Inertial Measurement Unit Based Upper Extremity Motion Characterization for Action Research Arm Test and Activities of Daily Living

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
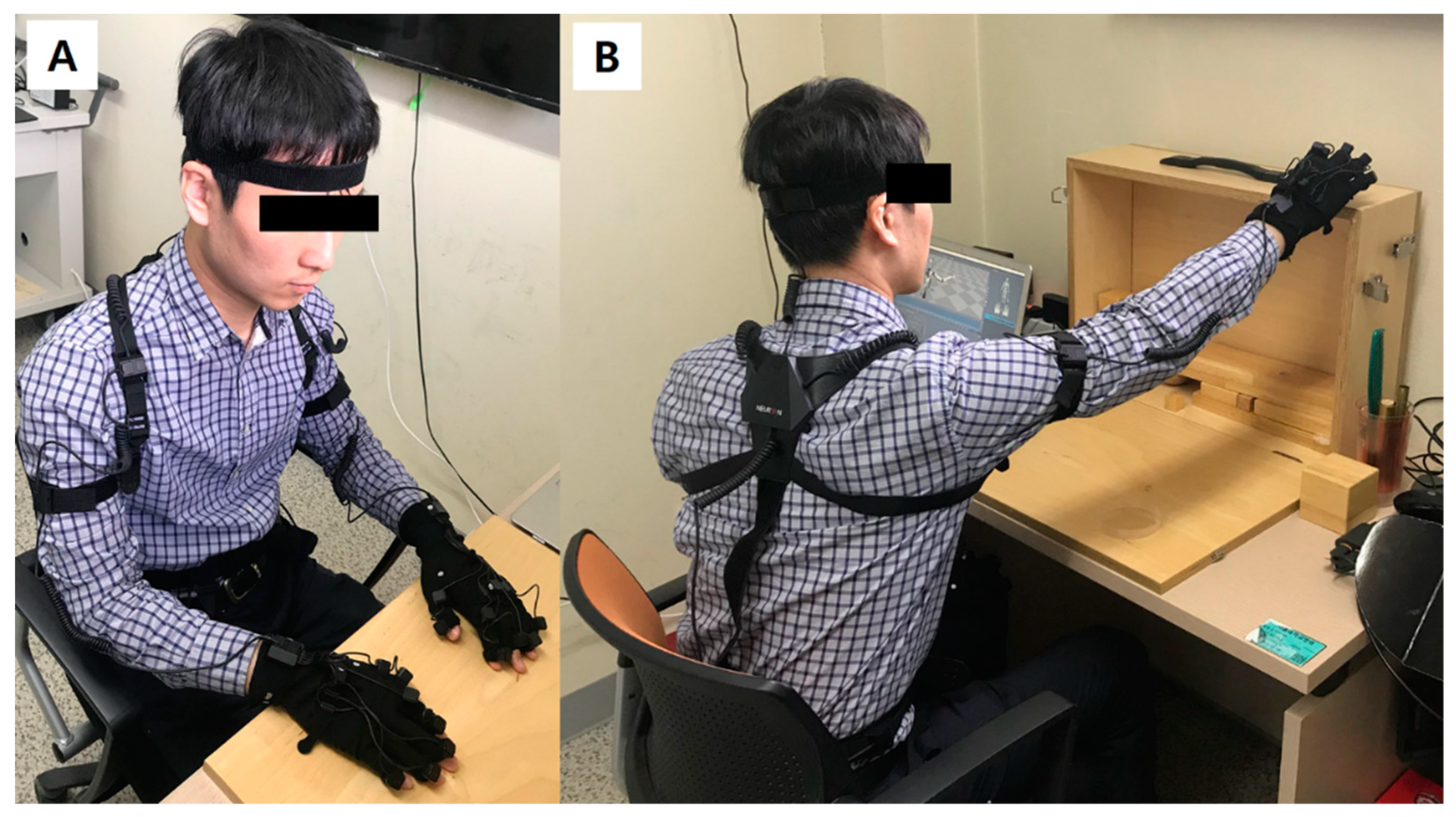
2.1. Upper Extremity Motion Capture System and Its Validation
2.2. Participants
2.3. Tasks and Procedure
2.4. Extracted Parameters
2.5. Statistical Analysis
3. Results
3.1. Validation of Upper Extremity Motion Capture System
3.2. Workspace and RoM in Basic Upper Extremity Movements
3.3. Characteristics of Grasping/Pinching and Reaching
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Declaration
Conflicts of Interest
References
- Bertani, R.; Melegari, C.; De Cola, M.C.; Bramanti, A.; Bramanti, P.; Calabro, R.S. Effects of robot-assisted upper limb rehabilitation in stroke patients: A systematic review with meta-analysis. Neurol. Sci. 2017, 38, 1561–1569. [Google Scholar] [CrossRef]
- Mehrholz, J.; Pohl, M.; Platz, T.; Kugler, J.; Elsner, B. Electromechanical and robot-assisted arm training for improving activities of daily living, arm function, and arm muscle strength after stroke. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, Y.; Kang, S.H.; Park, H.S.; Wu, Y.N.; Zhang, L.Q. Developing a multi-joint upper limb exoskeleton robot for diagnosis, therapy, and outcome evaluation in neurorehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 21, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Klamroth-Marganska, V.; Blanco, J.; Campen, K.; Curt, A.; Dietz, V.; Ettlin, T.; Felder, M.; Fellinghauer, B.; Guidali, M.; Kollmar, A.; et al. Three-dimensional, task-specific robot therapy of the arm after stroke: A multicentre, parallel-group randomised trial. Lancet Neurol. 2014, 13, 159–166. [Google Scholar] [CrossRef]
- Fasoli, S.E.; Krebs, H.I.; Stein, J.; Frontera, W.R.; Hogan, N. Effects of robotic therapy on motor impairment and recovery in chronic stroke. Arch. Phys. Med. Rehabil. 2003, 84, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Lo, H.S.; Xie, S.Q. Exoskeleton robots for upper-limb rehabilitation: State of the art and future prospects. Med. Eng. Phys. 2012, 34, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Valero-Cuevas, F.J.; Santello, M. On neuromechanical approaches for the study of biological and robotic grasp and manipulation. J. Neuroeng Rehabil. 2017, 14, 101. [Google Scholar] [CrossRef]
- Aizawa, J.; Masuda, T.; Koyama, T.; Nakamaru, K.; Isozaki, K.; Okawa, A.; Morita, S. Three-dimensional motion of the upper extremity joints during various activities of daily living. J. Biomech. 2010, 43, 2915–2922. [Google Scholar] [CrossRef]
- Gates, D.H.; Walters, L.S.; Cowley, J.; Wilken, J.M.; Resnik, L. Range of Motion Requirements for Upper-Limb Activities of Daily Living. Am. J. Occup. Ther. 2016, 70, 7001350010p1–7001350010p10. [Google Scholar] [CrossRef]
- Kim, K.; Song, W.K.; Lee, J.; Lee, H.Y.; Park, D.S.; Ko, B.W.; Kim, J. Kinematic analysis of upper extremity movement during drinking in hemiplegic subjects. Clin. Biomech. (Bristol, Avon) 2014, 29, 248–256. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Lum, P.S. Pilot testing of the spring operated wearable enhancer for arm rehabilitation (SpringWear). J. Neuroeng Rehabil. 2018, 15, 13. [Google Scholar] [CrossRef] [PubMed]
- Perez, R.; Costa, U.; Torrent, M.; Solana, J.; Opisso, E.; Caceres, C.; Tormos, J.M.; Medina, J.; Gomez, E.J. Upper limb portable motion analysis system based on inertial technology for neurorehabilitation purposes. Sensors 2010, 10, 10733–10751. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Markopoulos, P.; Yu, B.; Chen, W.; Timmermans, A. Interactive wearable systems for upper body rehabilitation: A systematic review. J. Neuroeng Rehabil. 2017, 14, 20. [Google Scholar] [CrossRef] [PubMed]
- Lyle, R.C. A performance test for assessment of upper limb function in physical rehabilitation treatment and research. Int. J. Rehabil. Res. 1981, 4, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Nam, H.S.; Seo, H.G.; Leigh, J.H.; Kim, Y.J.; Kim, S.; Bang, M.S. External Robotic Arm vs Upper Limb Exoskeleton: What Do the Potential Users Need? Unpublished.
- Hsieh, C.L.; Hsueh, I.P.; Chiang, F.M.; Lin, P.H. Inter-rater reliability and validity of the action research arm test in stroke patients. Age Ageing 1998, 27, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Koh, C.L.; Hsueh, I.P.; Wang, W.C.; Sheu, C.F.; Yu, T.Y.; Wang, C.H.; Hsieh, C.L. Validation of the action research arm test using item response theory in patients after stroke. J. Rehabil. Med. 2006, 38, 375–380. [Google Scholar] [CrossRef]
- Chen, H.F.; Lin, K.C.; Wu, C.Y.; Chen, C.L. Rasch validation and predictive validity of the action research arm test in patients receiving stroke rehabilitation. Arch. Phys. Med. Rehabil. 2012, 93, 1039–1045. [Google Scholar] [CrossRef]
- Yozbatiran, N.; Der-Yeghiaian, L.; Cramer, S.C. A standardized approach to performing the action research arm test. Neurorehabil. Neural Repair 2008, 22, 78–90. [Google Scholar] [CrossRef]
- Parker, V.M.; Wade, D.T.; Langton Hewer, R. Loss of arm function after stroke: Measurement, frequency, and recovery. Int. Rehabil. Med. 1986, 8, 69–73. [Google Scholar] [CrossRef]
- Van Andel, C.J.; Wolterbeek, N.; Doorenbosch, C.A.; Veeger, D.H.; Harlaar, J. Complete 3D kinematics of upper extremity functional tasks. Gait Posture 2008, 27, 120–127. [Google Scholar] [CrossRef]
- Krakauer, J.W. Arm function after stroke: From physiology to recovery. Semin. Neurol. 2005, 25, 384–395. [Google Scholar] [CrossRef] [PubMed]
- Shelton, F.N.; Reding, M.J. Effect of lesion location on upper limb motor recovery after stroke. Stroke 2001, 32, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Brunnstrom, S. Motor testing procedures in hemiplegia: Based on sequential recovery stages. Phys. Ther. 1966, 46, 357–375. [Google Scholar] [CrossRef] [PubMed]
- Shumway-Cook, A.; Woollacott, M.H. Motor Control: Translating Research into Clinical Practice, 5th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2017; pp. 465–489. [Google Scholar]
- Guccione, A.A.; Wong, R.; Avers, D. Geriatric Physical Therapy, 3rd ed.; Elsevier: Louis, MO, USA, 2012. [Google Scholar]
- Li, Z.; Milutinovic, D.; Rosen, J. From reaching to reach-to-grasp: The arm posture difference and its implications on human motion control strategy. Exp. Brain Res. 2017, 235, 1627–1642. [Google Scholar] [CrossRef] [PubMed]
- Scharoun, S.M.; Scanlan, K.A.; Bryden, P.J. Hand and Grasp Selection in a Preferential Reaching Task: The Effects of Object Location, Orientation, and Task Intention. Front. Psychol. 2016, 7, 360. [Google Scholar] [CrossRef] [PubMed]
- Luinge, H.J.; Veltink, P.H. Measuring orientation of human body segments using miniature gyroscopes and accelerometers. Med. Biol. Eng. Comput. 2005, 43, 273–282. [Google Scholar] [CrossRef]


{kind=link}
| Sensor Type | Axis | Average Change during Task (Across Subjects) | Intra-Subject CoV Average | Inter-Subject CoV | Estimated Real Distance * |
|---|---|---|---|---|---|
| Gyrosensor | Forearm supination/pronation | 36.65 ± 6.98° | 17.29% | 19.05% | - |
| Elbow flexion/extension | 69.96 ± 16.89° | 11.67% | 24.14% | - | |
| Accelerometer (forearm sensor) | z-axis distance (up/down) | 34.14 ± 4.15 cm | 6.18% | 12.17% | 34.0 cm |
| y-axis distance (front/back) | 33.54 ± 4.79 cm | 7.16% | 14.28% | 33.5 cm | |
| Accelerometer (hand sensor) | z-axis distance (up/down) | 36.78 ± 3.09 cm | 5.56% | 8.41% | 34.0 cm |
| y-axis distance (front/back) | 32.35 ± 4.64 cm | 9.49% | 14.33% | 33.5 cm |
| Axis | Right | Left | pa | |
|---|---|---|---|---|
| ARAT | x-axis (left-right, hand sensor) | 0.53 ± 0.11 m | 0.62 ± 0.07 m | 0.082 |
| y-axis (front-back, hand sensor) | 0.92 ± 0.08 m | 0.80 ± 0.11 m | 0.049 * | |
| z-axis (hand sensor) | 0.89 ± 0.10 m | 0.86 ± 0.08 m | 0.224 | |
| Shoulder abduction/adduction | 50.16 ± 11.14° | 55.34 ± 13.48° | 0.249 | |
| Shoulder flexion/extension | 79.52 ± 19.34° | 75.71 ± 21.56° | 0.478 | |
| Elbow flexion/extension | 109.15 ± 18.82° | 106.89 ± 12.83° | 0.705 | |
| Forearm supination/pronation | 105.23 ± 15.38° | 108.64 ± 12.64° | 0.426 | |
| Shoulder IR/ER | 91.99 ± 20.98° | 84.44 ± 44.75° | 0.584 | |
| Wrist dorsiflexion/volarflexion | 82.90 ± 22.52° | 81.26 ± 11.16° | 0.833 | |
| ADL tasks | x-axis (left-right, hand sensor) | 0.71 ± 0.22 m | 0.52 ± 0.13 m | 0.001 * |
| y-axis (front-back, hand sensor) | 0.70 ± 0.17 m | 0.53 ± 0.15 m | 0.011 * | |
| z-axis (hand sensor) | 0.86 ± 0.11 m | 0.65 ± 0.13 m | 0.001 * | |
| Shoulder abduction/adduction | 58.84 ± 14.53° | 35.43 ± 10.09° | <0.001 * | |
| Shoulder flexion/extension | 68.41 ± 17.56° | 40.49 ± 18.54° | 0.002 * | |
| Elbow flexion/extension | 120.61 ± 23.64° | 102.53 ± 19.51° | 0.044 * | |
| Forearm supination/pronation | 128.09 ± 22.04° | 108.00 ± 16.23° | 0.027 * | |
| Shoulder IR/ER | 111.56 ± 31.88° | 77.04 ± 21.28° | 0.030 * | |
| Wrist dorsiflexion/volarflexion | 113.70 ± 18.26° | 110.08 ± 12.16° | 0.526 |
| Axis | Grasping Initial Position | ROM during Reaching | p | Pinching Initial Position | ROM during Reaching | p | Grasp-Pinch p a | Reaching Difference p b |
|---|---|---|---|---|---|---|---|---|
| Shoulder abduction/adduction | 15.33 ± 6.91° (abduction) | 22.48 ± 19.81° (toward abduction) | 0.006 * | 19.39 ± 7.84° (abduction) | 23.67 ± 13.35° (toward abduction) | <0.001 * | 0.040 * | 0.015 * |
| Shouler flexion/extension | 22.99 ± 10.63° (extension) | 47.80 ± 17.70° (toward flexion) | <0.001 * | 29.12 ± 12.33° (extension) | 41.83 ± 13.69° (toward flexion) | <0.001 * | 0.038 * | 0.948 |
| Elbow flexion/extension | 87.87 ± 25.18° (near fully flexed) | 69.96 ± 16.89° (toward extension) | <0.001 * | 84.82 ± 20.25° (near fully flexed) | 67.91 ± 14.16° (toward extension) | <0.001 * | 0.543 | 0.849 |
| Forearm supination/pronation c | 34.37 ± 11.07° (supinated) | 36.65 ± 6.98° (toward pronation) | <0.001 * | 30.98 ± 13.71° (supinated) | 36.02 ± 12.44° (toward pronation) | <0.001 * | 0.181 | 0.294 |
| Shoulder IR/ER | 0.68 ± 23.56° (inward direction) | 16.55 ± 23.02° (toward external rotation) | 0.049 * | 2.01 ± 13.74° (inward direction) | 18.10 ± 13.02° (toward external rotation) | 0.002 * | 0.794 | 0.860 |
| Wrist deviation | 8.94 ± 12.12° (to thumb side) | −1.76 ± 10.21° (to finger side) | 0.599 | 1.05 ± 8.19° (to thumb side) | 4.81 ± 8.85° (to thumb side) | 0.120 | 0.004 * | 0.522 |
| Wrist rotation | 4.59 ± 7.35° (toward palm down) | 7.12 ± 4.59° (toward palm up) | 0.001 * | 0.80 ± 5.25° (toward palm down) | 4.75 ± 4.05° (toward palm up) | 0.005 * | 0.023 * | 0.385 |
| Wrist dorsiflexion/volarflexion | 18.79 ± 16.35° (dorsiflexed) | 6.79 ± 6.00° (toward volarflexion) | 0.006 * | 11.30 ± 13.90° (dorsiflexed) | 7.28 ± 11.22° (toward volarflexion) | 0.070 | 0.166 | 0.123 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nam, H.S.; Lee, W.H.; Seo, H.G.; Kim, Y.J.; Bang, M.S.; Kim, S. Inertial Measurement Unit Based Upper Extremity Motion Characterization for Action Research Arm Test and Activities of Daily Living. Sensors 2019, 19, 1782. https://0-doi-org.brum.beds.ac.uk/10.3390/s19081782
Nam HS, Lee WH, Seo HG, Kim YJ, Bang MS, Kim S. Inertial Measurement Unit Based Upper Extremity Motion Characterization for Action Research Arm Test and Activities of Daily Living. Sensors. 2019; 19(8):1782. https://0-doi-org.brum.beds.ac.uk/10.3390/s19081782
Chicago/Turabian StyleNam, Hyung Seok, Woo Hyung Lee, Han Gil Seo, Yoon Jae Kim, Moon Suk Bang, and Sungwan Kim. 2019. "Inertial Measurement Unit Based Upper Extremity Motion Characterization for Action Research Arm Test and Activities of Daily Living" Sensors 19, no. 8: 1782. https://0-doi-org.brum.beds.ac.uk/10.3390/s19081782