
New App-Based Dietary and Lifestyle Intervention on Weight Loss and Cardiovascular Health

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
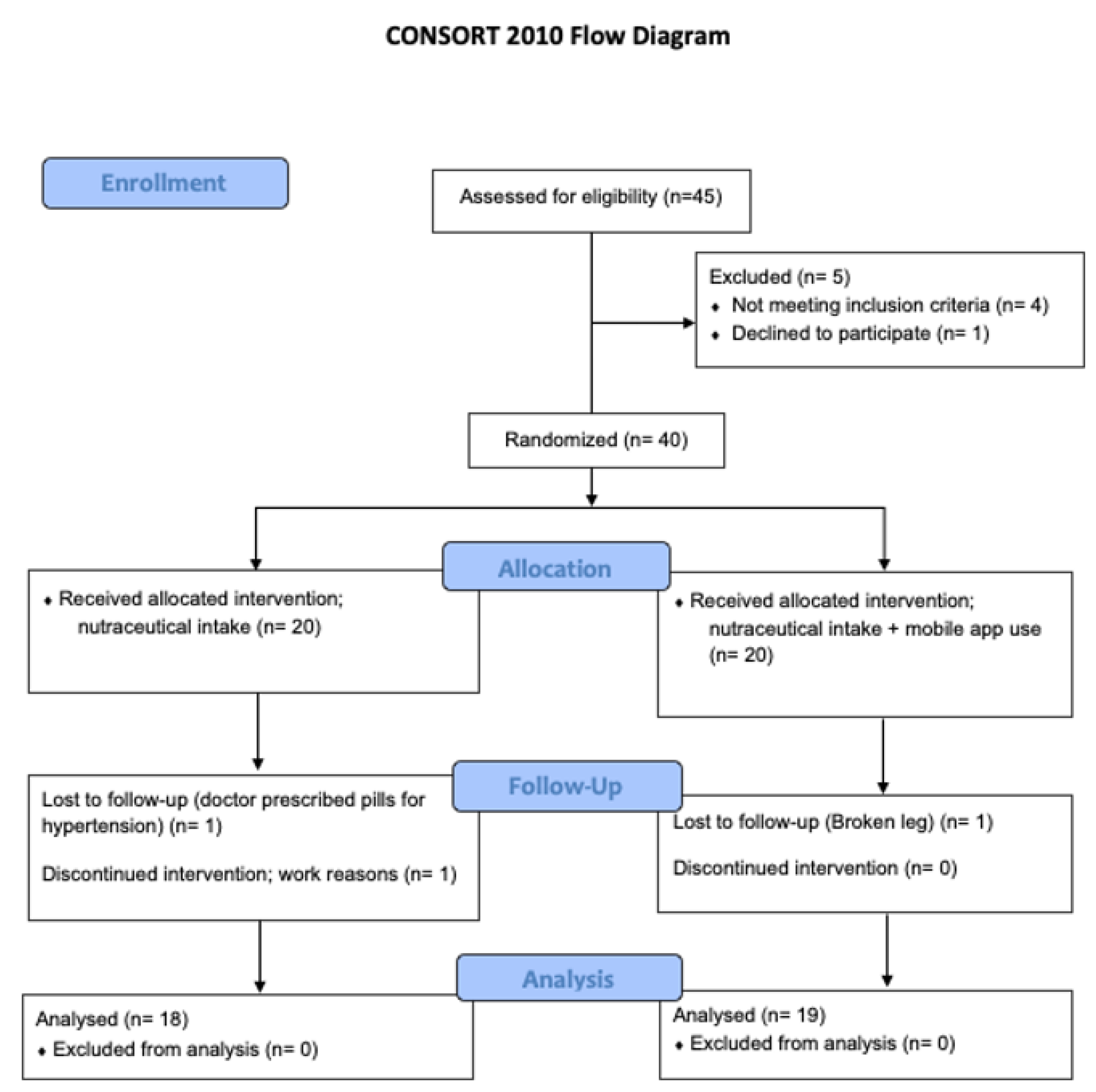
2.1. Study Design
2.2. Intervention
2.2.1. Dietary Supplement Formulation
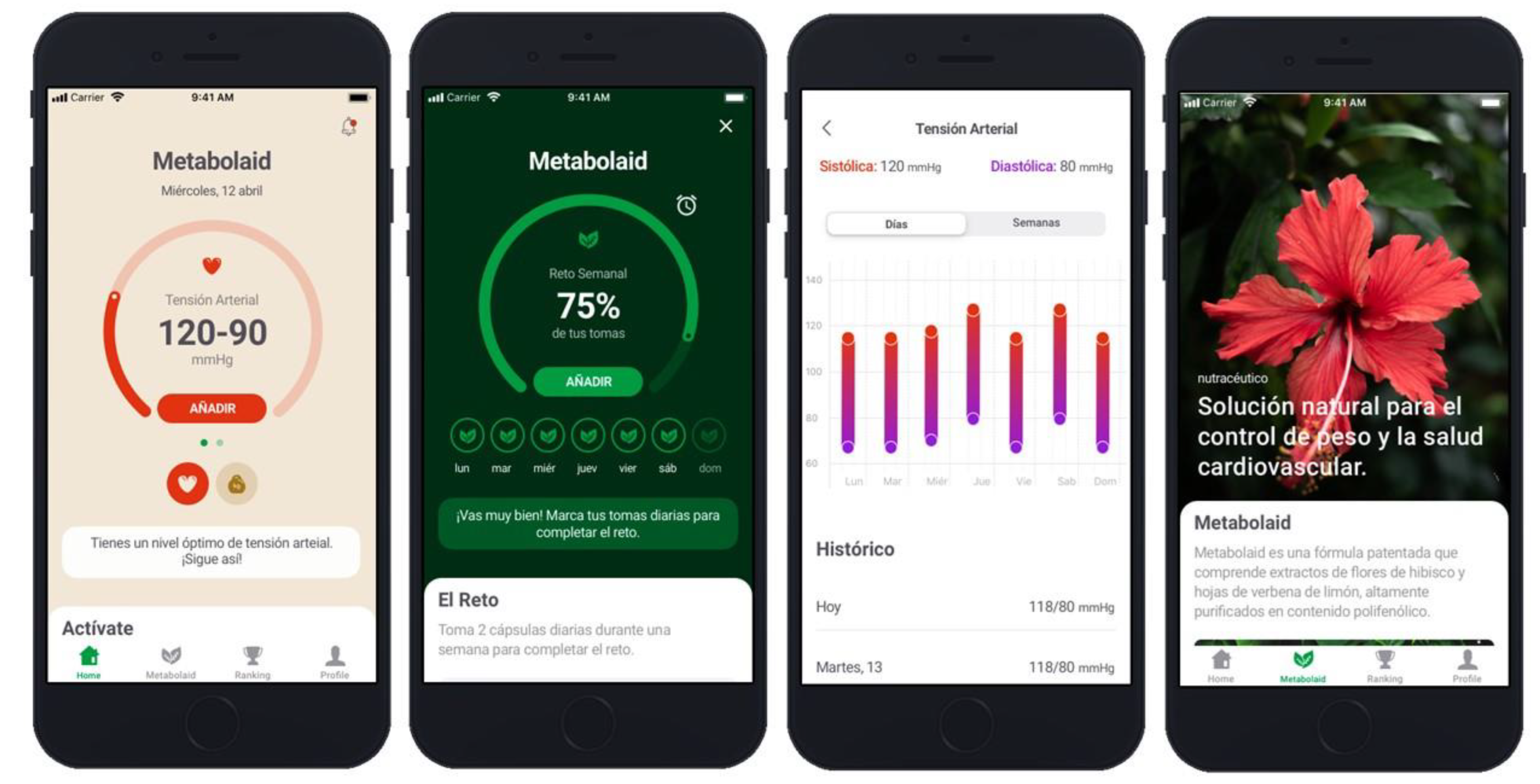
2.2.2. Mobile Application
2.3. Subjects
2.4. Trial Design
2.5. Declarations: Ethical Approval, Consent to Participate and Consent for Publication
2.6. Data Collection
2.6.1. Blood Pressure
2.6.2. Body Composition—Bioimpedance
2.6.3. Body Composition (BC)—Anthropometric Measurements
2.6.4. Triglycerides
2.6.5. Peak Expiratory Flow (PEF) and Forced Expiratory Volume in the First Second (FEV1)
2.6.6. Maximum Oxygen Uptake (VO2max)
2.6.7. Remote Physical Activity Tracking
2.6.8. Diet Record
2.6.9. Subject Opinion on App
2.7. Statistical Analysis
3. Results
3.1. Dietary Assessment
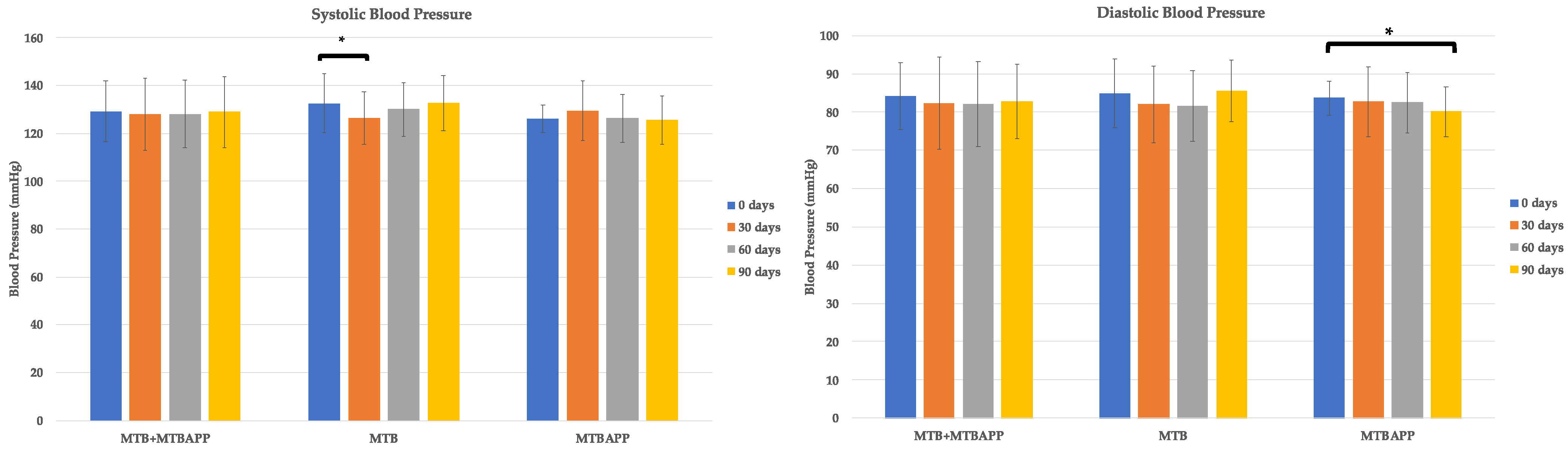
3.2. Blood Pressure
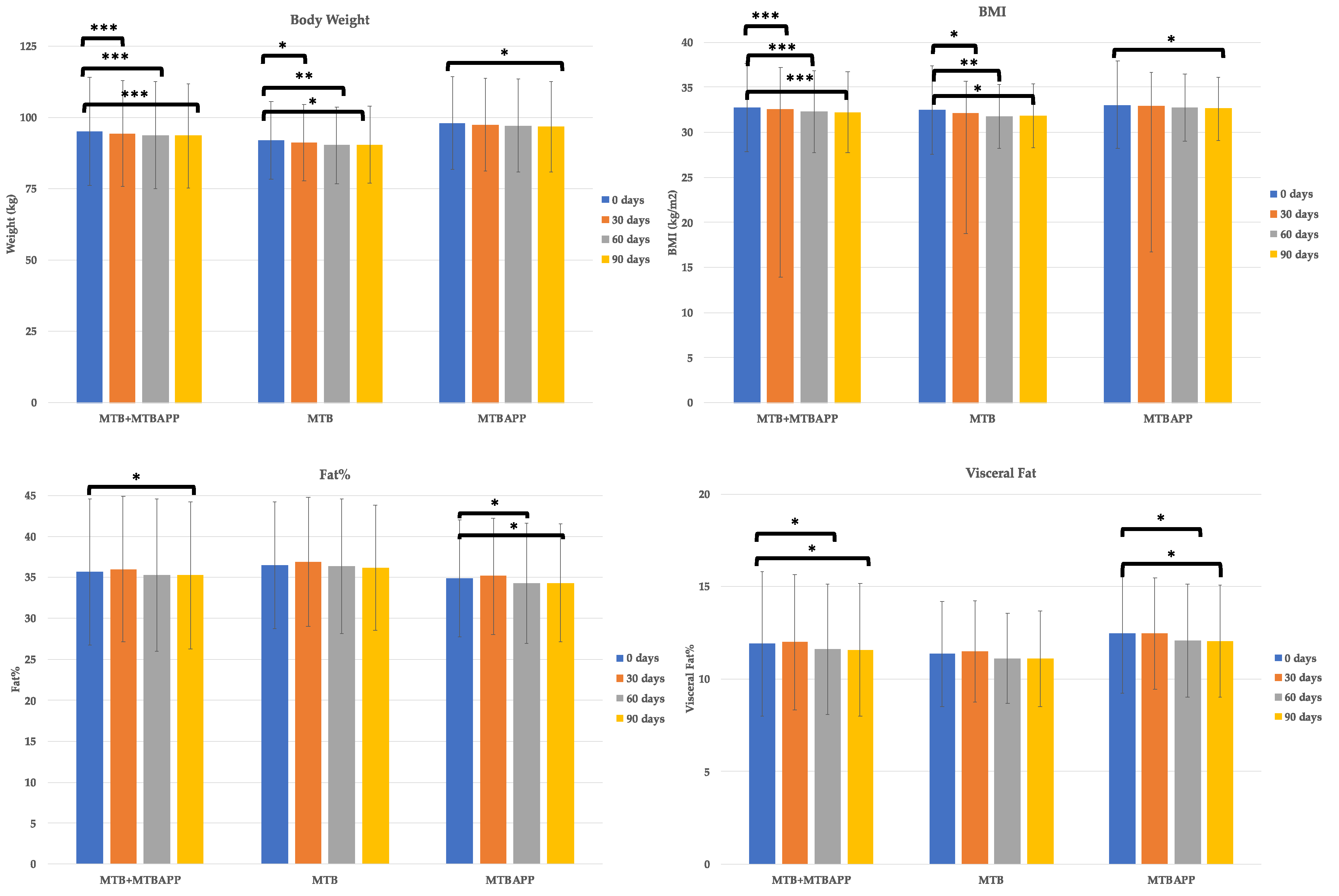
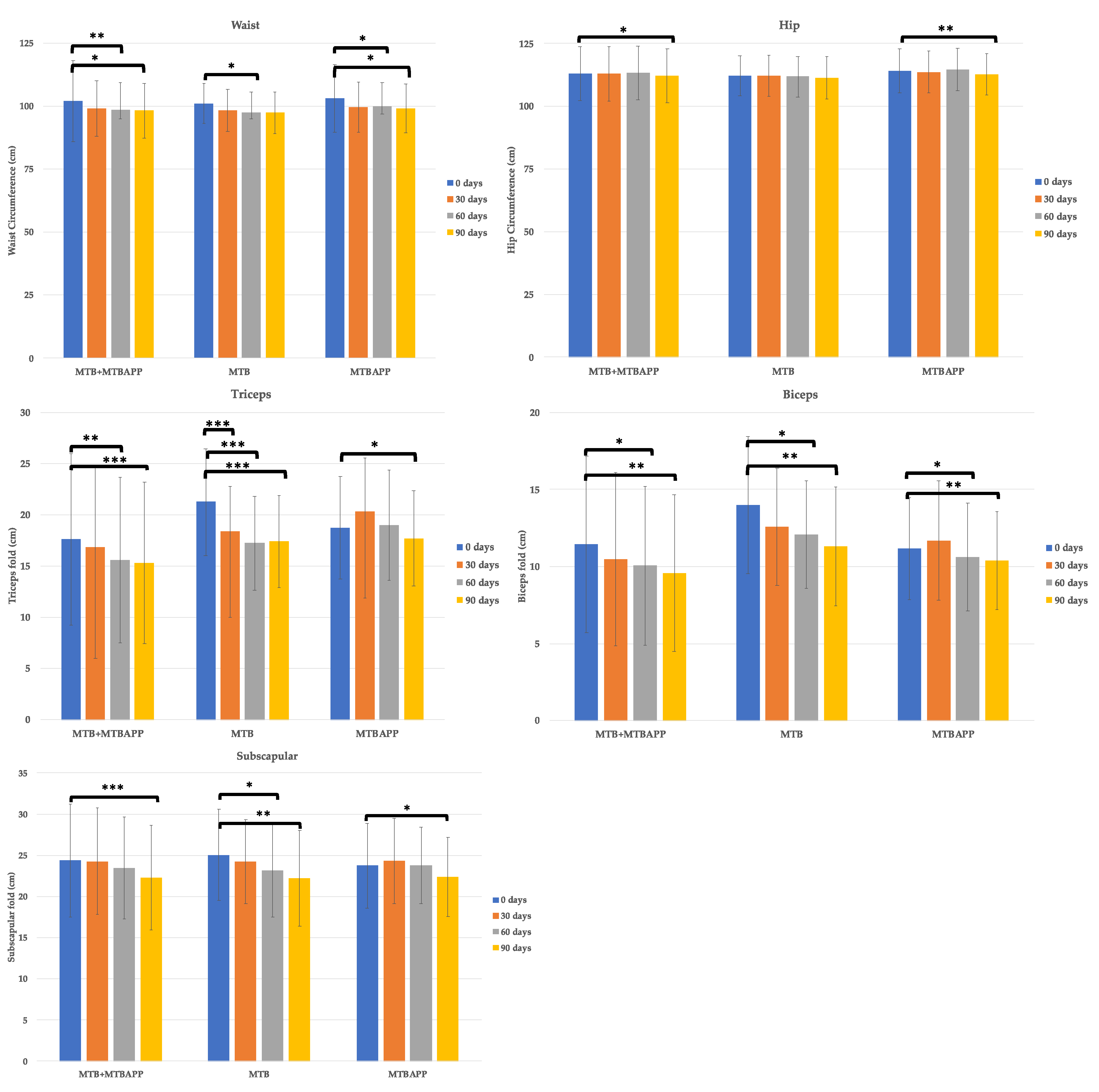
3.3. Body Weight, Bioelectric Impedance, and Anthropometric Measurements
3.4. Spirometry, Triglycerides, and One-Mile Walk
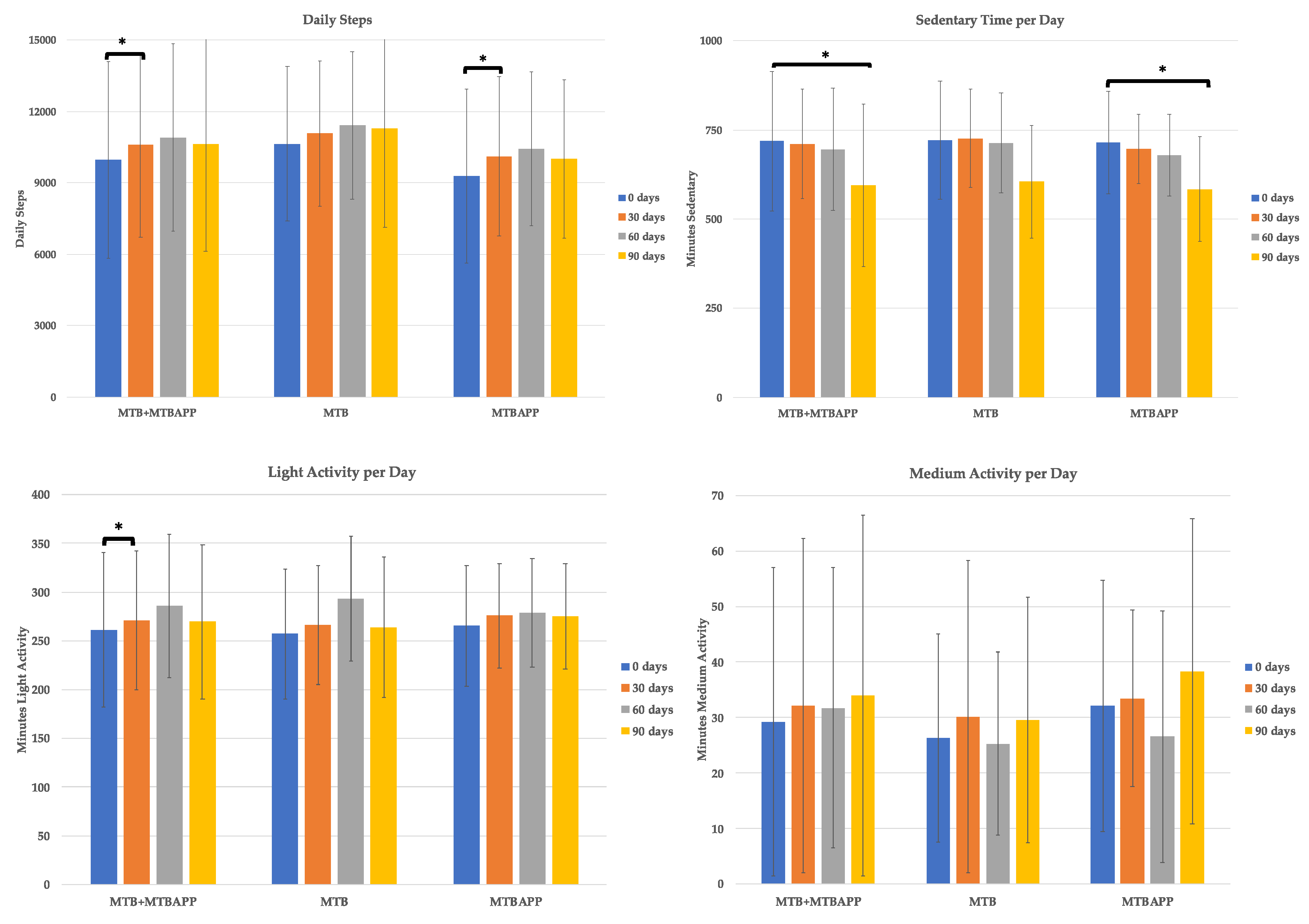
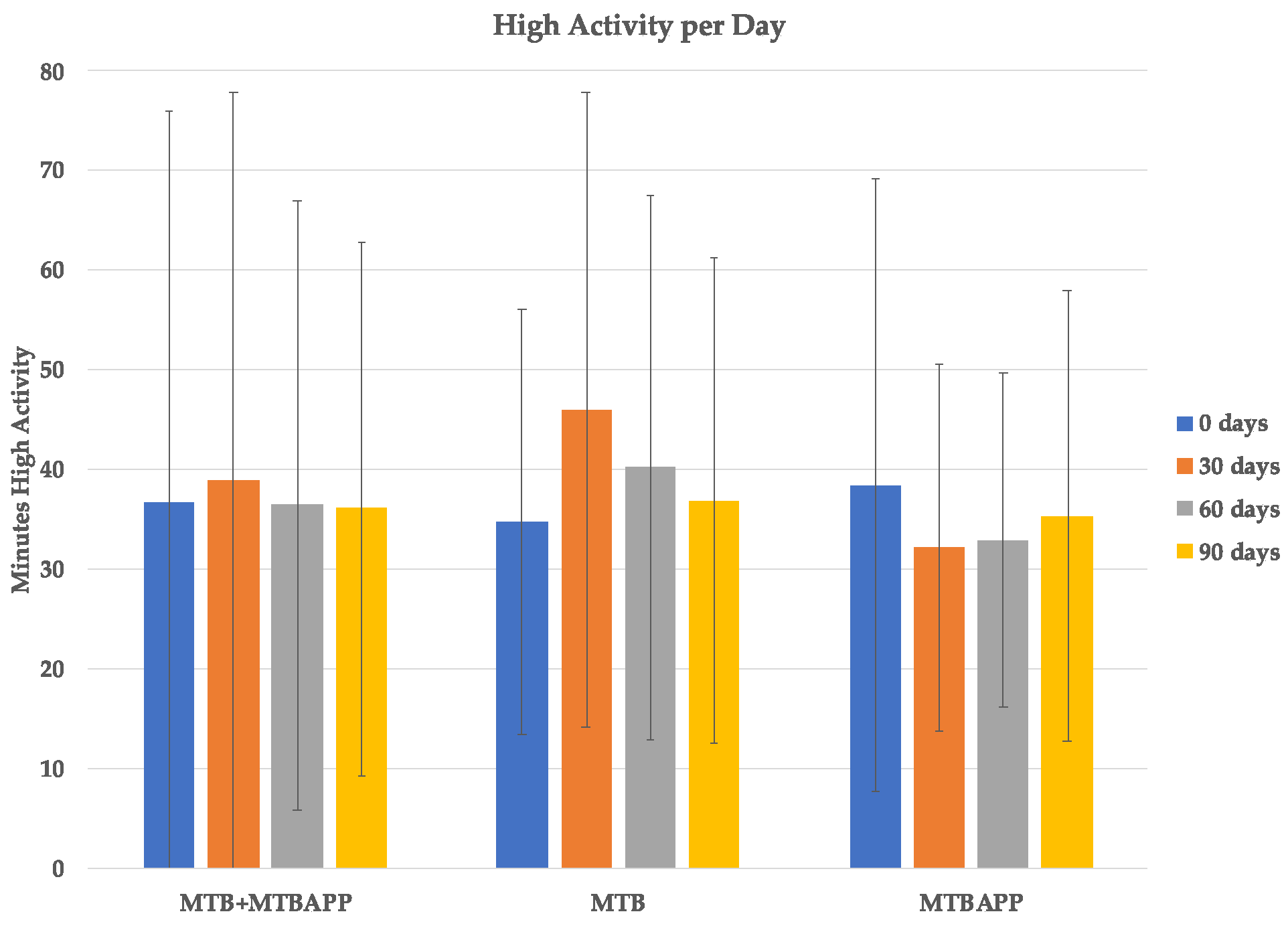
3.5. Physical Activity Data (Fitbit Trackers)
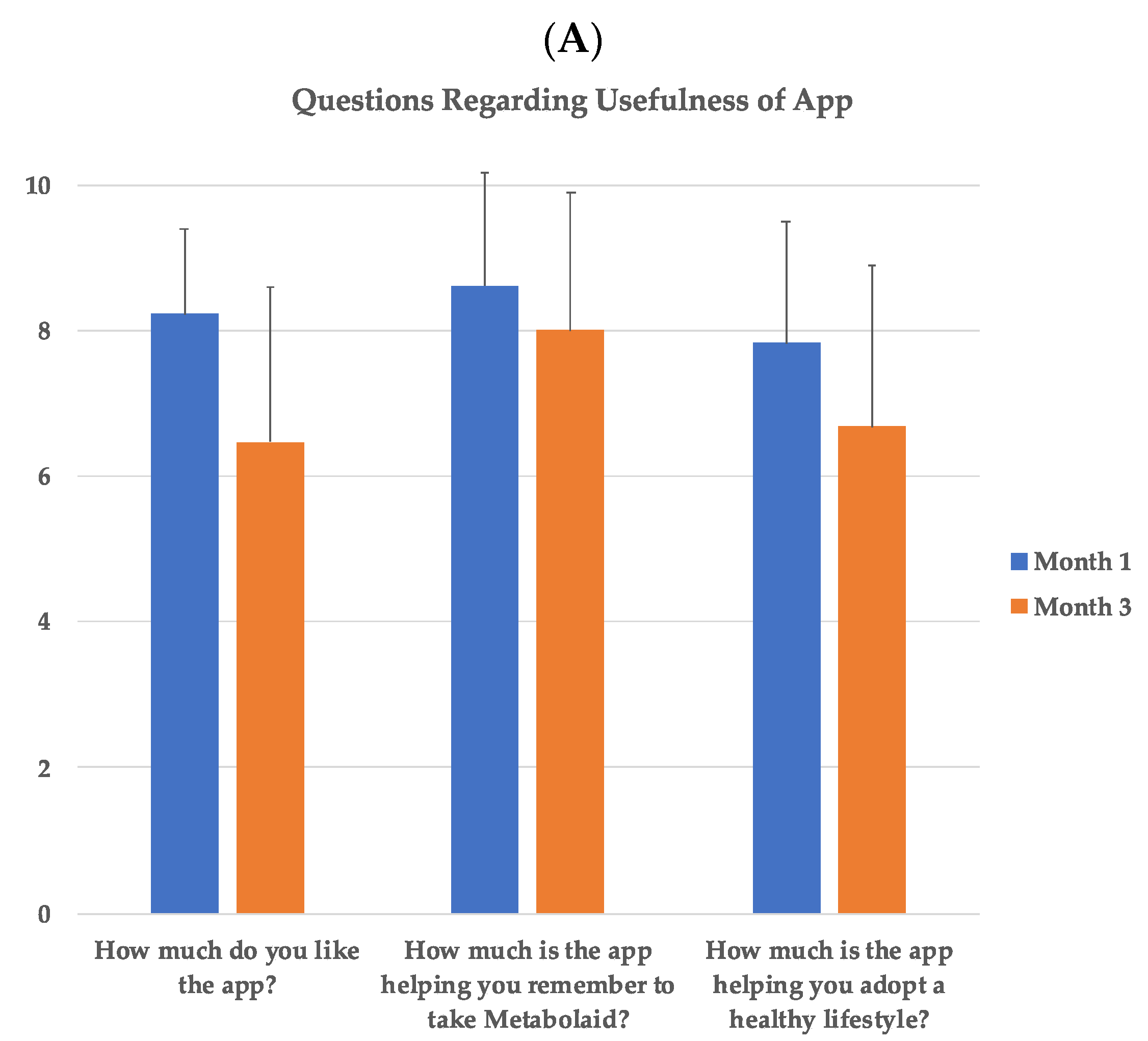
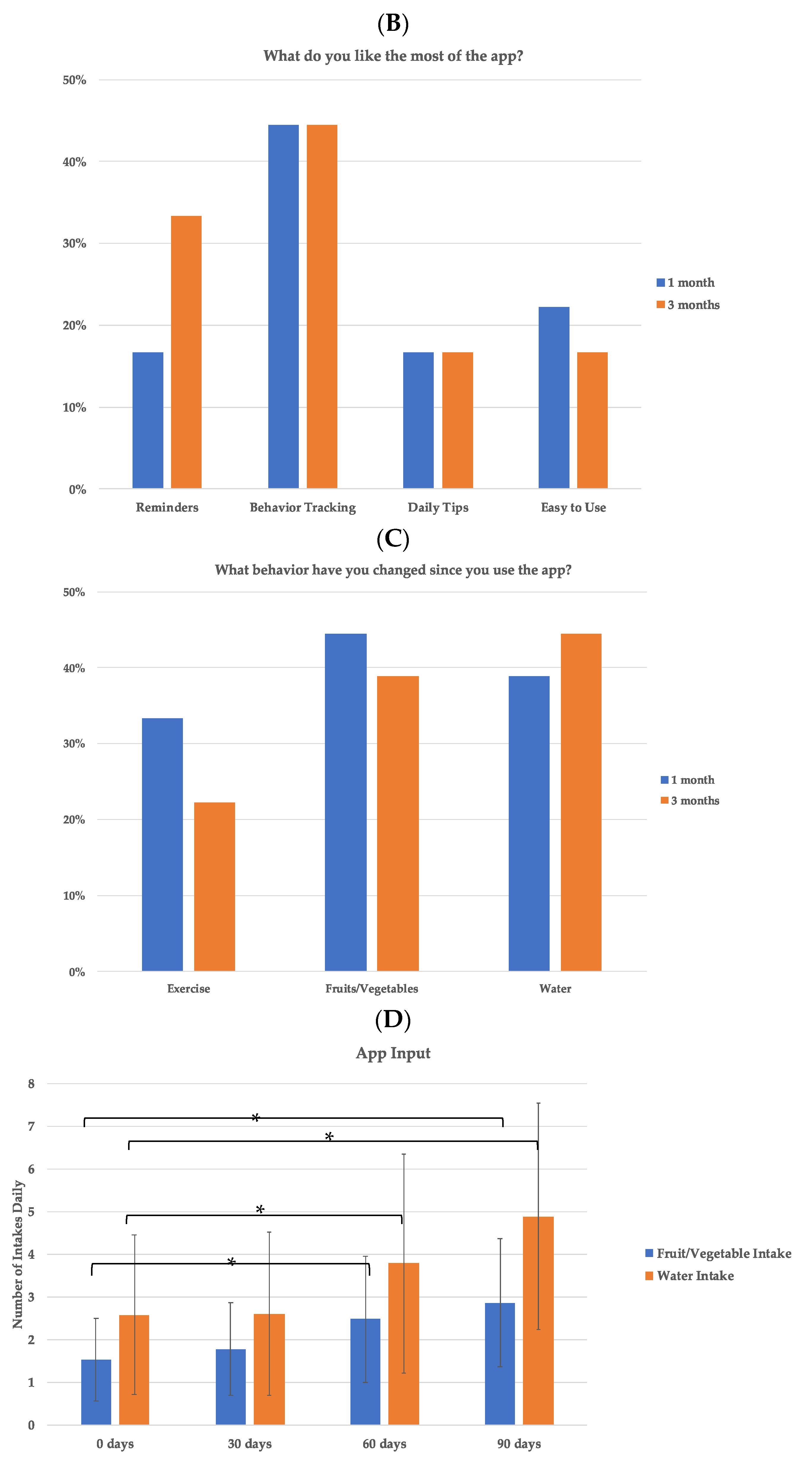
3.6. Subject Opinion on App
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Deng, G.; Yin, L.; Liu, W.; Liu, X.; Xiang, Q.; Qian, Z.; Ma, J.; Chen, H.; Wang, Y.; Hu, B.; et al. Associations of anthropometric adiposity indexes with hypertension risk: A systematic review and meta-analysis including PURE-China. Medicine 2018, 97, e13262. [Google Scholar] [CrossRef]
- Han, T.S.; Al-Gindan, Y.Y.; Govan, L.; Hankey, C.R.; Lean, M.E.J. Associations of BMI, waist circumference, body fat, and skeletal muscle with type 2 diabetes in adults. Acta Diabetol. 2019, 56, 947–954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whelton, P.K.; Williams, B. The 2018 European Society of Cardiology/European Society of Hypertension and 2017 American College of Cardiology/American Heart Association Blood Pressure Guidelines: More Similar than Different. JAMA 2018, 320, 1749–1750. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Jurik, R.; Stastny, P. Role of Nutrition and Exercise Programs in Reducing Blood Pressure: A Systematic Review. J. Clin. Med. 2019, 8, 1393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Homayouni, F.; Haidari, F.; Hedayati, M.; Zakerkish, M.; Ahmadi, K. Blood pressure lowering and anti-inflammatory effects of hesperidin in type 2 diabetes; a randomized double-blind controlled clinical trial. Phyther. Res. 2018, 32, 1073–1079. [Google Scholar] [CrossRef]
- Serban, C.; Sahebkar, A.; Ursoniu, S.; Andrica, F.; Banach, M. Effect of sour tea (Hibiscus sabdariffa L.) on arterial hypertension. J. Hypertens. 2015, 33, 1119–1127. [Google Scholar] [CrossRef] [Green Version]
- Xiong, X.; Wang, P.; Zhang, Y.; Li, X. Effects of traditional Chinese patent medicine on essential hypertension: A systematic review. Medicine 2015, 94, e442. [Google Scholar] [CrossRef] [PubMed]
- Dunn, J.; Runge, R.; Snyder, M. Wearables and the medical revolution. Per. Med. 2018, 15, 429–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- da Silva, V.J.; Souza, V.d.S.; da Cruz, R.G.; de Lucena, J.M.V.M.; Jazdi, N.; Junior, V.F.d.L. Commercial Devices-Based System Designed to Improve the Treatment Adherence of Hypertensive Patients. Sensors 2019, 19, 4539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SM, H. Medication Non-adherence: A Major Cause of Resistant Hypertension. Curr. Cardiol. Rep. 2020, 22, 1–7. [Google Scholar]
- Lee, C.J.; Kim, J.Y.; Shim, E.; Hong, S.H.; Lee, M.; Jeon, J.Y.; Park, S. The Effects of Diet Alone or in Combination with Exercise in Patients with Prehypertension and Hypertension: A Randomized Controlled Trial. Korean Circ. J. 2018, 48, 637–651. [Google Scholar] [CrossRef] [PubMed]
- Research2guidance—mHealth Economics 2016—Current Status and Trends of the mHealth App Market. Available online: https://research2guidance.com/product/mhealth-app-developer-economics-2016/ (accessed on 4 October 2021).
- Saghaei, M. An overview of randomization and minimization programs for randomized clinical trials. J. Med. Signals Sens. 2011, 1, 55–61. [Google Scholar] [CrossRef] [Green Version]
- Boix-Castejón, M.; Herranz-López, M.; Gago, A.P.; Olivares-Vicente, M.; Caturla, N.; Roche, E.; Micol, V. Correction: Hibiscus and lemon verbena polyphenols modulate appetite-related biomarkers in overweight subjects: A randomized controlled trial. Food Funct. 2018, 9, 4037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herranz-López, M.; Olivares-Vicente, M.; Encinar, J.A.; Barrajón-Catalán, E.; Segura-Carretero, A.; Joven, J.; Micol, V. Multi-targeted molecular effects of Hibiscus sabdariffa polyphenols: An opportunity for a global approach to obesity. Nutrients 2017, 9, 907. [Google Scholar] [CrossRef] [PubMed]
- Khalil, S.F.; Mohktar, M.S.; Ibrahim, F. The theory and fundamentals of bioimpedance analysis in clinical status monitoring and diagnosis of diseases. Sensors 2014, 14, 10895–10928. [Google Scholar] [CrossRef] [PubMed]
- Heaney, S.; O’Connor, H.; Michael, S.; Gifford, J.; Naughton, G. Nutrition knowledge in athletes: A systematic review. Int. J. Sport Nutr. Exerc. Metab. 2011, 21, 248–261. [Google Scholar] [CrossRef] [Green Version]
- da Silva, V.S.; Vieira, M.F.S. International society for the advancement of kinanthropometry (Isak) global: International accreditation scheme of the competent anthropometrist. Rev. Bras. Cineantropometria E Desempenho Hum. 2020, 22, 1–6. [Google Scholar] [CrossRef]
- Scafoglieri, A.; Tresignie, J.; Provyn, S.; Clarys, J.P.; Bautmans, I. Reproducibility, accuracy and concordance of Accutrend Plus for measuring circulating lipid concentration in adults. Biochem. Med. 2012, 22, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Ramos Hernández, C.; Núñez Fernández, M.; Pallares Sanmartín, A.; Mouronte Roibas, C.; Cerdeira Domínguez, L.; Botana Rial, M.I.; Blanco Cid, N.; Fernández Villar, A. Validation of the portable Air-Smart Spirometer. PLoS ONE 2018, 13, e0192789. [Google Scholar] [CrossRef]
- García-Río, F.; Calle Rubio, M.; Burgos, F.; Casan, P.; del Campo, F.; Gáldiz, J.; Giner, J.; González-Mangado, N.; Ortega, F.; Puente-Maestu, L. Spirometry. Spanish Society of Pulmonology and Thoracic Surgery (SEPAR). Arch. Bronconeumol. 2013, 49, 388–401. [Google Scholar] [CrossRef]
- Pober, D.M.; Freedson, P.S.; Kline, G.M.; McInnis, K.J.; Rippe, J.M. Development and validation of a one-mile treadmill walk test to predict peak oxygen uptake in healthy adults ages 40 to 79 years. Can. J. Appl. Physiol. 2002, 27, 575–589. [Google Scholar] [CrossRef] [Green Version]
- Tedesco, S.; Sica, M.; Ancillao, A.; Timmons, S.; Barton, J.; O’Flynn, B. Validity Evaluation of the Fitbit Charge2 and the Garmin vivosmart HR+ in Free-Living Environments in an Older Adult Cohort. JMIR mHealth uHealth 2019, 7, e13084. [Google Scholar] [CrossRef]
- Villinger, K.; Wahl, D.R.; Boeing, H.; Schupp, H.T.; Renner, B. The effectiveness of app-based mobile interventions on nutrition behaviours and nutrition-related health outcomes: A systematic review and meta-analysis. Obes. Rev. 2019, 20, 1465. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.-S.; Yang, W.-K.; Kim, H.Y.; Min, B.; Caturla, N.; Jones, J.; Park, Y.-C.; Lee, Y.-C.; Kim, S.-H. Metabolaid® Combination of Lemon Verbena and Hibiscus Flower Extract Prevents High-Fat Diet-Induced Obesity through AMP-Activated Protein Kinase Activation. Nutrients 2018, 10, 1204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boix-Castejón, M.; Herranz-López, M.; Olivares-Vicente, M.; Campoy, P.; Caturla, N.; Jones, J.; Zazo, J.M.; Roche, E.; Micol, V. Effect of metabolaid® on pre- and stage 1 hypertensive patients: A randomized controlled trial. J. Funct. Foods 2021, 84, 104583. [Google Scholar] [CrossRef]
- Marhuenda, J.; Perez-Piñero, S.; Victoria-Montesinos, D.; Abellán-Ruiz, M.S.; Caturla, N.; Jones, J.; López-Román, J. Correction: Marhuenda, J.; et al. A Randomized, Double-Blind, Placebo Controlled Trial to Determine the Effectiveness a Polyphenolic Extract (Hibiscus sabdariffa and Lippia citriodora) in the Reduction of Body Fat Mass in Healthy Subjects. Foods 2020, 9, 279. [Google Scholar] [CrossRef] [Green Version]
- Lenoir, L.; Rossary, A.; Joubert-Zakeyh, J.; Vergnaud-Gauduchon, J.; Farges, M.C.; Fraisse, D.; Texier, O.; Lamaison, J.L.; Vasson, M.P.; Felgines, C. Lemon verbena infusion consumption attenuates oxidative stress in dextran sulfate sodium-induced colitis in the rat. Dig. Dis. Sci. 2011, 56, 3534–3545. [Google Scholar] [CrossRef]
- Herranz-López, M.; Barrajón-Catalán, E.; Segura-Carretero, A.; Menéndez, J.A.; Joven, J.; Micol, V. Lemon verbena (Lippia citriodora) polyphenols alleviate obesity-related disturbances in hypertrophic adipocytes through AMPK-dependent mechanisms. Phytomedicine 2015, 22, 605–614. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.S.; Kim, J.K.; Kim, H.J.; Moon, S.R.; Shin, B.C.; Park, K.W.; Yang, H.O.; Kim, S.M.; Park, R. Hibiscus extract inhibits the lipid droplet accumulation and adipogenic transcription factors expression of 3T3-L1 preadipocytes. J. Altern. Complement. Med. 2003, 9, 499–504. [Google Scholar] [CrossRef]
- Hirunpanich, V.; Utaipat, A.; Morales, N.P.; Bunyapraphatsara, N.; Sato, H.; Herunsale, A.; Suthisisang, C. Hypocholesterolemic and antioxidant effects of aqueous extracts from the dried calyx of Hibiscus sabdariffa L. in hypercholesterolemic rats. J. Ethnopharmacol. 2006, 103, 252–260. [Google Scholar] [CrossRef]
- Laranjo, L.; Quiroz, J.C.; Tong, H.L.; Bazalar, M.A.; Coiera, E. A Mobile Social Networking App for Weight Management and Physical Activity Promotion: Results From an Experimental Mixed Methods Study. J. Med. Internet Res. 2020, 22, e19991. [Google Scholar] [CrossRef]
- Elliott, M.; Eck, F.; Khmelev, E.; Derlyatka, A.; Fomenko, O. Physical Activity Behavior Change Driven by Engagement with an Incentive-Based App: Evaluating the Impact of Sweatcoin. JMIR mHealth uHealth 2019, 7, e12445. [Google Scholar] [CrossRef] [Green Version]
- Serna, A.; Marhuenda, J.; Arcusa, R.; Pérez-Piñero, S.; Sánchez-Macarro, M.; García-Muñoz, A.M.; Victoria-Montesinos, D.; Cánovas, F.; López-Román, F.J. Effectiveness of a polyphenolic extract (Lippia citriodora and Hibiscus sabdariffa) on appetite regulation in overweight and obese grade I population: An 8-week randomized, double-blind, cross-over, placebo-controlled trial. Eur. J. Nutr. 2021, 1–17. [Google Scholar] [CrossRef]
- Marhuenda, J.; Pérez-Piñero, S.; Arcusa, R.; Victoria-Montesinos, D.; Cánovas, F.; Sánchez-Macarro, M.; García-Muñoz, A.M.; Querol-Calderón, M.; López-Román, F.J. A Randomized, Double-Blind, Placebo-Controlled Trial to Determine the Effectiveness of a Polyphenolic Extract (Hibiscus sabdariffa and Lippia citriodora) for Reducing Blood Pressure in Prehypertensive and Type 1 Hypertensive Subjects. Molecules 2021, 26, 1783. [Google Scholar] [CrossRef]
- Cheen, M.H.H.; Tan, Y.Z.; Oh, L.F.; Wee, H.L.; Thumboo, J. Prevalence of and factors associated with primary medication non-adherence in chronic disease: A systematic review and meta-analysis. Int. J. Clin. Pract. 2019, 73, e13350. [Google Scholar] [CrossRef]
- Marinho, F.S.; Moram, C.B.M.; Rodrigues, P.C.; Leite, N.C.; Salles, G.F.; Cardoso, C.R.L. Treatment Adherence and Its Associated Factors in Patients with Type 2 Diabetes: Results from the Rio de Janeiro Type 2 Diabetes Cohort Study. J. Diabetes Res. 2018, 2018, 8970196. [Google Scholar] [CrossRef]
- West, J.H.; Belvedere, L.M.; Andreasen, R.; Frandsen, C.; Cougar Hall, P.; Crookston, B.T. Controlling Your “App” etite: How Diet and Nutrition-Related Mobile Apps Lead to Behavior Change. JMIR mHealth uHealth 2017, 5, e95. [Google Scholar] [CrossRef]
- Fogg, B.J. Tiny Habits: The Small Changes That Change Everything; Houghton Mifflin Harcourt: Boston, MA, USA, 2019; 306p. [Google Scholar]
- Predictably Irrational: The Hidden Forces That Shape Our Decisions. PsycNET. Available online: https://psycnet.apa.org/record/2008-04432-000 (accessed on 4 October 2021).
- Zhang, Z.; Monro, J.; Venn, B.J. Development and Evaluation of an Internet-Based Diabetes Nutrition Education Resource. Nutrients 2019, 11, 1217. [Google Scholar] [CrossRef] [Green Version]
- Lisón, J.F.; Palomar, G.; Mensorio, M.S.; BAnõs, R.M.; Cebolla-Martí, A.; Botella, C.; Benavent-Caballer, V.; Rodilla, E. Impact of a Web-Based Exercise and Nutritional Education Intervention in Patients Who Are Obese with Hypertension: Randomized Wait-List Controlled Trial. J. Med. Internet Res. 2020, 22, e14196. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MTB (n = 18) | MTBAPP (n = 19) | p Value | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Age (years) | 46.1 ± 10.4 | 45.3 ± 6.40 | 0.858 |
| Systolic BP (mmHg) | 132 ± 16.3 | 126 ± 7.11 | 0.117 |
| Diastolic BP (mmHg) | 84.9 ± 11.7 | 83.8 ± 4.69 | 0.695 |
| Height (cm) | 167 ± 10.1 | 172 ± 8.47 | 0.322 |
| Weight (kg) | 90.9 ± 17.0 | 99.1 ± 21.6 | 0.359 |
| BMI (kg/m2) | 32.7 ± 4.75 | 33.2 ± 5.52 | 0.841 |
| Fat % | 37.0 ± 9.30 | 34.8 ± 8.53 | 0.606 |
| Visceral Fat % | 11.4 ± 3.70 | 12.9 ± 4.59 | 0.399 |
| Waist (cm) | 101 ± 10.5 | 105 ± 22.3 | 0.706 |
| Hip (cm) | 112 ± 10.7 | 115 ± 11.7 | 0.585 |
| Abd. perimeter (cm) | 108 ± 12.0 | 113 ± 16.4 | 0.577 |
| Triceps folds (mm) | 21.9 ± 6.30 | 19.0 ± 6.76 | 0.251 |
| Bicep folds (mm) | 14.4 ± 5.36 | 10.9 ± 3.98 | 0.076 |
| Subscapular folds (mm) | 24.6 ± 7.18 | 22.1 ± 6.06 | 0.573 |
| PEF (L/m) | 373 ± 150 | 520 ± 168 | 0.510 |
| FEV1 spirometry (L) | 3.02 ± 0.954 | 3.54 ± 0.716 | 0.198 |
| Triglycerides (mg/dL) | 138 ± 86.8 | 156 ± 138 | 0.674 |
| Time walk 1 mile (min) | 16.8 ± 2.33 | 16.8 ± 3.22 | 0.526 |
| Heart rate post-walk (bpm) | 121 ± 11.6 | 131 ± 14.2 | 0.515 |
| VO2 max (ml/kg/min) | 28.0 ± 12.6 | 26.4 ± 11.0 | 0.909 |
| 0 Days | 90 Days | 0 Days | 90 Days | Effect Time × Group | |||
|---|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | F | p | η2 | |
| Kcal | 1806 ± 511 | 1722 ± 483 | 1796 ± 431 | 1774 ± 337 | 0.413 | 0.525 | 0.012 |
| Carb (g) | 175 ± 59.2 | 173 ± 57.2 | 166 ± 45.2 | 168 ± 41.9 | 0.062 | 0.804 | 0.002 |
| Prot (g) | 102 ± 31.9 | 78.6 ± 27.5 | 94.2 ± 19.5 | 92.6 ± 14.7 | 5.580 | 0.024 * | 0.138 |
| Lip (g) | 75.7 ± 28.7 | 73.0 ± 23.1 | 78.7 ± 22.8 | 76.3 ± 20.9 | 0.001 | 0.965 | 0.000 |
| Vit. B12 (mg) | 4.51 ± 2.48 | 5.22 ± 4.16 | 6.80 ± 3.32 | 7.10 ± 6.43 | 0.047 | 0.829 | 0.001 |
| Na (mg) | 1783 ± 1403 | 2019 ± 1598 | 2604 ± 1323 | 2345 ± 1488 | 125.4 | 0.270 | 0.035 |
| Ca (mg) | 755 ± 330 | 841 ± 325 | 697 ± 286 | 759 ± 311 | 0.030 | 0.862 | 0.001 |
| Fe (mg) | 2.26 ± 1.18 | 1.92 ± 0.836 | 2.42 ± 0.423 | 2.16 ± 0.412 | 0.037 | 0.847 | 0.001 |
| Vit. C (mg) | 121 ± 81.6 | 127 ± 82.3 | 158 ± 87.3 | 158 ± 75.0 | 0.047 | 0.829 | 0.001 |
| Vit. D (µg) | 46.1 ± 63.9 | 10.6 ± 17.3 | 4.65 ± 3.92 | 54.5 ± 95.6 | 9.359 | 0.104 | 0.211 |
| Chol. (mg) | 340 ± 274 | 315 ± 190 | 322 ± 111 | 351 ± 125 | 0.451 | 0.506 | 0.013 |
| MTB | MTBAPP | |||
|---|---|---|---|---|
| 0 Days | 90 Days | 0 Days | 90 Days | |
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |
| Spirometry PEF (L/min) | 378.94 ± 147.60 | 398.78 ± 131.36 | 507.84 ± 157.48 | 496.63 ± 160.19 |
| Spirometry FEV1 (L) | 3.08 ± 0.95 | 3.18 ± 0.78 | 3.44 ± 0.70 | 3.45 ± 0.63 |
| Triglycerides (mg/dL) | 169.46 ± 76.20 | 204.00 ± 84.37 | 189.32 ± 121.64 | 163.42 ± 34.21 |
| Time to walk 1 mile (min.) | 17.19 ± 2.81 | 16.53 ± 2.46 | 16.56 ± 3.10 | 15.69 ± 2.37 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Rodríguez, A.; Martínez-Olcina, M.; Mora, J.; Navarro, P.; Caturla, N.; Jones, J. New App-Based Dietary and Lifestyle Intervention on Weight Loss and Cardiovascular Health. Sensors 2022, 22, 768. https://0-doi-org.brum.beds.ac.uk/10.3390/s22030768
Martínez-Rodríguez A, Martínez-Olcina M, Mora J, Navarro P, Caturla N, Jones J. New App-Based Dietary and Lifestyle Intervention on Weight Loss and Cardiovascular Health. Sensors. 2022; 22(3):768. https://0-doi-org.brum.beds.ac.uk/10.3390/s22030768
Chicago/Turabian StyleMartínez-Rodríguez, Alejandro, María Martínez-Olcina, Juan Mora, Pau Navarro, Nuria Caturla, and Jonathan Jones. 2022. "New App-Based Dietary and Lifestyle Intervention on Weight Loss and Cardiovascular Health" Sensors 22, no. 3: 768. https://0-doi-org.brum.beds.ac.uk/10.3390/s22030768