This section firstly addresses the statistical characterization of the RNFL thickness values using all previous asymmetry metrics. The mean, standard deviation and p-value were calculated for the subsets of healthy and glaucoma patients. Next, the chosen machine learning models, decision trees, are briefly described, and the design process for glaucoma screening is detailed.
3.1. Statistical Characterization of the Asymmetry Metrics
The thickness asymmetry has been calculated with the proposed metrics for each sector of the OCT and for the overall RNFL, considering two subsets, healthy and glaucoma patients (see
Table 2). In order to analyze the relevance of each asymmetry metric, statistical characterization has been performed.
Table 4 gathers the mean value, standard deviation and
p-value of each metric for all sectors (TS, T, TI, NS, N and NI) and for entire OCT scan (G) for the two subsets of healthy and glaucoma patients. The values of the non-normalized metrics
and
are given in µm, whereas the values of the normalized metrics are dimensionless and range from −1 to 1 in the case of
,
and
, and from 0 up to 1 in the case of the metrics based on the absolute value, i.e.,
,
and
.
As can be seen in
Table 4, the metrics not using absolute value (
,
,
and
) have mean values centered at zero and standard deviations lower in the group of healthy individuals than in the group of glaucoma patients. According to the definitions of these asymmetry metrics
,
,
and
, the statistical distributions of such asymmetry values will have be normal when the number of patients is high enough, due to the central limit theorem. The means of these normal distributions will always be approximately zero, considering that the direction in which the subtraction is calculated has been arbitrarily chosen, and the asymmetry must occur equiprobably in both directions (from the left eye to the right, or vice versa). Then, since the values follow a normal distribution with a zero mean, the variance of the distributions will be the distinguishing factor in the screening of healthy and glaucoma patients.
On the other hand, metrics based on the absolute value (
,
,
and
) have mean values greater than zero and standard deviations for the glaucoma subset slightly higher than for the subset of healthy patients. The absolute values of the asymmetry metrics cause normal distributions to become half-normal distributions [
31]. The mean of the half-normal distribution is
where
is the standard deviation of the initial normal distribution. That is, the mean of the new half-normal distribution is determined, proportionally, by the variance of the initial normal distribution, allowing the use of thresholds for the discrimination of healthy and glaucoma patients. Note that a greater variance will imply a higher mean value after taking the absolute value of the asymmetry for a specific sector.
The third characteristic gathered in
Table 4 is the
p-value, which determines the statistical significance of the hypothesis that the asymmetry of the RNFL thickness is statistically related to the occurrence of glaucoma disease. Then, a low
p-value indicates that the asymmetry metric in a given sector has sufficient statistical significance in the occurrence of glaucoma between the healthy and glaucoma subset of patients. Taking this into account, since the
p-values of the metrics
and
are the smallest of all the proposed metrics,
and
are the most useful and relevant as discriminant variables in patient classification.
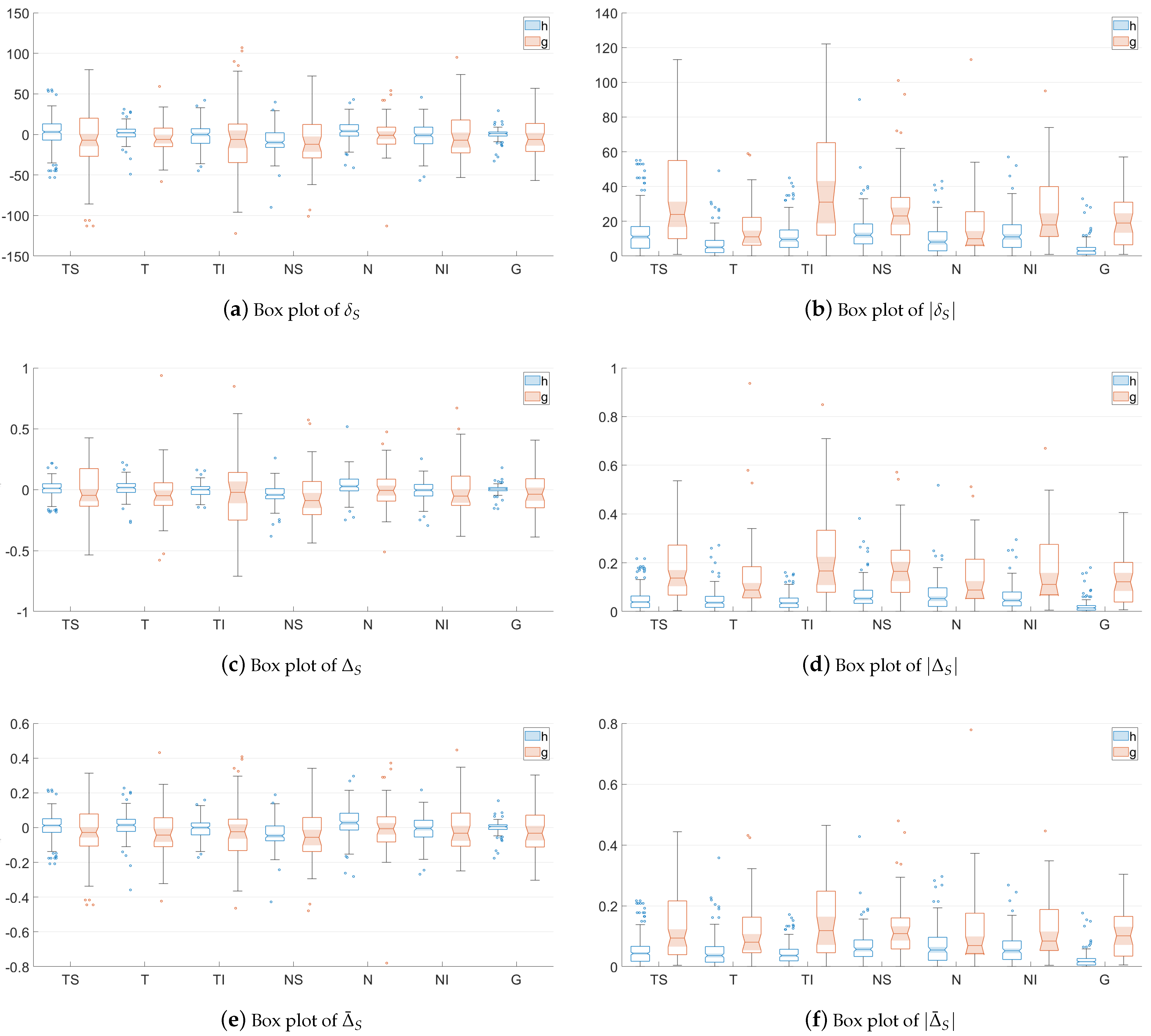
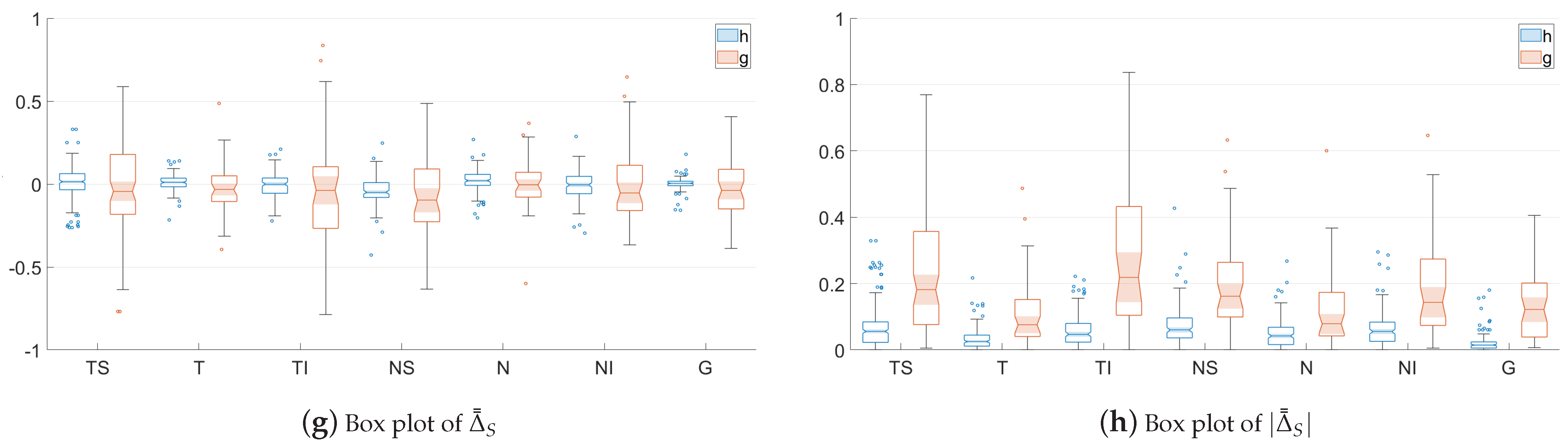
With the aim of easing the understanding of the distribution of the values provides by each asymmetry metric,
Figure 4 shows notched box plots of the proposed RNFL thickness asymmetry metrics for the healthy (
h) and glaucoma (
g) subsets of patients, depicted for each eye sector (TS, T, TI, NS, N and NI) and for the overall global thickness value (G). For each box, the central mark indicates the median, and the bottom and top edges of the box indicate the 25th and 75th percentiles, respectively. These percentiles delimit the so-called interquartile range. The whiskers extend to the most extreme values not considered outliers. Outliers are values located more than 1.5 times the interquartile range outside the upper or lower boundary of the box. The tapered and shaded regions, called notches, display the variability of the median between values. The width of a notch is computed so that boxes whose notches do not overlap have different medians at the 5% significance level—i.e., the true medians do differ with 95% confidence.
As can be seen in
Figure 4, these graphs corroborate the insights concluded above. The values of metrics
,
,
and
are distributed around zero, and there is greater dispersion for the subset of glaucoma patients. The box plots of
,
,
and
depict how the variances of the distributions not using absolute values have been transformed into the corresponding means of the related metrics with absolute values, according to Equation (
11). In addition, it can also be seen qualitatively how the notches with the least overlap for healthy and glaucoma patients are those corresponding to metrics
and
, especially in sectors TS and TI, although the distribution of asymmetry values considering the entire layer, G, has the greater separation. As will be proven numerically later, this fact graphically justifies the use of these metrics as the characteristics for the design of the classifier.
3.2. Decision Trees
Artificial intelligence (AI) is increasingly being incorporated into the diagnostic process in healthcare due to its ability to analyze data with complex artificial networks and to learn automatically, especially through machine learning (ML) and deep learning (DL) [
32,
33]. In this work, instead of using complex classification methods based on machine learning to diagnose glaucoma (see, e.g., [
34,
35,
36]), we chose classification trees [
37] for their simplicity, with the aim of transferring them to daily clinical practice in glaucoma screening.
Classification tree denotes the
classification and regression tree methodology (CART) used to describe decision tree algorithms that are used for classification learning tasks. A decision tree is a supervised machine learning algorithm with a tree-like structure which repeatedly splits the input dataset into classes, taking into account one exploratory variable at a time. These trees are used when the target variable is categorical and can assume only one of two mutually exclusive values (healthy and glaucoma, in our case) [
38,
39].
Considering the RNFL thickness in all sectors (TS, T, TI, NS, N and NI) and the global mean (G) of the peripapillary OCT, the proposed asymmetry metrics have been applied to generate a vector with the features of the subsets of healthy and glaucoma patients. With these features as input variables, a fitted binary classification decision tree has been designed for each asymmetry metric taking into account the labeling of each class (healthy or glaucoma patient).
The designed binary trees split branching nodes based on the values of the input features. One of the parameters of the model is the depth of the tree, which is related to the model complexity, and therefore, to the computational cost. The classification trees have been developed using five folds in the cross-validation. The results of the classification trees have been analyzed controlling the maximum depth of the trees (or maximum number of splits),
. Initially, the weights of the inputs corresponding to the class healthy and to the class glaucoma,
and
, respectively, were set to unity, i.e.,
and
.
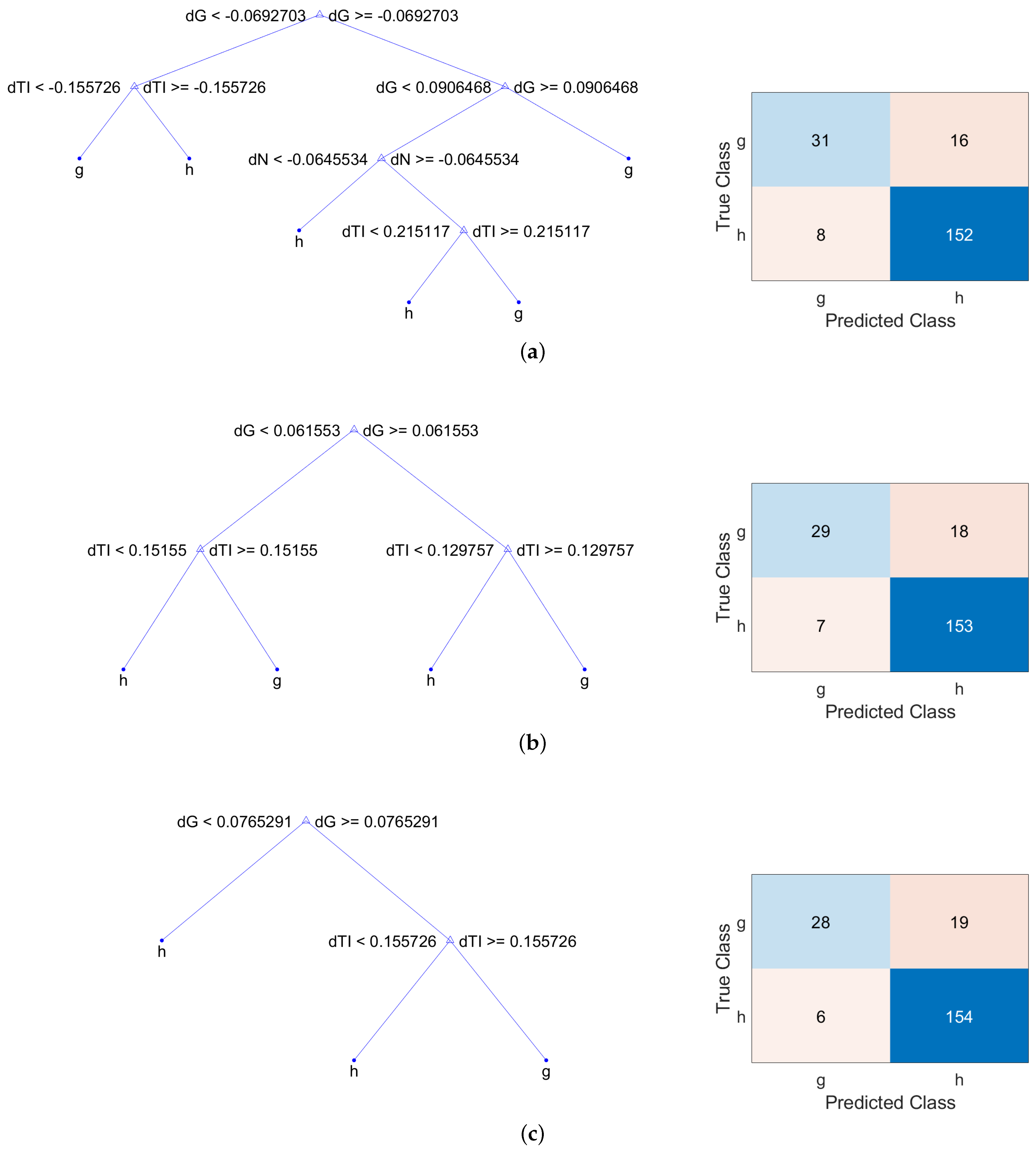
Table 5 gathers the classification loss for observations not used for training in deep decision trees (
) and shallower trees (
). The largest value of
for deep decision trees depends on the number of input features used, which in our case, were the seven asymmetry measurements performed in the six sectors and in the global average of the RNFL thickness. As can be seen, the classification loss decreases as the maximum number of splits is reduced, providing the best values for the metrics
,
and
. The best values have been highlighted in bold in
Table 5, and their corresponding decision trees and confusion matrices are shown in
Figure 5. The representation of each model is a binary tree where each root node represents a single input variable (asymmetry feature) and a split point on that variable. The leaf nodes of the tree contain an output variable which is used to predict if the input corresponds to a healthy or a glaucoma patient. Regarding the confusion matrices, they provide four outcomes:
True positive (): glaucoma patient predicted as glaucoma (top left element),
False positive (): healthy patient predicted as glaucoma (bottom left element),
True negative (): healthy patient predicted as healthy (bottom right element),
False negative (): glaucoma patient predicted as healthy (top right element).
In order to assess the performances of these three trees, the following parameters have been computed from the confusion matrix:
Sensitivity (recall or true positive rate,
):
Specificity (true negative rate,
):
Precision (positive predictive value,
:
As can be seen in
Table 6, these decision trees provide high accuracy (all of them higher than 87%), high specificity (higher than 95%) and high precision (higher than 79%). In order to improve the results, i.e., increase the sensitivity while keeping high values for the remaining parameters, the weight of the inputs corresponding to the class glaucoma has been increased from
to
.
Table 7 contains the classification loss values of the new models considering this weight in the glaucoma input observations.
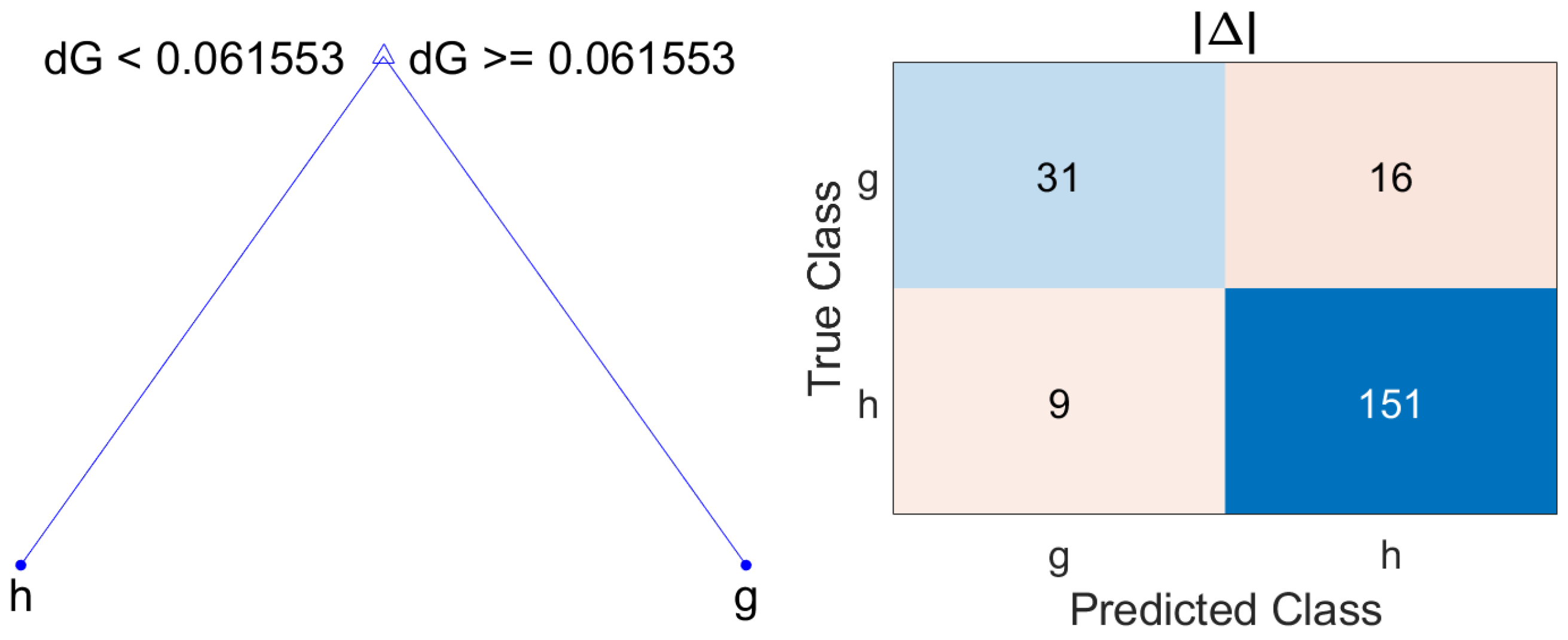
Based on the results of classification loss gathered in
Table 7, the model which offers the best performance with the minimum number of splits is
with
.
Figure 6 shows the resulting model and its corresponding confusion matrix. This classification tree provides the confusion matrix whose parameters are collected in
Table 8.
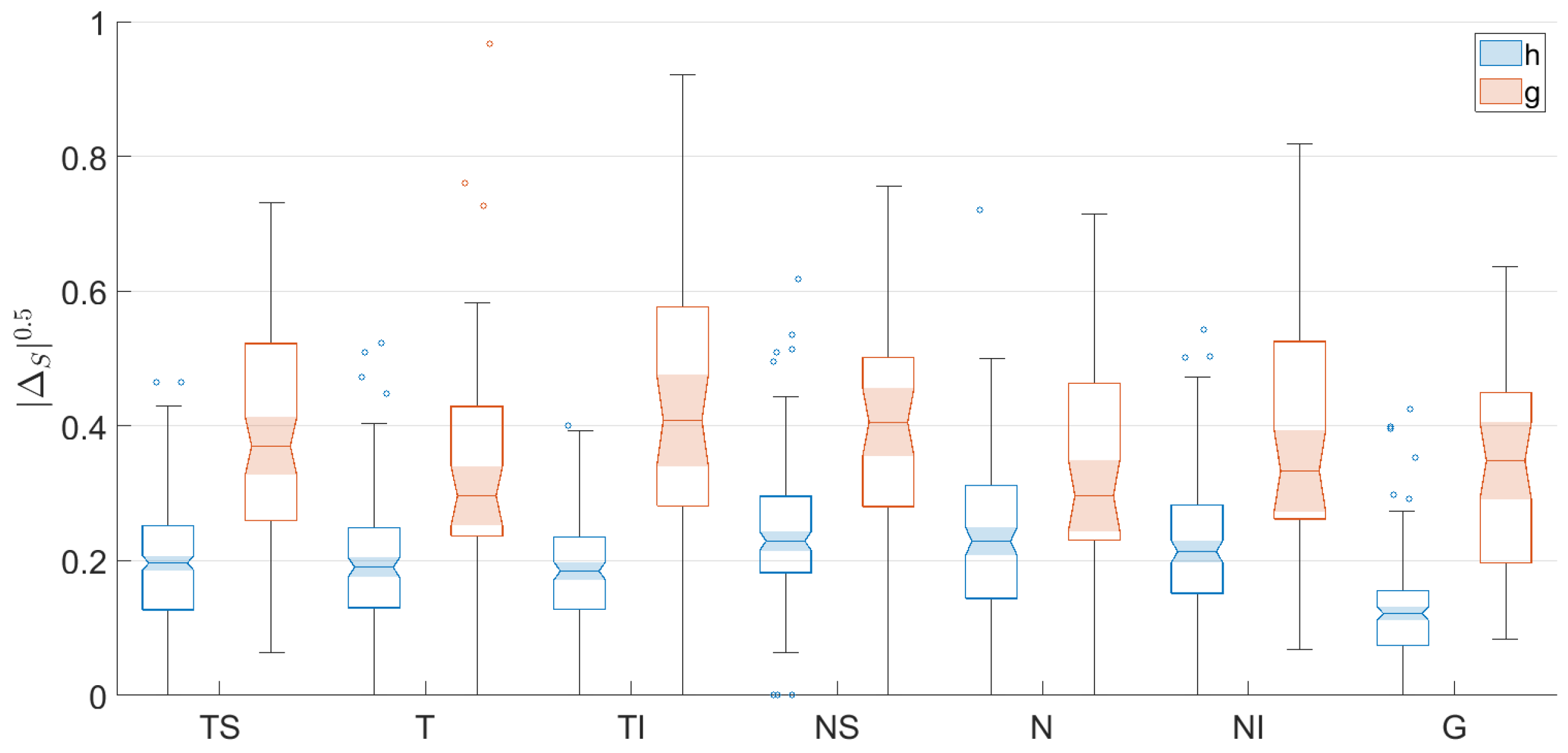
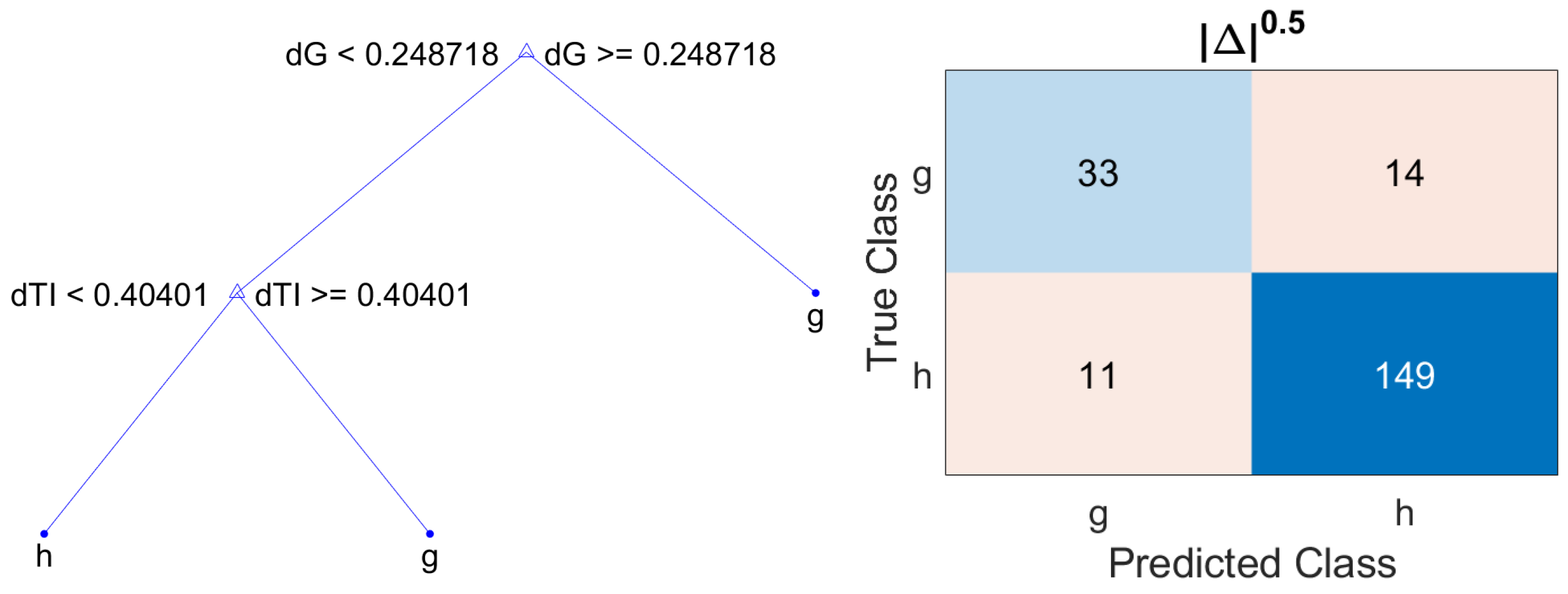
Finally, in order to further increase the number of true glaucoma patients detected, i.e., the sensitivity, and considering that the asymmetry metric
offers the lowest classification loss and taking into account that the asymmetry values range from 0 to 1 (since this measure is normalized by the sum of the RNFL thickness of each eye in the corresponding sector), the asymmetry metric
is proposed. The nonlinear operation of applying the square root to the non-negative real values provided by the metric
decompresses the distribution of the values corresponding to healthy and glaucoma patients. This process of encoding with this decompressive power-law nonlinearity is called gamma compression [
40]. As can be seen in
Table 9, which gathers the statistical parameters of the metric
, the mean values for healthy and glaucoma patients have increased in all sectors. In addition, the distances between the mean values for the subsets of healthy and glaucoma patients have further increased, compared to the values provided by
. This effect can be also observed in
Figure 7, where the notched box plots of each subset are further apart. The resulting decision tree using
and the corresponding confusion matrixes are shown in
Figure 8. The parameters of accuracy, sensitivity, specificity and precision are gathered in
Table 10.


 ,
, 









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}