
Soft System Based on Fiber Bragg Grating Sensor for Loss of Resistance Detection during Epidural Procedures: In Silico and In Vivo Assessment †

 ,
,  ,
, 
 , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Soft System for LOR Detection: Principle of Work, Design, Manufacturing and Metrological Assessment
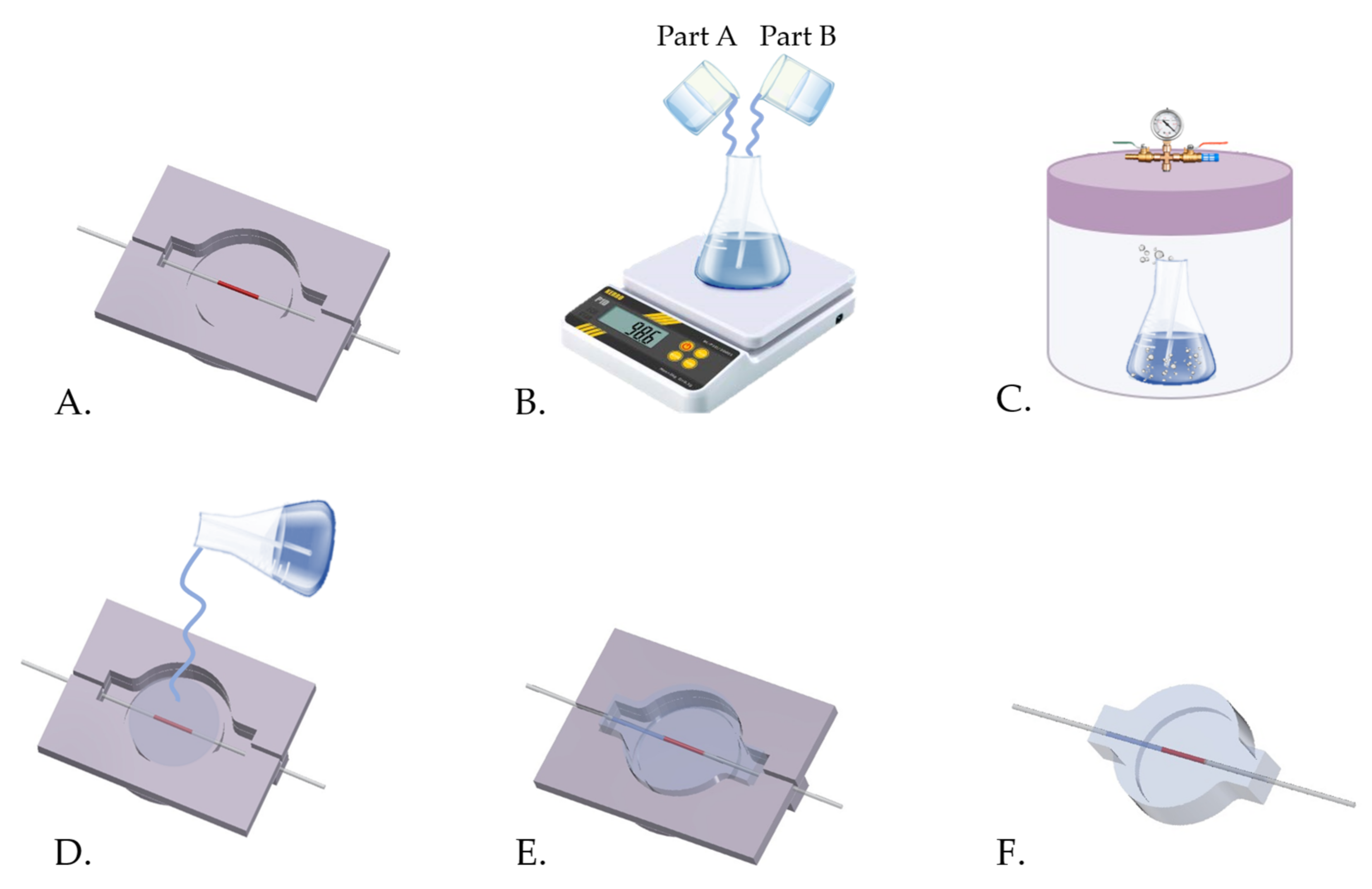
2.1. Design and Manufacturing
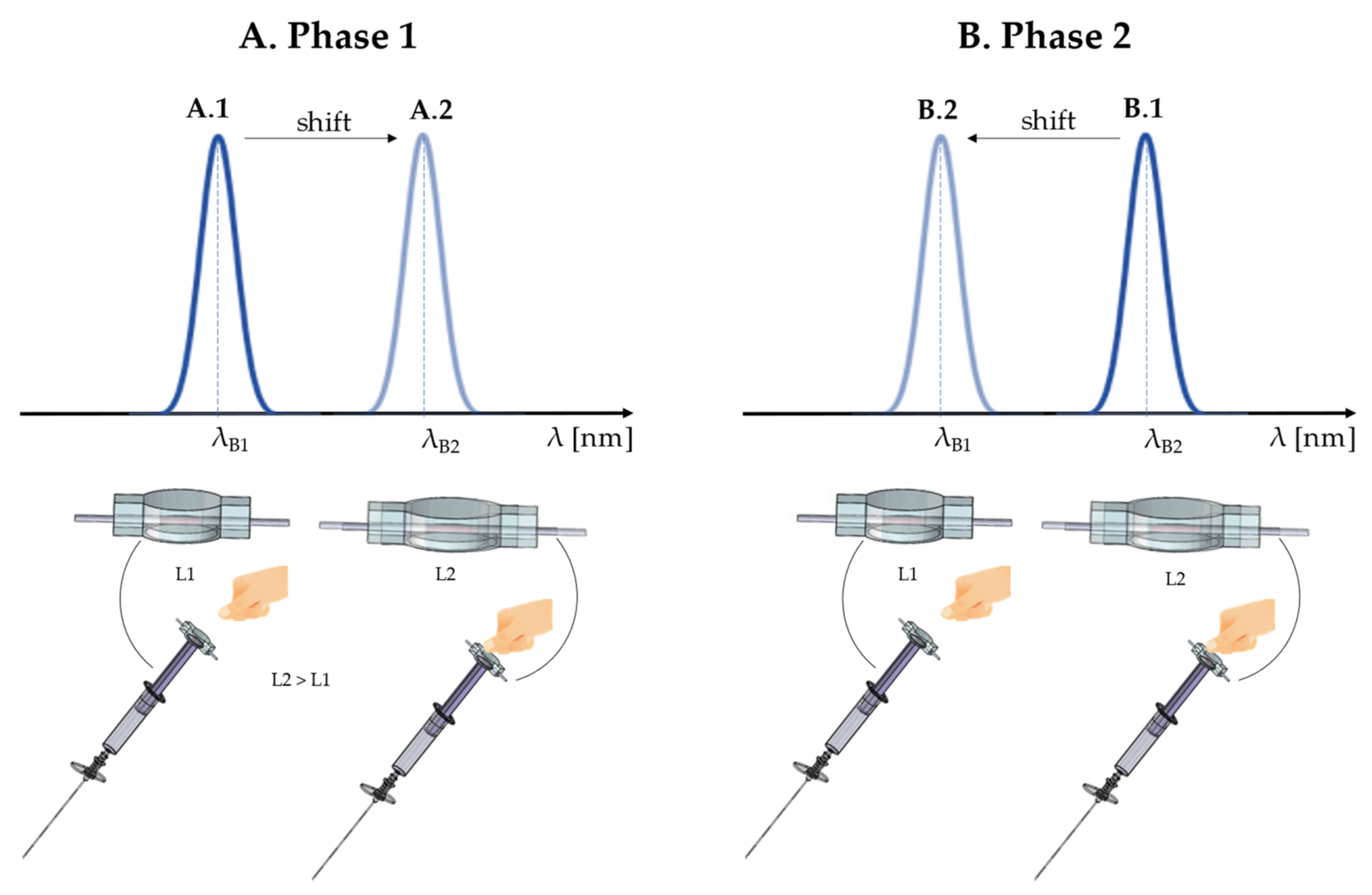
2.2. Soft System Based on Fiber Bragg Grating Sensor: Working Principle

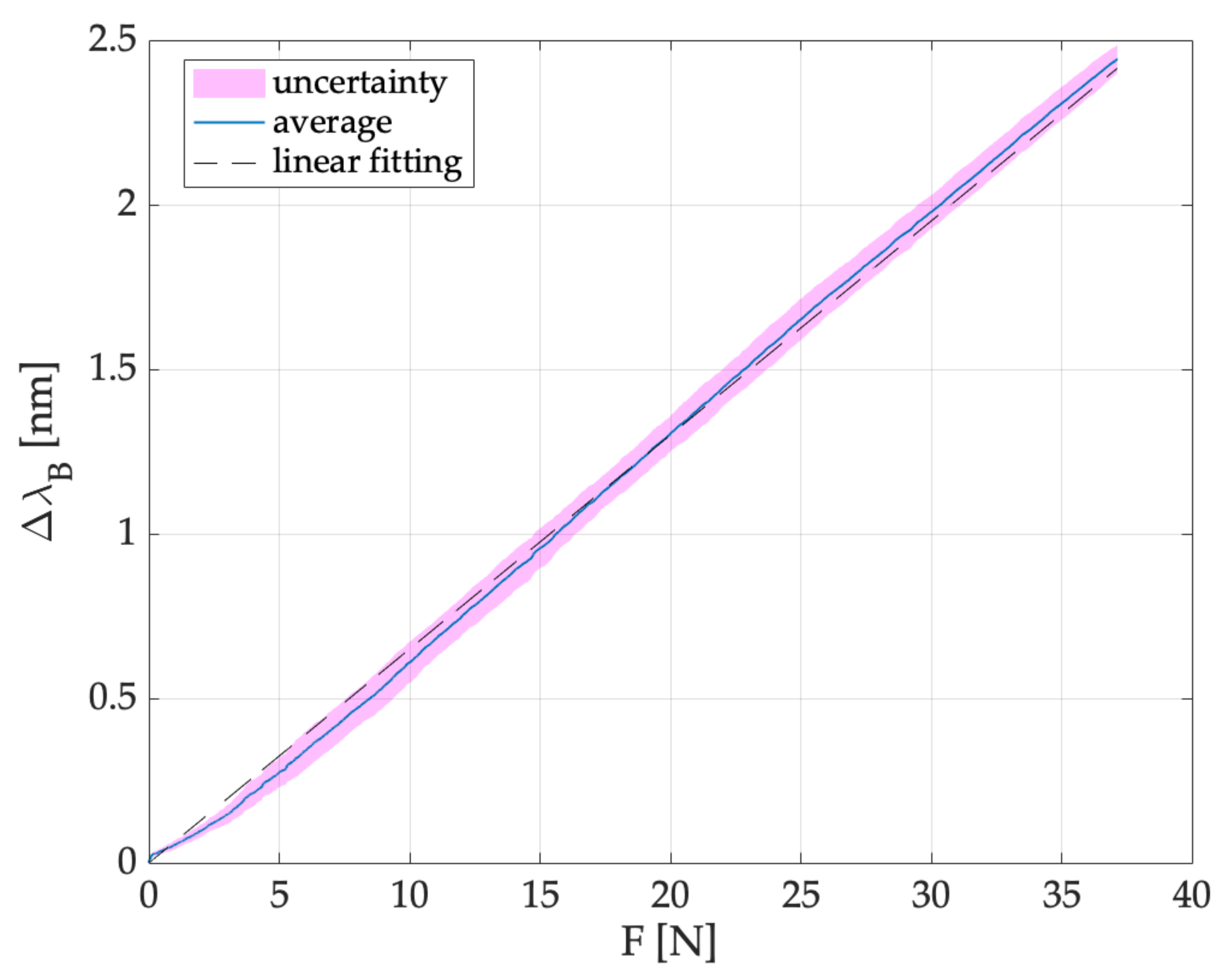
2.3. Metrological Characterization
3. Test and Feasibility Assessment of the Soft System for LOR Detection
3.1. In Silico Experiments
Data Analysis and Results
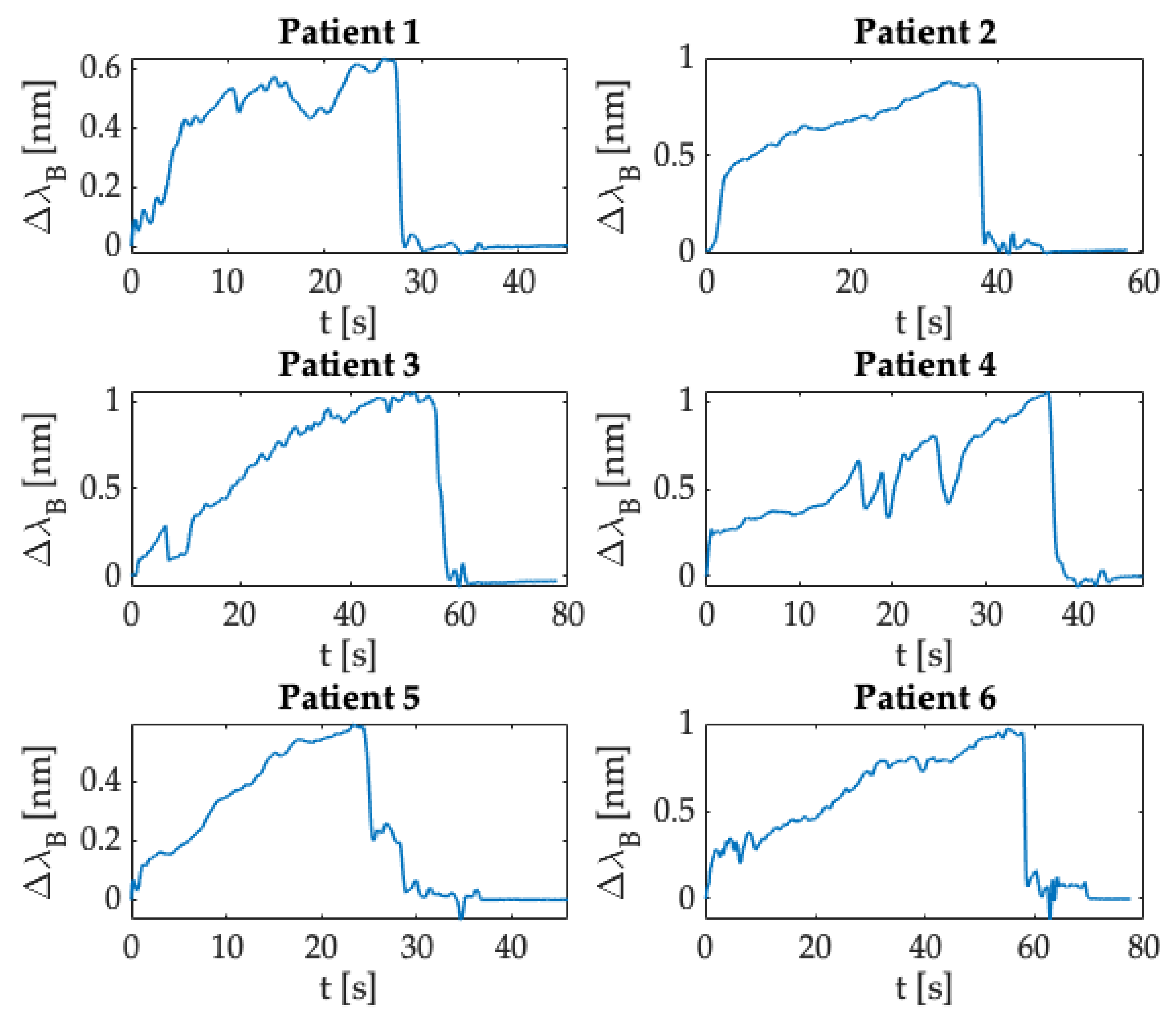
- (1)
- A first phase in which the ΔλB = 0 because the user was not yet pressing on the syringe’s plunger.
- (2)
- A quick increase in ΔλB when the user pressed on the syringe’s plunger.
- (3)
- A phase in which the ΔλB value exceeded a specified threshold when the user pushed the SS to advance the Tuohy needle through the different layers mimicking the anatomical soft tissues. The threshold value of ΔλB was different in each test according to the force applied by the user on the SS.
- (4)
- An abrupt downturn in the value of ΔλB due to the LOR corresponding to the transition from the material mimicking the ligamentum flavum to replacing the ES.
- (5)
- A final phase in which the ΔλB returned to zero at the end of the epidural puncture.
3.2. In Vivo Trials
Data Analysis and Results
4. Discussions and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Curatolo, M.; Bogduk, N. Pharmacologic Pain Treatment of Musculoskeletal Disorders: Current Perspectives and Future Prospects. Clin. J. Pain 2001, 17, 25–32. [Google Scholar] [CrossRef] [Green Version]
- Clinical Section. Proc. R. Soc. Med. 1953, 46, 713–716. [CrossRef] [Green Version]
- Hoy, D.; Brooks, P.; Blyth, F.; Buchbinder, R. The Epidemiology of low back pain. Best Pr. Res. Clin. Rheumatol. 2010, 24, 769–781. [Google Scholar] [CrossRef]
- White, A.H.; Derby, R.; Wynne, G. Epidural Injections for the Diagnosis and Treatment of Low-Back Pain. Spine 1980, 5, 78–86. [Google Scholar] [CrossRef]
- Anim-Somuah, M.; Smyth, R.M.; Cyna, A.M.; Cuthbert, A. Epidural versus non-epidural or no analgesia for pain management in labour. Cochrane Database Syst. Rev. 2018, 5, CD000331. [Google Scholar] [CrossRef]
- Lally, J.E.; Murtagh, M.J.; MacPhail, S.; Thomson, R. More in hope than expectation: A systematic review of women’s expectations and experience of pain relief in labour. BMC Med. 2008, 6, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, S.; Rosenfeld, J.A. The Effect of Epidural Anesthesia on the Length of Labor. Obstet. Gynecol. Surv. 1995, 50, 770–771. [Google Scholar] [CrossRef]
- Turnbull, D.K.; Shepherd, D. Post-dural puncture headache: Pathogenesis, prevention and treatment. Br. J. Anaesth. 2003, 91, 718–729. [Google Scholar] [CrossRef] [Green Version]
- Furness, G.; Reilly, M.P.; Kuchi, S. An evaluation of ultrasound imaging for identificationof lumbar intervertebral level. Anaesthesia 2002, 57, 277–280. [Google Scholar] [CrossRef]
- Kim, W.J.; Kim, T.H.; Shin, H.Y.; Kang, H.; Baek, C.W.; Jung, Y.H.; Woo, Y.-C.; Kim, J.Y.; Koo, G.H.; Park, S.G. Fluoroscope guided epidural needle insertioin in midthoracic region: Clinical evaluation of Nagaro’s method. Korean J. Anesthesiol. 2012, 62, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Chiu, S.C.; Bristow, S.J.; Gofeld, M. Near-Infrared Tracking System for Epidural Catheter Placement. Reg. Anesth. Pain Med. 2012, 37, 354–356. [Google Scholar] [CrossRef] [PubMed]
- Elsharkawy, H.; Sonny, A.; Chin, K.J. Localization of epidural space: A review of available technologies. J. Anaesthesiol. Clin. Pharmacol. 2017, 33, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.-C.; Chen, K.-B.; Chang, C.-S.; Wu, K.-C.; Liu, Y.-C.; Chen, C.-C.; Wu, R.S.-C. A ‘membrane in syringe’ technique that allows identification of the epidural space with saline while avoids injection of air into the epidural space. Acta Anaesthesiol. Sin. 2002, 40, 55–60. [Google Scholar]
- Sawada, A.; Kii, N.; Yoshikawa, Y.; Yamakage, M. Epidrum®: A new device to identify the epidural space with an epidural Tuohy needle. J. Anesth. 2011, 26, 292–295. [Google Scholar] [CrossRef] [PubMed]
- Carabuena, J.M.; Mitani, A.M.; Liu, X.; Kodali, B.S.; Tsen, L.C. The Learning Curve Associated with the Epidural Technique Using the Episure™ AutoDetect™ Versus Conventional Glass Syringe. Anesth. Analg. 2013, 116, 145–154. [Google Scholar] [CrossRef]
- Lechner, T.J.M.; Van Wijk, M.G.F.; Maas, A.J.J. Clinical results with a new acoustic device to identify the epidural space. Anaesthesia 2002, 57, 768–772. [Google Scholar] [CrossRef]
- Kim, S.W.; Kim, Y.M.; Kim, S.H.; Chung, M.H.; Choi, Y.R.; Choi, E.M. Comparison of loss of resistance technique between Epidrum® and conventional method for identifying the epidural space. Korean J. Anesthesiol. 2012, 62, 322–326. [Google Scholar] [CrossRef]
- Capogna, G.; Camorcia, M.; Coccoluto, A.; Micaglio, M.; Velardo, M. Experimental validation of the CompuFlo® epidural controlled system to identify the epidural space and its clinical use in difficult obstetric cases. Int. J. Obstet. Anesth. 2018, 36, 28–33. [Google Scholar] [CrossRef]
- Tesei, M.; Saccomandi, P.; Massaroni, C.; Quarta, R.; Carassiti, M.; Schena, E.; Setola, R. A cost-effective, non-invasive system for pressure monitoring during epidural needle insertion: Design, development and bench tests. In Proceedings of the 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 194–197. [Google Scholar] [CrossRef]
- Carassiti, M.; Mattei, A.; Quarta, R.; Massaroni, C.; Saccomandi, P.; Tesei, M.; Setola, R.; Schena, E. A New Pressure Guided Management Tool for Epidural Space Detection: Feasibility Assessment on a Simulator. Artif. Organs 2017, 41, E320–E325. [Google Scholar] [CrossRef]
- Carassiti, M.; Cataldo, R.; Formica, D.; Massaroni, C.; De Filippis, A.; Palermo, P.; Di Tocco, J.; Setola, R.; Valenti, C.; Schena, E. Anew pressure guided management tool for epidural space detection: Feasibility assessment in a clinical scenario. Minerva Anestesiol. 2020, 86, 736–741. [Google Scholar] [CrossRef]
- Baldini, F.; Giannetti, A.; Mencaglia, A.A.; Trono, C. Fiber Optic Sensors for Biomedical Applications. Curr. Anal. Chem. 2008, 4, 378–390. [Google Scholar] [CrossRef]
- Mishra, V.; Singh, N.; Tiwari, U.; Kapur, P. Fiber grating sensors in medicine: Current and emerging applications. Sens. Actuators A Phys. 2011, 167, 279–290. [Google Scholar] [CrossRef]
- Presti, D.L.; Massaroni, C.; Leitao, C.S.J.; Domingues, M.D.F.; Sypabekova, M.; Barrera, D.; Floris, I.; Massari, L.; Oddo, C.M.; Sales, S.; et al. Fiber Bragg Gratings for Medical Applications and Future Challenges: A Review. IEEE Access 2020, 8, 156863–156888. [Google Scholar] [CrossRef]
- Ambastha, S.; Umesh, S.; Dabir, S.; Asokan, S. Spinal needle force monitoring during lumbar puncture using fiber Bragg grating force device. J. Biomed. Opt. 2016, 21, 117002. [Google Scholar] [CrossRef] [PubMed]
- Carotenuto, B.; Micco, A.; Ricciardi, A.; Amorizzo, E.; Mercieri, M.; Cutolo, A.; Cusano, A. Lab in a needle for epidural space identification. In Proceedings of the 6th European Workshop on Optical Fibre Sensors (EWOFS2016), Limerick, Ireland, 31 May–3 June 2016; p. 99161. [Google Scholar] [CrossRef]
- Carotenuto, B.; Micco, A.; Ricciardi, A.; Amorizzo, E.; Mercieri, M.; Cutolo, A.; Cusano, A. Optical Guidance Systems for Epidural Space Identification. IEEE J. Sel. Top. Quantum Electron. 2016, 23, 371–379. [Google Scholar] [CrossRef]
- Carotenuto, B.; Ricciardi, A.; Micco, A.; Amorizzo, E.; Mercieri, M.; Cutolo, A.; Cusano, A. Optical fiber technology enables smart needles for epidurals: An in-vivo swine study. Biomed. Opt. Express 2019, 10, 1351–1364. [Google Scholar] [CrossRef] [PubMed]
- De Tommasi, F.; Presti, D.L.; Massaroni, C.; Schena, E.; Carassiti, M. FBG-based System for Loss of Resistance Detection During Epidural Injections. In Proceedings of the 2021 IEEE International Workshop on Metrology for Industry 4.0 & IoT (MetroInd4. 0&IoT), Roma, Italy, 7–9 June 2021; pp. 172–176. [Google Scholar] [CrossRef]
- Erdogan, T. Fiber grating spectra. J. Light. Technol. 1997, 15, 1277–1294. [Google Scholar] [CrossRef] [Green Version]
- Rao, Y.-J. In-fibre Bragg grating sensors. Meas. Sci. Technol. 1997, 8, 355–375. [Google Scholar] [CrossRef]
- Schena, E.; Massaroni, C.; Iacoponi, S.; Berte, A.; Leone, A.; Musicco, S.; Formica, D.; Raiano, L.; Carassiti, M.; Palermo, P.; et al. Force monitoring during Peripheral Nerve Blocks: Design and feasibility assessment of a new noninvasive system. In Proceedings of the 2019 II Workshop on Metrology for Industry 4.0 and IoT (MetroInd4.0&IoT), Naples, Italy, 4–6 June 2019; pp. 154–157. [Google Scholar] [CrossRef]
- Fyneface-Ogan, S. Anatomy and Clinical Importance of the Epidural Space. Epidural Analg. Curr. Views Approaches 2012, 12, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Segal, S.; Arendt, K.W. A Retrospective Effectiveness Study of Loss of Resistance to Air or Saline for Identification of the Epidural Space. Anesth. Analg. 2010, 110, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Ruppen, W.; Derry, S.; McQuay, H.; Moore, R.A. Incidence of Epidural Hematoma, Infection, and Neurologic Injury in Obstetric Patients with Epidural Analgesia/Anesthesia. J. Am. Soc. Anesthesiol. 2006, 105, 394–399. [Google Scholar] [CrossRef]
- Al-Fakih, E.; Abu Osman, N.A.; Adikan, F.R.M. The Use of Fiber Bragg Grating Sensors in Biomechanics and Rehabilitation Applications: The State-of-the-Art and Ongoing Research Topics. Sensors 2012, 12, 12890–12926. [Google Scholar] [CrossRef]
- Roesthuis, R.J.; Janssen, S.; Misra, S. On using an array of fiber Bragg grating sensors for closed-loop control of flexible minimally invasive surgical instruments. In Proceedings of the 2013 IEEE/Rsj International Conference on Intelligent Robots and Systems, Tokyo, Japan, 3–7 November 2013; pp. 2545–2551. [Google Scholar] [CrossRef]
- De Tommasi, F.; Massaroni, C.; Carnevale, A.; Presti, D.L.; De Vita, E.; Iadicicco, A.; Faiella, E.; Grasso, R.F.; Longo, U.G.; Campopiano, S.; et al. Fiber Bragg Grating Sensors for Temperature Monitoring During Thermal Ablation Procedure: Experimental Assessment of Artefact Caused by Respiratory Movements. IEEE Sensors J. 2021, 21, 13342–13349. [Google Scholar] [CrossRef]
- Dziuda, L.; Skibniewski, F.W.; Krej, M.; Lewandowski, J. Monitoring Respiration and Cardiac Activity Using Fiber Bragg Grating-Based Sensor. IEEE Trans. Biomed. Eng. 2012, 59, 1934–1942. [Google Scholar] [CrossRef] [PubMed]
- Massari, L.; Schena, E.; Massaroni, C.; Saccomandi, P.; Menciassi, A.; Sinibaldi, E.; Oddo, C.M. A Machine-Learning-Based Approach to Solve Both Contact Location and Force in Soft Material Tactile Sensors. Soft Robot. 2020, 7, 409–420. [Google Scholar] [CrossRef]











Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Tommasi, F.; Lo Presti, D.; Virgili, F.; Massaroni, C.; Schena, E.; Carassiti, M. Soft System Based on Fiber Bragg Grating Sensor for Loss of Resistance Detection during Epidural Procedures: In Silico and In Vivo Assessment. Sensors 2021, 21, 5329. https://0-doi-org.brum.beds.ac.uk/10.3390/s21165329
De Tommasi F, Lo Presti D, Virgili F, Massaroni C, Schena E, Carassiti M. Soft System Based on Fiber Bragg Grating Sensor for Loss of Resistance Detection during Epidural Procedures: In Silico and In Vivo Assessment. Sensors. 2021; 21(16):5329. https://0-doi-org.brum.beds.ac.uk/10.3390/s21165329
Chicago/Turabian StyleDe Tommasi, Francesca, Daniela Lo Presti, Francesca Virgili, Carlo Massaroni, Emiliano Schena, and Massimiliano Carassiti. 2021. "Soft System Based on Fiber Bragg Grating Sensor for Loss of Resistance Detection during Epidural Procedures: In Silico and In Vivo Assessment" Sensors 21, no. 16: 5329. https://0-doi-org.brum.beds.ac.uk/10.3390/s21165329