
Detection of Dental Caries and Cracks with Quantitative Light-Induced Fluorescence in Comparison to Radiographic and Visual Examination: A Retrospective Case Study

 , ,
, , 
Abstract
:1. Introduction
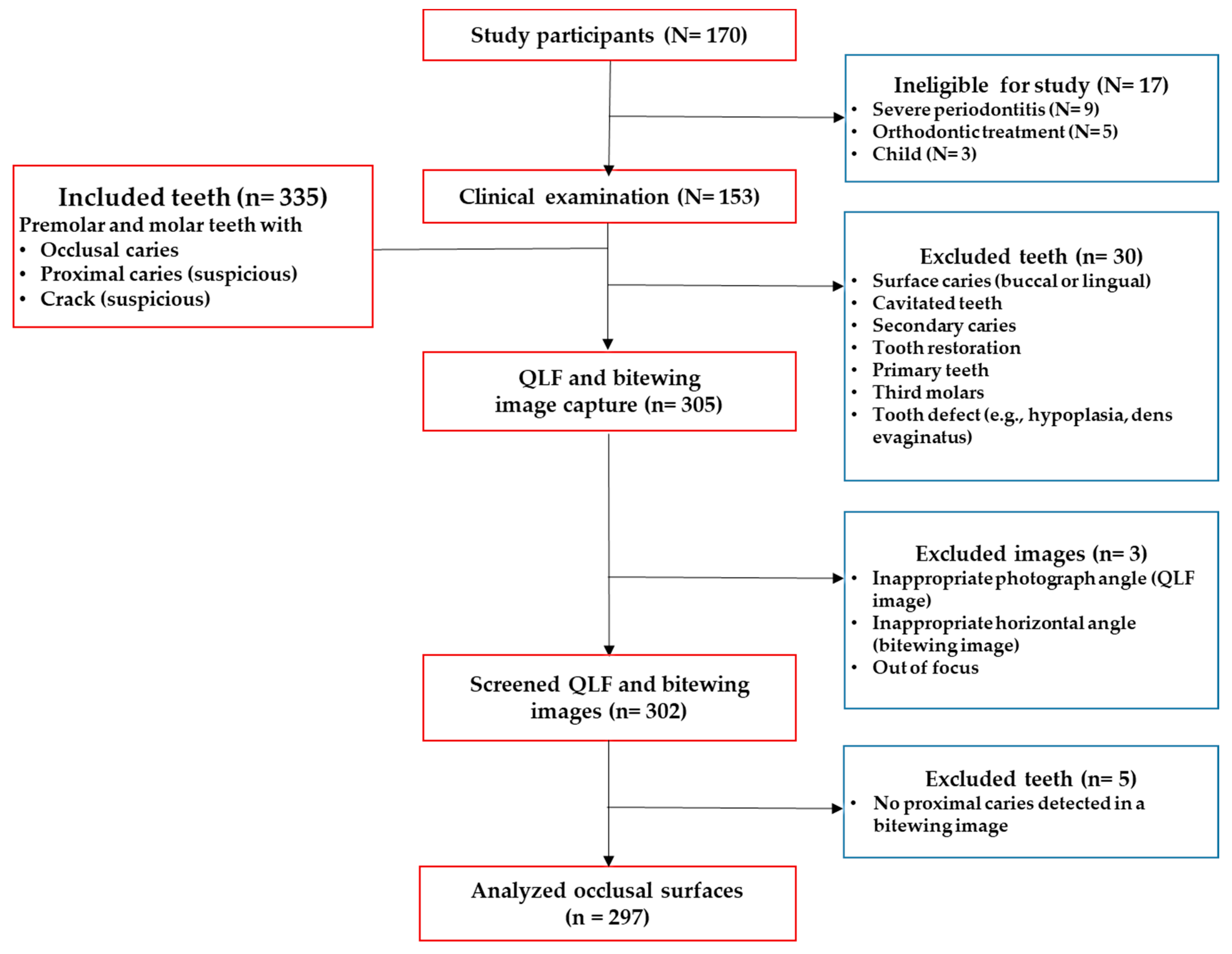
2. Materials and Methods
2.1. Clinical Examination
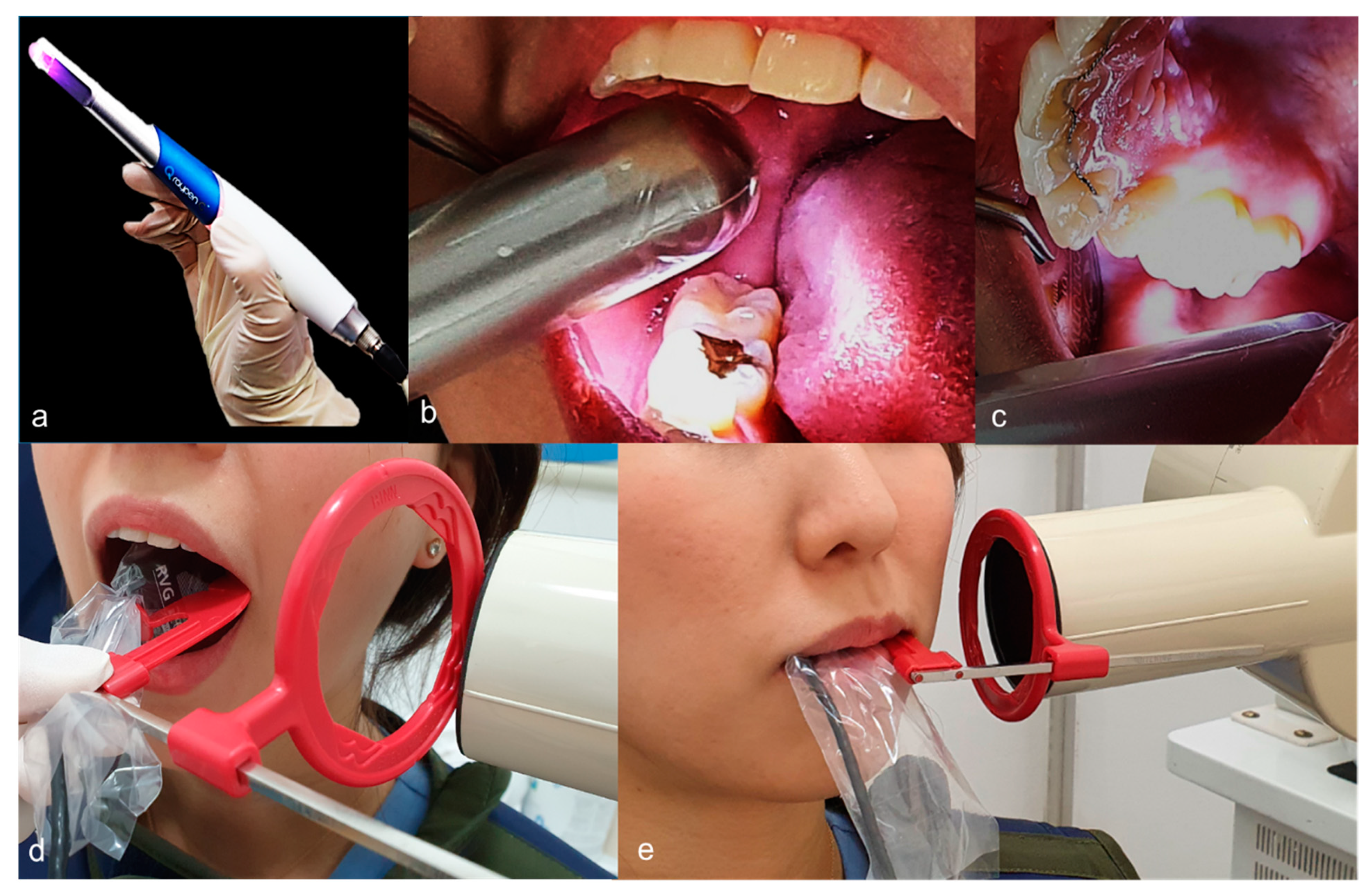
2.2. QLF System
2.3. Bitewing Radiography
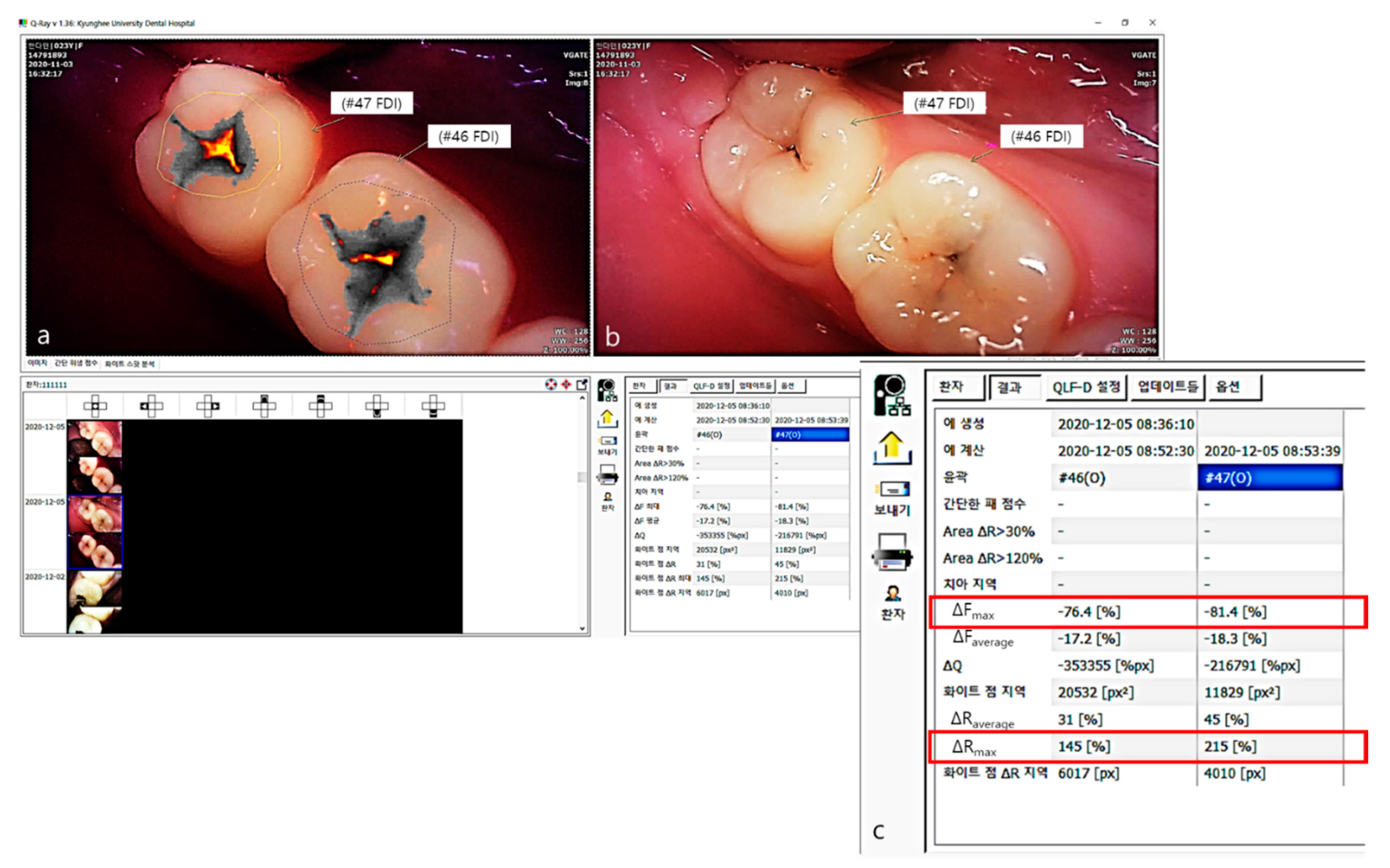
2.4. Scoring of QLF and Bitewing Images
2.5. Analysis of QLF Images Using QA2 Software
2.6. Statistical Analysis
3. Results
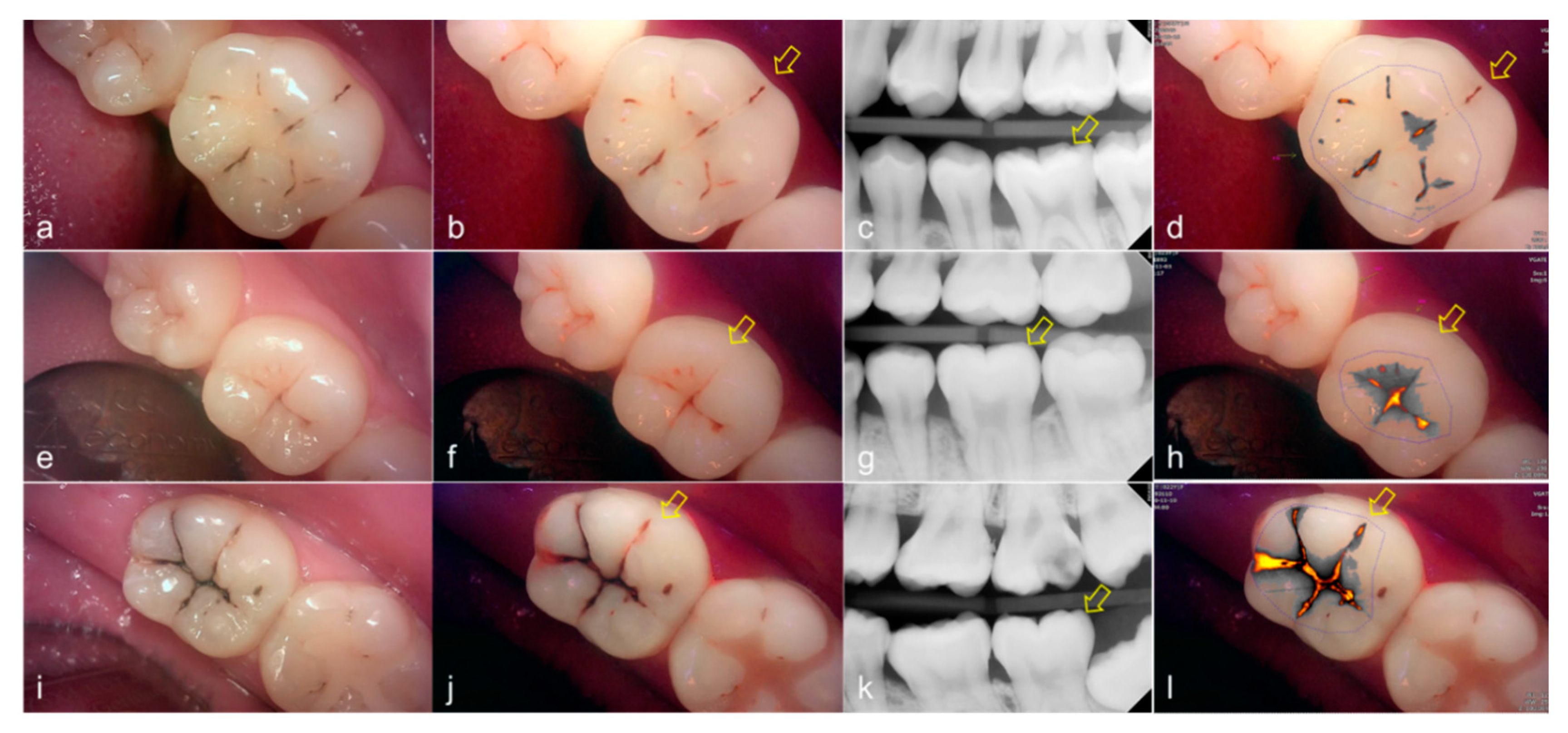
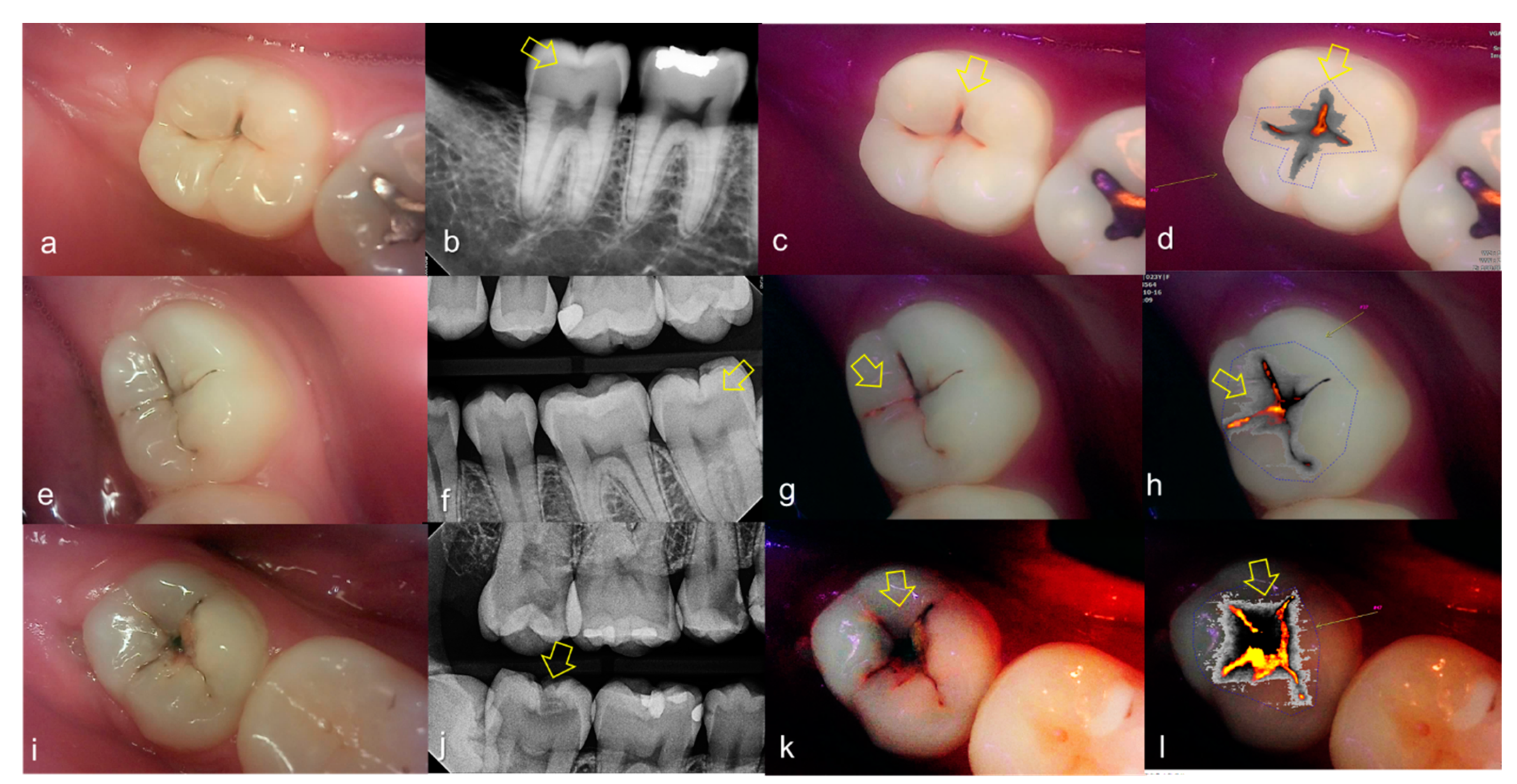
3.1. Occlusal Dental Caries
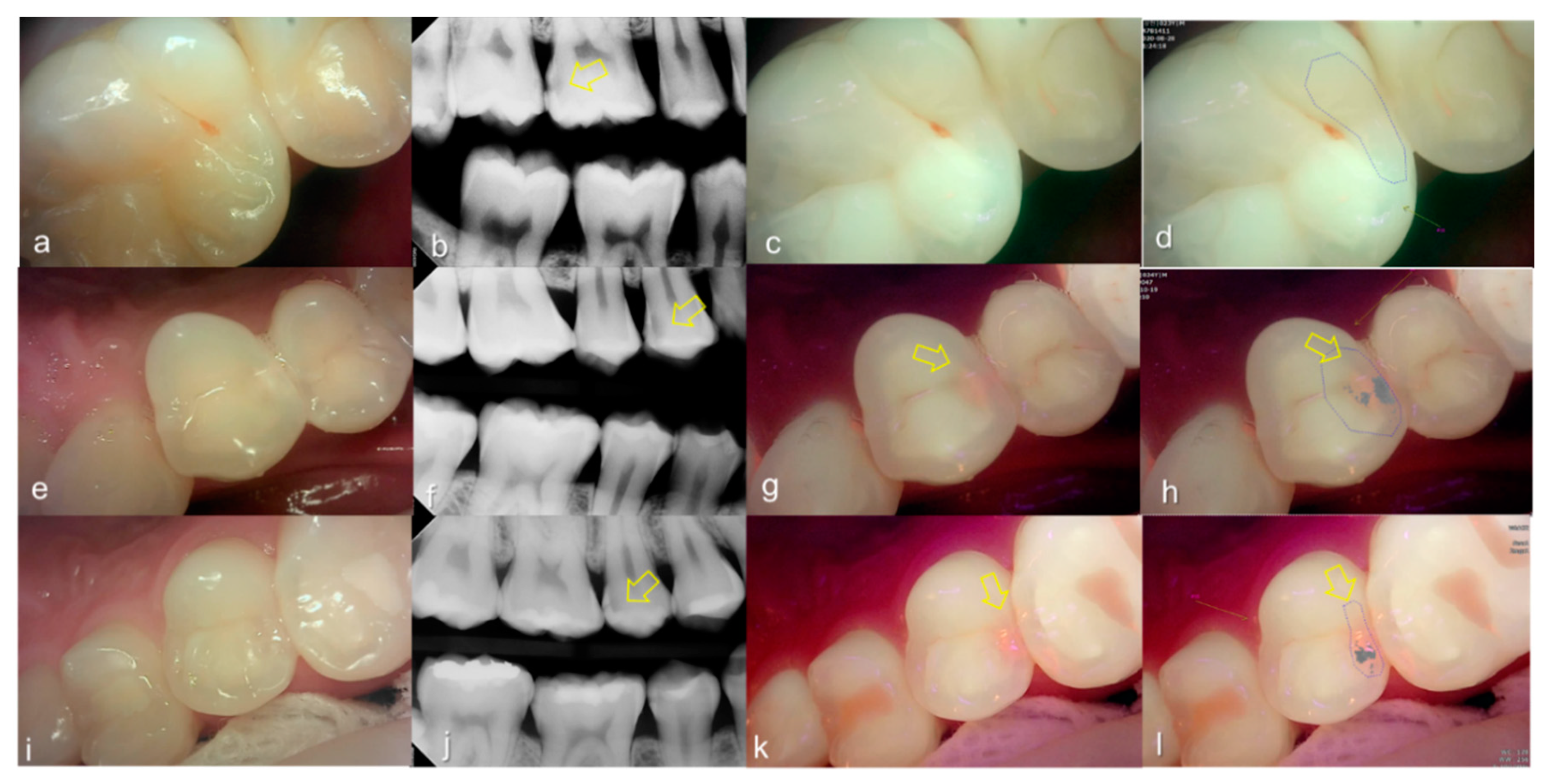
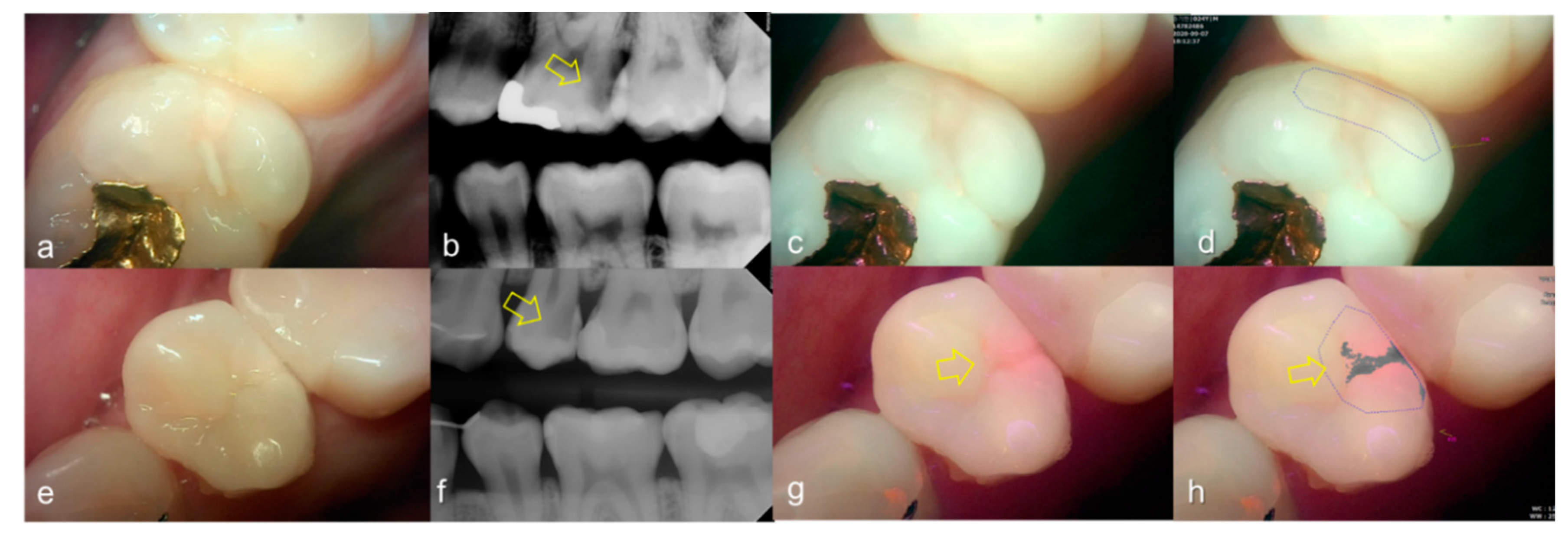
3.2. Proximal Dental Caries
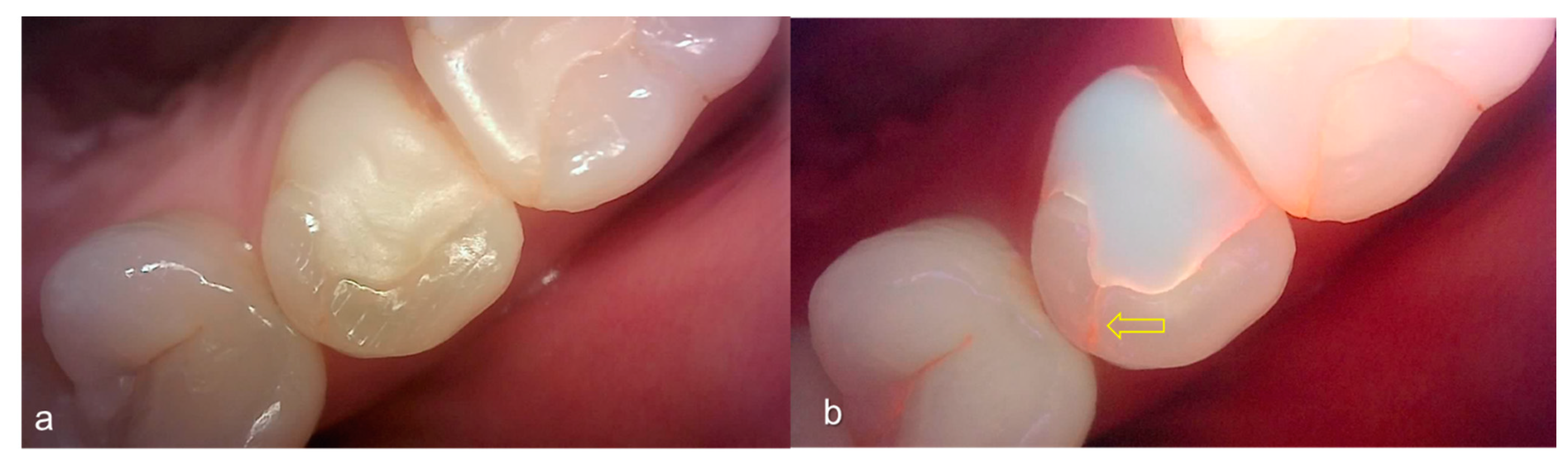
3.3. Crack
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Edman, K.; Öhrn, K.; Nordström, B.; Holmlund, A. Prevalence of dental caries and influencing factors, time trends over a 30-year period in an adult population. Epidemiological studies between 1983 and 2013 in the county of Dalarna, Sweden. Acta Odontol. Scand. 2016, 74, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Park, K.J.; Kroker, T.; Groß, U.; Zimmermann, O.; Krause, F.; Haak, R.; Ziebolz, D. Effectiveness of caries-preventing agents on initial carious lesions within the scope of orthodontic therapy. Korean J. Orthod. 2019, 49, 246–253. [Google Scholar] [CrossRef]
- Ricketts, D.; Kidd, E.; Weerheijm, K.; de Soet, H. Hidden caries: What is it? Does it exist? Does it matter? Int. Dent. J. 1997, 47, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Bader, J.D.; Shugars, D.A.; Bonito, A.J. Systematic reviews of selected dental caries diagnostic and management methods. J. Dent. Educ. 2001, 65, 960–968. [Google Scholar] [CrossRef] [PubMed]
- Cameron, C.E. Crack tooth syndrome. J. Am. Dent. Assoc. 1964, 68, 405–411. [Google Scholar] [CrossRef]
- Ellis, S.G. Incomplete tooth fracture-proposal for a new definition. Br. Dent. J. 2001, 190, 424–428. [Google Scholar] [CrossRef]
- Clark, D.J.; Sheets, C.G.; Paquette, J.M. Definitive diagnosis of early enamel and dentin cracks based on microscopic evaluation. J Esthet Restor Dent 2003, 15, 391–401. [Google Scholar] [CrossRef]
- Stephen, K.W.; Russell, J.I.; Creanor, S.L.; Burchell, C.K. Comparison of fibre optic transillumination with clinical and radiographic caries diagnosis. Community Dent. Oral Epidemiol. 1987, 5, 90–94. [Google Scholar] [CrossRef]
- Peers, A.; Hill, F.J.; Mitropoulos, C.M.; Holloway, P.J. Validity and reproducibility of clinical examination, fibre-optic transillumination, and bite-wing radiology for the diagnosis of small approximal carious lesions: An in vitro study. Caries Res. 1993, 27, 307–311. [Google Scholar] [CrossRef]
- Gao, A.; Cao, D.; Lin, Z. Diagnosis of cracked teeth using cone-beam computed tomography: Literature review and clinical experience. Dentomaxillofac Radiol. 2020, 9, 20200407. [Google Scholar] [CrossRef]
- Pretty, I.A. Caries detection and diagnosis: Novel technologies. J. Dent. 2006, 34, 727–739. [Google Scholar] [CrossRef]
- Pretty, I.A.; Ekstrand, K.R. Detection and monitoring of early caries lesions: A review. Eur. Arch Paediatr Dent. 2016, 17, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Hope, C.K.; de Josselin de Jong, E.; Field, M.R.; Valappil, S.P.; Higham, S.M. Photobleaching of red fluorescence in oral biofilms. J. Periodontal Res. 2011, 46, 228–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amaechi, B.T.; Higham, S.M. Quantitative light-induced fluorescence: A potential tool for general dental assessment. J. Biomed. Opt. 2002, 7, 7–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.S.; Lee, E.S.; Kwon, H.K.L.; Kim, B.I. Monitoring the maturation process of a dental microcosm biofilm using the Quantitative Light-induced Fluorescence-Digital (QLF-D). J. Dent. 2014, 42, 691–696. [Google Scholar] [CrossRef]
- Felix Gomez, G.; Eckert, G.J.; Ferreira Zandona, A. Orange/Red Fluorescence of Active Caries by Retrospective Quantitative Light-Induced Fluorescence Image Analysis. Caries Res. 2016, 50, 295–302. [Google Scholar] [CrossRef] [Green Version]
- Lee, E.S.; Kang, S.M.; Ko, H.Y.; Kwon, H.K.; Kim, B.I. Association between the cariogenicity of a dental microcosm biofilm and its red fluorescence detected by Quantitative Light-induced Fluorescence-Digital (QLF-D). J. Dent. 2013, 41, 1264–1270. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.E.; Kwon, H.K.; Kim, B.I. Recovery percentage of remineralization according to severity of early caries. Am. J. Dent. 2013, 26, 132–136. [Google Scholar]
- Ferreira Zandoná, A.; Ando, M.; Gomez, G.F.; Garcia-Corretjer, M.; Eckert, G.J.; Santiago, E.; Katz, B.P.; Zero, D.T. Longitudinal analyses of early lesions by fluorescence: An observational study. J. Dent. Res. 2013, 92, 84S–89S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira Zandoná, A.; Santiago, E.; Eckert, G.; Fontana, M.; Ando, M.; Zero, D.T. Use of ICDAS combined with quantitative light-induced fluorescence as a caries detection method. Caries Res. 2010, 44, 317–322. [Google Scholar] [CrossRef] [Green Version]
- Van der Veen, M.H.; de Jong, E.D.J. Application of quantitative light-induced fluorescence for assessing early caries lesions. Monogr Oral Sci. 2000, 17, 144–162. [Google Scholar]
- Ismail, A.I.; Sohn, W.; Tellez, M.; Amaya, A.; Sen, A.; Hasson, H.; Pitts, N.B. The international caries detection and assessment system (ICDAS): An integrated system for measuring dental caries. Community Dent. Oral Epidemiol. 2007, 35, 170–178. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.I. QLF concept and clinical implementation. J. Korean Dent. Assoc. 2011, 19, 443–450. [Google Scholar]
- Jung, E.H.; Lee, E.S.; Jung, H.I.; Kang, S.M.; de Jong, E.D.J.; Kim, B.I. Development of a fluorescence-image scoring system for assessing noncavitated occlusal caries. Photodiagn. Photodyn Ther. 2018, 21, 36–42. [Google Scholar] [CrossRef]
- Ekstrand, K.R.; Ricketts, D.N.; Kidd, E.A. Reproducibility and accuracy of three methods for assessment of demineralization depth of the occlusal surface: An in vitro examination. Caries Res. 1997, 31, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Young, D.A.; Nový, B.B.; Zeller, G.G.; Hale, R.; Hart, T.C.; Truelove, E.L. The American Dental Association Caries Classification System for clinical practice: A report of the American Dental Association Council on Scientific Affairs. J. Am. Dent Assoc. 2015, 146, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, K.; Qvist, V.; Thylstrup, A. Light microscope study of the effect of probing in occlusal surfaces. Caries Res. 1987, 21, 368–374. [Google Scholar] [CrossRef] [PubMed]
- van Dorp, C.S.; Exterkate, R.A.; ten Cate, J.M. The effect of dental probing on subsequent enamel demineralization. ASDC J. Dent Child. 1988, 55, 343–347. [Google Scholar]
- Wenzel, A.; Larsen, M.J.; Fejerskov, O. Detection of occlusal caries without cavitation by visual inspection, film radiographs, xeroradiographs, and digitized radiographs. Caries Res. 1991, 25, 365–371. [Google Scholar] [CrossRef]
- Ekstrand, K.R.; Kuzmina, I.; Bjørndal, L.; Thylstrup, A. Relationship between external and histologic features of progressive stages of caries in the occlusal fossa. Caries Res. 1995, 29, 243–250. [Google Scholar] [CrossRef]
- Thomas, M.F.; Ricketts, D.N.; Wilson, R.F. Occlusal caries diagnosis in molar teeth from bitewing and panoramic radiographs. Prim. Dent Care. 2001, 8, 63–69. [Google Scholar] [CrossRef]
- Jun, M.K.; Park, S.W.; Lee, E.S.; Kim, B.R.; Kim, B.I. Diagnosis and management of cracked tooth by quantitative light-induced fluorescence technology. Photodiagnosis Photodyn Ther. 2019, 26, 324–326. [Google Scholar] [CrossRef]
- Lagerweij, M.; van der Veen, M.; Ando, M.; Lukantsova, L.; Stookey, G. The validity and repeatability of three light-induced fluorescence systems: An in vitro study. Caries Res. 1999, 33, 220–226. [Google Scholar] [CrossRef]
- Hafström-Björkman, U.; Sundström, F.; de Jong, E.D.J.; Oliveby, A.; Angmar-Månsson, B. Comparison of laser fluorescence and longitudinal microradiography for quantitative assessment of in vitro enamel caries. Caries Res. 1992, 26, 241–247. [Google Scholar] [CrossRef]
- Amaechi, B.T.; Podoleanu, A.; Higham, S.M.; Jackson, D.A. Correlation of quantitative light-induced fluorescence and optical coherence tomography applied for detection and quantification of early dental caries. J. Biomed. Opt. 2003, 8, 642–647. [Google Scholar] [CrossRef]
- Stookey, G.K. Quantitative light fluorescence: A technology for early monitoring of the caries process. Dent. Clin. N. Am. 2005, 49, 753–770. [Google Scholar] [CrossRef] [PubMed]
- Arnold, W.H.; Gaengler, P.; Kalkutschke, L. Three-dimensional reconstruction of approximal subsurface caries lesions in deciduous molars. Clin. Oral Investig. 1998, 2, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Rayner, J.A.; Southam, J.C. Pulp changes in deciduous teeth associated with deep carious dentine. J. Dent. 1979, 7, 39–42. [Google Scholar] [CrossRef]
- Kim, E.S.; Lee, E.S.; Kang, S.M.; Jung, E.H.; de Jong, E.D.J.; Jung, H.I.; Kim, B.I. A new screening method to detect proximal dental caries using fluorescence imaging. Photodiagnosis Photodyn Ther. 2007, 20, 257–262. [Google Scholar] [CrossRef]
- Milicich, G.; Rainey, J.T. Clinical presentations of stress distribution in teeth and the significance in operative dentistry. Pract. Periodontics Aesthet. Dent. 2000, 12, 695–700. [Google Scholar] [PubMed]
- Liu, H.H.; Sidhu, S.K. Cracked teeth--treatment rationale and case management: Case reports. Quintessence Int. 1995, 26, 485–492. [Google Scholar]
- Çapar, İ.D.; Uysal, B.; Ok, E.; Arslan, H. Effect of the size of the apical enlargement with rotary instruments, single-cone filling, post space preparation with drills, fiber post removal, and root canal filling removal on apical crack initiation and propagation. J. Endod. 2015, 41, 253–256. [Google Scholar] [CrossRef] [PubMed]
- Ehrmann, E.H.; Tyas, M.J. Cracked tooth syndrome: Diagnosis, treatment and correlation between symptoms and post-extraction findings. Aust. Dent. J. 1990, 35, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Lynch, C.D.; McConnell, R.J. The cracked tooth syndrome. J. Can. Dent. Assoc. 2002, 68, 470–475. [Google Scholar] [PubMed]
- Imai, K.; Shimada, Y.; Sadr, A.; Sumi, Y.; Tagami, J. Noninvasive cross-sectional visualization of enamel cracks by optical coherence tomography in vitro. J. Endod. 2012, 38, 1269–1274. [Google Scholar] [CrossRef] [PubMed]
- Kalyan Chakravarthy, P.V.; Telang, L.A.; Nerali, J.; Telang, A. Cracked tooth: A report of two cases and role of cone beam computed tomography in diagnosis. Case Rep. Dent. 2012, 2012, 525364. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Yan, X.B.; Lui, D.G.; Zhang, W.L.; Zhang, Y.; Ma, X.C. Detection of dental root fractures by using cone-beam computed tomography. Dentomaxillofac. Radiol. 2011, 40, 290–298. [Google Scholar] [CrossRef] [Green Version]
- Jun, M.K.; Ku, H.M.; Kim, E.; Kim, H.E.; Kwon, H.K.; Kim, B.I. Detection and Analysis of Enamel Cracks by Quantitative Light-induced Fluorescence Technology. J. Endod. 2016, 42, 500–504. [Google Scholar] [CrossRef]
- Volgenant, C.M.; van der Veen, M.H.; de Soet, J.J.; ten Cate, J.M. Effect of metalloporphyrins on red autofluorescence from oral bacteria. Eur. J. Oral Sci. 2013, 121, 156–161. [Google Scholar] [CrossRef]
- Gmür, R.; Giertsen, E.; van der Veen, M.H.; de Jong, E.D.J.; Jacob, M.; Guggenheim, B. In vitro quantitative light-induced fluorescence to measure changes in enamel mineralization. Clin. Oral Investig. 2006, 10, 187–195. [Google Scholar] [CrossRef] [Green Version]
- Angmar-Månsson, B.; ten Bosch, J.J. Quantitative light-induced fluorescence (QLF): A method for assessment of incipient caries lesions. Dentomaxillofac. Radiol. 2001, 30, 298–307. [Google Scholar] [CrossRef]
- Alammari, M.R.; Smith, P.W.; de Jong, E.D.J.; Higham, S.M. Quantitative light-induced fluorescence (QLF): A tool for early occlusal dental caries detection and supporting decision making in vivo. J. Dent. 2013, 41, 127–132. [Google Scholar] [CrossRef]
- Estai, M.; Bunt, S.; Kanagasingam, Y.; Kruger, E.; Tennant, M. Diagnostic accuracy of teledentistry in the detection of dental caries: A systematic review. J. Evid. Based Dent. Pract. 2016, 16, 161–172. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Score | ADA * Criteria | QLF Criteria | ADA * Criteria | X-ray Criteria | |
|---|---|---|---|---|---|
| Occlusal dental caries | 0 | Sound | No fluorescence loss and no red fluorescence increase in pits and/or fissures | Sound | No radiolucency visible |
| 1 | Initial | Fluorescence loss and red fluorescence present as a line or spot in pits and/or fissures | Initial | Radiolucency visible in the enamel | |
| 2 | Moderate | Fluorescence loss and red fluorescence glow extending around pits and fissures | Moderate | Radiolucency in the dentine but restricted to the outer 1/3 of the dentine | |
| 3 | Advanced | Red fluorescence glow extending around pits and fissures and a dark shadow from dentin present | Advanced | Radiolucency extending to the middle 1/3 of the dentine | |
| Proximal dental caries | 0 | Sound or Initial | No fluorescence loss and no red fluorescence increase in occlusal surface (mesial or distal side) | Sound | |
| 1 | Moderate | Fluorescence loss and red fluorescence present in occlusal surface (mesial or distal side) | Initial | Radiolucency visible in the enamel | |
| 2 | Advanced | Fluorescence loss and red fluorescence glow extending around occlusal surface (mesial or distal side) | Radiolucency in the dentine but restricted to the outer 1/3 of the dentine | ||
| 3 | Moderate | Radiolucency extending to the middle 1/3 of the dentine | |||
| 4 | Advanced | Radiolucency in the pulpal 1/3 of the dentine | |||
| Score | QLF Criteria | Visual Criteria | |||
| Crack | 0 | No fluorescence loss and no red fluorescence increase in crack site | No detectable crack line | ||
| 1 | Fluorescence loss and red fluorescence present as a line in crack site | Ambiguous detectable crack line | |||
| 2 | Fluorescence loss and red fluorescence glow extending around crack site | Distinct detectable crack line |
| Occlusal Dental Caries Score (QLF Criteria) | QLF Parameters | |||
|---|---|---|---|---|
| |ΔFmax| | p-Value | ΔRmax | p-Value | |
| 1 | 50.67 ab | <0.0001 1 | 49.34 a | <0.0001 1 |
| 2 | 63.69 ac | 105.65 b | ||
| 3 | 77.42 bc | 221.87 ab | ||
| Proximal Dental Caries Score (X-ray Criteria) | QLF Parameters | |||
| |ΔFmax| | p-Value | ΔRmax | p-Value | |
| 1 | 3.12 ab | <0.0001 1 | 0.00 | 0.0083 1 |
| 2 | 7.13 c | 0.00 | ||
| 3 | 17.64 ac | 16.61 | ||
| 4 | 19.56 b | 12.80 | ||
| Crack Score (QLF Criteria) | QLF Parameters | |||
| |ΔFmax| | p-Value | ΔRmax | p-Value | |
| 1 | 19.84 | 0.010 2 | 22.44 | 0.011 2 |
| 2 | 40.24 | 67.60 | ||
| Total Number of Teeth | Cut-Off Value | Sensitivity | Specificity | AUROC | ||
|---|---|---|---|---|---|---|
| Occlusal dental caries | 177 | |ΔFmax| | 59.85 | 0.76 | 0.74 | 0.84 |
| ΔRmax | 74.50 | 0.83 | 0.82 | 0.91 | ||
| Proximal dental caries | 91 | |ΔFmax| | 5.95 | 0.74 | 0.73 | 0.81 |
| ΔRmax | 0.00 | 0.83 | 0.00 | 0.59 | ||
| Crack | 29 | |ΔFmax| | 20.80 | 0.85 | 0.67 | 0.83 |
| ΔRmax | 39.00 | 0.75 | 0.78 | 0.82 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, S.H.; Lee, S.R.; Choi, J.Y.; Choi, Y.S.; Kim, S.H.; Yoon, H.C.; Nelson, G. Detection of Dental Caries and Cracks with Quantitative Light-Induced Fluorescence in Comparison to Radiographic and Visual Examination: A Retrospective Case Study. Sensors 2021, 21, 1741. https://0-doi-org.brum.beds.ac.uk/10.3390/s21051741
Oh SH, Lee SR, Choi JY, Choi YS, Kim SH, Yoon HC, Nelson G. Detection of Dental Caries and Cracks with Quantitative Light-Induced Fluorescence in Comparison to Radiographic and Visual Examination: A Retrospective Case Study. Sensors. 2021; 21(5):1741. https://0-doi-org.brum.beds.ac.uk/10.3390/s21051741
Chicago/Turabian StyleOh, Song Hee, Sae Rom Lee, Jin Young Choi, Yong Suk Choi, Seong Hun Kim, Hong Cheol Yoon, and Gerald Nelson. 2021. "Detection of Dental Caries and Cracks with Quantitative Light-Induced Fluorescence in Comparison to Radiographic and Visual Examination: A Retrospective Case Study" Sensors 21, no. 5: 1741. https://0-doi-org.brum.beds.ac.uk/10.3390/s21051741