
IoMT-Based Osteosarcoma Cancer Detection in Histopathology Images Using Transfer Learning Empowered with Blockchain, Fog Computing, and Edge Computing

 , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
2. Literature Review
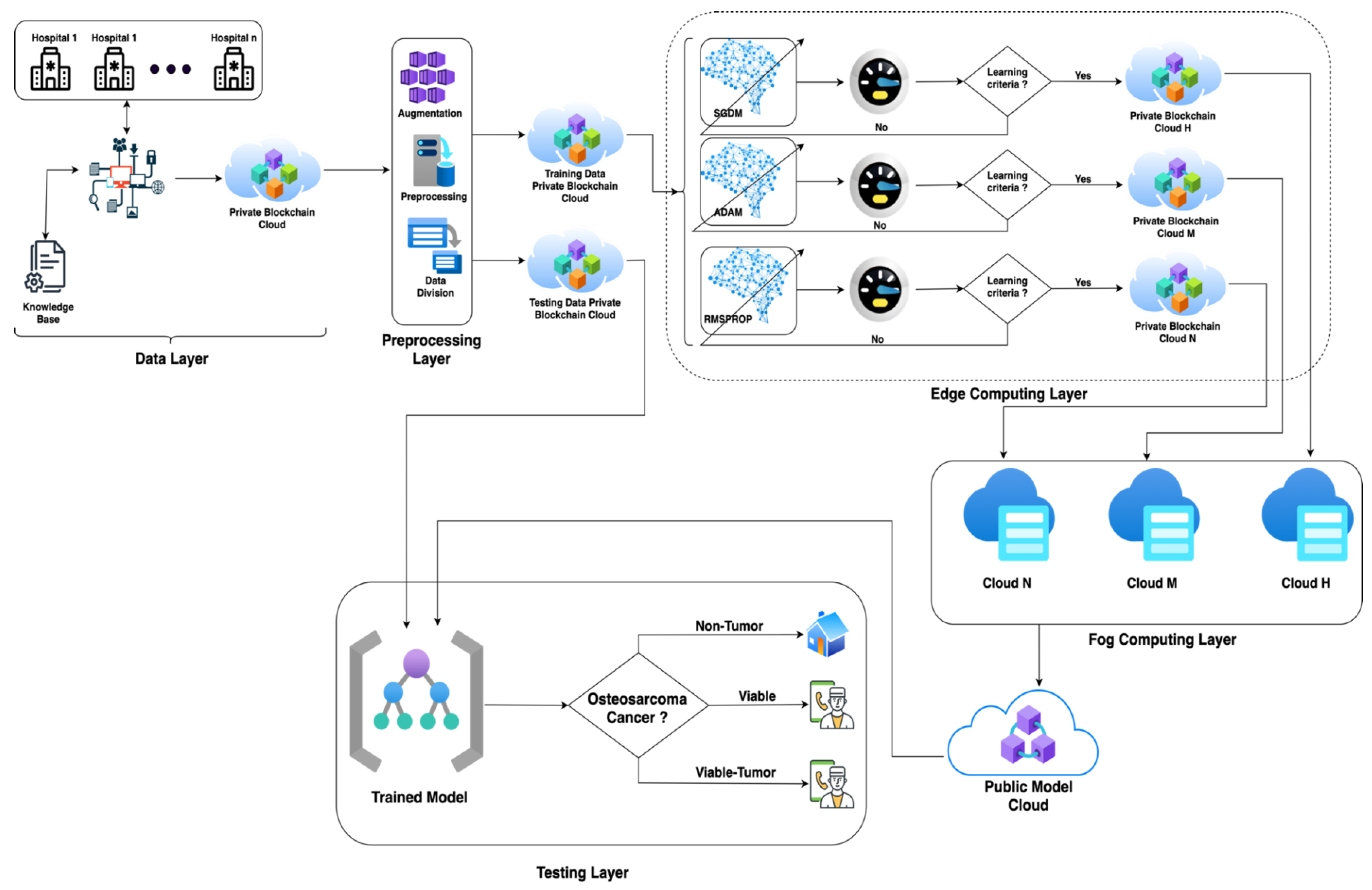
- We employed transfer learning with three different optimizers to minimize the training time and maximize the classification accuracy of the proposed model;
- The Internet of Medical Things (IoMT) has been incorporated into the proposed model for data collection;
- To ensure the security and privacy of the patient data, the proposed model uses blockchain technology;
- The suggested model employs edge computing to process and filter IoMT-generated data closer to the devices, resulting in increased speed and reliability;
- The fog computing layer is employed to further optimize the models and overcome the processing deficiency of the edge devices.
3. Materials and Methods
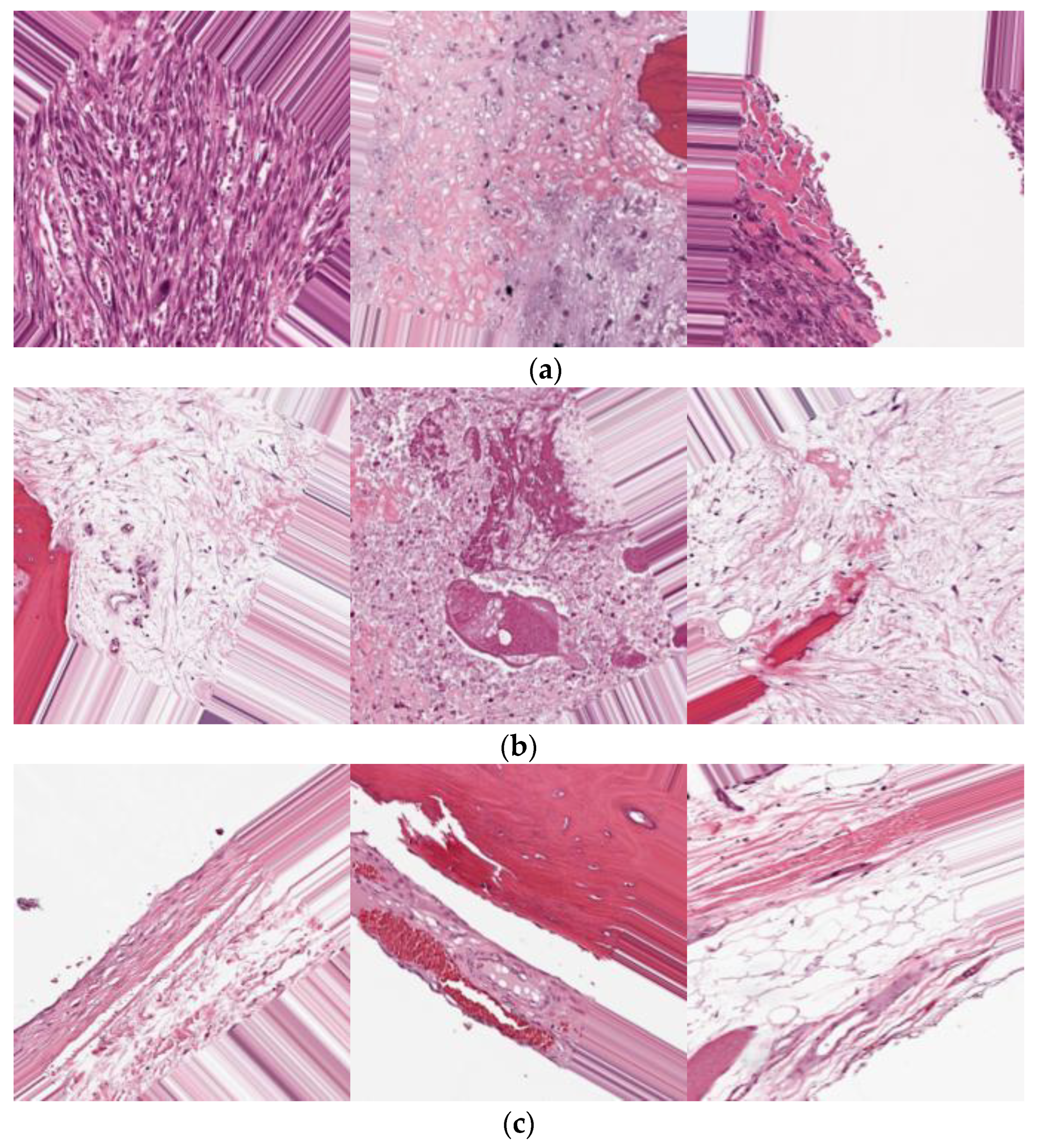
4. Dataset
5. Simulation and Results
6. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Cancer Society. Available online: https://www.cancer.org/cancer/osteosarcoma/about/key-statistics.html#:~:text=Osteosarcoma%20is%20not%20a%20common,ages%20of%2010%20and%2030 (accessed on 25 May 2022).
- Seigel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics 2022. CA A Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef]
- Chen, C.X.; Zhang, D.; Li, N.; Qian, X.J.; Wu, S.J.; Gail, S. Osteosarcoma segmentation in MRI based on Zernike moment and SVM. Chin. J. Biomed. Eng. 2013, 22, 70–78. [Google Scholar]
- Jia, H.; Zhao, X.; Qin, L.; Cai, X. Imaging method for osteosarcoma diagnosis and clinical staging information optimization. J. Med. Imaging Health Inform. 2021, 11, 871–877. [Google Scholar] [CrossRef]
- Baidya Kayal, E.; Kandasamy, D.; Sharma, R.; Bakhshi, S.; Mehndiratta, A. Segmentation of osteosarcoma tumor using diffusion weighted MRI: A comparative study using nine segmentation algorithms. Signal Image Video Process. 2019, 14, 727–735. [Google Scholar] [CrossRef]
- Loraksa, C.; Mongkolsomlit, S.; Nimsuk, N.; Uscharapong, M.; Kiatisevi, P. Effectiveness of Learning Systems from Common Image File Types to Detect Osteosarcoma Based on Convolutional Neural Networks (CNNs) Models. J. Imaging 2022, 8, 2. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Huang, L.; Xia, W.; Zhang, B.; Qiu, B.; Gao, X. Multiple supervised residual network for osteosarcoma segmentation in CT images. Comput. Med. Imaging Graph. 2018, 63, 1–8. [Google Scholar] [CrossRef]
- Goode, A.; Gilbert, B.; Harkes, J.; Jukic, D.; Satyanarayanan, M. OpenSlide: A vendor-neutral software foundation for digital pathology. J. Pathol. Inform. 2013, 4, 27. [Google Scholar] [CrossRef]
- Leavey, P.; Sengupta, A.; Rakheja, D.; Daescu, O.; Arunachalam, H.B.; Mishra, R. Osteosarcoma data from UT Southwestern/UT Dallas for Viable and Necrotic Tumor Assessment. Cancer Imaging Arch. 2019, 14. Available online: https://wiki.cancerimagingarchive.net/pages/viewpage.action?pageId=52756935#527569357c5a8c0c0cef44e488b824bd7de60428 (accessed on 18 July 2022).
- Ding, C.; He, X.; Zha, H.; Simon, H.D. Adaptive dimension reduction for clustering high dimensional data. Proc. Int. Conf. Data Min. 2002, 147–154. [Google Scholar]
- Mehmood, S.; Ghazal, T.M.; Khan, M.A.; Zubair, M.; Naseem, M.T.; Faiz, T.; Ahmad, M. Malignancy Detection in Lung and Colon Histopathology Images Using Transfer Learning with Class Selective Image Processing. IEEE Access 2022, 10, 25657–25668. [Google Scholar] [CrossRef]
- Taleb, N.; Mehmood, S.; Zubair, M.; Naseer, I.; Mago, B.; Nasir, M.U. Ovary Cancer Diagnosing Empowered with Machine Learning. In Proceedings of the 2022 International Conference on Business Analytics for Technology and Security (ICBATS), Dubai, United Arab Emirates, 16 February 2022; pp. 1–6. [Google Scholar]
- Nadeem, M.W.; Goh, H.G.; Khan, M.A.; Hussain, M.; Mushtaq, M.F.; Ponnusamy, V.A. Fusion-based machine learning architecture for heart disease prediction. Comput. Mater. Contin. 2021, 67, 2481–2496. [Google Scholar]
- Siddiqui, S.Y.; Athar, A.; Khan, M.A.; Abbas, S.; Saeed, Y.; Khan, M.F.; Hussain, M. Modelling, simulation, and optimization of diagnosis cardiovascular disease using computational intelligence approaches. J. Med. Imaging Health Inform. 2021, 10, 1005–1022. [Google Scholar] [CrossRef]
- Ahmed, U. Prediction of Diabetes Empowered with Fused Machine Learning. IEEE Access 2022, 10, 8529–8538. [Google Scholar] [CrossRef]
- Nasir, M.U.; Khan, M.A.; Zubair, M.; Ghazal, T.M.; Said, R.A.; Al Hamadi, H. Single and mitochondrial gene inheritance disorder prediction using machine learning. Comput. Mater. Contin. 2022, 73, 954–963. [Google Scholar]
- Rahman, A.U.; Alqahtani, A.; Aldhafferi, N.; Nasir, M.U.; Khan, M.F.; Khan, M.A.; Mosavi, A. Histopathologic Oral Cancer Prediction Using Oral Squamous Cell Carcinoma Biopsy Empowered with Transfer Learning. Sensors 2022, 22, 3833. [Google Scholar] [CrossRef]
- Bakheet, S. An svm framework for malignant melanoma detection based on optimized hog features. Computation 2017, 5, 4. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.Q.; Hussain, A.; Rehman, S.U.; Khan, U.; Maqsood, M.; Mehmood, K.; Khan, M.A. Classification of melanoma and nevus in digital images for diagnosis of skin cancer. IEEE Access 2019, 7, 90132–90144. [Google Scholar] [CrossRef]
- Rahmawaty, M.; Nugroho, H.A.; Triyani, Y.; Ardiyanto, I.; Soesanti, I. Classification of breast ultrasound images based on texture analysis. In Proceedings of the 2016 1st International Conference on Biomedical Engineering (IBIOMED), Yogyakarta, Indonesia, 5–6 October 2016; pp. 1–6. [Google Scholar]
- Solmaz, A.; Tajeripour, F. Detection of brain tumor in 3D MRI images using local binary patterns and histogram orientation gradient. Neurocomputing 2016, 219, 526–535. [Google Scholar]
- Bansal, P.; Kumar, S.; Srivastava, R.; Agarwal, S. Using transfer learning and hierarchical classifier to diagnose melanoma from dermoscopic images. Int. J. Healthc. Inf. Syst. Inform. (IJHISI) 2021, 16, 73–86. [Google Scholar] [CrossRef]
- Bisla, D.; Choromanska, A.; Berman, R.S.; Stein, J.A.; Polsky, D. Towards automated melanoma detection with deep learning: Data purification and augmentation. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition Workshops, Long Beach, CA, USA, 16–17 June 2019; pp. 2720–2728. [Google Scholar]
- Cao, Z.; Duan, L.; Yang, G. An experimental study on breast lesion detection and classification from ultrasound images using deep learning architectures. BMC Med. Imaging 2019, 19, 51. [Google Scholar] [CrossRef]
- Li, Y.; Deng, L.; Yang, X. Early diagnosis of gastric cancer based on deep learning combined with the spectral-spatial classification method. Biomed. Opt. Express 2019, 10, 4999–5014. [Google Scholar] [CrossRef] [PubMed]
- Srinivasu, P.N.; SivaSai, J.G.; Ijaz, M.F.; Bhoi, A.K.; Kim, W.; Kang, J.J. Classification of skin disease using deep learning neural networks with MobileNet V2 and LSTM. Sensors 2021, 21, 2852. [Google Scholar] [CrossRef] [PubMed]
- Almaraz-Damian, J.-A.; Ponomaryov, V.; Sadovnychiy, S.; Castillejos-Fernandez, H. Melanoma and nevus skin lesion classification using handcraft and deep learning feature fusion via mutual information measures. Entropy 2020, 22, 484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasan, A.M.; Jalab, H.A.; Meziane, F.; Kahtan, H.; Al-Ahmad, A.S. Combining deep and handcrafted image features for MRI brain scan classification. IEEE Access 2019, 7, 79959–79967. [Google Scholar] [CrossRef]
- Abdel-Basset, M.; El-Shahat, D.; El-henawy, I.; de Albuquerque, V.H.C.; Mirjalili, S. A new fusion of grey wolf optimizer algorithm with a two-phase mutation for feature selection. Expert Syst. Appl. 2020, 139, 112824. [Google Scholar] [CrossRef]
- Al-Tashi, Q.; Abdulkadir, S.J.; Rais, H.M.; Mirjalili, S.; Alhussian, H.; Ragab, M.G.; Alqushaibi, A. Binary multi-objective grey wolf optimizer for feature selection in classification. IEEE Access 2020, 8, 106247–106263. [Google Scholar] [CrossRef]
- Bansal, P.; Kumar, S.; Pasrija, S.; Kumar, S. A hybrid grasshopper and new cat swarm optimization algorithm for feature selection and optimization of multi-layer perceptron. Soft Comput. 2020, 24, 15463–15489. [Google Scholar] [CrossRef]
- Elgamal, Z.M.; Yasin, N.B.M.; Tubishat, M.; Alswaitti, M.; Mirjalili, S. An improved harris hawks optimization algorithm with simulated annealing for feature selection in the medical field. IEEE Access 2020, 8, 186638–186652. [Google Scholar] [CrossRef]
- El-Kenawy, E.M.; Eid, M.M.; Saber, M.; Ibrahim, A. MbGWO-SFS: Modified binary grey wolf optimizer based on stochastic fractal search for feature selection. IEEE Access 2020, 8, 107635–107649. [Google Scholar] [CrossRef]
- El-Kenawy, E.M.; Ibrahim, A.; Mirjalili, S.; Eid, M.M.; Hussein, S.E. Novel feature selection and voting classifier algorithms for COVID-19 classification in CT images. IEEE Access 2020, 8, 179317–179335. [Google Scholar] [CrossRef]
- Nasor, M.; Obaid, W. Segmentation of osteosarcoma in MRI images by K-means clustering, Chan-Vese segmentation, and iterative Gaussian filtering. IET Image Process. 2021, 15, 1310–1318. [Google Scholar] [CrossRef]
- Vandana, B.S.; Antony, P.J.; Alva, S.R. Analysis of malignancy using enhanced graphcut-based clustering for diagnosis of bone cancer. In Information and Communication Technology for Sustainable Development; Springer: Berlin/Heidelberg, Germany, 2020; pp. 453–462. [Google Scholar]
- Altameem, T. Fuzzy rank correlation-based segmentation method and deep neural network for bone cancer identification. Neural Comput. Appl. 2020, 32, 805–815. [Google Scholar] [CrossRef]
- Mishra, R.; Daescu, O.; Leavey, P.; Rakheja, D.; Sengupta, A. Histopathological diagnosis for viable and non-viable tumor prediction for osteosarcoma using convolutional neural network. In Proceedings of the 13th International Symposium on Bioinformatics Research and Applications (ISBRA), Honolulu, HI, USA, 30 May–2 June 2017; Springer: Cham, Switzerland, 2017. [Google Scholar]
- Arunachalam, H.B.; Mishra, R.; Armaselu, B.; Daescu, O.; Martinez, M.; Leavey, P.; Rakheja, D.; Cederberg, K.; Sengupta, A.; Ni’Suilleabhain, M. Computer aided image segmentation and classification for viable and non-viable tumor identification in osteosarcoma. In Proceedings of the Pacific Symposium on Biocomputing, Kohala Coast, HI, USA, 3–7 January 2017; pp. 195–206. [Google Scholar]
- Mishra, R.; Daescu, O.; Leavey, P.; Rakheja, D.; Sengupta, A. Convolutional neural network for histopathological analysis of osteosarcoma. J. Comput. Biol. 2018, 25, 313–325. [Google Scholar] [CrossRef] [PubMed]
- D’Acunto, M.; Martinelli, M.; Morono, D. From human mesenchymal stromal cells to osteosarcoma cells classification by deep learning. J. Intell. Fuzzy Syst. 2020, 37, 7199–7206. [Google Scholar] [CrossRef] [Green Version]
- Anisuzzaman, D.M.; Barzekar, H.; Tong, L.; Luo, J.; Yu, Z. A deep learning study on osteosarcoma detection from histological images. arXiv 2020, arXiv:2011.01177. [Google Scholar] [CrossRef]
- Arunachalam, H.B.; Mishra, R.; Daescu, O.; Cederberg, K.; Rakheja, D.; Sengupta, A.; Leonard, D.; Hallac, R.; Leavey, P. Viable and necrotic tumor assessment from whole slide images of osteosarcoma using machine-learning and deep-learning models. PLoS ONE 2019, 14, 0210706. [Google Scholar] [CrossRef]
- Pan, L.; Wang, H.; Wang, L.; Ji, B.; Liu, M.; Chongcheawchamnan, M.; Yuan, J.; Peng, S. Noise-reducing attention cross fusion learning transformer for histological image classification of osteosarcoma. Biomed. Signal. Process. Control. 2022, 77, 103824. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Steps | Code |
|---|---|
| 1 | Data source (hospital1, hospital2, hospital3, ………, hospital) (knowledge base) |
| 2 | IoMT (data source) |
| 3 | Private cloud blockchain secured (data) |
| 4 | Data pre-processing (augmentation, contrast correction, data division) |
| 5 | Store pre-processed train data→private cloud (blockchain secured) |
| 6 | Store pre-processed test data→private cloud (blockchain secured) |
| 7 | Edge computing layer Transfer learning
Cloud N← Cloud M← Cloud H← Public model cloud (trained model)← |
| 8 | Import test data→private cloud Import trained model→public model cloud |
| 9 | Apply testing (predict osteosarcoma cancer) |
| 10 | Apply statistical matrix (model performance) |
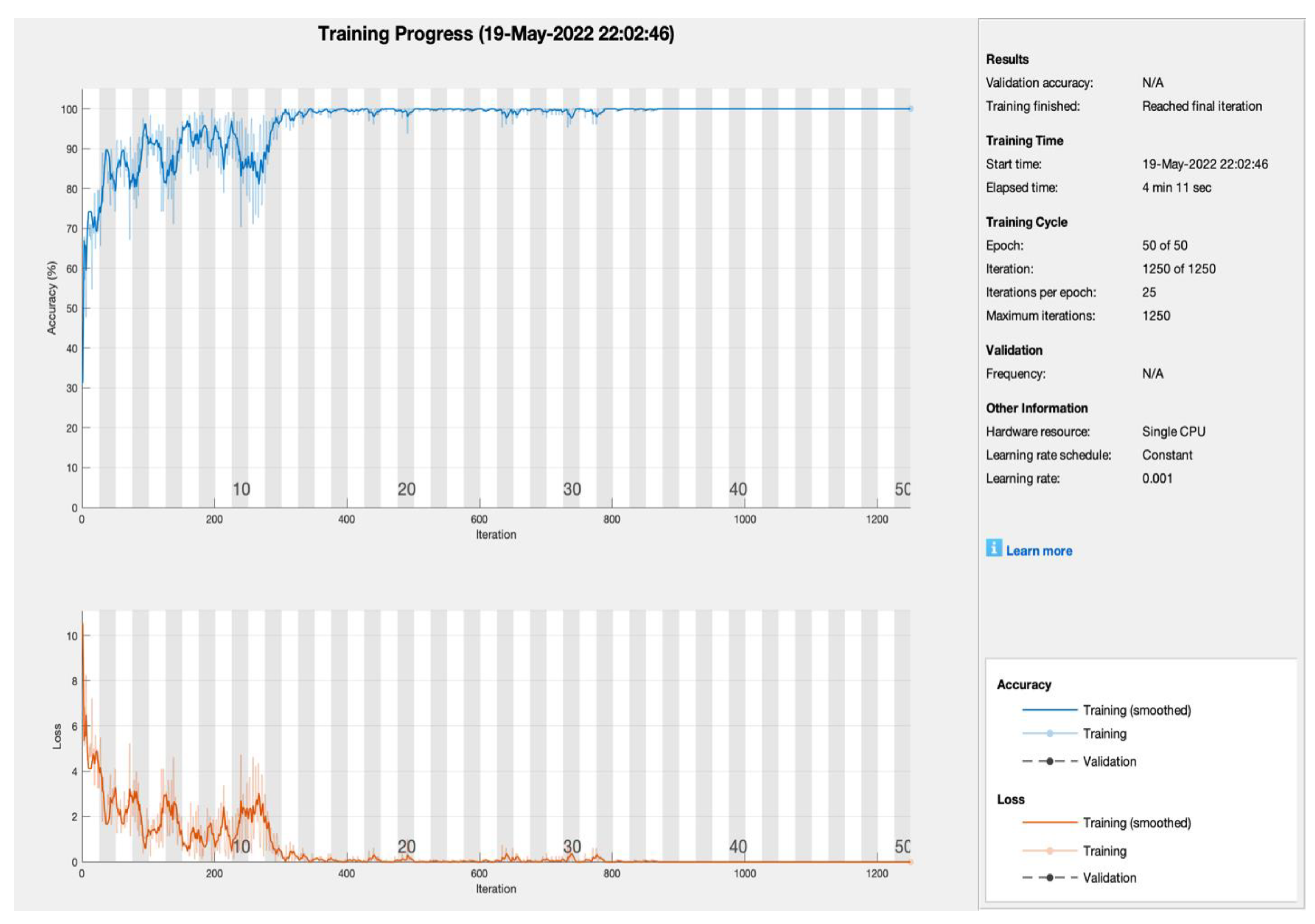
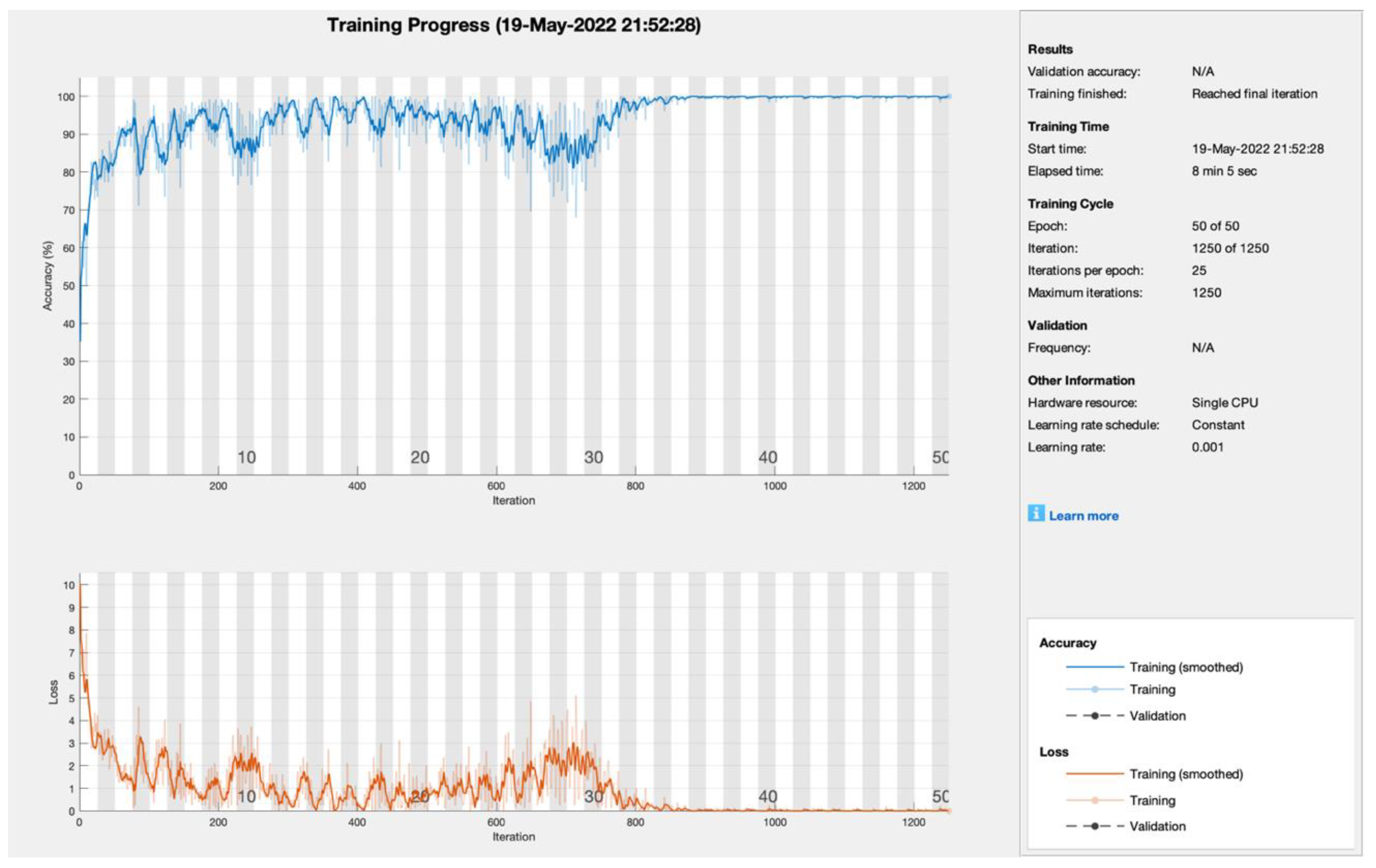
| AlexNet | |||||
|---|---|---|---|---|---|
| Model | Iterations | Learning Rate | Epoch | PA (%) | CMR (%) |
| SGDM | 1250 | 0.001 | 50 | 99.8 | 0.2 |
| ADAM | 99.5 | 0.5 | |||
| RMSProp | 99.5 | 0.5 | |||
| SGDM | 750 | 0.001 | 30 | 98.88 | 1.12 |
| ADAM | 98.01 | 1.99 | |||
| RMSProp | 97.99 | 2.01 | |||
| SGDM | 500 | 0.001 | 20 | 92.8 | 7.2 |
| ADAM | 91.5 | 8.5 | |||
| RMSProp | 90.06 | 9.94 | |||
| Total Samples (990) | Non-Tumor | Viable Tumor | Viable |
|---|---|---|---|
| Non-Tumor | 328 | 0 | 3 |
| Viable Tumor | 0 | 330 | 5 |
| Viable | 2 | 0 | 322 |
| Total Samples (990) | Non-Tumor | Viable Tumor | Viable |
|---|---|---|---|
| Non-Tumor | 330 | 0 | 3 |
| Viable Tumor | 0 | 330 | 4 |
| Viable | 0 | 0 | 323 |
| Total Samples (990) | Non-Tumor | Viable Tumor | Viable |
|---|---|---|---|
| Non-Tumor | 330 | 0 | 3 |
| Viable Tumor | 0 | 329 | 2 |
| Viable | 0 | 1 | 325 |
| Solver Name | Statistical Parameters | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PA | CMR | Sen | Spec | F1 | PPV | NPV | FPR | FNR | LPR | LNR | FMI | |
| SGDM | 99.30 | 0.70 | 98.80 | 99.55 | 98.95 | 99.10 | 99.40 | 0.45 | 1.20 | 218.02 | 0.01 | 98.95 |
| ADAM | 99.09 | 0.91 | 98.20 | 99.55 | 98.65 | 99.09 | 99.10 | 0.45 | 1.80 | 216.05 | 0.02 | 98.65 |
| RMSPROP | 99.30 | 0.70 | 98.80 | 99.55 | 98.95 | 99.10 | 99.39 | 0.45 | 1.20 | 217.37 | 0.01 | 98.95 |
| Article Authors | Year | Model/Classifier | Blockchain | IoMT | Fog/Edge Computing | Accuracy (%) |
|---|---|---|---|---|---|---|
| Mishra, Rashika et al. [38] | 2017 | CNN | No | No | No | 84 |
| Arunachalam, Harish Babu et al. [39] | 2017 | K-means, flood-fill algorithm | No | No | No | 95.5 |
| Mishra et al. [40] | 2018 | AlexNet, LeNet, and VGGNet | No | No | No | 92 |
| Anisuzzaman et al. [42] | 2021 | VGG19 | No | No | No | 96 |
| Arunachalam, Harish Babu et al. [43] | 2019 | Complex trees (CT) Support vector Machine (SVM) Ensemble learners (ENS) | No | No | No | 89.9 |
| Liangrui Pan et.al. [44] | 2022 | NRCA-FCFL | No | No | No | 99.17 |
| Proposed Model | 2022 | AlexNet with SGDM, ADAM, RMSprop. Blockchain, edge, and fog computing | Yes | Yes | Yes | 99.30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nasir, M.U.; Khan, S.; Mehmood, S.; Khan, M.A.; Rahman, A.-u.; Hwang, S.O. IoMT-Based Osteosarcoma Cancer Detection in Histopathology Images Using Transfer Learning Empowered with Blockchain, Fog Computing, and Edge Computing. Sensors 2022, 22, 5444. https://0-doi-org.brum.beds.ac.uk/10.3390/s22145444
Nasir MU, Khan S, Mehmood S, Khan MA, Rahman A-u, Hwang SO. IoMT-Based Osteosarcoma Cancer Detection in Histopathology Images Using Transfer Learning Empowered with Blockchain, Fog Computing, and Edge Computing. Sensors. 2022; 22(14):5444. https://0-doi-org.brum.beds.ac.uk/10.3390/s22145444
Chicago/Turabian StyleNasir, Muhammad Umar, Safiullah Khan, Shahid Mehmood, Muhammad Adnan Khan, Atta-ur Rahman, and Seong Oun Hwang. 2022. "IoMT-Based Osteosarcoma Cancer Detection in Histopathology Images Using Transfer Learning Empowered with Blockchain, Fog Computing, and Edge Computing" Sensors 22, no. 14: 5444. https://0-doi-org.brum.beds.ac.uk/10.3390/s22145444