Reliability of Kinovea® Software and Agreement with a Three-Dimensional Motion System for Gait Analysis in Healthy Subjects

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Ethical Aspects
2.3. Instrumentation
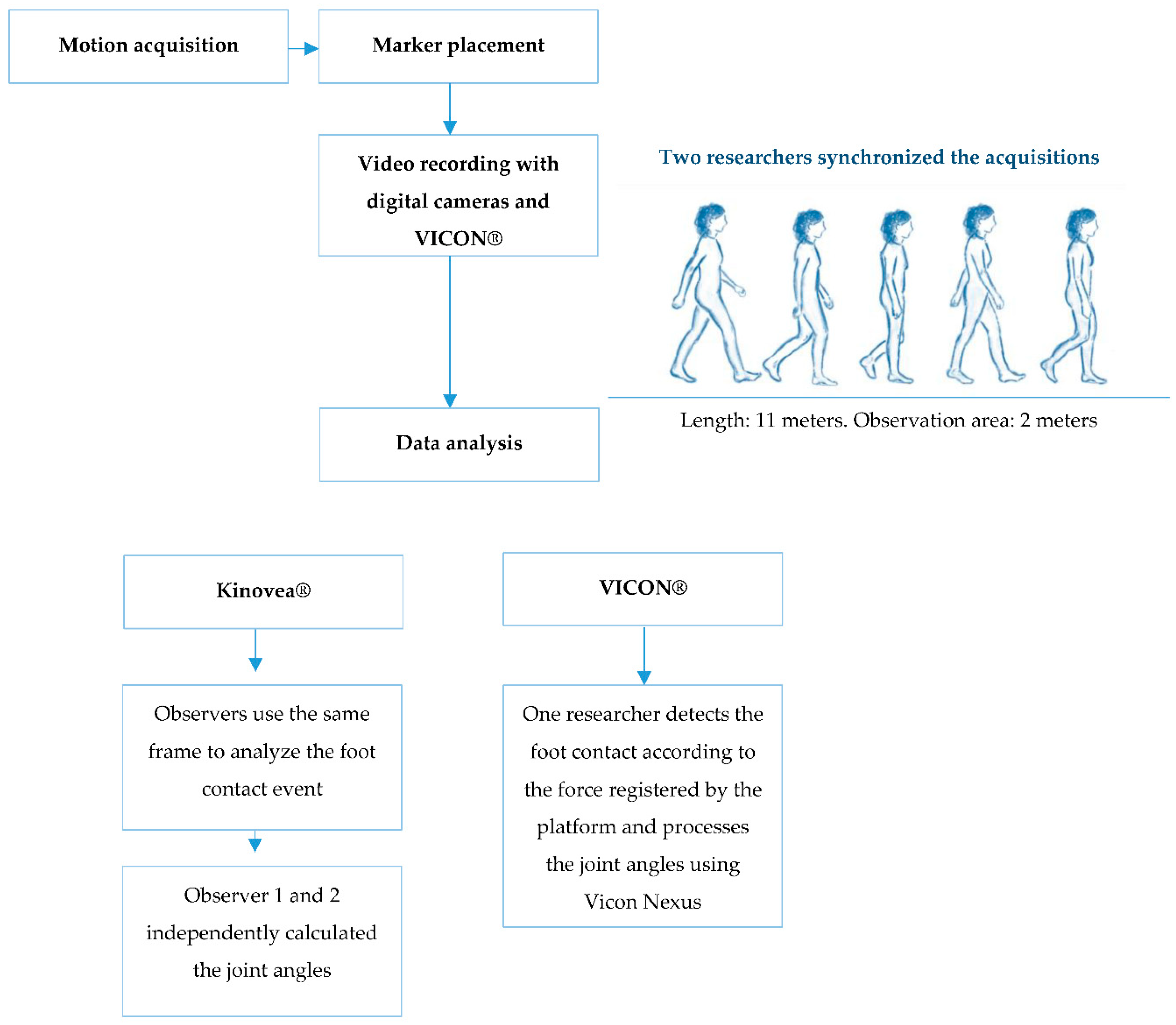
2.4. Procedures
2.5. Analysis of Data
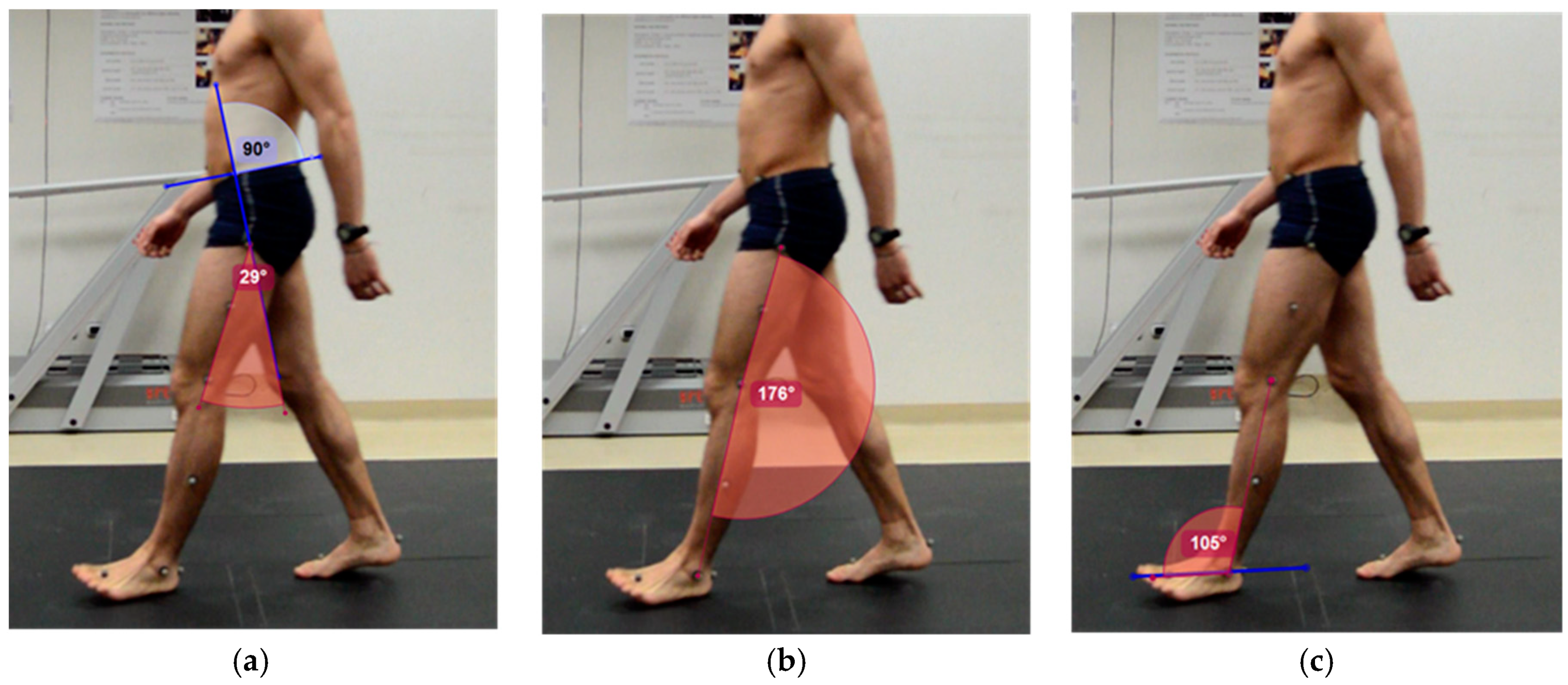
- Hip. A line is drawn through the anterior superior iliac spine and the posterior superior iliac spine. Perpendicular to this, another line is drawn that passes through the greater trochanter. The angle formed by the latter and the line joining the greater trochanter to the external femoral condyle will form the joint range of the hip.
- Knee. A line is drawn between the reference points of greater trochanter and femoral condyle, and another between femoral condyle and external malleolus. The angle formed between the two lines will be used for calculating the knee joint range. In this work, 180 degrees will be considered as the neutral position of the knee. Joint range is calculated by the following equation:Knee Joint Range = 180-(angle obtained with Kinovea®), positive values correspond to knee flexion and negative values to extension.
- Ankle. A line is drawn that joins the markers of the head of the second metatarsal and the calcaneus. The angle formed between this and the line passing through the femoral condyle and the external malleolus is used to calculate the ankle joint range. In this work, 90 degrees will be considered as the neutral position of the ankle. Joint range is calculated by the following equation:Ankle Joint Range = 90-(angle obtained with Kinovea®), positive values correspond to dorsiflexion, and negative values to plantar flexion.
2.6. Sample Size Calculation
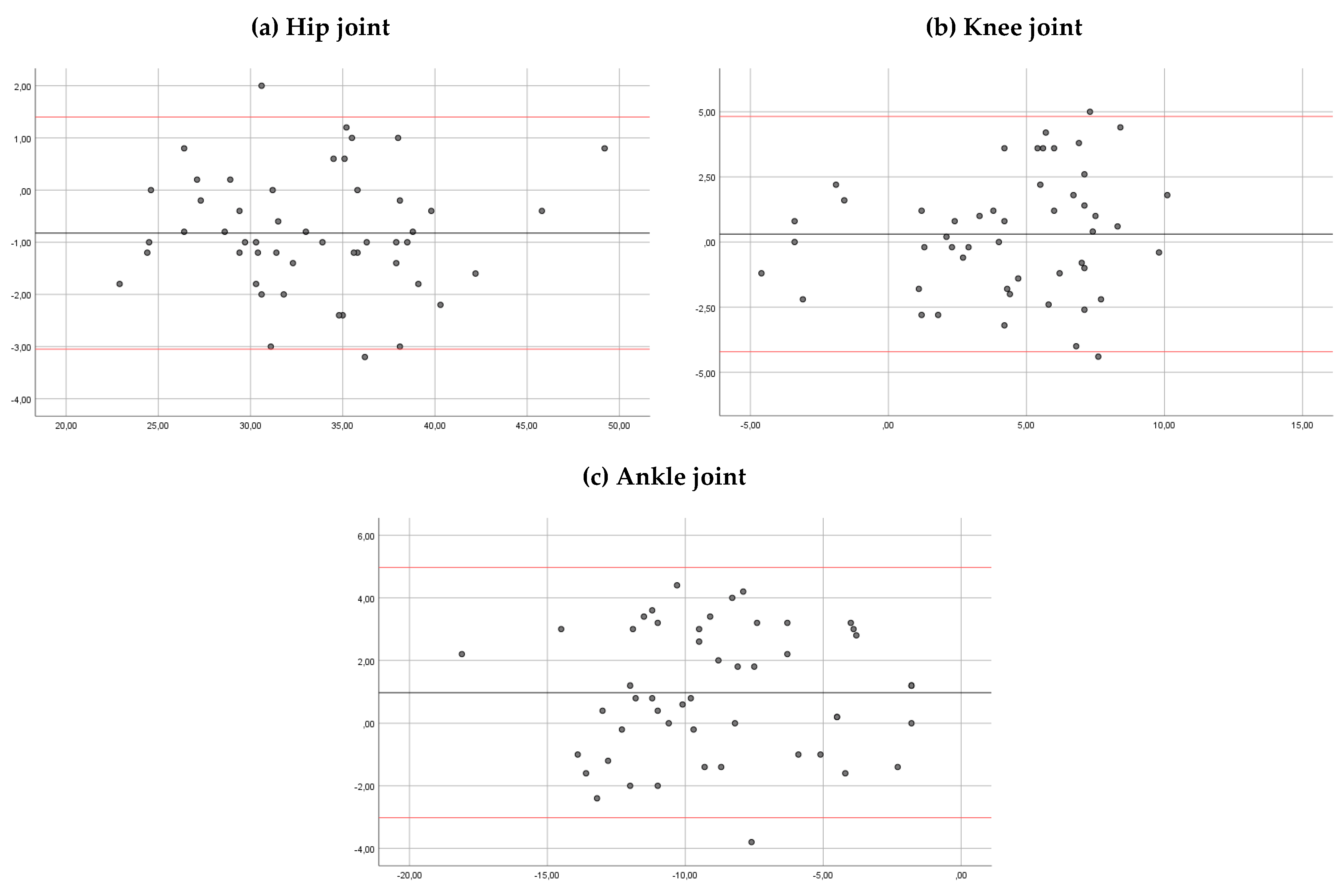
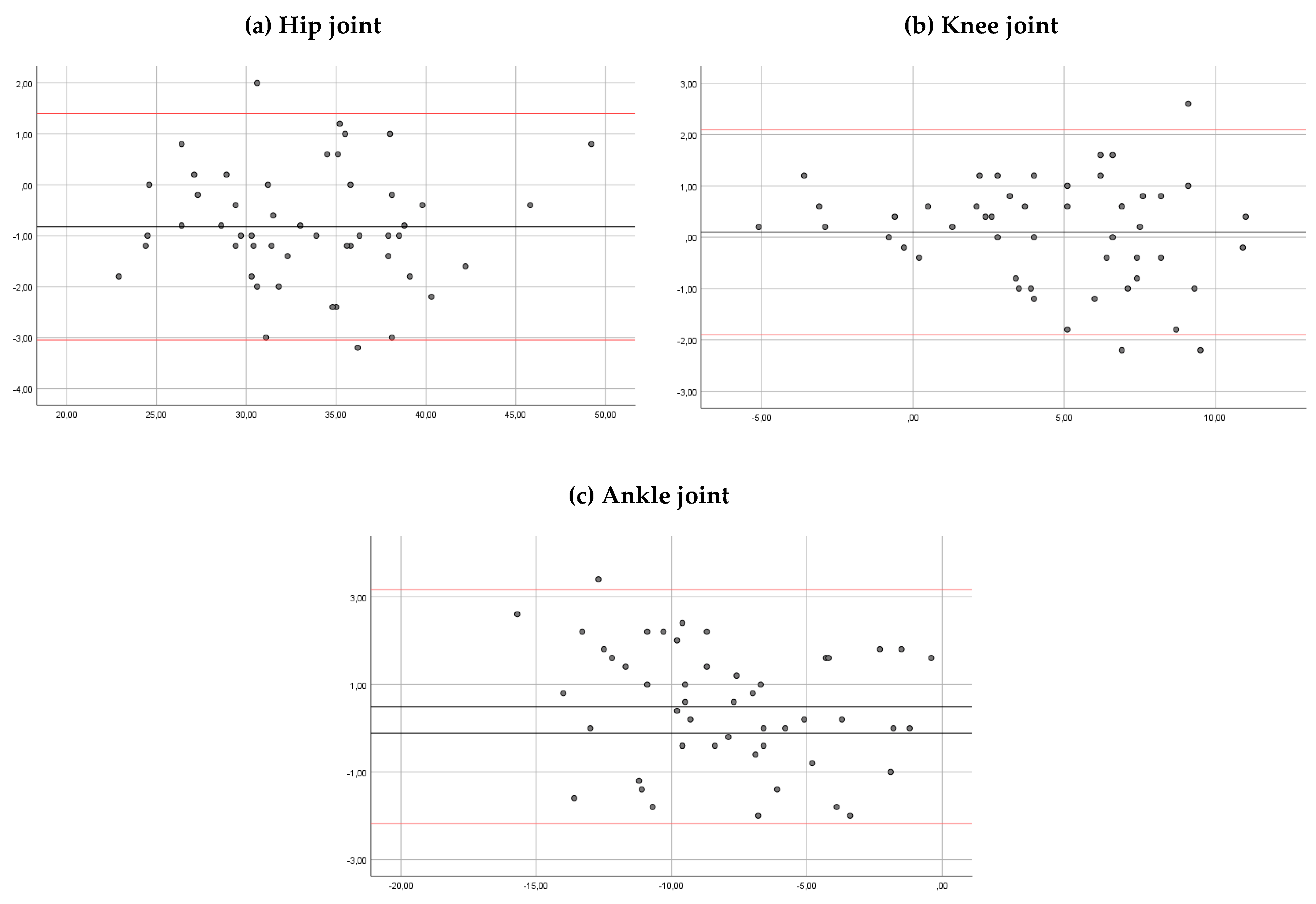
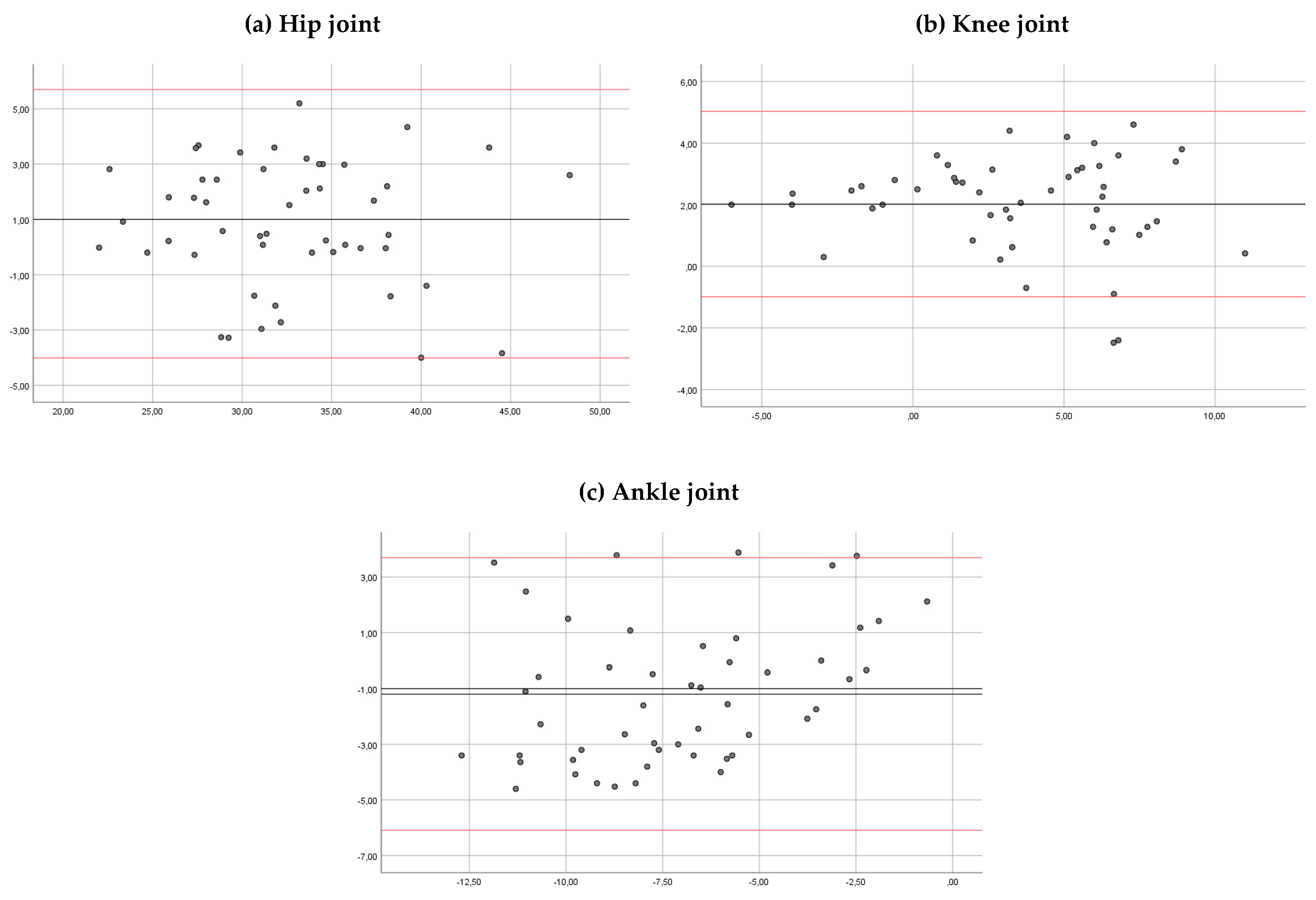
2.7. Statistical Analysis
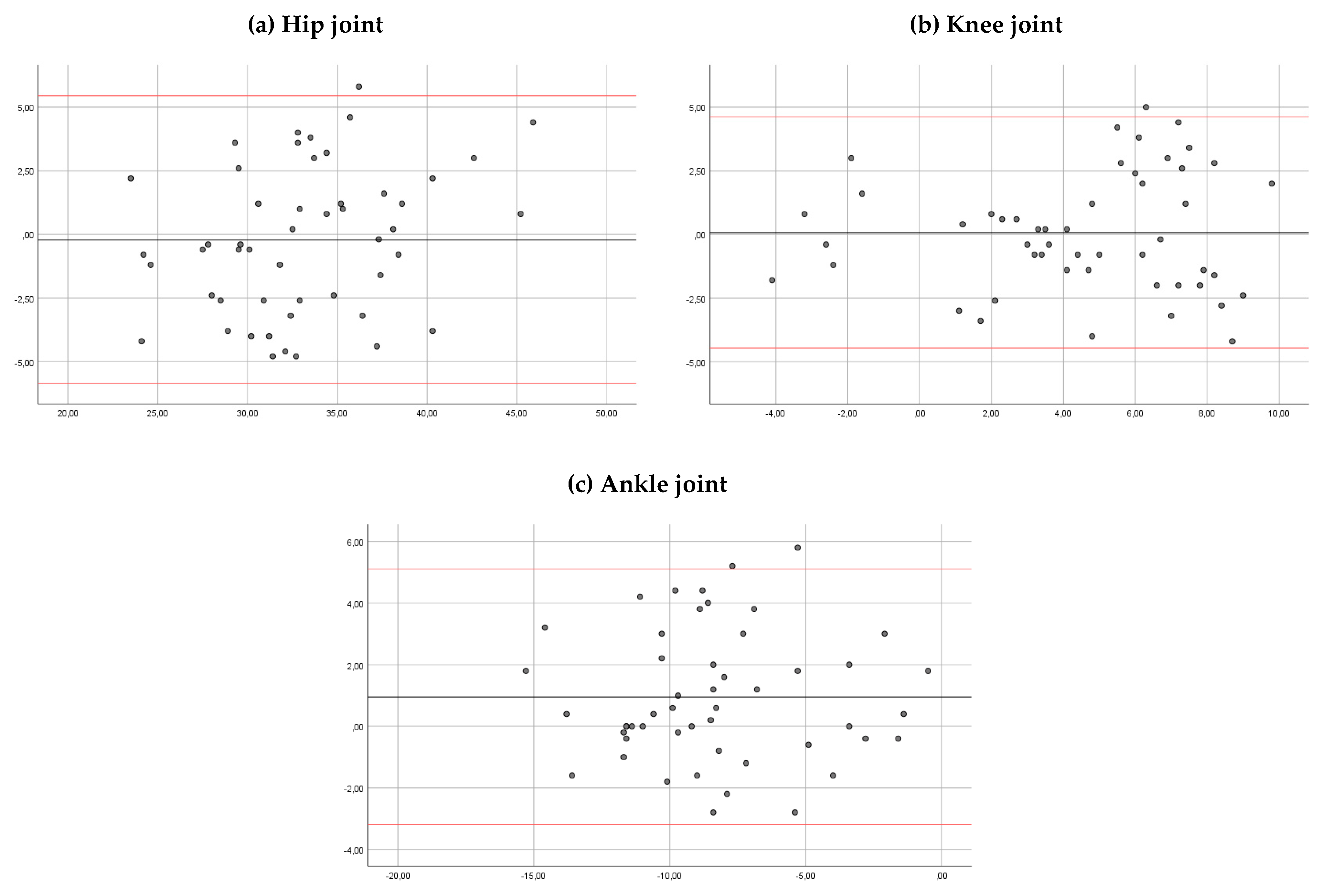
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| G.A.I.T. | Gait Assessment and Intervention Tool |
| LAMBECOM | Laboratory of Analysis of Movement, Biomechanics, Ergonomics and Motor Control |
| ICC | Intraclass Correlation Coefficient |
| CI | Confidence Interval |
| SD | Standard Deviation |
| MD | Mean of the differences |
References
- Harvey, A.; Gorter, J.W. Video gait analysis for ambulatory children with cerebral palsy: Why, when, where and how! Gait Posture 2011, 33, 501–503. [Google Scholar] [CrossRef]
- Daly, J.J.; Nethery, J.; McCabe, J.P.; Brenner, I.; Rogers, J.; Gansen, J.; Butler, K.; Burdsall, R.; Roenigk, K.; Holcomb, J. Development and testing of the Gait Assessment and Intervention Tool (G.A.I.T.): A measure of coordinated gait components. J. Neurosci. Methods 2009, 178, 334–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gor-García-Fogeda, M.D.; Cano-de la Cuerda, R.; Carratalá-Tejada, M.; Alguacil-Diego, I.M.; Molina-Rueda, F. Observational gait assessments in people with neurological disorders: A systematic review. Arch. Phys. Med. Rehabil. 2016, 97, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.R.; Hillman, S.J.; Richardson, A.M.; Herman, J.L.; Robb, J.E. Reliability and validity of the Visual Gait Assessment Scale for children with hemiplegic cerebral palsy when use by experienced and inexperienced observers. Gait Posture 2008, 27, 648–652. [Google Scholar] [CrossRef] [PubMed]
- Mills, K. Motion analysis in the clinic: There’s an app for that. J. Physiother. 2015, 61, 49–50. [Google Scholar] [CrossRef] [Green Version]
- Bertelsen, M.L.; Jensen, J.F.; Nielsen, M.H.; Nielsen, R.O.; Rasmussen, S. Foot strike patterns among novice runners wearing a conventional, neutral running shoe. Gait Posture 2012, 38, 354–356. [Google Scholar] [CrossRef] [PubMed]
- Damsted, C.; Larsen, L.H.; Nielsen, R.O. Reliability of video-based identification of footstrike pattern and video time frame at initial contact in recreational runners. Gait Posture 2015, 42, 32–35. [Google Scholar] [CrossRef] [PubMed]
- Damsted, C.; Nielsen, R.O.; Larsen, L.H. Reliability of video-based quantification of the knee- and hip angle at foot strike during running. Int. J. Sports Phys. Ther. 2015, 10, 147–154. [Google Scholar]
- Balsalobre-Fernández, C.; Tejero-González, C.M.; del Campo-Vecino, J.; Bavaresco, N. The concurrent validity and reliability of a low cost, high-speed camera-based method for measuring the flight time of vertical jumps. J. Strength Cond. Res. 2014, 28, 528–533. [Google Scholar] [CrossRef]
- de Almeida, M.O.; Saragiotto, B.T.; Yamato, T.P.; Lopes, A.D. Is the rearfoot pattern the most frequently foot strike pattern among recreational shod distance runners? Phys. Ther. Sport. 2015, 16, 29–33. [Google Scholar] [CrossRef]
- Elwardany, S.H.; El-Sayed, W.H.; Ali, M.F. Reliability of Kinovea computer program in measuring cervical range of motion in sagittal plane. Open Access Libr. J. 2015, 2, 68651. [Google Scholar] [CrossRef]
- El-Raheem, R.M.A.; Kamel, R.M.; Ali, M.F. Reliability of using Kinovea program in measuring dominant wrist joint range of motion. Trends Appl. Sci. Res. 2015, 10, 224–230. [Google Scholar]
- Mathew, J.; Vanlalpeki, T.; Nair, G.G. Gait evaluation of institutionalized elders. A feasibility study. Indian J. Gerontol. 2017, 31, 71–83. [Google Scholar]
- Davis, R.B.; Ounpuu, S.; Tyburski, D.; Gage, J.R. A gait analysis data collection and reduction technique. Hum. Mot. Sci. 1991, 10, 575–587. [Google Scholar] [CrossRef]
- Kadaba, M.P.; Ramakrishnan, H.K.; Wootten, M.E. Measurement of lower extremity kinematics during level walking. J. Orthop. Res. 1990, 8, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Vicon Motion System. Plug-in Gait Product Guide—Foundation Notes Revision 2.0. Available online: https://www.vicon.com/downloads/documentation/plug-in-gait-product-guide (accessed on 20 March 2020).
- Vicon Documentation. Available online: https://docs.vicon.com/display/Nexus25/Plug-in+Gait+kinematic+variables (accessed on 22 March 2019).
- Lambrecht, S.; Harutyunyan, A.; Tanghe, K.; Afschrift, M.; De Schutter, J.; Jonkers, I. Real-time gait event detection based on kinematic data coupled to a biomechanical model. Sensors 2017, 17, 671. [Google Scholar] [CrossRef] [Green Version]
- Walter, S.D.; Eliasziw, M.; Donner, A. Sample size and optimal designs for reliability studies. Stat. Med. 1998, 17, 101–110. [Google Scholar] [CrossRef]
- Bartlett, J.; Frost, C. Reliability, repeatability and reproducibility: Analysis of measurement errors in continuous variables. Ultrasound Obstet. Gynecol. 2008, 31, 466–475. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Yeo, S.S.; Park, G.Y. Accuracy verification of spatio-temporal and kinematic parameters for gait using inertial measurement unit system. Sensors 2020, 20, 1343. [Google Scholar] [CrossRef] [Green Version]
- Perry, J. Gait Analysis: Normal and Pathological Function; Slack Inc.: Thorofare, NJ, USA, 1992. [Google Scholar]
- Wilken, J.M.; Rodriguez, K.M.; Brawner, M.; Darter, B.J. Reliability and minimal detectible change values for gait kinematics and kinetics in healthy adults. Gait Posture 2012, 5, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Meldrum, D.; Shouldice, C.; Conroy, R.; Jones, K.; Forward, M. Test-retest reliability of three dimensional gait analysis: Including a novel approach to visualising agreement of gait cycle waveforms with Bland and Altman plots. Gait Posture 2014, 39, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- McGinley, J.L.; Baker, R.; Wolfe, R.; Morris, M.E. The reliability of three-dimensional kinematic gait measurements: A systematic review. Gait Posture 2009, 29, 360–369. [Google Scholar] [CrossRef]
- Baker, R.; Esquenazi, A.; Benedetti, M.G.; Desloovere, K. Gait analysis: Clinical facts. Eur. J. Phys. Rehabil. Med. 2016, 52, 560–574. [Google Scholar]
- Littrell, M.E.; Chang, Y.H.; Selgrade, B.P. Development and assessment of a low-cost clinical gait analysis system. J. Appl. Biomech. 2018, 34, 503–508. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Angles (Degrees) | Intra-Rater Reliability | ||||
|---|---|---|---|---|---|
| Session 1 | Session 2 | ICC | 95% CI | p | |
| Hip | (a) 33.06 (5.7) | (a) 33.4 (4.87) | (a) 0.886 | (a) 0.799 to 0.935 | (a) < 0.01 * |
| (b) 33.8 (5.52) | (b) 33.6 (5.06) | (b) 0.863 | (b) 0.758 to 0.922 | (b) < 0.01 * | |
| Knee | (a) 4.55 (3.8) | (a) 4.36 (3.5) | (a) 0.859 | (a) 0.751 to 0.920 | (a) < 0.01 * |
| (b) 4.45 (3.95) | (b) 4.11 (3.52) | (b) 0.868 | (b) 0.768 to 0.925 | (b) < 0.01 * | |
| Ankle | (a) −7.77 (3.7) | (a) −8.86 (3.6) | (a) 0.875 | (a) 0.780 to 0.929 | (a) < 0.01 * |
| (b) −8.2 (4.01) | (b) −9.46 (3.84) | (b) 0.878 | (b) 0.784 to 0.931 | (b) < 0.01 * | |
| Angles (Degrees) | Observer 1 vs. 2 | ||||
|---|---|---|---|---|---|
| Observer 1 | Observer 2 | ICC | 95% CI | p-Value | |
| Hip | 33.06 (5.7) | 33.8 (5.52) | 0.962 | 0.933 to 0.978 | <0.01 * |
| Knee | 4.55 (3.8) | 4.45 (3.95) | 0.989 | 0.981 to 0.994 | <0.01 * |
| Ankle | −7.77 (3.7) | −8.2 (4.01) | 0.973 | 0.952 to 0.984 | <0.01 * |
| Kinematic (Degrees) | Kinovea vs. Vicon | ||||
|---|---|---|---|---|---|
| Kinovea | Vicon | MD | 95% CI | p-Value | |
| Hip | 33.06 (5.7) | 32.2 (5.82) | 0.80 | 0.12 to 1.49 | 0.022 |
| Knee | 4.55 (3.8) | 2.53 (3.93) | 2.02 | 1.58 to 2.45 | <0.01 |
| Ankle | −7.77 (3.7) | −6.50 (2.82) | −1.27 | −2.03 to -0.51 | <0.01 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-González, P.; Koutsou, A.; Cuesta-Gómez, A.; Carratalá-Tejada, M.; Miangolarra-Page, J.C.; Molina-Rueda, F. Reliability of Kinovea® Software and Agreement with a Three-Dimensional Motion System for Gait Analysis in Healthy Subjects. Sensors 2020, 20, 3154. https://0-doi-org.brum.beds.ac.uk/10.3390/s20113154
Fernández-González P, Koutsou A, Cuesta-Gómez A, Carratalá-Tejada M, Miangolarra-Page JC, Molina-Rueda F. Reliability of Kinovea® Software and Agreement with a Three-Dimensional Motion System for Gait Analysis in Healthy Subjects. Sensors. 2020; 20(11):3154. https://0-doi-org.brum.beds.ac.uk/10.3390/s20113154
Chicago/Turabian StyleFernández-González, Pilar, Aikaterini Koutsou, Alicia Cuesta-Gómez, María Carratalá-Tejada, Juan Carlos Miangolarra-Page, and Francisco Molina-Rueda. 2020. "Reliability of Kinovea® Software and Agreement with a Three-Dimensional Motion System for Gait Analysis in Healthy Subjects" Sensors 20, no. 11: 3154. https://0-doi-org.brum.beds.ac.uk/10.3390/s20113154