
A Data-Driven Approach to Physical Fatigue Management Using Wearable Sensors to Classify Four Diagnostic Fatigue States

 , , , and
, , , and
Abstract
:1. Introduction
2. Related Works
3. Materials and Methods
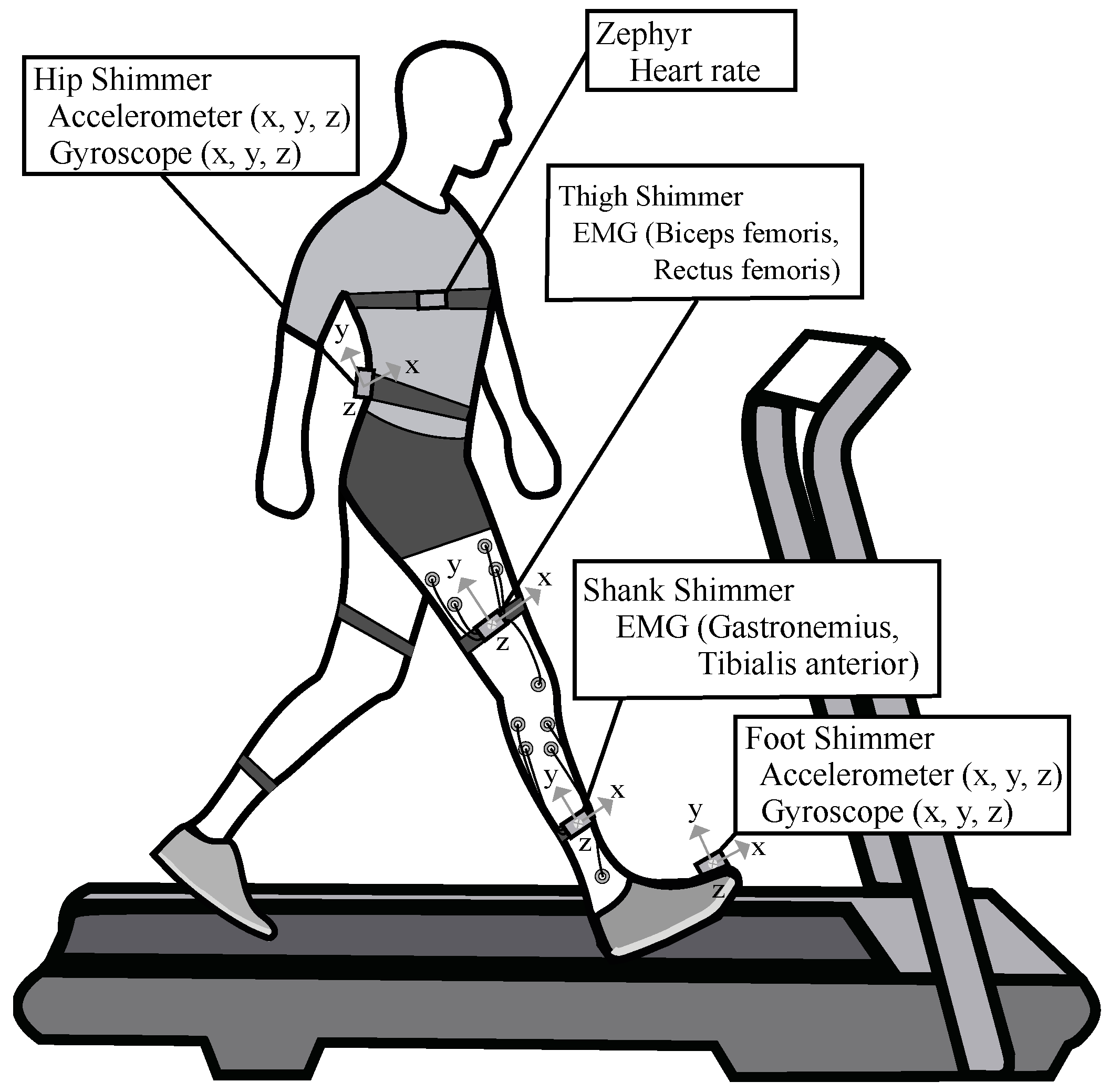
3.1. Experimental Setup
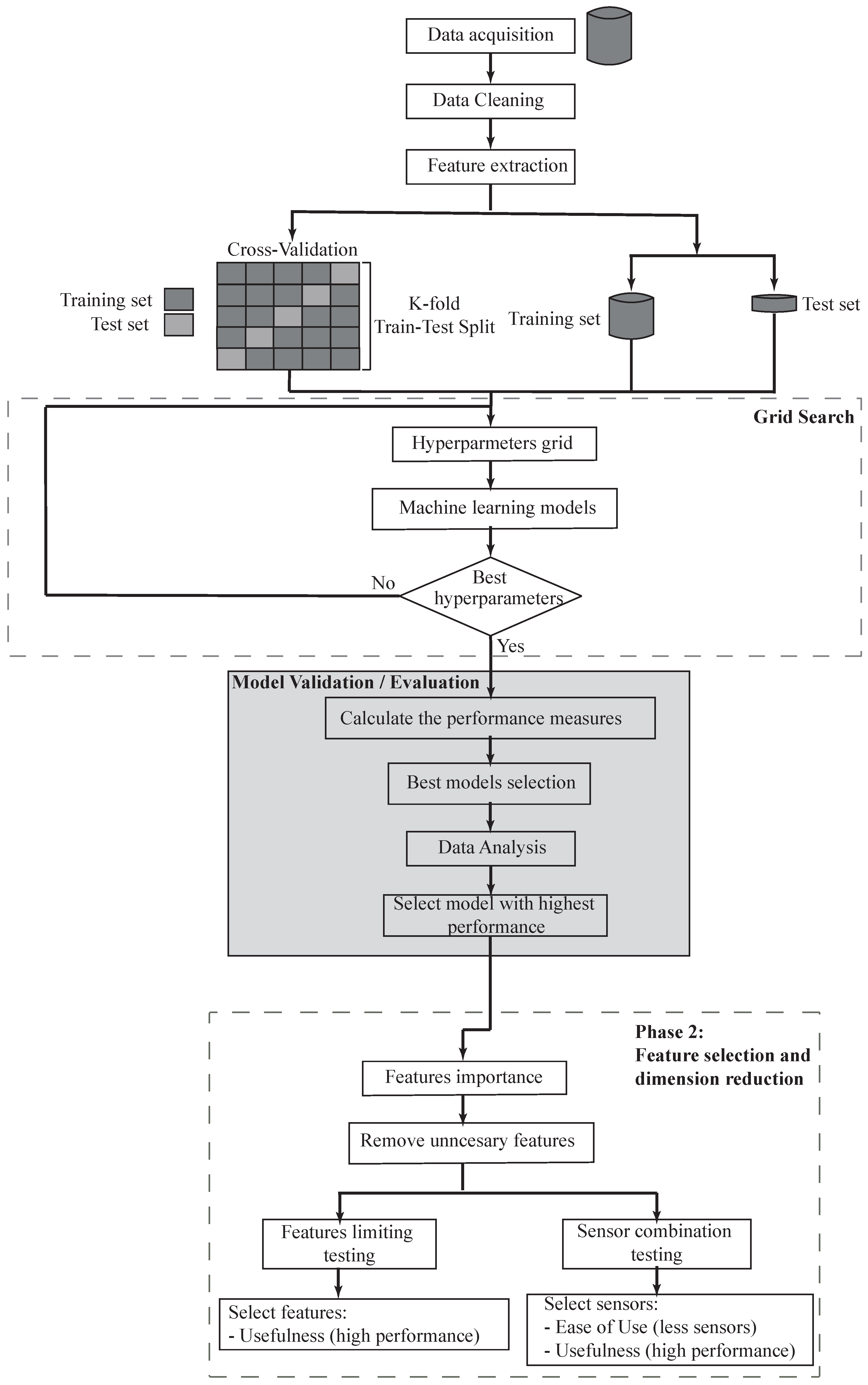
3.2. Proposed Approach for Fatigue Classifier
3.3. Phase 1: Fatigue Detection
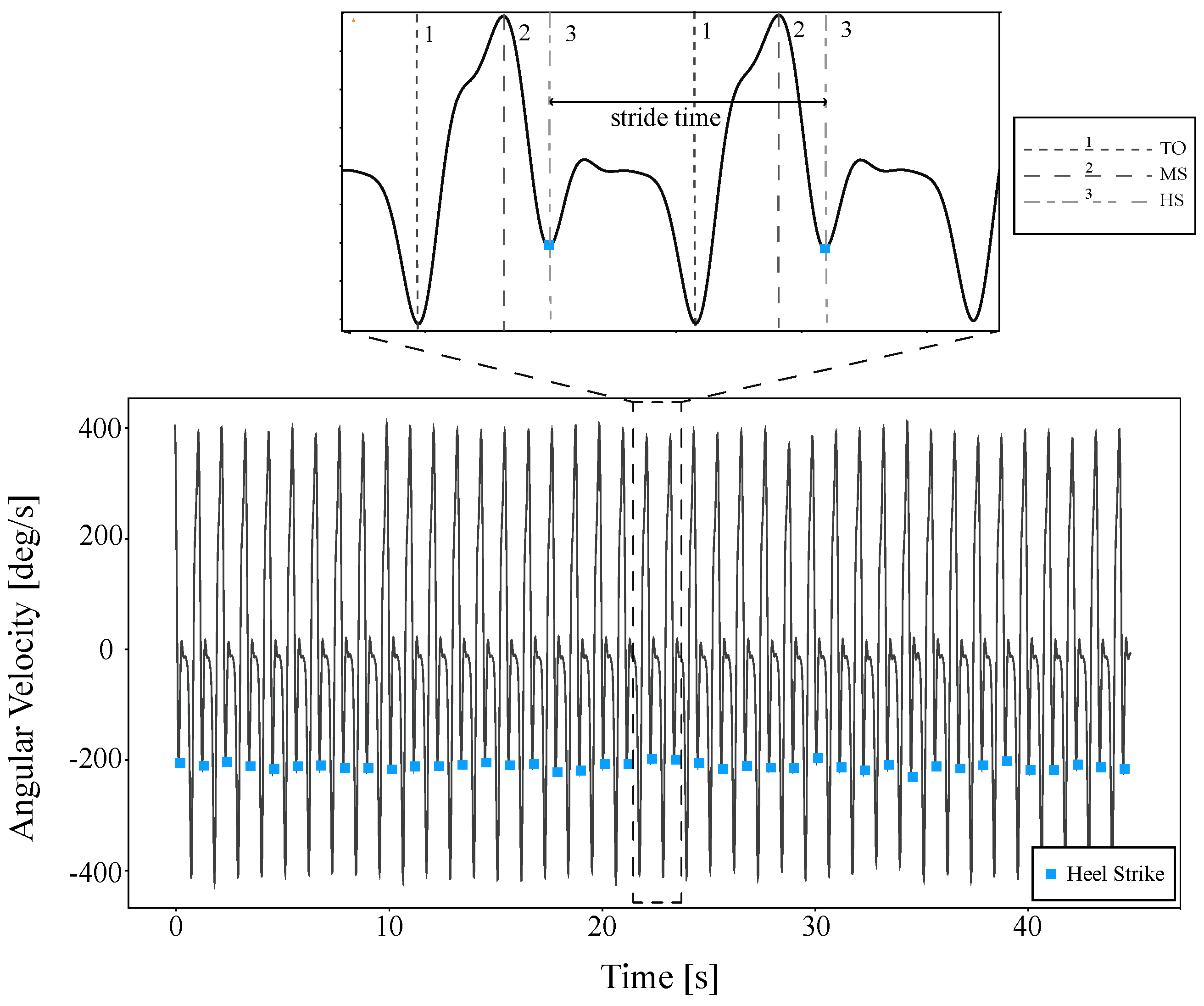
3.3.1. Data Preprocessing
3.3.2. Model Construction and Validation
3.3.3. Data Analysis
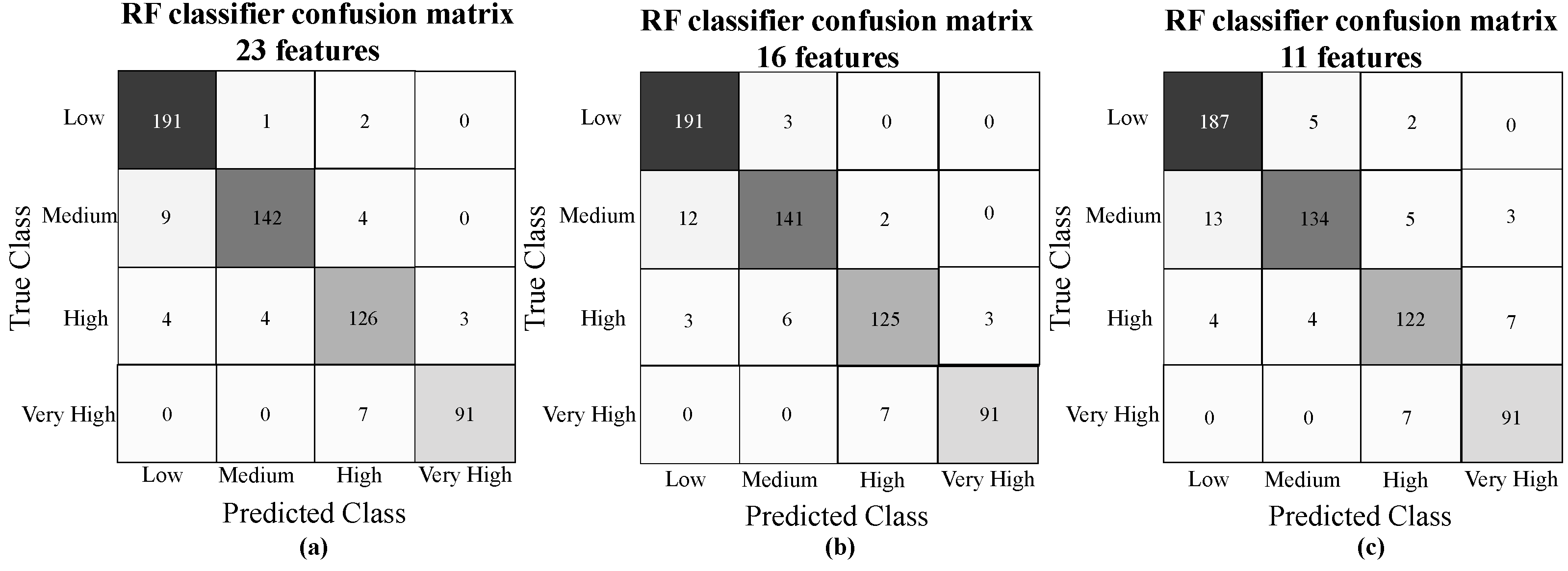
3.4. Phase 2: Feature Selection and Dimension Reduction
4. Results
5. Discussion
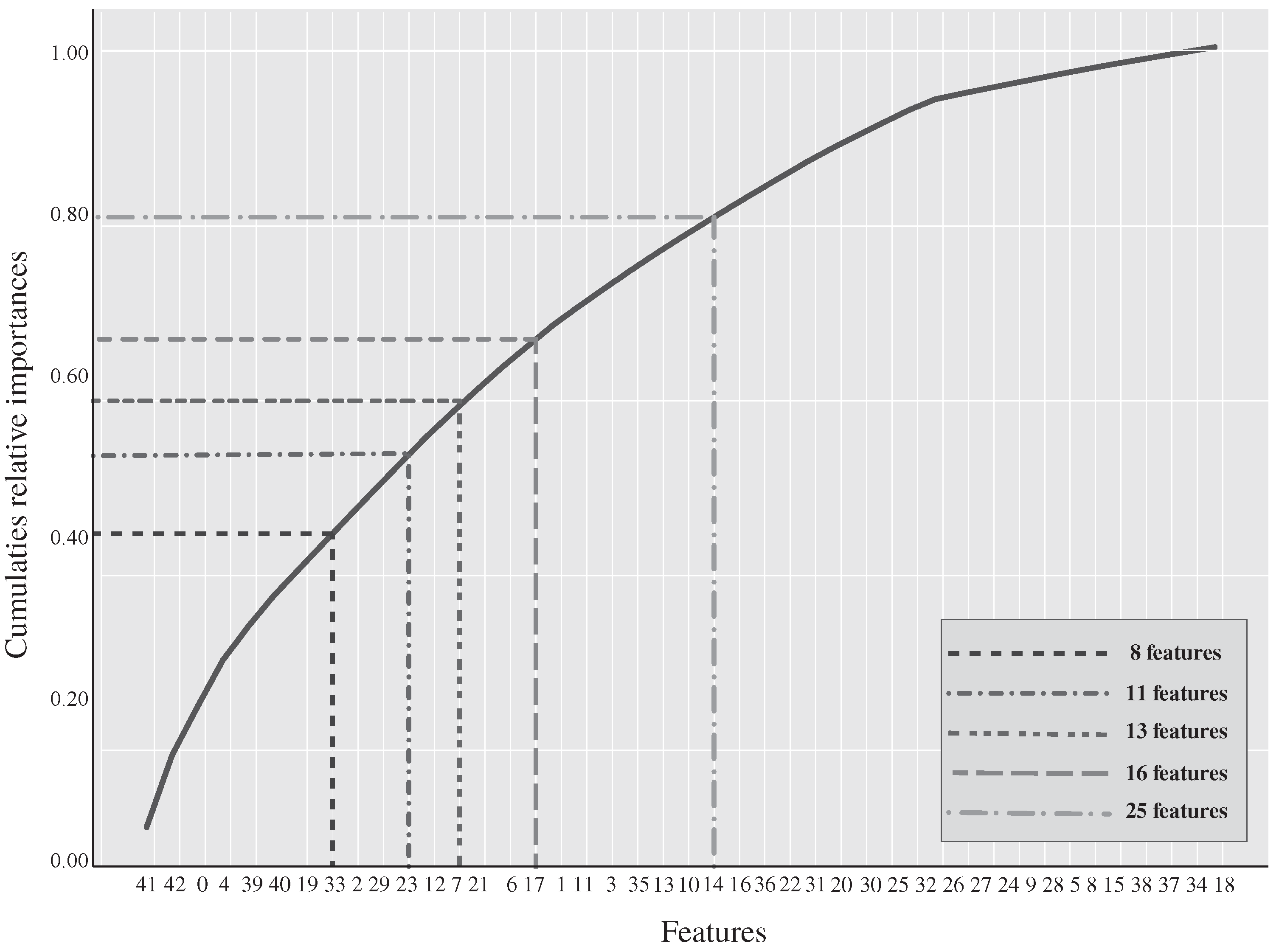
- EMG RMS signals (features 41, 42, 39, 40) represent the square root of the average power of the EMG signal for a given period. Decrease over time of these signals led to the detection of muscle fatigue.
- Gait Acceleration Mean (feature 0) reflects the mean duration of each gait cycle. The fatigued musculoskeletal system is less able to attenuate heel strike-initiated shock waves, which could be observed as an increase in the amplitude of the acceleration measured at the foot. If the mean gait cycle time increased significantly with elapsed walking time indicates that the individual is fatigued.
- Gait Acceleration Median (feature 4) is the median value for each gait cycle acceleration.
- Spine Acceleration Mean (features 19 and 29) represents the torso acceleration over each gait cycle. These features show that if participants kept consistent torso movement over gait cycles, then it likely corresponds to their walking behavior and the patient is less likely to report physical fatigue.
- Spine Acceleration Median (features 33 and 23) is a measure of the central tendency of the torso acceleration distribution. Where the participant maintains a high level of spine acceleration, they are more likely to feel physically fatigued.
- Gait Maximum Acceleration (features 2 and 12) as the gait cycle time increased significantly with increasing fatigue, gait acceleration decreases. If the participant reduces their walking speed, then a decrease in peak gait acceleration is generated, indicating that the participant is fatigued.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Salakari, M.R.; Surakka, T.; Nurminen, R.; Pylkkänen, L. Effects of rehabilitation among patients with advances cancer: A systematic review. Acta Oncol. 2015, 54, 618–628. [Google Scholar] [CrossRef]
- Zanuso, S.; Balducci, S.; Jimenez, A. Physical activity, a key factor to quality of life in type 2 diabetic patients. Diabetes/Metab. Res. Rev. 2009, 25, S24–S28. [Google Scholar] [CrossRef]
- Zanuso, S.; Jimenez, A.; Pugliese, G.; Corigliano, G.; Balducci, S. Exercise for the management of type 2 diabetes: A review of the evidence. Acta Diabetol. 2010, 47, 15–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warburton, D.E.; Nicol, C.W.; Bredin, S.S. Health benefits of physical activity: The evidence. CMAJ 2006, 174, 801–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauman, A.E. Updating the evidence that physical activity is good for health: An epidemiological review 2000–2003. J. Sci. Med. Sport 2004, 7, 6–19. [Google Scholar] [CrossRef]
- Oguma, Y.; Shinoda-Tagawa, T. Physical activity decreases cardiovascular disease risk in women: Review and meta-analysis. Am. J. Prev. Med. 2004, 26, 407–418. [Google Scholar] [CrossRef] [PubMed]
- Vuori, I. Physical inactivity is a cause and physical activity is a remedy for major public health problems. Kinesiology 2004, 36, 123–153. [Google Scholar]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical Activity and Public Health. Med. Sci. Sport. Exerc. 2007, 39, 1423–1434. [Google Scholar] [CrossRef] [Green Version]
- Pinto-Bernal, M.J.; Aguirre, A.; Cifuentes, C.A.; Munera, M. Wearable Sensors for Monitoring Exercise and Fatigue Estimation in Rehabilitation. In Internet of Medical Things; CRC Press: Boca Raton, FL, USA, 2021; pp. 83–110. [Google Scholar]
- Kristensen, T.; Kornitzer, M.; Alfredsson, L.; Marmot, M.; Logstrup, S.; Williams, C. Social Factors, Work, Stress and Cardiovascular Disease Prevention in the European Union; European Heart Network: Brussels, Belgium, 1998. [Google Scholar]
- Priest, N.; Armstrong, R.; Doyle, J.; Waters, E. Interventions implemented through sporting organisations for increasing participation in sport. Cochrane Database Syst. Rev. 2008, 18, CD004812. [Google Scholar] [CrossRef]
- Livingstone, M.; Robson, P.; Wallace, J.; McKinley, M. How active are we? Levels of routine physical activity in children and adults. Proc. Nutr. Soc. 2003, 62, 681–701. [Google Scholar] [CrossRef] [Green Version]
- Pollock, M.L.; Gaesser, G.A.; Butcher, J.D.; Després, J.P.; Dishman, R.K.; Franklin, B.A.; Garber, C.E. The recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness, and flexibility in healthy adults. Schweiz. Z. Sportmed. 1998, 41, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.B.; Schnohr, P.; Schroll, M.; Hein, H.O. All-Cause Mortality Associated with Physical Activity during Leisure Time, Work, Sports, and Cycling to Work. Arch. Intern. Med. 2000, 160, 1621–1628. [Google Scholar] [CrossRef] [PubMed]
- Schnohr, P.; Marott, J.L.; Jensen, J.S.; Jensen, G.B. Intensity versus duration of cycling, impact on all-cause and coronary heart disease mortality: The Copenhagen City Heart Study. Eur. J. Prev. Cardiol. 2012, 19, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E. Prescribing exercise as preventive therapy. Can. Med. Assoc. J. 2006, 174, 961–974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cup, E.H.; Pieterse, A.J.; ten Broek-Pastoor, J.M.; Munneke, M.; van Engelen, B.G.; Hendricks, H.T.; van der Wilt, G.J.; Oostendorp, R.A. Exercise Therapy and Other Types of Physical Therapy for Patients With Neuromuscular Diseases: A Systematic Review. Arch. Phys. Med. Rehabil. 2007, 88, 1452–1464. [Google Scholar] [CrossRef] [PubMed]
- Manley, A.F. Physical Activity and Health: A Report of the Surgeon General; Diane Publishing: Darby, PA, USA, 1996. [Google Scholar]
- Lee, I.M.; Sesso, H.D.; Oguma, Y.; Paffenbarger, R.S. Relative intensity of physical activity and risk of coronary heart disease. Circulation 2003, 107, 1110–1116. [Google Scholar] [CrossRef] [Green Version]
- American College of Sports Medicine. ACSM’s Health-Related Physical Fitness Assessment Manual; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Balducci, S.; Sacchetti, M.; Haxhi, J.; Orlando, G.; D’Errico, V.; Fallucca, S.; Menini, S.; Pugliese, G. Physical exercise as therapy for type 2 diabetes mellitus. Diabetes/Metab. Res. Rev. 2014, 30, 13–23. [Google Scholar] [CrossRef]
- Dun, Y.; Smith, J.R.; Liu, S.; Olson, T.P. High-Intensity Interval Training in Cardiac Rehabilitation. Sports Med. 2019, 42, 587–605. [Google Scholar] [CrossRef]
- Tanasescu, M.; Leitzmann, M.F.; Rimm, E.B.; Willett, W.C.; Stampfer, M.J.; Hu, F.B. Exercise type and intensity in relation to coronary heart disease in men. J. Am. Med. Assoc. 2002, 288, 1994–2000. [Google Scholar] [CrossRef]
- Oldervoll, L.; Kaasa, S.; Hjermstad, M.; Lund, J.; Loge, J. Physical exercise results in the improved subjective well-being of a few or is effective rehabilitation for all cancer patients? Eur. J. Cancer 2004, 40, 951–962. [Google Scholar] [CrossRef]
- Fleig, L.; Lippke, S.; Pomp, S.; Schwarzer, R. Exercise maintenance after rehabilitation: How experience can make a difference. Psychol. Sport Exerc. 2011, 12, 293–299. [Google Scholar] [CrossRef]
- Göhner, W.; Seelig, H.; Fuchs, R. Intervention effects on cognitive antecedents of physical exercise: A 1-year follow-up study. Appl. Psychol. Health Well-Being 2009, 1, 233–256. [Google Scholar] [CrossRef]
- Abd-Elfattah, H.M.; Abdelazeim, F.H.; Elshennawy, S. Physical and cognitive consequences of fatigue: A review. J. Adv. Res. 2015, 6, 351–358. [Google Scholar] [CrossRef]
- Baussard, L.; Carayol, M.; Porro, B.; Baguet, F.; Cousson-gelie, F. European Journal of Oncology Nursing Fatigue in cancer patients: Development and validation of a short form of the Multidimensional Fatigue Inventory ( MFI-10 ). Eur. J. Oncol. Nurs. 2018, 36, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Alghannam, A.F.; Tsintzas, K.; Thompson, D.; Bilzon, J.; Betts, J.A. Exploring mechanisms of fatigue during repeated exercise and the dose dependent effects of carbohydrate and protein ingestion: Study protocol for a randomised controlled trial. Trials 2014, 15, 95. [Google Scholar] [CrossRef] [Green Version]
- Ozalp, O.; Inal-Ince, D.; Calik, E.; Vardar-Yagli, N.; Saglam, M.; Savci, S.; Arikan, H.; Bosnak-Guclu, M.; Coplu, L. Extrapulmonary features of bronchiectasis: Muscle function, exercise capacity, fatigue, and health status. Multidiscip. Respir. Med. 2012, 7, 3. [Google Scholar] [CrossRef] [Green Version]
- Lu, L.; Megahed, F.M.; Sesek, R.F.; Cavuoto, L.A. A survey of the prevalence of fatigue, its precursors and individual coping mechanisms among US manufacturing workers. Appl. Ergon. 2017, 65, 139–151. [Google Scholar] [CrossRef]
- Zamunér, A.R.; Moreno, M.A.; Camargo, T.M.; Graetz, J.P.; Rebelo, A.C.; Tamburús, N.Y.; da Silva, E. Assessment of subjective perceived exertion at the anaerobic threshold with the Borg CR-10 scale. J. Sport. Sci. Med. 2011, 10, 130–136. [Google Scholar]
- Curt, G.A.; Breitbart, W.; Cella, D.; Groopman, J.E.; Horning, S.J.; Itri, L.M.; Johnson, D.H.; Miaskowski, C.; Scherr, S.L.; Portenoy, R.K.; et al. Impact of cancer-related fatigue on the lives of patients: New findings from the Fatigue Coalition. Oncologist 2000, 5, 353–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Annett, J. Subjective rating scales: Science or art? Ergonomics 2002, 45, 966–987. [Google Scholar] [CrossRef] [PubMed]
- Williams, N. The Borg rating of perceived exertion (RPE) scale. Occup. Med. 2017, 67, 404–405. [Google Scholar] [CrossRef] [Green Version]
- Borg, G. Borg’s range model and scales. Int. J. Sport Psychol. 2001, 32, 110–126. [Google Scholar]
- Sehle, A.; Vieten, M.; Sailer, S.; Mündermann, A.; Dettmers, C. Objective assessment of motor fatigue in multiple sclerosis: The Fatigue index Kliniken Schmieder (FKS). J. Neurol. 2014, 261, 1752–1762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maman, Z.S.; Chen, Y.J.; Baghdadi, A.; Lombardo, S.; Cavuoto, L.A.; Megahed, F.M. A data analytic framework for physical fatigue management using wearable sensors. Expert Syst. Appl. 2020, 155, 113405. [Google Scholar] [CrossRef]
- Qi, J.; Yang, P.; Waraich, A.; Deng, Z.; Zhao, Y.; Yang, Y. Examining sensor-based physical activity recognition and monitoring for healthcare using Internet of Things: A systematic review. J. Biomed. Inform. 2018, 87, 138–153. [Google Scholar] [CrossRef]
- Zeni, A.I.; Hoffman, M.D.; Clifford, P.S. Relationships among heart rate, lactate concentration, and perceived effort for different types of rhythmic exercise in women. Arch. Phys. Med. Rehabil. 1996, 77, 237–241. [Google Scholar] [CrossRef]
- Poole, D.C.; Burnley, M.; Vanhatalo, A.; Rossiter, H.B.; Jones, A.M. Critical power: An important fatigue threshold in exercise physiology. Med. Sci. Sport. Exerc. 2016, 48, 2320–2334. [Google Scholar] [CrossRef] [Green Version]
- Pettersson, S.; Lundberg, I.; Liang, M.; Pouchot, J.; Welin Henriksson, E. Determination of the minimal clinically important difference for seven measures of fatigue in Swedish patients with systemic lupus erythematosus. Scand. J. Rheumatol. 2015, 44, 206–210. [Google Scholar] [CrossRef]
- Yu, F.; Bilberg, A.; Stenager, E.; Rabotti, C.; Zhang, B.; Mischi, M. A wireless body measurement system to study fatigue in multiple sclerosis. Physiol. Meas. 2012, 33, 2033–2048. [Google Scholar] [CrossRef] [Green Version]
- Möhler, F.; Ringhof, S.; Debertin, D.; Stein, T. Influence of fatigue on running coordination: A UCM analysis with a geometric 2D model and a subject-specific anthropometric 3D model. Hum. Mov. Sci. 2019, 66, 133–141. [Google Scholar] [CrossRef]
- Kang, S.R.; Min, J.Y.; Yu, C.; Kwon, T.K. Effect of whole body vibration on lactate level recovery and heart rate recovery in rest after intense exercise. Technol. Health Care 2017, 25, 115–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glynn, A.J.; Fiddler, H. The Physiotherapist’s Pocket Guide to Exercise E-Book: Assessment, Prescription and Training; Elsevier Health Sciences: Amsterdam, The Netherlands, 2009. [Google Scholar]
- Aubert, A.E.; Seps, B.; Beckers, F. Heart rate variability in athletes. Sport. Med. 2003, 33, 889–919. [Google Scholar] [CrossRef]
- Achten, J.; Jeukendrup, A.E. Heart rate monitoring. Sport. Med. 2003, 33, 517–538. [Google Scholar] [CrossRef]
- Da Cunha, F.A.; Farinatti, P.d.T.V.; Midgley, A.W. Methodological and practical application issues in exercise prescription using the heart rate reserve and oxygen uptake reserve methods. J. Sci. Med. Sport. 2011, 14, 46–57. [Google Scholar] [CrossRef]
- Goodwin, M.L.; Harris, J.E.; Hernández, A.; Gladden, L.B. Blood lactate measurements and analysis during exercise: A guide for clinicians. J. Diabetes Sci. Technol. 2007, 1, 558–569. [Google Scholar] [CrossRef] [Green Version]
- Jansen, T.C.; van Bommel, J.; Bakker, J. Blood lactate monitoring in critically ill patients: A systematic health technology assessment. Crit. Care Med. 2009, 37, 2827–2839. [Google Scholar]
- Saey, D.; Michaud, A.; Couillard, A.; Côté, C.H.; Mador, M.J.; LeBlanc, P.; Jobin, J.; Maltais, F. Contractile fatigue, muscle morphometry, and blood lactate in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2005, 171, 1109–1115. [Google Scholar] [CrossRef] [Green Version]
- Helbostad, J.L.; Sturnieks, D.L.; Menant, J.; Delbaere, K.; Lord, S.R.; Pijnappels, M. Consequences of lower extremity and trunk muscle fatigue on balance and functional tasks in older people: A systematic literature review. BMC Geriatr. 2010, 10, 56. [Google Scholar] [CrossRef] [Green Version]
- Wan, J.-J.; Qin, Z.; Wang, P.-Y.; Sun, Y.; Liu, X. Muscle fatigue: General understanding and treatment. Exp. Mol. Med. 2017, 49, e384. [Google Scholar] [CrossRef]
- Karthick, P.A.; Ghosh, D.M.; Ramakrishnan, S. Surface electromyography based muscle fatigue detection using high-resolution time-frequency methods and machine learning algorithms. Comput. Methods Programs Biomed. 2018, 154, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Subasi, A.; Kiymik, M.K. Muscle fatigue detection in EMG using time-frequency methods, ICA and neural networks. J. Med. Syst. 2010, 34, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Al-Mulla, M.R.; Sepulveda, F.; Colley, M. A Review of Non-Invasive Techniques to Detect and Predict Localised Muscle Fatigue. Sensors 2011, 11, 3545–3594. [Google Scholar] [CrossRef] [Green Version]
- Camomilla, V.; Bergamini, E.; Fantozzi, S.; Vannozzi, G. Trends Supporting the In-Field Use of Wearable Inertial Sensors for Sport Performance Evaluation: A Systematic Review. Sensors 2018, 18, 873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ejupi, A.; Gschwind, Y.J.; Valenzuela, T.; Lord, S.R.; Delbaere, K. A Kinect and Inertial Sensor-Based System for the Self-Assessment of Fall Risk: A Home-Based Study in Older People. Hum.-Comput. Interact. 2016, 31, 261–293. [Google Scholar] [CrossRef]
- Manchola, S.; Bernal, P.; Munera, M.; Cifuentes, C.A. Gait Phase Detection for Lower-Limb Exoskeletons using Foot Motion Data from a Single Inertial Measurement Unit in Hemiparetic Individuals. Sensors 2019, 19, 2988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aguirre, A.; Casas, J.; Céspedes, N.; Múnera, M.; Rincon-Roncancio, M.; Cuesta-Vargas, A.; Cifuentes, C.A. Feasibility study: Towards Estimation of Fatigue Level in Robot-Assisted Exercise for Cardiac Rehabilitation. In Proceedings of the 2019 IEEE 16th International Conference on Rehabilitation Robotics (ICORR), Toronto, ON, Canada, 24–28 June 2019; pp. 911–916. [Google Scholar]
- Céspedes, N.; Múnera, M.; Gómez, C.; Cifuentes, C.A. Social Human-Robot Interaction for Gait Rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 1299–1307. [Google Scholar] [CrossRef]
- Segala, D.B.; Chelidze, D.; Adams, A.; Schiffman, J.M.; Hasselquist, L. Tracking Physiological Fatigue in Prolonged Load Carriage Walking Using Phase Space Warping and Smooth Orthogonal Decomposition. In Proceedings of the ASME International Mechanical Engineering Congress and Exposition, Boston, MA, USA, 31 October–6 November 2008; Volume 48630, pp. 323–331. [Google Scholar]
- Mugnosso, M.; Marini, F.; Holmes, M.; Morasso, P.; Zenzeri, J. Muscle fatigue assessment during robot-mediated movements. J. Neuroeng. Rehabil. 2018, 15, 1–14. [Google Scholar] [CrossRef]
- Chan, V.C.; Beaudette, S.M.; Smale, K.B.; Beange, K.H.; Graham, R.B. A subject-specific approach to detect fatigue-related changes in spine motion using wearable sensors. Sensors 2020, 20, 2646. [Google Scholar] [CrossRef]
- Ross, L.M.; Porter, R.R.; Durstine, J.L. High-intensity interval training (HIIT) for patients with chronic diseases. J. Sport Health Sci. 2016, 5, 139–144. [Google Scholar] [CrossRef] [Green Version]
- García-López, J.; Morante, J.C.; Ogueta-Alday, A.; Rodríguez-Marroyo, J.A. The Type Of Mat (Contact vs. Photocell) Affects Vertical Jump Height Estimated From Flight Time. J. Strength Cond. Res. 2013, 27, 1162–1167. [Google Scholar] [CrossRef]
- Aguirre, A.; Pinto, M.J.; Cifuentes, C.A.; Perdomo, O.; Díaz, C.A.; Múnera, M. Machine Learning Approach for Fatigue Estimation in Sit-to-Stand Exercise. Sensors 2021, 21, 5006. [Google Scholar] [CrossRef]
- Zhang, J.; Lockhart, T.E.; Soangra, R. Classifying lower extremity muscle fatigue during walking using machine learning and inertial sensors. Ann. Biomed. Eng. 2014, 42, 600–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karg, M.; Venture, G.; Hoey, J.; Kulić, D. Human movement analysis as a measure for fatigue: A hidden Markov-based approach. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 470–481. [Google Scholar] [CrossRef] [PubMed]
- Karg, M.; Kühnlenz, K.; Buss, M.; Seiberl, W.; Tusker, F.; Schmeelk, M.; Schwirtz, A. Expression and automatic recognition of exhaustion in natural walking. In Proceedings of the IADIS Interfaces and Human Computer Interaction (IHCI), Amsterdam, The Netherlands, 25–27 July 2008; pp. 165–172. [Google Scholar]
- Kavanagh, J.J.; Morrison, S.; Barrett, R.S. Lumbar and cervical erector spinae fatigue elicit compensatory postural responses to assist in maintaining head stability during walking. J. Appl. Physiol. 2006, 101, 1118–1126. [Google Scholar] [CrossRef]
- Yoshino, K.; Motoshige, T.; Araki, T.; Matsuoka, K. Effect of prolonged free-walking fatigue on gait and physiological rhythm. J. Biomech. 2004, 37, 1271–1280. [Google Scholar] [CrossRef] [PubMed]
- Maman, Z.S.; Yazdi, M.A.A.; Cavuoto, L.A.; Megahed, F.M. A data-driven approach to modeling physical fatigue in the workplace using wearable sensors. Appl. Ergon. 2017, 65, 515–529. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Roan, M.; Smith, B.; Lockhart, T.E. Gait analysis to classify external load conditions using linear discriminant analysis. Hum. Mov. Sci. 2009, 28, 226–235. [Google Scholar] [CrossRef] [Green Version]
- Helbostad, J.L.; Leirfall, S.; Moe-Nilssen, R.; Sletvold, O. Physical fatigue affects gait characteristics in older persons. J. Gerontol. Ser. Biol. Sci. Med Sci. 2007, 62, 1010–1015. [Google Scholar] [CrossRef]
- Winter, D.A. Human balance and posture control during standing and walking. Gait Posture 1995, 3, 193–214. [Google Scholar] [CrossRef]
- Warburton, D.E.; Gledhill, N.; Quinney, A. Musculoskeletal fitness and health. Can. J. Appl. Physiol. 2001, 26, 217–237. [Google Scholar] [CrossRef]
- Swift-Spong, K.; Short, E.; Wade, E.; Matarić, M.J. Effects of comparative feedback from a socially assistive robot on self-efficacy in post-stroke rehabilitation. In Proceedings of the 2015 IEEE International Conference on Rehabilitation Robotics (ICORR), Singapore, 11–14 August 2015; pp. 764–769. [Google Scholar]
- Fasola, J.; Matarić, M.J. A socially assistive robot exercise coach for the elderly. J. Hum.-Robot Interact. 2013, 2, 3–32. [Google Scholar] [CrossRef] [Green Version]
- Casas, J.; Senft, E.; Gutierrez, L.F.; Rincon-Rocancio, M.; Munera, M.; Belpaeme, T.; Cifuentes, C.A. Social assistive robots: Assessing the impact of a training assistant robot in cardiac rehabilitation. Int. J. Soc. Robot. 2020, 1–15. [Google Scholar] [CrossRef]
- Cifuentes, C.A.; Pinto, M.J.; Céspedes, N.; Múnera, M. Social robots in therapy and care. Curr. Robot. Rep. 2020, 1, 59–74. [Google Scholar] [CrossRef]
- Céspedes Gómez, N.; Irfan, B.; Senft, E.; Cifuentes, C.A.; Gutierrez, L.F.; Rincon-Roncancio, M.; Belpaeme, T.; Munera, M. A Socially Assistive Robot for Long-Term Cardiac Rehabilitation in the Real World. Front. Neurorobot. 2021, 15, 21. [Google Scholar]
- Gockley, R.; Bruce, A.; Forlizzi, J.; Michalowski, M.; Mundell, A.; Rosenthal, S.; Sellner, B.; Simmons, R.; Snipes, K.; Schultz, A.C.; et al. Designing robots for long-term social interaction. In Proceedings of the 2005 IEEE/RSJ International Conference on Intelligent Robots and Systems, Edmonton, AB, Canada, 2–6 August 2005; pp. 1338–1343. [Google Scholar]
- Gockley, R.; MatariĆ, M.J. Encouraging physical therapy compliance with a hands-off mobile robot. In Proceedings of the 1st ACM SIGCHI/SIGART Conference on Human–Robot Interaction, Salt Lake City, UT, USA, 2–3 March 2006; pp. 150–155. [Google Scholar]
- Matarić, M.J.; Eriksson, J.; Feil-Seifer, D.J.; Winstein, C.J. Socially assistive robotics for post-stroke rehabilitation. J. Neuroeng. Rehabil. 2007, 4, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Smets, E.M.; Garssen, B.; Bonke, B.; De Haes, J.C. The multidimensional Fatigue Inventory (MFI) psychometric qualities of an instrument to assess fatigue. J. Psychosom. Res. 1995, 39, 315–325. [Google Scholar] [CrossRef] [Green Version]
- Kakria, P.; Tripathi, N.; Kitipawang, P. A real-time health monitoring system for remote cardiac patients using smartphone and wearable sensors. Int. J. Telemed. Appl. 2015, 2015, 373474. [Google Scholar] [CrossRef] [Green Version]
- Moohialdin, A.S.; Suhariadi, B.T.; Siddiqui, M.K. Practical validation measurements of a physiological status monitoring sensor in real construction activities. In Proceedings of the Streamlining Information Transfer between Construction and Structural Engineering, Brisbane, Australia, 3–5 December 2018. [Google Scholar]
- Swain, D.P.; Brawner, C.A.; American College of Sports Medicine. ACSM’s Resource Manual for Guidelines for Exercise Testing and Prescription; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2014. [Google Scholar]
- Taborri, J.; Rossi, S.; Palermo, E.; Patanè, F.; Cappa, P. A Novel HMM Distributed Classifier for the Detection of Gait Phases by Means of a Wearable Inertial Sensor Network. Sensors 2014, 14, 16212–16234. [Google Scholar] [CrossRef] [PubMed]
- Sabatini, A.; Martelloni, C.; Scapellato, S.; Cavallo, F. Assessment of Walking Features From Foot Inertial Sensing. IEEE Trans. Biomed. Eng. 2005, 52, 486–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotiadis, D.; Hermens, H.; Veltink, P. Inertial Gait Phase Detection for control of a drop foot stimulator. Med. Eng. Phys. 2010, 32, 287–297. [Google Scholar] [CrossRef]
- Bao, L.; Intille, S.S. Activity recognition from user-annotated acceleration data. In Proceedings of the International Conference on Pervasive Computing, Vienna, Austria, 21–23 April 2004; Springer: Berlin/Heidelberg, Germany, 2004. [Google Scholar]
- Pirttikangas, S.; Fujinami, K.; Nakajima, T. Feature selection and activity recognition from wearable sensors. In International Symposium on Ubiquitious Computing Systems; Springer: Berlin/Heidelberg, Germany, 2006; pp. 516–527. [Google Scholar]
- Reaz, M.B.I.; Hussain, M.S.; Mohd-Yasin, F. Techniques of EMG signal analysis: Detection, processing, classification and applications. Biol. Proced. Online 2006, 8, 11–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wojtys, E.M.; Wylie, B.B.; Huston, L.J. The effects of muscle fatigue on neuromuscular function and anterior tibial translation in healthy knees. Am. J. Sport. Med. 1996, 24, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Kern, N.; Schiele, B.; Schmidt, A. Multi-sensor activity context detection for wearable computing. In European Symposium on Ambient Intelligence; Springer: Berlin/Heidelberg, Germany, 2003; pp. 220–232. [Google Scholar]
- Marras, W.S.; Lavender, S.A.; Leurgans, S.E.; Rajulu, S.L.; Allread, S.W.G.; Fathallah, F.A.; Ferguson, S.A. The role of dynamic three-dimensional trunk motion in occupationally-related. Spine 1993, 18, 617–628. [Google Scholar] [CrossRef] [PubMed]
- Huynh, T.; Schiele, B. Analyzing features for activity recognition. In Proceedings of the 2005 Joint Conference on Smart Objects and Ambient Intelligence: Innovative Context-Aware Services: Usages and Technologies, Grenoble, France, 12–14 October 2005; pp. 159–163. [Google Scholar]
- Heinz, E.A.; Kunze, K.S.; Sulistyo, S.; Junker, H.; Lukowicz, P.; Tröster, G. Experimental evaluation of variations in primary features used for accelerometric context recognitionIn European Symposium on Ambient Intelligence; Springer: Berlin/Heidelberg, Germany, 2003; pp. 252–263. [Google Scholar]
- Krause, A.; Siewiorek, D.P.; Smailagic, A.; Farringdon, J. Unsupervised, Dynamic Identification of Physiological and Activity Context in Wearable Computing. ISWC 2003, 3, 88. [Google Scholar]
- Lee, S.W.; Mase, K. Activity and location recognition using wearable sensors. IEEE Pervasive Comput. 2002, 1, 24–32. [Google Scholar]
- Lessley, D.; Crandall, J.; Shaw, G.; Kent, R.; Funk, J. A Normalization Technique for Developing Corridors from Individual Subject Responses; Technical Report; SAE Technical Paper: Detroit, MI, USA, 2004. [Google Scholar]
- Moorhouse, K. An improved normalization methodology for developing mean human response curves. In Proceedings of the International Technical Conference on the Enhanced Safety of Vehicles, Seoul, Korea, 27–30 May 2013. [Google Scholar]
- Yoganandan, N.; Arun, M.W.; Pintar, F.A. Normalizing and scaling of data to derive human response corridors from impact tests. J. Biomech. 2014, 47, 1749–1756. [Google Scholar] [CrossRef]
- Kohavi, R. A study of cross-validation and bootstrap for accuracy estimation and model selection. In Proceedings of the 14th International Joint Conference on Artificial Intelligence, IJCAI, Montreal, QC, Canada, 20–25 August 1995; Volume 14, pp. 1137–1145. [Google Scholar]
- Jain, A.K.; Duin, R.P.W.; Mao, J. Statistical pattern recognition: A review. IEEE Trans. Pattern Anal. Mach. Intell. 2000, 22, 4–37. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Cocea, M. Semi-random partitioning of data into training and test sets in granular computing context. Granul. Comput. 2017, 2, 357–386. [Google Scholar] [CrossRef] [Green Version]
- Browne, M.W. Cross-validation methods. J. Math. Psychol. 2000, 44, 108–132. [Google Scholar] [CrossRef] [Green Version]
- Dag, A.; Topuz, K.; Oztekin, A.; Bulur, S.; Megahed, F.M. A probabilistic data-driven framework for scoring the preoperative recipient-donor heart transplant survival. Decis. Support Syst. 2016, 86, 1–12. [Google Scholar] [CrossRef]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Han, J.; Pei, J.; Kamber, M. Data Mining: Concepts and Techniques; Elsevier: Amsterdam, The Netherlands, 2011. [Google Scholar]
- James, G.; Witten, D.; Hastie, T.; Tibshirani, R. An Introduction to Statistical Learning; Springer: Berlin/Heidelberg, Germany, 2013; Volume 112. [Google Scholar]
- Kuhn, M.; Johnson, K. Applied Predictive Modeling; Springer: Berlin/Heidelberg, Germany, 2013; Volume 26. [Google Scholar]
- Fernández, A.; García, S.; Galar, M.; Prati, R.C.; Krawczyk, B.; Herrera, F. Learning from Imbalanced Data Sets; Springer: Berlin/Heidelberg, Germany, 2018; Volume 10. [Google Scholar]
- Krawczyk, B. Learning from imbalanced data: Open challenges and future directions. Prog. Artif. Intell. 2016, 5, 221–232. [Google Scholar] [CrossRef] [Green Version]
- Skiena, S.S. The Data Science Design Manual; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Khalid, S.; Khalil, T.; Nasreen, S. A survey of feature selection and feature extraction techniques in machine learning. In Proceedings of the 2014 Science and Information Conference, London, UK, 27–29 August 2014; pp. 372–378. [Google Scholar]
- Ravi, N.; Dandekar, N.; Mysore, P.; Littman, M.L. Activity Recognition from Accelerometer Data; AAAI: Pittsburgh, PA, USA, 2005; Volume 5, pp. 1541–1546. [Google Scholar]
- Casas, J.; Irfan, B.; Senft, E.; Gutiérrez, L.; Rincon-Roncancio, M.; Munera, M.; Belpaeme, T.; Cifuentes, C.A. Social Assistive Robot for Cardiac Rehabilitation: A Pilot Study with Patients with Angioplasty. In Proceedings of the Companion of the 2018 ACM/IEEE International Conference on Human-Robot Interaction, HRI’18, Chicago, IL, USA, 5–8 March 2018; pp. 79–80. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Research | Physical Activity | Fatigue Detection Technique | Method |
|---|---|---|---|
| Maman et al. (2020) [38] | Manufacturing task | IMUs, HR, Borg Scale | SVM, RF, LR, PLR |
| Maman et al. (2017) [74] | Manufacturing task | IMUs, HR, Borg Scale | PLR |
| Zhang et al. (2014) [69] | Walking | 3D optical tracking, IMUs | SVM |
| Karg et al. (2014) [70] | Squats | 3D optical tracking, subjective scale | HMM, LR |
| Lee et al. (2009) [75] | Walking | 3D optical tracking | LDA, Statistical test |
| Karg et al. (2008) [71] | Walking | 3D optical tracking | LDA, SVM, kNN, NB |
| Helbostad et al. (2007) [76] | Walking | Accelerometers | Statistical test |
| Kavanagh et al. (2006) [72] | Walking | EMG | Statistical test |
| Yoshino et al. (2004) [73] | Walking | subjective scale, EMG, accelerometers | LR |
| Gender | Age | BMI [kg/m] | Walking Speed [m/s] |
|---|---|---|---|
| Male | 21.83 ± 1.40 | 22.84 ± 2.90 | 0.18 ± 0.37 |
| Female | 21.64 ± 0.74 | 22.25 ± 3.09 | 0.18 ± 0.35 |
| Borg CR10 Value | Description | Classification |
|---|---|---|
| 0 | No exertion at all | Low |
| 1 | Very easy | |
| 2 | Easy | |
| 3 | Somewhat moderate | Moderate |
| 4 | Moderate | |
| 5 | Somewhat hard | |
| 6 | Hard | High |
| 7 | Very Hard | |
| 8 | Very Very Hard | |
| 9 | Extremely hard | Very High |
| 10 | Maximum exertion |
| N | Feature | Description | Ref. |
|---|---|---|---|
| 0 | gait_mean_acce | Average gait acceleration | |
| 1 | gait_std_acce | Average gait acceleration std | |
| 2 | gait_max_acce | Average gait maximum acceleration | |
| 3 | gait_var_acce | Average gait acceleration variance | |
| 4 | gait_median_acce | Average median gait acceleration | |
| 5 | gait_energy_acce | Average gait acceleration energy | |
| 6 | gait_entropy_acce | Average gait acceleration entropy | |
| 7 | gait_kurtosis_acce | Average gait acceleration kurtosis | |
| 8 | gait_maxfreq_acce | Average gait acceleration maxfreq | |
| 9 | gait_stdfreq_acce | Average gait gyro stdfreq | |
| 10 | gait_mean_gyro | Average gait angular velocity mean | |
| 11 | gait_std_gyro | Average gait angular velocity std | |
| 12 | gait_max_gyro | Average gait maximum angular velocity | |
| 13 | gait_var_gyro | Average gait angular velocity variance | |
| 14 | gait_median_gyro | Average median gait angular velocity | |
| 15 | gait_energy_gyro | Average gait angular velocity energy | |
| 16 | gait_entropy_gyro | Average gait angular velocity entropy | |
| 17 | gait_curtosis_gyro | Average gait angular velocity kurtosis | |
| 18 | gait_maxfreq_gyro | Average gait angular velocity maxfreq | |
| 19 | l2_mean_acce | Average ts acceleration | [9,95] |
| 20 | l2_std_acce | Average ts acceleration std | [98,99] |
| 21 | l2_max_acce | Average ts maximum acceleration | [94,100] |
| 22 | l2_var_acce | Average ts acceleration variance | [101,102] |
| 23 | l2_median_acce | Average ts acceleration velocity | [76,103] |
| 24 | l2_energy_acce | Average median ts acceleration energy | [70]. |
| 25 | l2_entropy_acce | Average ts acceleration entropy | |
| 26 | l2_kurtosis_acce | Average ts acceleration kurtosis | |
| 27 | l2_maxfreq_acce | Average ts acceleration maxfreq | |
| 28 | l2_stdfreq_acce | Average ts acceleration maxfreq std | |
| 29 | l2_mean_gyro | Average ts angular velocity mean | |
| 30 | l2_std_gyro | Average ts angular velocity std | |
| 31 | l2_max_gyro | Average ts maximum angular velocity | |
| 32 | l2_var_gyro | Average ts angular velocity variance | |
| 33 | l2_median_gyro | Average median ts angular velocity | |
| 34 | l2_energy_gyro | Average ts angular velocity energy | |
| 35 | l2_entropy_gyro | Average ts angular velocity entropy | |
| 36 | l2_Kurtosis_gyro | Average ts angular velocity kurtosis | |
| 37 | l2_maxfreq_gyro | Average angular velocity maxfreq | |
| 38 | l2_stdfreq_gyro | Average ts angular velocity maxfreq std | |
| 39 | rms_gastro | RMS envelope of the gastrocnemius signal | |
| 40 | rms_tibilisAnterior | RMS envelope of the tibilis anterior signal | |
| 41 | rms_rectusFemoris | RMS envelope of the rectus femoris signal | |
| 42 | rms_bicepsFemoris | RMSenvelope of the biceps femoris signal |
| Class | Number of Samples |
|---|---|
| Very High | 463 (15.86%) |
| High | 732 (25.08%) |
| Moderate | 771 (26.41%) |
| Low | 953 (32.65%) |
| Total | 2919 (100%) |
| Model | Hyperparameters | Accuracy | Precision | Recall | F1-Score |
|---|---|---|---|---|---|
| RF | estimators = 100 | 0.965 | 0.931 | 0.929 | 0.928 |
| ANN | activation = tanh solver = adam HLS = (100, 100, 100) alpha = 0.0001 learning_rate = ‘constant’ max_iter = 1000 | 0.949 | 0.896 | 0.898 | 0.894 |
| SVM | kernel = rbf class_weight = ‘balanced’ C = 64 | 0.907 | 0.809 | 0.809 | 0.806 |
| DT | criterion = entropy max depth = 12 min samples split = 11 min samples leaf = 4 | 0.907 | 0.806 | 0.805 | 0.804 |
| KNN | neighbors = 3 | 0.908 | 0.807 | 0.805 | 0.804 |
| LR | solver = newton-cg C = 1,000,000 | 0.822 | 0.626 | 0.624 | 0.620 |
| Sensors | Estimators | Features | Accuracy | Precision | Recall | F1-Score |
|---|---|---|---|---|---|---|
| 60 | 25 | 0.965 | 0.934 | 0.928 | 0.930 | |
| Thigh (EMG), | 40 | 16 | 0.965 | 0.932 | 0.927 | 0.929 |
| Shank (EMG), | 80 | 13 | 0960 | 0921 | 0916 | 0917 |
| L5-S1, Foot | 80 | 11 | 0963 | 0.926 | 0.925 | 0.925 |
| 100 | 8 | 0946 | 0.895 | 0.883 | 0.888 | |
| L5-S1, Foot | 80 | 17 | 0.940 | 0.883 | 0.876 | 0.879 |
| L5-S1 | 80 | 16 | 0.839 | 0678 | 0.658 | 0.664 |
| Foot | 80 | 19 | 0921 | 0.856 | 0.827 | 0.838 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pinto-Bernal, M.J.; Cifuentes, C.A.; Perdomo, O.; Rincón-Roncancio, M.; Múnera, M. A Data-Driven Approach to Physical Fatigue Management Using Wearable Sensors to Classify Four Diagnostic Fatigue States. Sensors 2021, 21, 6401. https://0-doi-org.brum.beds.ac.uk/10.3390/s21196401
Pinto-Bernal MJ, Cifuentes CA, Perdomo O, Rincón-Roncancio M, Múnera M. A Data-Driven Approach to Physical Fatigue Management Using Wearable Sensors to Classify Four Diagnostic Fatigue States. Sensors. 2021; 21(19):6401. https://0-doi-org.brum.beds.ac.uk/10.3390/s21196401
Chicago/Turabian StylePinto-Bernal, Maria J., Carlos A. Cifuentes, Oscar Perdomo, Monica Rincón-Roncancio, and Marcela Múnera. 2021. "A Data-Driven Approach to Physical Fatigue Management Using Wearable Sensors to Classify Four Diagnostic Fatigue States" Sensors 21, no. 19: 6401. https://0-doi-org.brum.beds.ac.uk/10.3390/s21196401