick, High Precision qPCR. Sensors 2018, 18, 2583. [Google Scholar] [CrossRef] [PubMed]
- Urraca, J.L.; Castellari, M.; Barrios, C.A.; Moreno-Bondi, M.C. Multiresidue analysis of fluoroquinolone antimicrobials in chicken meat by molecularly imprinted solid-phase extraction and high performance liquid chromatography. J. Chromatogr. A 2014, 1343, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Alvarez, M.; Mazzotta, E.; Malitesta, C.; Martin-Esteban, A. Evaluation of electrochemically synthesized sulfadimethoxine-imprinted polymer for solidphase microextraction of sulfonamides. J. Mol. Recogn. 2014, 27, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Haupt, K.; Mosbach, K. Plastic antibodies: Developments and applications. Trends Biotechnol. 1998, 16, 468–475. [Google Scholar] [CrossRef]
- Mazzotta, E.; Turco, A.; Chianella, I.; Guerreiro, A.; Piletsky, S.A.; Malitesta, C. Solid-phase synthesis of electroactive nanoparticles of molecularly imprinted polymers. A novel platform for indirect electrochemical sensing applications. Sens. Actuator B-Chem. 2016, 229, 174–180. [Google Scholar] [CrossRef]
- Haupt, K. Imprinted polymers—Tailor-made mimics of antibodies and receptors. Chem. Commun. 2003, 2, 171–178. [Google Scholar] [CrossRef]
- Chen, Y.; Chen, L.; Bi, R.; Xu, L.; Liu, Y. A potentiometric chiral sensor for L-Phenylalanine based on crosslinked polymethylacrylic acid-polycarbazole hybrid molecularly imprinted polymer. Anal. Chim. Acta 2012, 754, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Vasapollo, G.; Del Sole, R.; Mergola, L.; Lazzoi, M.R.; Scardino, A.; Scorrano, S.; Mele, G. Molecularly Imprinted Polymers: Present and Future Prospective. Int. J. Mol. Sci. 2011, 12, 5908–5945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reimhult, K.; Yoshimatsu, K.; Risveden, K.; Chen, S.; Ye, L.; Krozer, A. Characterization of QCM sensor surfaces coated with molecularly imprinted nanoparticles. Biosens. Bioelectron. 2008, 23, 1908–1914. [Google Scholar] [CrossRef] [PubMed]
- Yaqub, S.; Latif, U.; Dickert, F.L. Plastic antibodies as chemical sensor material for atrazine detection. Sens. Actuator B-Chem. 2011, 160, 227–233. [Google Scholar] [CrossRef]
- Wojnarowicz, A.; Sharma, P.S.; Sosnowska, M.; Lisowski, W.; Huynh, T.-P.; Pszona, M.; Borowicz, P.; D’Souza, F.; Kutner, W. An electropolymerized molecularly imprinted polymer for selective carnosine sensing with impedimetric capacity. J. Mater. Chem. B 2016, 4, 1156–1165. [Google Scholar] [CrossRef] [Green Version]
- Gutierrez-Climente, R.; Gomez-Caballero, A.; Halhalli, M.; Sellergren, B.; Aranzazu Goicolea, M.; Barrio, R.J. Iniferter-mediated grafting of molecularly imprinted polymers on porous silica beads for the enantiomeric resolution of drugs. J. Mol. Recogn. 2016, 29, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Moreira, F.T.C.; Sharma, S.; Dutra, R.A.F.; Noronha, J.P.C.; Cass, A.E.G.; Sales, M.G.F. Detection of cardiac biomarker proteins using a disposable based on a molecularly imprinted polymer grafted onto graphite. Microchim. Acta 2015, 182, 975–983. [Google Scholar] [CrossRef]
- Karimian, N.; Vagin, M.; Zavar, M.H.A.; Chamsaz, M.; Turner, A.P.F.; Tiwari, A. An ultrasensitive molecularly-imprinted human cardiac troponin sensor. Biosens. Bioelectron. 2013, 50, 492–498. [Google Scholar] [CrossRef] [PubMed]
- El-Din, E.M.R.S.; El-Sokkary, M.M.A.; Bassiouny, M.R.; Hassan, R. Epidemiology of Neonatal Sepsis and Implicated Pathogens: A Study from Egypt. Biomed. Res. Int. 2015, 2015, 509484. [Google Scholar]
- Roger, T.; Schneider, A.; Weier, M.; Sweep, F.C.G.J.; Le Roy, D.; Bernhagend, J.; Calandra, T.; Giannoni, E. High expression levels of macrophage migration inhibitory factor sustain the innate immune responses of neonates. Proc. Natl. Acad. Sci. USA 2016, 113, E997–E1005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchegger, P.; Lieberzeit, P.A.; Preininger, C. Thermo-Nanoimprinted Biomimetic Probe for LPS and LTA Immunosensing. Anal. Chem. 2014, 86, 1679–1686. [Google Scholar] [CrossRef] [PubMed]
- Sener, G.; Ozgur, E.; Rad, A.Y.; Uzun, L.; Say, R.; Denizli, A. Rapid real-time detection of procalcitonin using a microcontact imprinted surface plasmon resonance biosensor. Analyst 2013, 138, 6422–6428. [Google Scholar] [CrossRef] [PubMed]
- Ge, L.; Wang, S.; Yu, J.; Li, N.; Ge, S.; Yan, M. Molecularly Imprinted Polymer Grafted Porous Au-Paper Electrode for an Microfluidic Electro-Analytical Origami Device. Adv. Funct. Mater. 2013, 23, 3115–3123. [Google Scholar] [CrossRef]
- Jiang, H.; Jiang, D.; Shao, J.; Sun, X. Magnetic molecularly imprinted polymer nanoparticles based electrochemical sensor for the measurement of Gram-negative bacterial quorum signaling molecules (N-acyl-homoserine-lactones). Biosens. Bioelectron. 2016, 75, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Chen, M.; Zhang, H.; Wen, W.; Zhang, X.; Wang, S. Enhanced electrochemiluminescence of RuSi nanoparticles for ultrasensitive detection of ochratoxin A by energy transfer with CdTe quantum dots. Biosens. Bioelectron. 2016, 79, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Liu, L.; He, Y.; He, Q.; Ma, H. Quantum-dots-encoded-microbeads based molecularly imprinted polymer. Biosens. Bioelectron. 2016, 77, 886–893. [Google Scholar] [CrossRef] [PubMed]
- Tretjakov, A.; Syritski, V.; Reut, J.; Boroznjak, R.; Oepik, A. Molecularly imprinted polymer film interfaced with Surface Acoustic Wave technology as a sensing platform for label-free protein detection. Anal. Chim. Acta 2016, 902, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Afzal, A.; Iqbal, N.; Mujahid, A.; Schirhagl, R. Advanced vapor recognition materials for selective and fast responsive surface acoustic wave sensors: A review. Anal. Chim. Acta 2013, 787, 36–49. [Google Scholar] [CrossRef] [PubMed]
- Maouche, N.; Ktari, N.; Bakas, I.; Fourati, N.; Zerrouki, C.; Seydou, M.; Maurel, F.; Chehimi, M.M. A surface acoustic wave sensor functionalized with a polypyrrole molecularly imprinted polymer for selective dopamine detection. J. Mol. Recogn. 2015, 28, 667–678. [Google Scholar] [CrossRef] [PubMed]
- Levite, M. Dopamine and T cells: Dopamine receptors and potent effects on T cells, dopamine production in T cells, and abnormalities in the dopaminergic system in T cells in autoimmune, neurological and psychiatric diseases. Acta Physiol. 2016, 216, 42–89. [Google Scholar] [CrossRef] [PubMed]
- Rapid Point of Care Molecular Diagnostic Test for Ebola Virus. Available online: http://www.lucigen.com/docs/posters/ASM-Biodefense-2015-ebola.pdf (accessed on 24 October 2018).
- Cheung, T.K.W.; Chin, A.W.H.; Chan, K.H.; Schumaker, M.; Mak, P.W.Y.; Leung, H.S.Y.; Wong, A.; Peiris, J.S.M.; Petrauskene, O.V.; Poon, L.L.M. Evaluation of novel H1N1-specific primer-probe sets using commercial RT-PCR mixtures and a premixed reaction stored in a lyophilized format. J. Virol. Methods 2010, 165, 302–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishioka, R.; Satomura, A.; Yamada, J.; Kuroda, K.; Ueda, M. Rapid preparation of mutated influenza hemagglutinins for influenza virus pandemic prevention. AMB Express 2016, 6, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Y.; Hogberg, J.; Christine, T.; Florian, L.; Monsalve, L.G.; Rodriguez, S.; Cao, C.; Wolff, A.; Ruano-Lopez, J.M.; Bang, D.D. Pre-storage of gelified reagents in a lab-on-a-foil system for rapid nucleic acid analysis. Lab Chip 2013, 13, 1509–1514. [Google Scholar] [CrossRef] [PubMed]
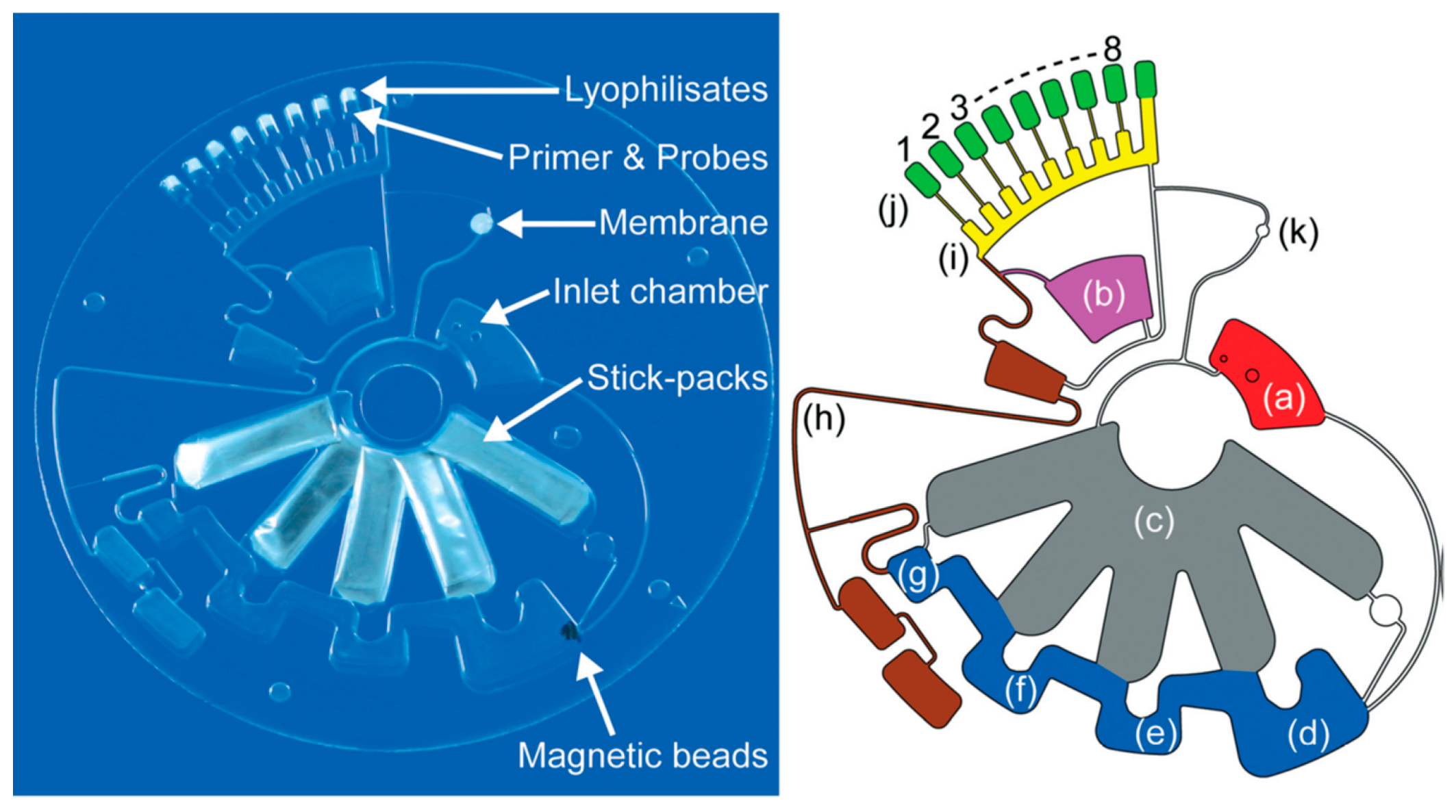
- Stumpf, F.; Schwemmer, F.; Hutzenlaub, T.; Baumann, D.; Strohmeier, O.; Dingemanns, G.; Simons, G.; Sager, C.; Plobner, L.; von Stetten, F.; et al. LabDisk with complete reagent prestorage for sample-to-answer nucleic acid based detection of respiratory pathogens verified with influenza A H3N2 virus. Lab Chip 2016, 16, 199–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, E.M. Hydrogel: Preparation, characterization, and applications: A review. J. Adv. Res. 2015, 6, 105–121. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.K.; Dong, L.; Beebe, D.J.; Jiang, H. Autonomously-triggered microfluidic cooling using thermo-responsive hydrogels. Lab Chip 2007, 7, 310–315. [Google Scholar] [CrossRef] [PubMed]
- Niedl, R.R.; Beta, C. Hydrogel-driven paper-based microfluidics. Lab Chip 2015, 15, 2452–2459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, X.; Tian, T.; Jia, S.; Zhu, Z.; Ma, Y.; Sun, J.; Lin, Z.; Yang, C.J. Target-Responsive DNA Hydrogel Mediated “Stop-Flow” Microfluidic Paper-Based Analytic Device for Rapid, Portable and Visual Detection of Multiple Targets. Anal. Chem. 2015, 87, 4275–4282. [Google Scholar] [CrossRef] [PubMed]
- Karfa, P.; Roy, E.; Patra, S.; Kumar, D.; Madhuri, R.; Sharma, P.K. A fluorescent molecularly-imprinted polymer gate with temperature and pH as inputs for detection of alpha-fetoprotein. Biosens. Bioelectron. 2016, 78, 454–463. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.Y.; Ding, W.X.; Wang, X.M.; Cao, R.F.; Zhang, M.Y.; Lv, P.L.; Xu, F. Smartphone-Based Accurate Analysis of Retinal Vasculature towards Point-of-Care Diagnostics. Sci. Rep. 2016, 6, 9. [Google Scholar] [CrossRef] [PubMed]
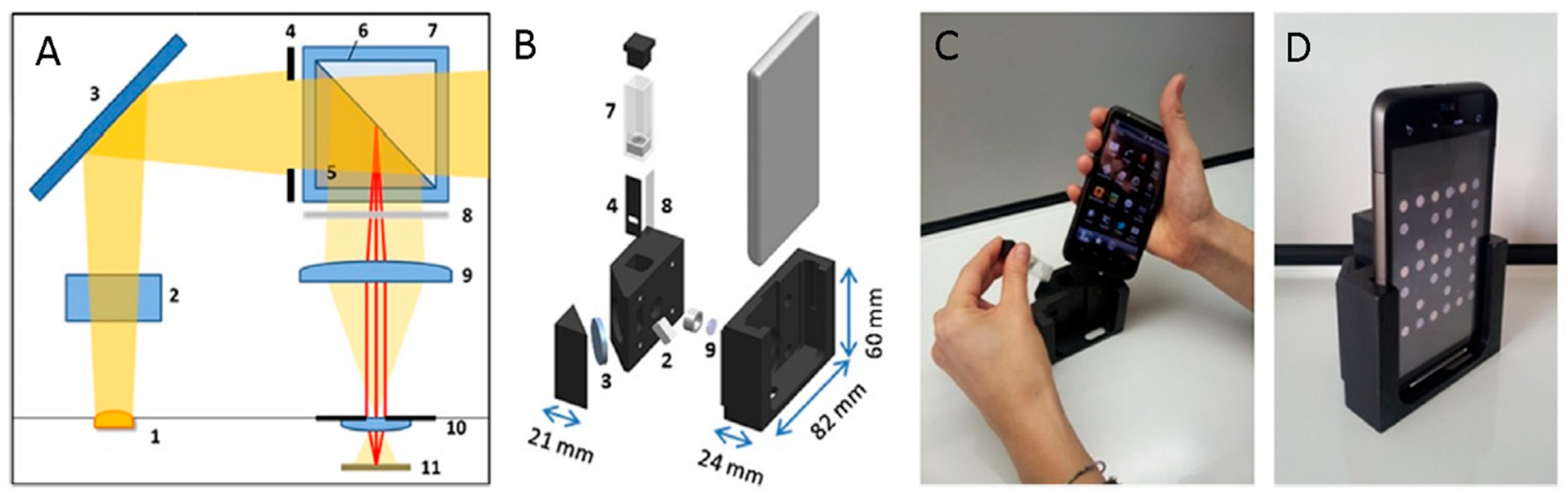
- Giavazzi, F.; Salina, M.; Ceccarello, E.; Ilacqua, A.; Damin, F.; Sola, L.; Chiari, M.; Chini, B.; Cerbino, R.; Bellini, T.; et al. A fast and simple label-free immunoassay based on a smartphone. Biosens. Bioelectron. 2014, 58, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Liu, Q.; Chen, S.; Cheng, F.; Wang, H.; Peng, W. Surface Plasmon Resonance Biosensor Based on Smart Phone Platforms. Sci. Rep. 2015, 5, 12864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanakasabapathy, M.K.; Sadasivam, M.; Singh, A.; Preston, C.; Thirumalaraju, P.; Venkataraman, M.; Bormann, C.L.; Draz, M.S.; Petrozza, J.C.; Shafiee, H. An automated smartphone-based diagnostic assay for point-of-care semen analysis. Sci. Transl. Med. 2017, 9, 13. [Google Scholar] [CrossRef] [PubMed]
- Lillehoj, P.B.; Huang, M.-C.; Truong, N.; Ho, C.-M. Rapid electrochemical detection on a mobile phone. Lab Chip 2013, 13, 2950–2955. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Lu, Y.; Zhang, Q.; Liu, L.; Li, S.; Yao, Y.; Jiang, J.; Liu, G.L.; Liu, Q. Protein detecting with smartphone-controlled electrochemical impedance spectroscopy for point-of-care applications. Sens. Actuator B-Chem. 2016, 222, 994–1002. [Google Scholar] [CrossRef]
- Mega, J.L.; Close, S.L.; Wiviott, S.D.; Shen, L.; Walker, J.R.; Simon, T.; Antman, E.M.; Braunwald, E.; Sabatine, M.S. Genetic variants in ABCB1 and CYP2C19 and cardiovascular outcomes after treatment with clopidogrel and prasugrel in the TRITON-TIMI 38 trial: A pharmacogenetic analysis. Lancet 2010, 376, 1312–1319. [Google Scholar] [CrossRef]
- Chan, N.C.; Eikelboom, J.W.; Ginsberg, J.S.; Lauw, M.N.; Vanassche, T.; Weitz, J.I.; Hirsh, J. Role of phenotypic and genetic testing in managing clopidogrel therapy. Blood 2014, 124, 689–699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Notarangelo, F.M.; Maglietta, G.; Bevilacqua, P.; Cereda, M.; Merlini, P.A.; Villani, G.Q.; Moruzzi, P.; Patrizi, G.; Malagoli Tagliazucchi, G.; Crocamo, A.; et al. Pharmacogenomic Approach to Selecting Antiplatelet Therapy in Patients with Acute Coronary Syndromes: The PHARMCLO Trial. J. Am. Coll. Cardiol. 2018, 71, 1869–1877. [Google Scholar] [CrossRef] [PubMed]
- Molecular Diagnostics Market by Application (Infectious Disease (Hepatitis, HIV), Oncology, Genetic Testing), Technology (PCR, DNA Sequencing & NGS), End User (Hospital/Academic Laboratory), Product & Service (Reagent, Software)—Global Forecast to 2023. Available online: https://www.marketsandmarkets.com/Market-Reports/molecular-diagnostic-market-833.html (accessed on 10 July 2018).
- Molecular Diagnostics Market Size, Share & Trend Analysis Report by Technology (PCR, ISH, INNAT, Chips & Microarrays, Mass spectrometry, Sequencing, TMA), and Segment Forecasts, 2018–2024. Available online: https://www.grandviewresearch.com/industry-analysis/molecular-diagnostics-market (accessed on 11 July 2018).
- Stratistics Market Research Consulting Web Page. Lab-on-a-Chip—Global Market Outlook (2016–2022). Available online: http://www.strategymrc.com/report/lab-on-a-chip-market (accessed on 11 July 2018).
- Park, J.; Kim, J.; Kim, S.-Y.; Cheong, W.H.; Jang, J.; Park, Y.-G.; Na, K.; Kim, Y.-T.; Heo, J.H.; Lee, C.Y.; et al. Soft, smart contact lenses with integrations of wireless circuits, glucose sensors, and displays. Sci. Adv. 2018, 4, eaap9841. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Qiu, Y.; Ameri, S.K.; Jang, H.; Dai, Z.; Huang, Y.; Lu, N. Low-cost, μm-thick, tape-free electronic tattoo sensors with minimized motion and sweat artifacts. NPJ Flex. Electr. 2018, 2, 6. [Google Scholar] [CrossRef]
















© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Primiceri, E.; Chiriacò, M.S.; Notarangelo, F.M.; Crocamo, A.; Ardissino, D.; Cereda, M.; Bramanti, A.P.; Bianchessi, M.A.; Giannelli, G.; Maruccio, G. Key Enabling Technologies for Point-of-Care Diagnostics. Sensors 2018, 18, 3607. https://0-doi-org.brum.beds.ac.uk/10.3390/s18113607
Primiceri E, Chiriacò MS, Notarangelo FM, Crocamo A, Ardissino D, Cereda M, Bramanti AP, Bianchessi MA, Giannelli G, Maruccio G. Key Enabling Technologies for Point-of-Care Diagnostics. Sensors. 2018; 18(11):3607. https://0-doi-org.brum.beds.ac.uk/10.3390/s18113607
Chicago/Turabian StylePrimiceri, Elisabetta, Maria Serena Chiriacò, Francesca M. Notarangelo, Antonio Crocamo, Diego Ardissino, Marco Cereda, Alessandro P. Bramanti, Marco A. Bianchessi, Gianluigi Giannelli, and Giuseppe Maruccio. 2018. "Key Enabling Technologies for Point-of-Care Diagnostics" Sensors 18, no. 11: 3607. https://0-doi-org.brum.beds.ac.uk/10.3390/s18113607