A Novel Singular Value Decomposition-Based Denoising Method in 4-Dimensional Computed Tomography of the Brain in Stroke Patients with Statistical Evaluation

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Material and Methods
2.1. Patient Groups
2.2. Data Acquisition and Reconstruction
2.3. The SVD Technique
2.4. Denoising Based on SVD
2.5. Quantitative Image Analysis
2.6. Statistical Analysis
3. Results
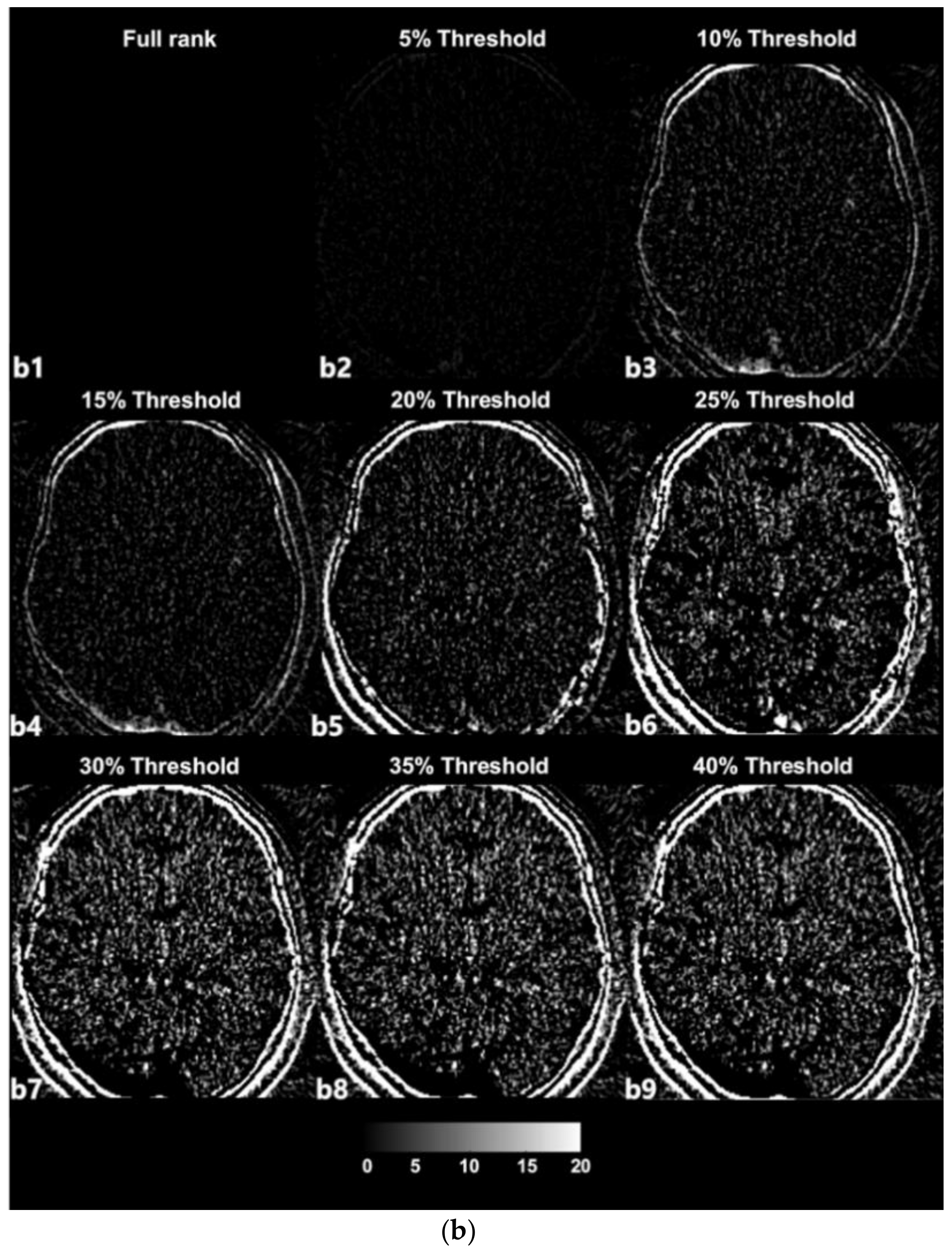
3.1. SVD-Based Noise Removal
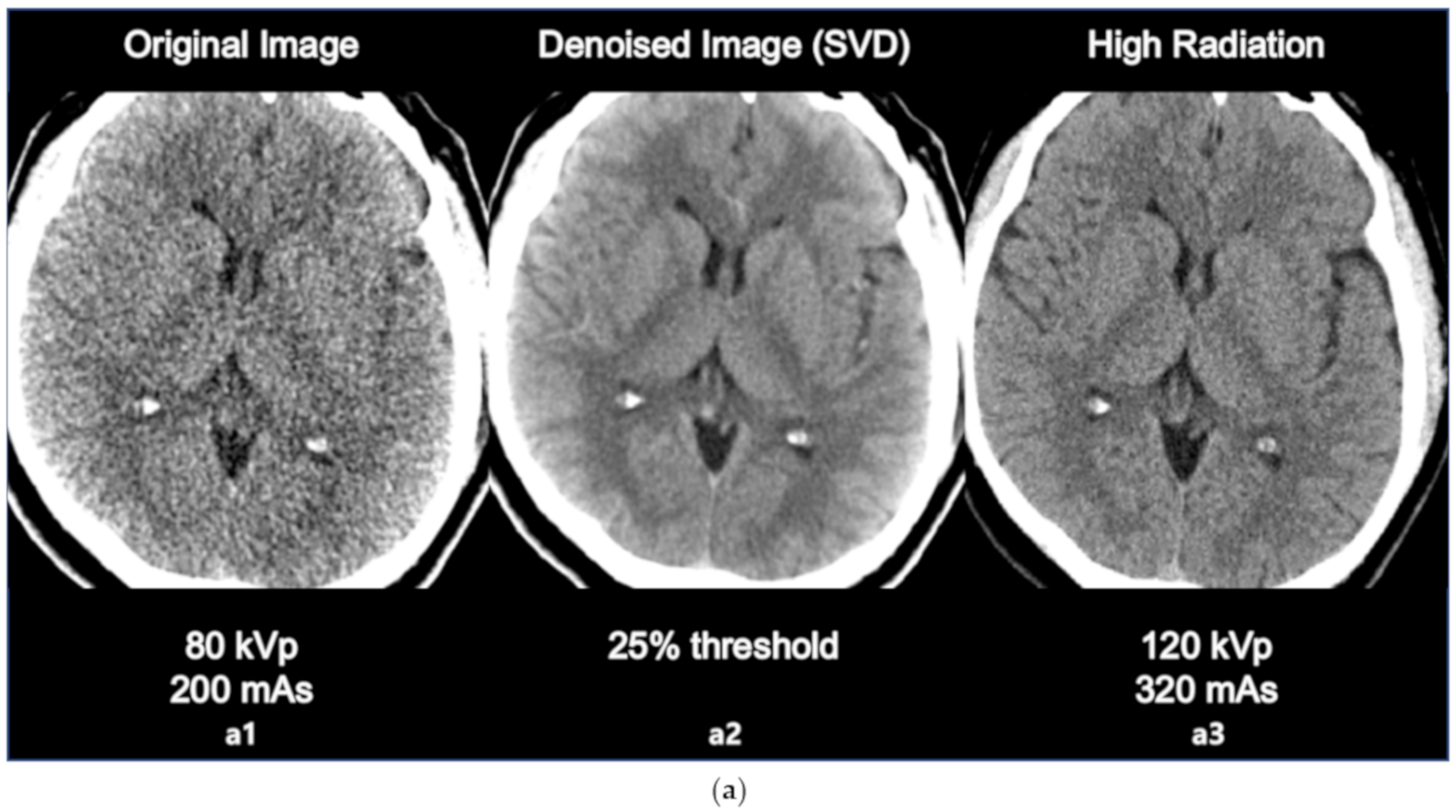
3.2. Comparison with High Radiation Dose Image
3.3. Quantitative Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| SC | singular component |
References
- Feigin, V.L.; Lawes, C.M.; Bennett, D.A.; Anderson, C.S. Stroke epidemiology: a review of population-based studies of incidence, prevalence, and case-fatality in the late 20th century. Lancet Neurol. 2003, 2, 43–53. [Google Scholar] [CrossRef]
- Ovbiagele, B.; Nguyen-Huynh, M.N. Stroke epidemiology: advancing our understanding of disease mechanism and therapy. Neurotherapeutics 2011, 8, 319–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guzik, A.; Bushnell, C. Stroke epidemiology and risk factor management. Continuum (Minneap. Minn.) 2017, 23, 15–39. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-H.; Park, H.-Y.; Lee, H.-S.; Ha, Y.-S.; Cheong, J.-S.; Cho, K.H.; Kim, N.-H.; Lee, K.S.; Kim, H.S.; Oh, G.-J. Effects of Community-based Stroke Education and Advocacy on the Time from Stroke Onset to Hospital Arrival in Ischemic Stroke Patients. J. Korean Neurol. Assoc. 2015, 33, 265–271. [Google Scholar] [CrossRef]
- Disorders NIoN; Group Sr-PSS. Tissue plasminogen activator for acute ischemic stroke. N. Engl. J. Med. 1995, 333, 1581–1588. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.T.; Shin, D.S.; Nam, T.S.; Jung, E.S.; Choi, S.M.; Son, E.J.; Kim, B.C.; Kim, M.K.; Cho, K.H.; Seo, J.J. Clinical usefulness of perfusion CT in acute ischemic stroke. J. Korean Neurol. Assoc. 2002, 20, 585–591. [Google Scholar]
- Karwacki, G.M.; Vögele, S.; Blackham, K.A. Dose reduction in perfusion CT in stroke patients by lowering scan frequency does not affect automatically calculated infarct core volumes. J. Neuroradiol. 2019, 46, 351–358. [Google Scholar] [CrossRef]
- Becks, M.J.; Manniesing, R.; Vister, J.; Pegge, S.A.; Steens, S.C.; Van Dijk, E.J.; Prokop, M.; Meijer, F.J.A. Brain CT perfusion improves intracranial vessel occlusion detection on CT angiography. J. Neuroradiol. 2019, 46, 124–129. [Google Scholar] [CrossRef]
- Yaghi, S.; Bianchi, N.; Amole, A.; Hinduja, A. ASPECTS is a predictor of favorable CT perfusion in acute ischemic stroke. J. Neuroradiol. 2014, 41, 184–187. [Google Scholar] [CrossRef]
- Kidwell, C.S.; Hsia, A.W. Imaging of the brain and cerebral vasculature in patients with suspected stroke: Advantages and disadvantages of CT and MRI. Curr. Neurol. Neurosci. Rep. 2006, 6, 9–16. [Google Scholar] [CrossRef]
- Vymazal, J.; Rulseh, A.M.; Keller, J.; Janouskova, L. Comparison of CT and MR imaging in ischemic stroke. Insights Imaging 2012, 3, 619–627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCollough, C.H.; Primak, A.N.; Braun, N.; Kofler, J.; Yu, L.; Christner, J.A. Strategies for Reducing Radiation Dose in CT. Radiol. Clin. N. Am. 2009, 47, 27–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.; Wang, X.; Mou, X.; Chen, Y.; Liu, S. Low dose CT image reconstruction based on structure tensor total variation using accelerated fast iterative shrinkage thresholding algorithm. Sensors 2020, 20, 1647. [Google Scholar] [CrossRef] [Green Version]
- Lee, W.-J.; Ahn, B.-S.; Park, Y.-S. Radiation Dose and Image Quality of Low-dose Protocol in Chest CT: Comparison of Standard-dose Protocol. J. Radiat. Prot. Res. 2012, 37, 84–89. [Google Scholar] [CrossRef]
- Pyeon, D.-Y.; Kim, J.; Baek, C.-H.; Jung, Y.-J. Singular Value Decomposition based Noise Reduction Technique for Dynamic PET Image: Preliminary study. J. Radiol. Sci. Technol. 2016, 39, 227–236. [Google Scholar] [CrossRef]
- Hoang, J.K.; Wang, C.; Frush, D.; Enterline, D.S.; Samei, E.; Toncheva, G.; Lowry, C.; Yoshizumi, T.T. Estimation of Radiation Exposure for Brain Perfusion CT: Standard Protocol Compared With Deviations in Protocol. Am. J. Roentgenol. 2013, 201, 730. [Google Scholar] [CrossRef] [PubMed]
- Riederer, I.; Zimmer, C.; Pfeiffer, D.; Wunderlich, S.; Poppert, H.; Rummeny, E.J.; Huber, A. Radiation dose reduction in perfusion CT imaging of the brain using a 256-slice CT: 80 mAs versus 160 mAs. Clin. Imaging 2018, 50, 188–193. [Google Scholar] [CrossRef]
- Labay, V.; Bornemann, J. Matrix singular value decomposition for pole-free solutions of homogeneous matrix equations as applied to numerical modeling methods. IEEE Microwave Guided Wave Lett. 1992, 2, 49–51. [Google Scholar] [CrossRef] [Green Version]
- Sato, H.; Iwai, T. A Riemannian optimization approach to the matrix singular value decomposition. SIAM J. Optimiz. 2013, 23, 188–212. [Google Scholar] [CrossRef]
- Ding, C.; Ye, J. 2-dimensional singular value decomposition for 2d maps and images. In Proceedings of the 2005 SIAM International Conference on Data Mining, Newport Beach, CA, USA, 21–25 April 2005. [Google Scholar]
- Lyra-Leite, D.M.; Da Costa, J.P.C.L.; De Carvalho, J.L.A. Improved MRI reconstruction and denoising using SVD-based low-rank approximation. In 2012 Workshop on Engineering Applications; IEEE: Piscataway, NJ, USA, 2012; pp. 1–6. [Google Scholar] [CrossRef]
- Bartuschat, D.; Borsdorf, A.; Köstler, H.; Rubinstein, R.; Stürmer, M. A Parallel K-SVD Implementation for CT Image Denoising; Fridrich-Alexander University: Erlangen, Germany, 2009. [Google Scholar]
- Feng, F.; Wang, J. A novel denoising approach to SVD filtering based on DCT and PCA in CT image. J. Biomed. Eng. Shengwu Yixue Gongchengxue Zazhi 2013, 30, 932–935. [Google Scholar]
- Shlens, J. A tutorial on principal component analysis derivation, discussion and singular value decomposition. Mar 2003, 25, 1–16. [Google Scholar]
- Jung, Y.-J.; Gonzalez, J.; Godavarty, A. Functional near-infrared imaging reconstruction based on spatiotemporal features: Venous occlusion studies. Appl. Opt. 2015, 54, D82–D90. [Google Scholar] [CrossRef]
- Park, H.-Y.; Pyeon, D.-Y.; Ali, Y.; Jung, Y.-J. Dynamic Computed Tomography based on Spatio-temporal Analysis in Acute Stroke: Preliminary Study. J. Radiol. Sci. Technol. 2016, 39, 543–547. [Google Scholar] [CrossRef]
- Korn, A.; Fenchel, M.; Bender, B.; Danz, S.; Hauser, T.K.; Ketelsen, D.; Flohr, T.; Claussen, C.D.; Heuschmid, M.; Ernemann, U.; et al. Iterative reconstruction in head CT: image quality of routine and low-dose protocols in comparison with standard filtered back-projection. AJNR Am. J. Neuroradiol. 2012, 33, 218–224. [Google Scholar] [CrossRef] [Green Version]
- Edfors, O.; Sandell, M.; Van de Beek, J.J.; Wilson, S.K.; Borjesson, P.O. OFDM channel estimation by singular value decomposition. IEEE Trans. Commun. 1998, 46, 931–939. [Google Scholar] [CrossRef] [Green Version]
- Jha, S.K.; Yadava, R.D.S. Denoising by singular value decomposition and its application to electronic nose data processing. IEEE Sens. J. 2010, 11, 35–44. [Google Scholar] [CrossRef]
- Othman, A.; Afat, S.; Brockmann, M.A.; Nikoubashman, O.; Brockmann, C.; Nikolaou, K.; Wiesmann, M. Radiation dose reduction in perfusion CT imaging of the brain: A review of the literature. J. Neuroradiol. 2016, 43, 1–5. [Google Scholar] [CrossRef]
- Ohno, Y.; Takenaka, D.; Kanda, T.; Yoshikawa, T.; Matsumoto, S.; Sugihara, N.; Sugimura, K. Adaptive iterative dose reduction using 3D processing for reduced-and low-dose pulmonary CT: comparison with standard-dose CT for image noise reduction and radiological findings. AJR Am. J. Roentgenol. 2012, 199, W477–W485. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| OG | 5% | 10% | 15% | 20% | 25% | 30% | 35% | 40% | |
|---|---|---|---|---|---|---|---|---|---|
| (a) | |||||||||
| Mean | 64.78 | 66.70 | 69.99 | 70.26 | 72.37 | 73.67 | 73.06 | 74.77 | 75.59 |
| SD | 20.12 | 21.39 | 21.31 | 23.09 | 23.60 | 23.85 | 25.41 | 25.15 | 25.12 |
| t | 0 | −2.148 | −3.145 | −2.650 | −3.344 | −3.764 | −2.514 | −2.664 | −2.908 |
| p | 0 | * 0.022 | ** 0.003 | ** 0.008 | 0.002 | *** <0.001 | * 0.011 | ** 0.008 | ** 0.005 |
| (b) | |||||||||
| Mean | 0.65 | 0.67 | 0.75 | 0.80 | 0.87 | 0.89 | 0.89 | 0.92 | 0.93 |
| SD | 0.53 | 0.52 | 0.56 | 0.54 | 0.55 | 0.56 | 0.56 | 0.57 | 0.57 |
| t | 0 | −1.892 | −2.835 | −4.146 | −5.855 | −6.080 | −5.927 | −6.304 | −6.327 |
| p | 0 | 0.037 | ** 0.005 | *** <0.001 | *** <0.001 | *** <0.001 | *** <0.001 | *** <0.001 | *** <0.001 |
| OG | 5% | 10% | 15% | 20% | 25% | 30% | 35% | 40% | |
|---|---|---|---|---|---|---|---|---|---|
| (a) | |||||||||
| Subject#1 | 0 | −0.04 | 0.01 | 0.01 | 20.05 | 20.67 | 21.26 | 21.24 | 24.24 |
| Subject#2 | 0 | 0.53 | 4.95 | 10.35 | 6.97 | 7.02 | 28.24 | 28.24 | 28.24 |
| Subject#3 | 0 | 0.05 | 0.27 | 2.92 | 3.49 | 3.57 | 2.34 | 2.34 | 6.42 |
| Subject#4 | 0 | 0.72 | 0.67 | 12.87 | 20.11 | 20.92 | 17.41 | 24.72 | 24.72 |
| Subject#5 | 0 | 0.02 | 2.73 | 3.25 | 3.64 | 4.76 | 4.76 | 4.76 | 6.15 |
| Subject#6 | 0 | 0.48 | 4.55 | −5.56 | −4.34 | −4.29 | −35.36 | −35.36 | −35.36 |
| Subject#7 | 0 | 0.67 | 3.11 | −2.98 | −2.74 | −2.47 | 3.54 | 3.54 | 5.19 |
| Subject#8 | 0 | 7.80 | 10.29 | −3.51 | −3.51 | −4.65 | −4.65 | −4.65 | −4.65 |
| Subject#9 | 0 | 0.12 | 3.34 | 5.18 | 5.18 | 8.52 | 8.52 | 1.05 | 1.05 |
| Subject#10 | 0 | −1.39 | 29.56 | 27.30 | 34.51 | 26.63 | 26.63 | 43.70 | 43.70 |
| Subject#11 | 0 | 0.37 | −0.16 | −7.83 | −3.75 | −3.75 | −3.75 | −3.75 | −3.75 |
| Subject#12 | 0 | 0.63 | 16.69 | 25.02 | 16.48 | 16.47 | 16.47 | 8.49 | 7.81 |
| Subject#13 | 0 | 10.58 | 14.30 | 15.43 | 16.29 | 26.32 | 26.32 | 26.32 | 26.32 |
| Subject#14 | 0 | 1.91 | 3.08 | 8.27 | 13.28 | 13.31 | 13.31 | 24.14 | 24.14 |
| Subject#15 | 0 | 0.05 | 5.14 | 5.90 | 8.36 | 22.63 | 22.63 | 22.63 | 22.63 |
| Subject#16 | 0 | 0.04 | 0.47 | 0.61 | −1.61 | −1.57 | −2.14 | 0.69 | 0.69 |
| Subject#17 | 0 | 13.84 | 2.60 | 2.60 | −0.86 | −0.84 | −0.84 | −0.84 | 9.27 |
| Subject#18 | 0 | 0.02 | 0.01 | 6.38 | 7.74 | 8.84 | 8.84 | 8.84 | 10.98 |
| Subject#19 | 0 | 1.45 | 2.19 | −1.69 | 2.42 | 2.81 | 2.81 | 14.26 | 14.26 |
| Subject#20 | 0 | 0.40 | 0.37 | 4.93 | 9.91 | 12.89 | 9.26 | 9.26 | 3.97 |
| Mean | 1.91 | 5.21 | 5.47 | 7.58 | 8.89 | 8.28 | 9.98 | 10.80 | |
| SD | 3.88 | 7.22 | 9.00 | 9.88 | 10.30 | 14.35 | 16.33 | 16.19 | |
| t | −2.148 | −3.145 | −2.650 | −3.344 | −3.764 | −2.514 | −2.664 | −2.908 | |
| p | * 0.022 | * 0.003 | * 0.008 | 0.002 | * 0.001 | * 0.011 | * 0.008 | * 0.005 | |
| (b) | |||||||||
| Subject#1 | 0 | 0.01 | 0.01 | 0.01 | 0.28 | 0.32 | 0.32 | 0.32 | 0.41 |
| Subject#2 | 0 | 0.01 | 0.07 | 0.23 | 0.33 | 0.33 | 0.47 | 0.47 | 0.47 |
| Subject#3 | 0 | 0.00 | 0.01 | 0.05 | 0.06 | 0.07 | 0.04 | 0.04 | 0.03 |
| Subject#4 | 0 | −0.01 | −0.01 | 0.12 | 0.33 | 0.38 | 0.41 | 0.42 | 0.42 |
| Subject#5 | 0 | 0.00 | 0.01 | 0.02 | 0.02 | 0.02 | 0.02 | 0.02 | 0.02 |
| Subject#6 | 0 | 0.06 | 0.30 | 0.40 | 0.39 | 0.39 | 0.36 | 0.36 | 0.36 |
| Subject#7 | 0 | 0.10 | 0.26 | 0.29 | 0.30 | 0.31 | 0.32 | 0.32 | 0.31 |
| Subject#8 | 0 | 0.11 | 0.08 | 0.14 | 0.14 | 0.14 | 0.14 | 0.14 | 0.14 |
| Subject#9 | 0 | 0.00 | 0.02 | 0.01 | 0.01 | 0.01 | 0.01 | 0.07 | 0.07 |
| Subject#10 | 0 | 0.06 | 0.55 | 0.57 | 0.67 | 0.55 | 0.55 | 0.61 | 0.61 |
| Subject#11 | 0 | 0.03 | 0.12 | 0.23 | 0.24 | 0.24 | 0.24 | 0.24 | 0.24 |
| Subject#12 | 0 | −0.01 | 0.01 | 0.07 | 0.07 | 0.07 | 0.07 | 0.09 | 0.09 |
| Subject#13 | 0 | 0.01 | 0.01 | 0.00 | 0.00 | 0.02 | 0.02 | 0.02 | 0.02 |
| Subject#14 | 0 | −0.08 | 0.01 | 0.05 | 0.21 | 0.21 | 0.21 | 0.44 | 0.44 |
| Subject#15 | 0 | 0.00 | 0.38 | 0.38 | 0.36 | 0.55 | 0.55 | 0.55 | 0.55 |
| Subject#16 | 0 | 0.00 | 0.02 | 0.10 | 0.37 | 0.37 | 0.34 | 0.39 | 0.39 |
| Subject#17 | 0 | 0.14 | 0.14 | 0.14 | 0.16 | 0.16 | 0.16 | 0.16 | 0.13 |
| Subject#18 | 0 | 0.01 | 0.01 | 0.17 | 0.17 | 0.17 | 0.17 | 0.17 | 0.32 |
| Subject#19 | 0 | 0.04 | 0.01 | −0.01 | 0.02 | 0.02 | 0.02 | 0.06 | 0.06 |
| Subject#20 | 0 | −0.02 | −0.02 | −0.01 | 0.32 | 0.38 | 0.44 | 0.44 | 0.56 |
| Mean | 0.02 | 0.10 | 0.15 | 0.22 | 0.23 | 0.24 | 0.27 | 0.28 | |
| SD | 0.05 | 0.15 | 0.16 | 0.17 | 0.17 | 0.18 | 0.18 | 0.19 | |
| t | −1.892 | −2.835 | −4.146 | −5.855 | −6.080 | −5.927 | −6.304 | −6.327 | |
| p | * 0.037 | * 0.005 | * <0.001 | * <0.001 | * <0.001 | * <0.001 | * <0.001 | * <0.001 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, W.; Hong, J.-Y.; Kim, J.-Y.; Paik, S.-h.; Lee, S.H.; Park, J.-S.; Lee, G.; Kim, B.M.; Jung, Y.-J. A Novel Singular Value Decomposition-Based Denoising Method in 4-Dimensional Computed Tomography of the Brain in Stroke Patients with Statistical Evaluation. Sensors 2020, 20, 3063. https://0-doi-org.brum.beds.ac.uk/10.3390/s20113063
Yang W, Hong J-Y, Kim J-Y, Paik S-h, Lee SH, Park J-S, Lee G, Kim BM, Jung Y-J. A Novel Singular Value Decomposition-Based Denoising Method in 4-Dimensional Computed Tomography of the Brain in Stroke Patients with Statistical Evaluation. Sensors. 2020; 20(11):3063. https://0-doi-org.brum.beds.ac.uk/10.3390/s20113063
Chicago/Turabian StyleYang, WonSeok, Jun-Yong Hong, Jeong-Youn Kim, Seung-ho Paik, Seung Hyun Lee, Ji-Su Park, Gihyoun Lee, Beop Min Kim, and Young-Jin Jung. 2020. "A Novel Singular Value Decomposition-Based Denoising Method in 4-Dimensional Computed Tomography of the Brain in Stroke Patients with Statistical Evaluation" Sensors 20, no. 11: 3063. https://0-doi-org.brum.beds.ac.uk/10.3390/s20113063