
Foot and Lower Limb Clinical and Structural Changes in Overuse Injured Recreational Runners Using Floating Heel Shoes: Preliminary Results of a Randomised Control Trial

 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
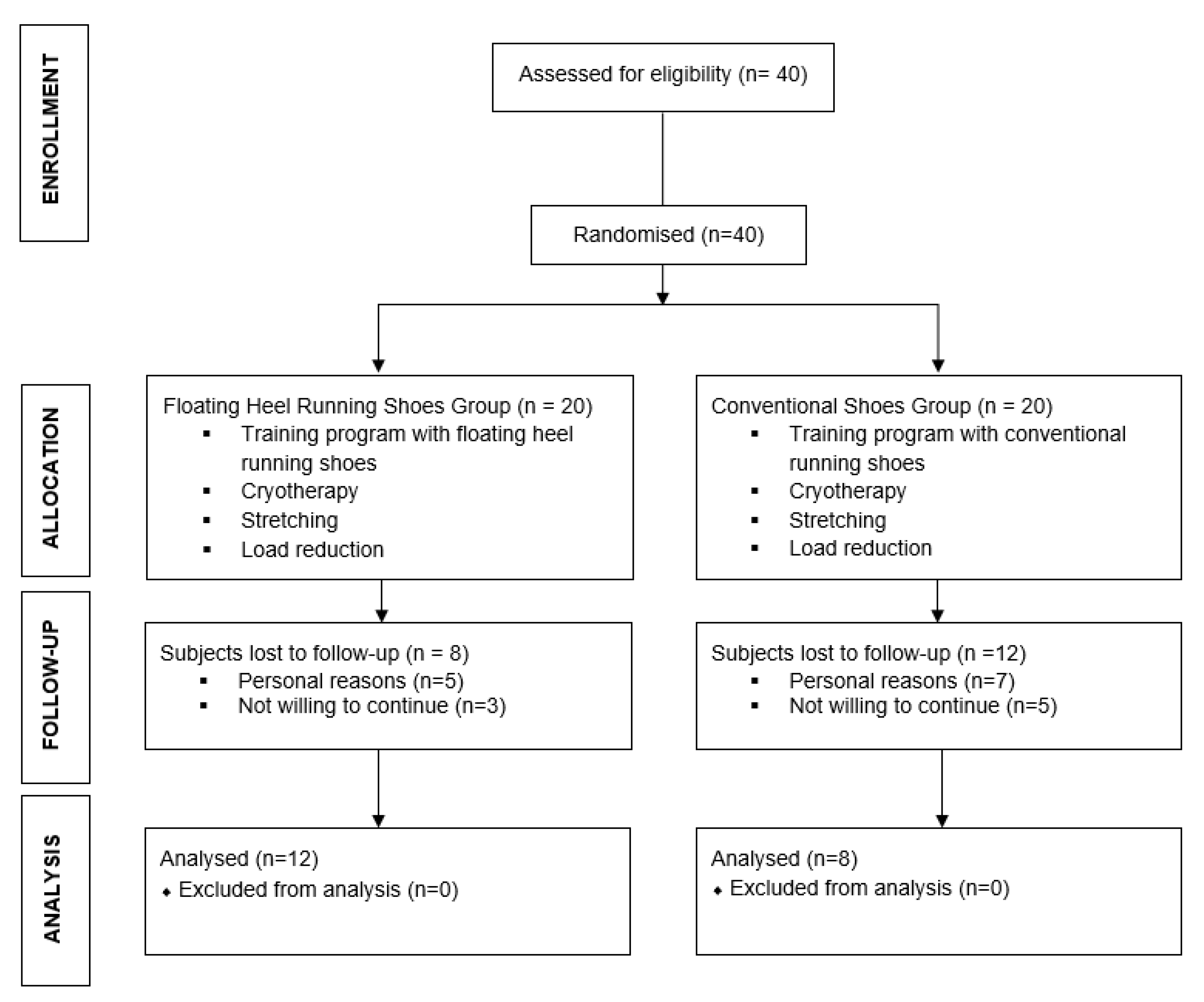
2.1. Participants
2.2. Study Design
2.3. Intervention
- FHSG: followed a training programme to get used to FHS. Through the 12-week intervention the amount of FHS running was increased progressively. From week 1 until week 8, the runners combined both types of running shoes: conventional footwear and FHS. From week 9 until the end of the study, the runners used FHS only. Table 1 shows the training program followed by the FHSG runners.
- CSG: trained in the same way, but using their conventional footwear.
2.4. Outcomes
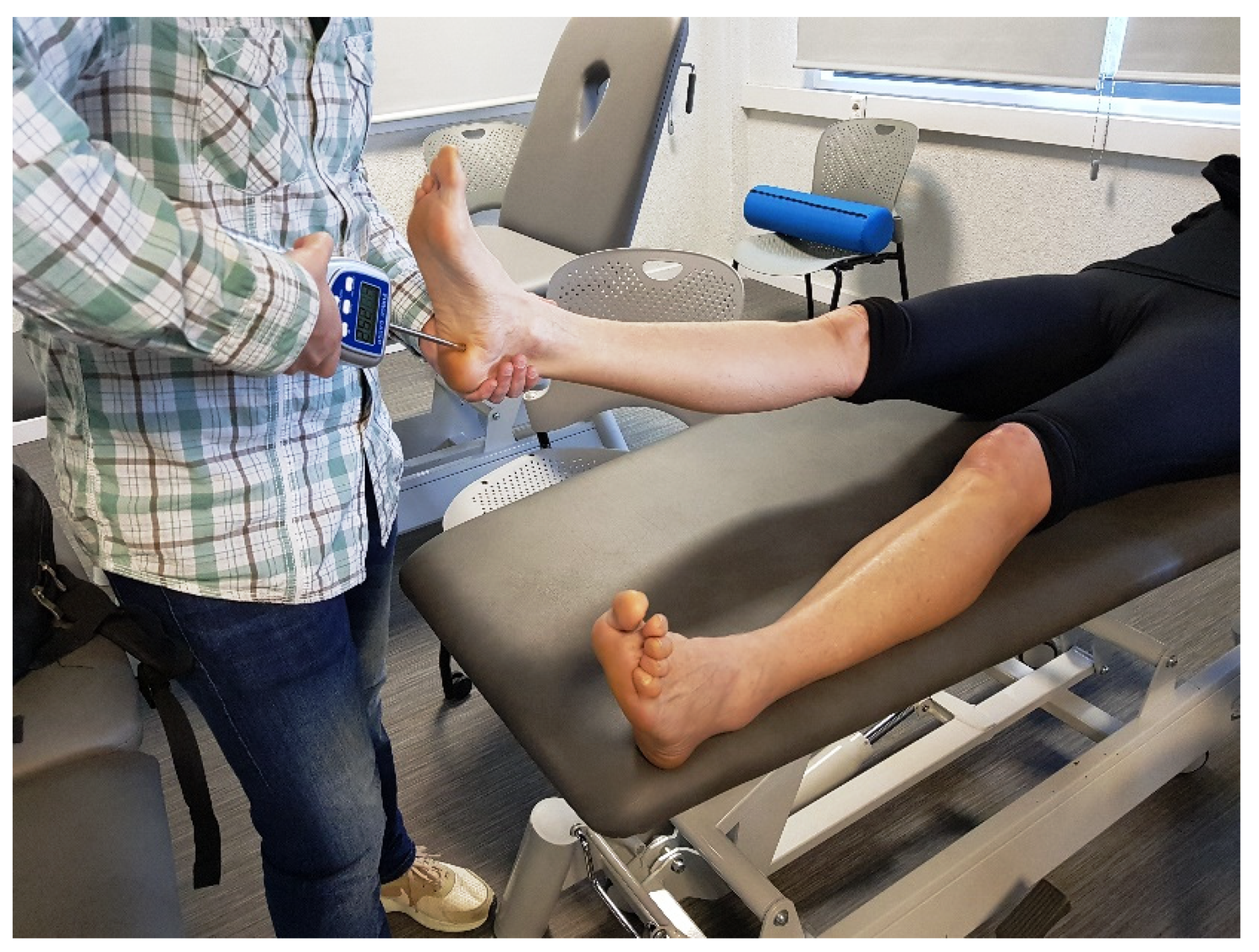
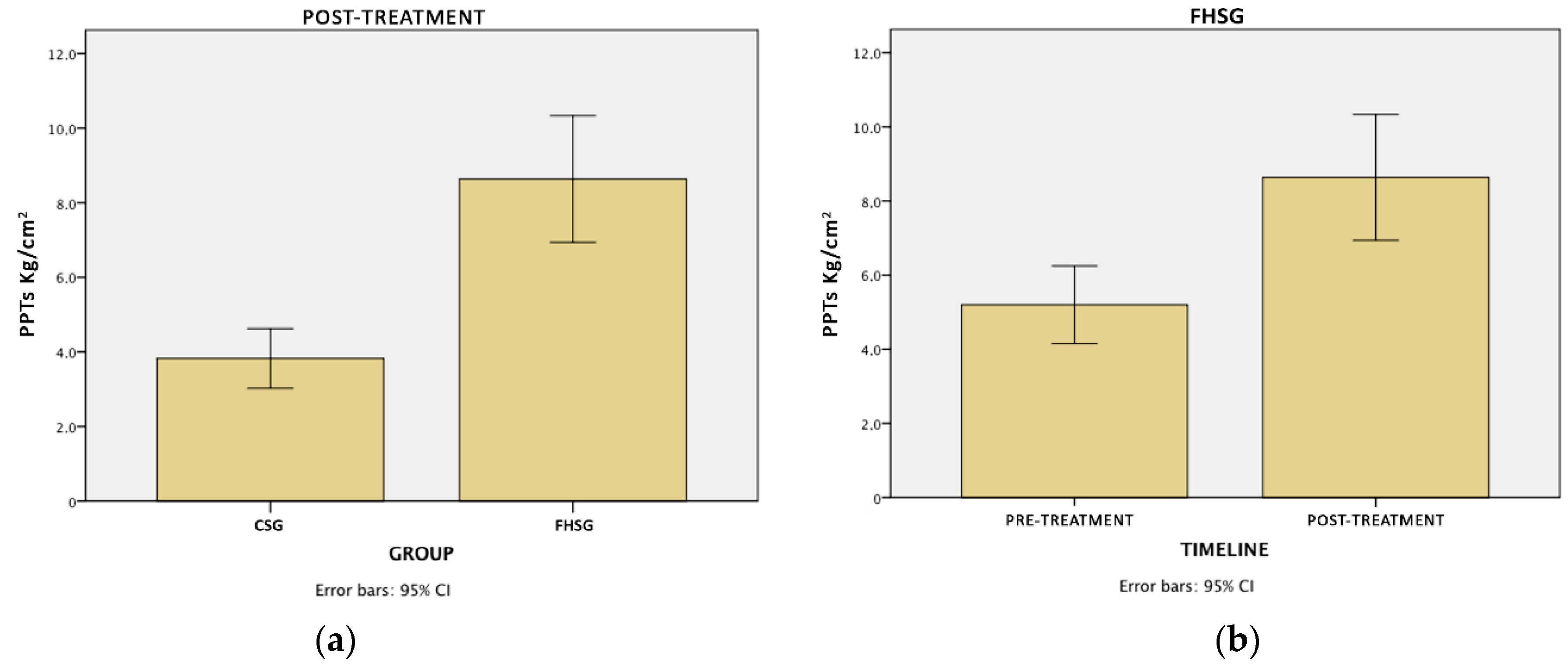
2.4.1. Pressure Pain Thresholds (PPTs)
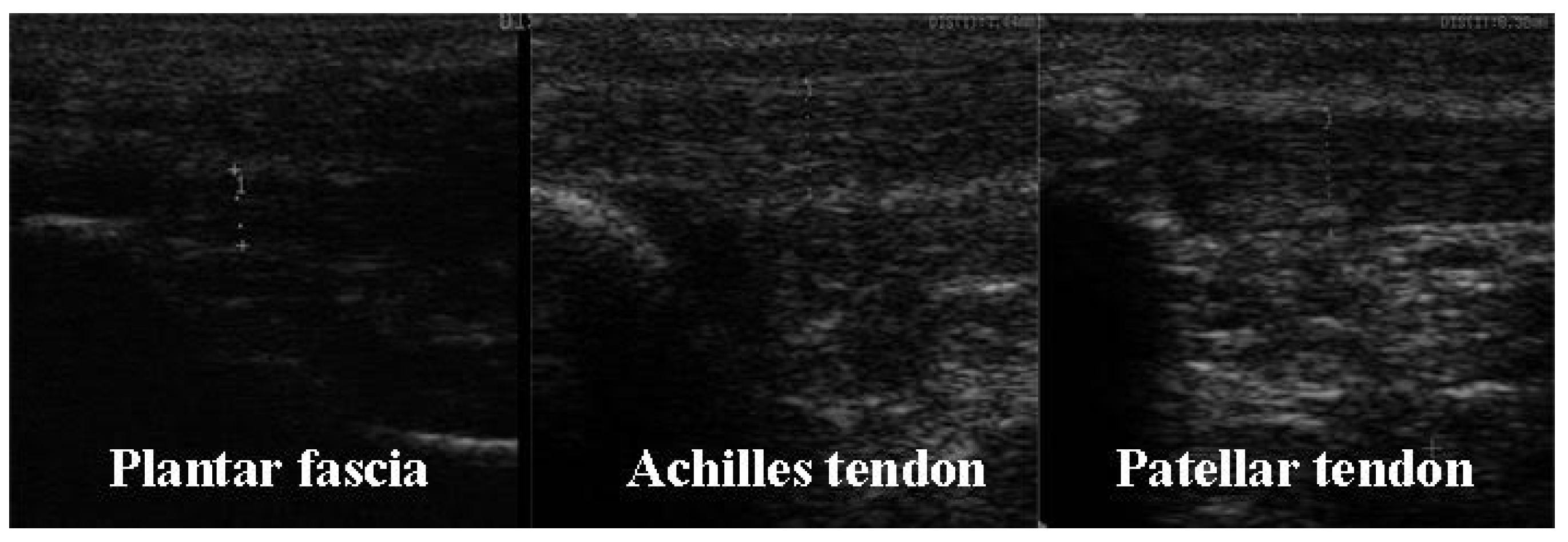
2.4.2. Ultrasonography
2.4.3. Oslo Sports Trauma Research Centre Overuse Injury Questionnaire (OSTRC-O)
2.4.4. Statistical Analysis
3. Results
4. Discussion
4.1. Limitations
4.2. Suggestions for Further Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Deelen, I.; Janssen, M.; Vos, S.; Kamphuis, C.B.M.; Ettema, D. Attractive Running Environments for All? A Cross-Sectional Study on Physical Environmental Characteristics and Runners’ Motives and Attitudes, in Relation to the Experience of the Running Environment. BMC Public Health 2019, 19, 366. [Google Scholar] [CrossRef] [PubMed]
- Lohman, E.B.; Balan Sackiriyas, K.S.; Swen, R.W. A Comparison of the Spatiotemporal Parameters, Kinematics, and Biomechanics between Shod, Unshod, and Minimally Supported Running as Compared to Walking. Phys. Ther. Sport Off. J. Assoc. Chart. Physiother. Sports Med. 2011, 12, 151–163. [Google Scholar] [CrossRef]
- Van Gent, R.N.; Siem, D.; van Middelkoop, M.; van Os, A.G.; Bierma-Zeinstra, S.M.A.; Koes, B.W. Incidence and Determinants of Lower Extremity Running Injuries in Long Distance Runners: A Systematic Review. Br. J. Sports Med. 2007, 41, 469–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Messier, S.P.; Martin, D.F.; Mihalko, S.L.; Ip, E.; DeVita, P.; Cannon, D.W.; Love, M.; Beringer, D.; Saldana, S.; Fellin, R.E.; et al. A 2-Year Prospective Cohort Study of Overuse Running Injuries: The Runners and Injury Longitudinal Study (TRAILS). Am. J. Sports Med. 2018, 46, 2211–2221. [Google Scholar] [CrossRef]
- Daoud, A.I.; Geissler, G.J.; Wang, F.; Saretsky, J.; Daoud, Y.A.; Lieberman, D.E. Foot Strike and Injury Rates in Endurance Runners: A Retrospective Study. Med. Sci. Sports Exerc. 2012, 44, 1325–1334. [Google Scholar] [CrossRef] [Green Version]
- Malisoux, L.; Chambon, N.; Delattre, N.; Gueguen, N.; Urhausen, A.; Theisen, D. Injury Risk in Runners Using Standard or Motion Control Shoes: A Randomised Controlled Trial with Participant and Assessor Blinding. Br. J. Sports Med. 2016, 50, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Milner, C.E.; Ferber, R.; Pollard, C.D.; Hamill, J.; Davis, I.S. Biomechanical Factors Associated with Tibial Stress Fracture in Female Runners. Med. Sci. Sports Exerc. 2006, 38, 323–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lieberman, D.E.; Warrener, A.G.; Wang, J.; Castillo, E.R. Effects of Stride Frequency and Foot Position at Landing on Braking Force, Hip Torque, Impact Peak Force and the Metabolic Cost of Running in Humans. J. Exp. Biol. 2015, 218, 3406–3414. [Google Scholar] [CrossRef] [Green Version]
- Heiderscheit, B.C.; Chumanov, E.S.; Michalski, M.P.; Wille, C.M.; Ryan, M.B. Effects of Step Rate Manipulation on Joint Mechanics during Running. Med. Sci. Sports Exerc. 2011, 43, 296–302. [Google Scholar] [CrossRef] [Green Version]
- Futrell, E.E.; Gross, K.D.; Reisman, D.; Mullineaux, D.R.; Davis, I.S. Transition to Forefoot Strike Reduces Load Rates More Effectively than Altered Cadence. J. Sport Health Sci. 2020, 9, 248–257. [Google Scholar] [CrossRef]
- Altman, A.R.; Davis, I.S. Barefoot Running: Biomechanics and Implications for Running Injuries. Curr. Sports Med. Rep. 2012, 11, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Hreljac, A. Impact and Overuse Injuries in Runners. Med. Sci. Sports Exerc. 2004, 36, 845–849. [Google Scholar] [CrossRef]
- Lopes, A.D.; Hespanhol Júnior, L.C.; Yeung, S.S.; Costa, L.O.P. What Are the Main Running-Related Musculoskeletal Injuries? A Systematic Review. Sports Med. Auckl. N. Z. 2012, 42, 891–905. [Google Scholar] [CrossRef] [PubMed]
- Davis, I.S.; Futrell, E. Gait Retraining: Altering the Fingerprint of Gait. Phys. Med. Rehabil. Clin. N. Am. 2016, 27, 339–355. [Google Scholar] [CrossRef] [Green Version]
- Barton, C.J.; Bonanno, D.R.; Carr, J.; Neal, B.S.; Malliaras, P.; Franklyn-Miller, A.; Menz, H.B. Running Retraining to Treat Lower Limb Injuries: A Mixed-Methods Study of Current Evidence Synthesised with Expert Opinion. Br. J. Sports Med. 2016, 50, 513–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Almeida, M.O.; Saragiotto, B.T.; Yamato, T.P.; Lopes, A.D. Is the Rearfoot Pattern the Most Frequently Foot Strike Pattern among Recreational Shod Distance Runners? Phys. Ther. Sport Off. J. Assoc. Chart. Physiother. Sports Med. 2015, 16, 29–33. [Google Scholar] [CrossRef]
- Lieberman, D.E.; Venkadesan, M.; Werbel, W.A.; Daoud, A.I.; D’Andrea, S.; Davis, I.S.; Mang’eni, R.O.; Pitsiladis, Y. Foot Strike Patterns and Collision Forces in Habitually Barefoot versus Shod Runners. Nature 2010, 463, 531–535. [Google Scholar] [CrossRef]
- Delgado, T.L.; Kubera-Shelton, E.; Robb, R.R.; Hickman, R.; Wallmann, H.W.; Dufek, J.S. Effects of Foot Strike on Low Back Posture, Shock Attenuation, and Comfort in Running. Med. Sci. Sports Exerc. 2013, 45, 490–496. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.H.; McPhail, A.J.C.; An, W.W.; Naqvi, W.M.; Chan, D.L.H.; Au, I.P.H.; Luk, A.T.W.; Chen, T.L.; Cheung, R.T.H. A New Footwear Technology to Promote Non-Heelstrike Landing and Enhance Running Performance: Fact or Fad? J. Sports Sci. 2017, 35, 1533–1537. [Google Scholar] [CrossRef]
- Beneyto, F. Shoe with a Suspended Heel and Method for Facilitating Adaptation to the Natural Suspended Heel Running Technique. European Patent Application EP3061361A4, 21 October 2014. [Google Scholar]
- Barnes, A.; Gamez-Pay, J.; Castelli, A.; Heller, B. Foot Strike Patterns in Runners Wearing Floating Heel, Minimalist and Conventional Footwear. In Proceedings of the 33rd International Conference on Biomechanics in Sports, Poitiers, France, 29 June–3 July 2015; Volume 2015, pp. 519–522. [Google Scholar]
- Gamez-Paya, J.; Barnes, A.; Castelli, A.; Alarcon-Jimenez, J.; Heller, B. Kinematic Analysis of a New Running Shoe Concept Based on a Biomimetic Approach, the Floating Heel Running Shoe. In Proceedings of the 8th World Congress of Biomechanics, Dublin, Ireland, 8–12 July 2018. [Google Scholar]
- Saxelby, J.; Gamez-Paya, J.; Heller, B. A Holistic Approach To Managing a Runner With Recalcitrant Plantar Fasciitis Outside the Clinic. Podaitry Now 2017, 20, 8–12. [Google Scholar]
- Knapik, J.J.; Orr, R.; Pope, R.; Grier, T. Injuries And Footwear (Part 2): Minimalist Running Shoes. J. Spec. Oper. Med. 2016, 16, 89–96. [Google Scholar]
- Schulz, K.F.; Altman, D.G.; Moher, D.; The CONSORT Group. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. Trials 2010, 11, 32. [Google Scholar] [CrossRef] [Green Version]
- Souza, R.B. An Evidence-Based Videotaped Running Biomechanics Analysis. Phys. Med. Rehabil. Clin. N. Am. 2016, 27, 217–236. [Google Scholar] [CrossRef] [Green Version]
- Kregel, J.; van Wilgen, C.P.; Zwerver, J. Pain Assessment in Patellar Tendinopathy Using Pain Pressure Threshold Algometry: An Observational Study. Pain Med. 2013, 14, 1769–1775. [Google Scholar] [CrossRef] [Green Version]
- Rolke, R.; Baron, R.; Maier, C.; Tölle, T.R.; Treede, D.R.; Beyer, A.; Binder, A.; Birbaumer, N.; Birklein, F.; Bötefür, I.C.; et al. Quantitative Sensory Testing in the German Research Network on Neuropathic Pain (DFNS): Standardized Protocol and Reference Values. Pain 2006, 123, 231–243. [Google Scholar] [CrossRef]
- Slater, H.; Thériault, E.; Ronningen, B.O.; Clark, R.; Nosaka, K. Exercise-Induced Mechanical Hypoalgesia in Musculotendinous Tissues of the Lateral Elbow. Man. Ther. 2010, 15, 66–73. [Google Scholar] [CrossRef] [Green Version]
- Chesterton, L.S.; Sim, J.; Wright, C.C.; Foster, N.E. Interrater Reliability of Algometry in Measuring Pressure Pain Thresholds in Healthy Humans, Using Multiple Raters. Clin. J. Pain 2007, 23, 760–766. [Google Scholar] [CrossRef]
- Reeves, J.L.; Jaeger, B.; Graff-Radford, S.B. Reliability of the Pressure Algometer as a Measure of Myofascial Trigger Point Sensitivity. Pain 1986, 24, 313–321. [Google Scholar] [CrossRef]
- Giles, L.S.; Webster, K.E.; McClelland, J.A.; Cook, J. Can Ultrasound Measurements of Muscle Thickness Be Used to Measure the Size of Individual Quadriceps Muscles in People with Patellofemoral Pain? Phys. Ther. Sport Off. J. Assoc. Chart. Physiother. Sports Med. 2015, 16, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, Y.; Muraoka, Y.; Kubo, K.; Suzuki, Y.; Fukunaga, T. Changes in Muscle Size and Architecture Following 20 Days of Bed Rest. J. Gravit. Physiol. J. Int. Soc. Gravit. Physiol. 2000, 7, 53–59. [Google Scholar]
- Abe, T.; Loenneke, J.P.; Thiebaud, R.S. Ultrasound Assessment of Hamstring Muscle Size Using Posterior Thigh Muscle Thickness. Clin. Physiol. Funct. Imaging 2016, 36, 206–210. [Google Scholar] [CrossRef]
- Benítez-Martínez, J.C.; Valera-Garrido, F.; Martínez-Ramírez, P.; Ríos-Díaz, J.; Del Baño-Aledo, M.E.; Medina-Mirapeix, F. Lower Limb Dominance, Morphology, and Sonographic Abnormalities of the Patellar Tendon in Elite Basketball Players: A Cross-Sectional Study. J. Athl. Train. 2019, 54, 1280–1286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brushøj, C.; Henriksen, B.M.; Albrecht-Beste, E.; Hölmich, P.; Larsen, K.; Bachmann Nielsen, M. Reproducibility of Ultrasound and Magnetic Resonance Imaging Measurements of Tendon Size. Acta Radiol. Stockh. Swed. 2006, 47, 954–959. [Google Scholar] [CrossRef]
- Clarsen, B.; Myklebust, G.; Bahr, R. Development and Validation of a New Method for the Registration of Overuse Injuries in Sports Injury Epidemiology: The Oslo Sports Trauma Research Centre (OSTRC) Overuse Injury Questionnaire. Br. J. Sports Med. 2013, 47, 495–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bailón-Cerezo, J.; Clarsen, B.; Sánchez-Sánchez, B.; Torres-Lacomba, M. Cross-Cultural Adaptation and Validation of the Oslo Sports Trauma Research Center Questionnaires on Overuse Injury and Health Problems (2nd Version) in Spanish Youth Sports. Orthop. J. Sports Med. 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, R.; Rubin, D.B. Meta-Analytic Procedures for Combining Studies with Multiple Effect Sizes. Psychol. Bull. 1986, 99, 400–406. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988; ISBN 0-8058-0283-5. [Google Scholar]
- Abate, M.; Silbernagel, K.G.; Siljeholm, C.; Di Iorio, A.; De Amicis, D.; Salini, V.; Werner, S.; Paganelli, R. Pathogenesis of Tendinopathies: Inflammation or Degeneration? Arthritis Res. Ther. 2009, 11, 235. [Google Scholar] [CrossRef] [Green Version]
- Kerrigan, D.C.; Franz, J.R.; Keenan, G.S.; Dicharry, J.; Della Croce, U.; Wilder, R.P. The Effect of Running Shoes on Lower Extremity Joint Torques. PM R. 2009, 1, 1058–1063. [Google Scholar] [CrossRef]
- Syha, R.; Peters, M.; Birnesser, H.; Niess, A.; Hirschmueller, A.; Dickhuth, H.-H.; Sandrock, M. Computer-Based Quantification of the Mean Achilles Tendon Thickness in Ultrasound Images: Effect of Tendinosis. Br. J. Sports Med. 2007, 41, 897–902, discussion 902. [Google Scholar] [CrossRef] [Green Version]
- Comin, J.; Cook, J.L.; Malliaras, P.; McCormack, M.; Calleja, M.; Clarke, A.; Connell, D. The Prevalence and Clinical Significance of Sonographic Tendon Abnormalities in Asymptomatic Ballet Dancers: A 24-Month Longitudinal Study. Br. J. Sports Med. 2013, 47, 89–92. [Google Scholar] [CrossRef]
- Chimenti, R.L.; Flemister, A.S.; Tome, J.; McMahon, J.M.; Houck, J.R. Patients With Insertional Achilles Tendinopathy Exhibit Differences in Ankle Biomechanics as Opposed to Strength and Range of Motion. J. Orthop. Sports Phys. Ther. 2016, 46, 1051–1060. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Deng, L.; Yang, Y.; Li, L.; Fu, W. Acute Shoe Effects on Achilles Tendon Loading in Runners with Habitual Rearfoot Strike Pattern. Gait Posture 2020, 82, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Franke, T.P.C.; de Vet, H.C.W.; Huisstede, B.M.A. Minimally Important Change and Smallest Detectable Change of the OSTRC Questionnaire in Half- and Full-marathon Runners. Scand. J. Med. Sci. Sports 2021, 31, 1048–1058. [Google Scholar] [CrossRef]
- Sussmilch-Leitch, S.P.; Collins, N.J.; Bialocerkowski, A.E.; Warden, S.J.; Crossley, K.M. Physical Therapies for Achilles Tendinopathy: Systematic Review and Meta-Analysis. J. Foot Ankle Res. 2012, 5, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malliaras, P.; Barton, C.J.; Reeves, N.D.; Langberg, H. Achilles and Patellar Tendinopathy Loading Programmes: A Systematic Review Comparing Clinical Outcomes and Identifying Potential Mechanisms for Effectiveness. Sports Med. Auckl. N. Z. 2013, 43, 267–286. [Google Scholar] [CrossRef]
- Rathleff, M.S.; Mølgaard, C.M.; Fredberg, U.; Kaalund, S.; Andersen, K.B.; Jensen, T.T.; Aaskov, S.; Olesen, J.L. High-Load Strength Training Improves Outcome in Patients with Plantar Fasciitis: A Randomized Controlled Trial with 12-Month Follow-Up. Scand. J. Med. Sci. Sports 2015, 25, e292–e300. [Google Scholar] [CrossRef]
- Alfredson, H.; Pietilä, T.; Jonsson, P.; Lorentzon, R. Heavy-Load Eccentric Calf Muscle Training for the Treatment of Chronic Achilles Tendinosis. Am. J. Sports Med. 1998, 26, 360–366. [Google Scholar] [CrossRef] [Green Version]
- Jensen, K.; Di Fabio, R.P. Evaluation of Eccentric Exercise in Treatment of Patellar Tendinitis. Phys. Ther. 1989, 69, 211–216. [Google Scholar] [CrossRef]
- Cannell, L.J.; Taunton, J.E.; Clement, D.B.; Smith, C.; Khan, K.M. A Randomised Clinical Trial of the Efficacy of Drop Squats or Leg Extension/Leg Curl Exercises to Treat Clinically Diagnosed Jumper’s Knee in Athletes: Pilot Study. Br. J. Sports Med. 2001, 35, 60–64. [Google Scholar] [CrossRef]
- Allison, G.T.; Purdam, C. Eccentric Loading for Achilles Tendinopathy--Strengthening or Stretching? Br. J. Sports Med. 2009, 43, 276–279. [Google Scholar] [CrossRef] [Green Version]
- LaStayo, P.; Marcus, R.; Dibble, L.; Frajacomo, F.; Lindstedt, S. Eccentric Exercise in Rehabilitation: Safety, Feasibility, and Application. J. Appl. Physiol. 2013, 116, 1426–1434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LaStayo, P.C.; Marcus, R.L.; Dibble, L.E.; Smith, S.B.; Beck, S.L. Eccentric Exercise versus Usual-Care with Older Cancer Survivors: The Impact on Muscle and Mobility—An Exploratory Pilot Study. BMC Geriatr. 2011, 11, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Concannon, M.; Pringle, B. Psychology in Sports Injury Rehabilitation. Br. J. Nurs. 2012, 21, 484–490. [Google Scholar] [CrossRef] [Green Version]
- Buist, I.; Bredeweg, S.W.; Bessem, B.; van Mechelen, W.; Lemmink, K.A.P.M.; Diercks, R.L. Incidence and Risk Factors of Running-Related Injuries during Preparation for a 4-Mile Recreational Running Event. Br. J. Sports Med. 2010, 44, 598–604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hannigan, J.J.; Pollard, C.D. Differences in Running Biomechanics between a Maximal, Traditional, and Minimal Running Shoe. J. Sci. Med. Sport 2020, 23, 15–19. [Google Scholar] [CrossRef] [Green Version]
- Ortega, J.A.; Healey, L.A.; Swinnen, W.; Hoogkamer, W. Energetics and Biomechanics of Running Footwear with Increased Longitudinal Bending Stiffness: A Narrative Review. Sports Med. Auckl. N. Z. 2021, 51, 873–894. [Google Scholar] [CrossRef]
- Behling, A.-V.; Nigg, B.M. Relationships between the Foot Posture Index and Static as Well as Dynamic Rear Foot and Arch Variables. J. Biomech. 2020, 98, 109448. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical Power Analyses Using G* Power 3.1: Tests for Correlation and Regression Analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Week | Number of Sessions | Training |
|---|---|---|
| 1 | 3 | 3 sets of 3 min with FHRS, 2 min rest |
| 2 | 3 | 3 sets of 5 min with FHRS, 2 min rest |
| 3 | 3 | 3 sets of 6 min with FHRS, 2 min rest |
| 4 | 3 | 3 sets of 8 min with FHRS, 2 min rest |
| 5 | 3 | 2 sets of 12 min with FHRS, 2 min rest |
| 6 | 3 | 2 sets of 15 min with FHRS, 2 min rest |
| 7 | 3 | 2 sets of 20 min with FHRS, 2 min rest |
| 8 | 3 | 2 sets of 25 min with FHRS, 2 min rest |
| 9 | 3 | 100% of the session running with FHRS |
| 10 | 3 | 100% of the session running with FHRS |
| 11 | 3 | 100% of the session running with FHRS |
| 12 | 3 | 100% of the session running with FHRS |
| Type of Injury | FHSG (n = 12) | CSG (n = 8) |
|---|---|---|
| Plantar fasciitis | 5 (42) | 1 (13) |
| Achilles tendinopathy | 3 (25) | 4 (50) |
| Patellar tendinopathy | 2 (17) | 3 (38) |
| Iliotibial band syndrome | 2 (17) | 0 (0) |
| Measures | Time Mean ± SD | Mean Differences and Size Effect (d) | |||
|---|---|---|---|---|---|
| Pre | Post | Within-Group Differences | Between-Group Differences (Post) | ||
| PPTs (kg/cm2) | FHSG | 5.2 ± 2.4 | 8.6 ± 3.8 | 3.4 †; d = 1.1 | 4.8 †; d = 0.8 |
| CSG | 4.7 ± 1.5 | 3.8 ± 0.8 | −0.8 | ||
| Ultrasonography (mm) | |||||
| Rectus femoris | FHSG | 22.5 ± 3.3 | 20.6 ± 4.3 | −1.9 *; d = 0.5 | 1.3 |
| CSG | 20.4 ± 3.7 | 19.3 ± 3.3 | −1.1 | ||
| Vastus intermedius | FHSG | 21.8 ± 3.9 | 19.5 ± 4.1 | −2.3 *; d = 0.6 | 3.1 |
| CSG | 17.0 ± 4.2 | 16.4 ± 5.0 | 0.6 | ||
| Vastus lateralis | FHSG | 24.7 ± 4.9 | 22.7 ± 4.7 | −2.0 *; d = 0.4 | 2.2 |
| CSG | 21.7 ± 4.7 | 20.6 ± 4.1 | −1.1 | ||
| Hamstrings | FHSG | 29.8 ± 4.6 | 30.9 ± 3.4 | 1.2 | −0.1 |
| CSG | 31.3 ± 4.0 | 31.0 ± 3.7 | −0.3 | ||
| Patellar tendon | FHSG | 4.5 ± 0.7 | 4.2 ± 0.7 | −0.3 | 0.4 |
| CSG | 4.0 ± 0.5 | 3.8 ± 0.5 | −0.2 | ||
| Achilles tendon | FHSG | 5.3 ± 1.5 | 5.3 ± 1.7 | −0.0 | 0.8 |
| CSG | 4.9 ± 1.4 | 6.0 ± 1.4 | 1.1 *; d = 0.8 | ||
| Plantaris fascia | FHSG | 3.2 ± 1.3 | 2.6 ± 0.6 | −0.5 | −0.1 |
| CSG | 2.5±0.4 | 2.8±0.8 | 0.3 | ||
| Measures | Time Median (Interquartile Range) | p Value Wilcoxon Test and Size Effect (r) | p Value U Mann-Whitney and Size Effect (r) | ||
|---|---|---|---|---|---|
| Pre | Post | Within-Group Differences | Between-Group Differences (Post) | ||
| OSTRC-O score | FHSG | 73.5 (24.5) | 47 (13) | p < 0.01 r = 0.7 | p < 0.001 r = 0.8 |
| CSG | 76.6 (4.5) | 67.5 (14.5) | p > 0.05 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gamez-Paya, J.; Dueñas, L.; Arnal-Gómez, A.; Benítez-Martínez, J.C. Foot and Lower Limb Clinical and Structural Changes in Overuse Injured Recreational Runners Using Floating Heel Shoes: Preliminary Results of a Randomised Control Trial. Sensors 2021, 21, 7814. https://0-doi-org.brum.beds.ac.uk/10.3390/s21237814
Gamez-Paya J, Dueñas L, Arnal-Gómez A, Benítez-Martínez JC. Foot and Lower Limb Clinical and Structural Changes in Overuse Injured Recreational Runners Using Floating Heel Shoes: Preliminary Results of a Randomised Control Trial. Sensors. 2021; 21(23):7814. https://0-doi-org.brum.beds.ac.uk/10.3390/s21237814
Chicago/Turabian StyleGamez-Paya, Javier, Lirios Dueñas, Anna Arnal-Gómez, and Josep Carles Benítez-Martínez. 2021. "Foot and Lower Limb Clinical and Structural Changes in Overuse Injured Recreational Runners Using Floating Heel Shoes: Preliminary Results of a Randomised Control Trial" Sensors 21, no. 23: 7814. https://0-doi-org.brum.beds.ac.uk/10.3390/s21237814