
The Applicability of Shear Wave Elastography to Assess Myotendinous Stiffness of Lower Limbs during an Incremental Isometric Strength Test
 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Procedure
2.2. Isometric Muscle Contraction Work
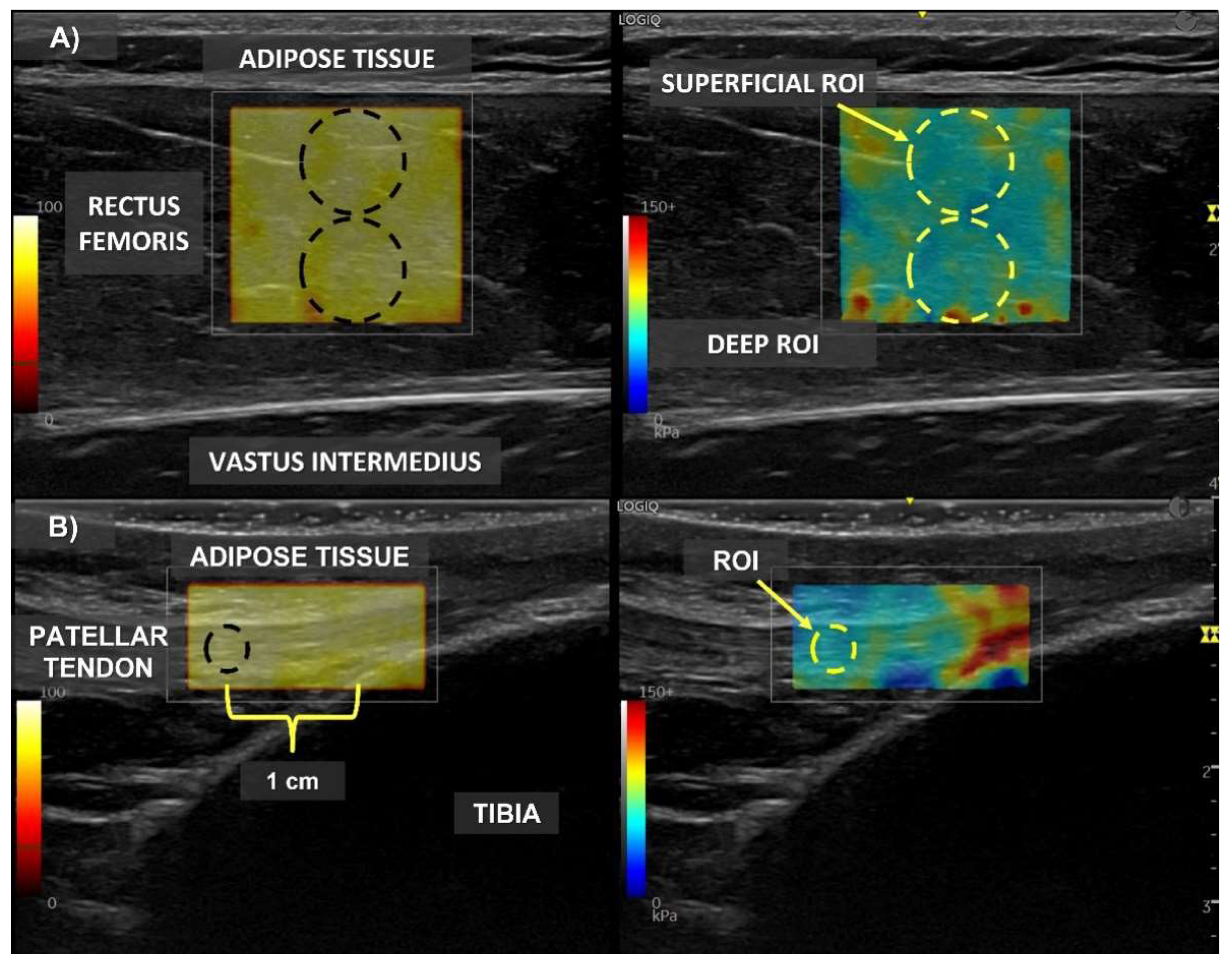
2.3. Shear Wave Elastography Assessment
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gavronski, G.; Veraksitš, A.; Vasar, E.; Maaroos, J. Evaluation of viscoelastic parameters of the skeletal muscles in junior triathletes. Physiol. Meas. 2007, 28, 625–637. [Google Scholar] [CrossRef] [PubMed]
- Granata, K.P.; Padua, D.A.; Wilson, S.E. Gender differences in active musculoskeletal stiffness. Part II. Quantification of leg stiffness during functional hopping tasks. J. Electromyogr. Kinesiol. 2002, 12, 127–135. [Google Scholar] [CrossRef]
- Wojtys, E.M.; Huston, L.J.; Schock, H.J.; Boylan, J.P.; Ashton-Miller, J.A. Gender differences in muscular protection of the knee in torsion in size-matched athletes. J. Bone Jt. Surg. Am. 2003, 85, 782–789. [Google Scholar] [CrossRef] [PubMed]
- Padua, D.A.; Carcia, C.R.; Arnold, B.L.; Granata, K.P. Gender differences in leg stiffness and stiffness recruitment strategy during two-legged hopping. J. Mot. Behav. 2005, 37, 111–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pruyn, E.C.; Watsford, M.L.; Murphy, A.J. Validity and reliability of three methods of stiffness assessment. J. Sport Health Sci. 2016, 5, 476–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siracusa, J.; Charlot, K.; Malgoyre, A.; Conort, S.; Tardo-Dino, P.E.; Bourrilhon, C.; Garcia-Vicencio, S. Resting Muscle Shear Modulus Measured With Ultrasound Shear-Wave Elastography as an Alternative Tool to Assess Muscle Fatigue in Humans. Front. Physiol. 2019, 10, 626. [Google Scholar] [CrossRef]
- Andonian, P.; Viallon, M.; Goff, C.L.; de Bourguignon, C.; Tourel, C.; Morel, J.; Giardini, G.; Gergele, L.; Millet, G.P.; Croisille, P. Correction: Shear-Wave Elastography Assessments of Quadriceps Stiffness Changes prior to, during and after Prolonged Exercise: A Longitudinal Study during an Extreme Mountain Ultra-Marathon. PLoS ONE 2016, 11, e0167668. [Google Scholar] [CrossRef]
- Bravo-Sanchez, A.; Abian, P.; Jimenez, F.; Abian-Vicen, J. Structural and mechanical properties of the Achilles tendon in senior badminton players: Operated vs. non-injured tendons. Clin. Biomech. 2021, 85, 105366. [Google Scholar] [CrossRef]
- Ramirez-delaCruz, M.; Bravo-Sanchez, A.; Esteban-Garcia, P.; Jimenez, F.; Abian-Vicen, J. Effects of Plyometric Training on Lower Body Muscle Architecture, Tendon Structure, Stiffness and Physical Performance: A Systematic Review and Meta-analysis. Sports Med. Open 2022, 8, 40. [Google Scholar] [CrossRef] [PubMed]
- Bravo-Sanchez, A.; Abian, P.; Sousa, F.; Jimenez, F.; Abian-Vicen, J. Influence of Badminton Practice on Age-Related Changes in Patellar and Achilles Tendons. J. Aging Phys. Act. 2021, 29, 382–390. [Google Scholar] [CrossRef]
- Davis, J.J.T.; Gruber, A.H. Leg Stiffness, Joint Stiffness, and Running-Related Injury: Evidence From a Prospective Cohort Study. Orthop. J. Sports Med. 2021, 9, 23259671211011213. [Google Scholar] [CrossRef] [PubMed]
- Couppe, C.; Kongsgaard, M.; Aagaard, P.; Vinther, A.; Boesen, M.; Kjaer, M.; Magnusson, S.P. Differences in tendon properties in elite badminton players with or without patellar tendinopathy. Scand. J. Med. Sci. Sports 2013, 23, e89–e95. [Google Scholar] [CrossRef] [PubMed]
- Seynnes, O.R.; Erskine, R.M.; Maganaris, C.N.; Longo, S.; Simoneau, E.M.; Grosset, J.F.; Narici, M.V. Training-induced changes in structural and mechanical properties of the patellar tendon are related to muscle hypertrophy but not to strength gains. J. Appl. Physiol. (1985) 2009, 107, 523–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, P.; Bojsen-Moller, J.; Aagaard, P.; Kjaer, M.; Magnusson, S.P. Mechanical properties of the human patellar tendon, in vivo. Clin. Biomech. 2006, 21, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Prado-Costa, R.; Rebelo, J.; Monteiro-Barroso, J.; Preto, A.S. Ultrasound elastography: Compression elastography and shear-wave elastography in the assessment of tendon injury. Insights Imaging 2018, 9, 791–814. [Google Scholar] [CrossRef]
- Park, G.Y.; Kwon, D.R. Application of real-time sonoelastography in musculoskeletal diseases related to physical medicine and rehabilitation. Am. J. Phys. Med. Rehabil. 2011, 90, 875–886. [Google Scholar] [CrossRef]
- Alfuraih, A.M.; Tan, A.L.; O’Connor, P.; Emery, P.; Wakefield, R.J. The effect of ageing on shear wave elastography muscle stiffness in adults. Aging Clin. Exp. Res. 2019, 31, 1755–1763. [Google Scholar] [CrossRef] [Green Version]
- Sendur, H.N.; Cindil, E.; Cerit, M.N.; Kilic, P.; Gultekin, I.I.; Oktar, S.O. Evaluation of effects of aging on skeletal muscle elasticity using shear wave elastography. Eur. J. Radiol. 2020, 128, 109038. [Google Scholar] [CrossRef]
- Pang, J.; Wu, M.; Liu, X.; Gao, K.; Liu, Y.; Zhang, Y.; Zhang, E.; Zhang, T. Age-Related Changes in Shear Wave Elastography Parameters of the Gastrocnemius Muscle in Association with Physical Performance in Healthy Adults. Gerontology 2021, 67, 306–313. [Google Scholar] [CrossRef]
- Romano, A.; Staber, D.; Grimm, A.; Kronlage, C.; Marquetand, J. Limitations of Muscle Ultrasound Shear Wave Elastography for Clinical Routine-Positioning and Muscle Selection. Sensors 2021, 21, 8490. [Google Scholar] [CrossRef]
- Bravo-Sanchez, A.; Abian, P.; Sanchez-Infante, J.; Esteban-Gacia, P.; Jimenez, F.; Abian-Vicen, J. Objective Assessment of Regional Stiffness in Vastus Lateralis with Different Measurement Methods: A Reliability Study. Sensors 2021, 21, 3213. [Google Scholar] [CrossRef] [PubMed]
- Shinohara, M.; Sabra, K.; Gennisson, J.L.; Fink, M.; Tanter, M. Real-time visualization of muscle stiffness distribution with ultrasound shear wave imaging during muscle contraction. Muscle Nerv. 2010, 42, 438–441. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, S.; Shan, X.; Kawakami, Y. Dependence of muscle and deep fascia stiffness on the contraction levels of the quadriceps: An in vivo supersonic shear-imaging study. J. Electromyogr. Kinesiol. 2019, 45, 33–40. [Google Scholar] [CrossRef]
- Soldos, P.; Besenyi, Z.; Hideghety, K.; Pavics, L.; Hegedus, A.; Racz, L.; Kopper, B. Comparison of Shear Wave Elastography and Dynamometer Test in Muscle Tissue Characterization for Potential Medical and Sport Application. Pathol. Oncol. Res. 2021, 27, 1609798. [Google Scholar] [CrossRef] [PubMed]
- Koo, T.K.; Guo, J.Y.; Cohen, J.H.; Parker, K.J. Quantifying the passive stretching response of human tibialis anterior muscle using shear wave elastography. Clin. Biomech. 2014, 29, 33–39. [Google Scholar] [CrossRef]
- Corrigan, P.; Zellers, J.A.; Balascio, P.; Silbernagel, K.G.; Cortes, D.H. Quantification of Mechanical Properties in Healthy Achilles Tendon Using Continuous Shear Wave Elastography: A Reliability and Validation Study. Ultrasound Med. Biol. 2019, 45, 1574–1585. [Google Scholar] [CrossRef]
- Rouissi, M.; Chtara, M.; Owen, A.; Chaalali, A.; Chaouachi, A.; Gabbett, T.; Chamari, K. Effect of leg dominance on change of direction ability amongst young elite soccer players. J. Sports Sci. 2016, 34, 542–548. [Google Scholar] [CrossRef]
- Bolsterlee, B.; Gandevia, S.C.; Herbert, R.D. Effect of Transducer Orientation on Errors in Ultrasound Image-Based Measurements of Human Medial Gastrocnemius Muscle Fascicle Length and Pennation. PLoS ONE 2016, 11, e0157273. [Google Scholar] [CrossRef] [Green Version]
- Taljanovic, M.S.; Gimber, L.H.; Becker, G.W.; Latt, L.D.; Klauser, A.S.; Melville, D.M.; Gao, L.; Witte, R.S. Shear-Wave Elastography: Basic Physics and Musculoskeletal Applications. Radiographics 2017, 37, 855–870. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.Z.; Guo, J.Y.; Li, T.J.; Zhou, Y.; Shi, W.; Zheng, Y.P. Age and Sex Effects on the Active Stiffness of Vastus Intermedius under Isometric Contraction. Biomed. Res. Int. 2017, 2017, 9469548. [Google Scholar] [CrossRef]
- Alfuraih, A.M.; O’Connor, P.; Hensor, E.; Tan, A.L.; Emery, P.; Wakefield, R.J. The effect of unit, depth, and probe load on the reliability of muscle shear wave elastography: Variables affecting reliability of SWE. J. Clin. Ultrasound 2018, 46, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Yu, H.K.; Sheng, S.Y.; Liang, S.M.; Lu, H.; Chen, R.Y.; Pan, M.; Wen, Z.B. Quantitative evaluation of passive muscle stiffness by shear wave elastography in healthy individuals of different ages. Eur. Radiol. 2021, 31, 3187–3194. [Google Scholar] [CrossRef] [PubMed]

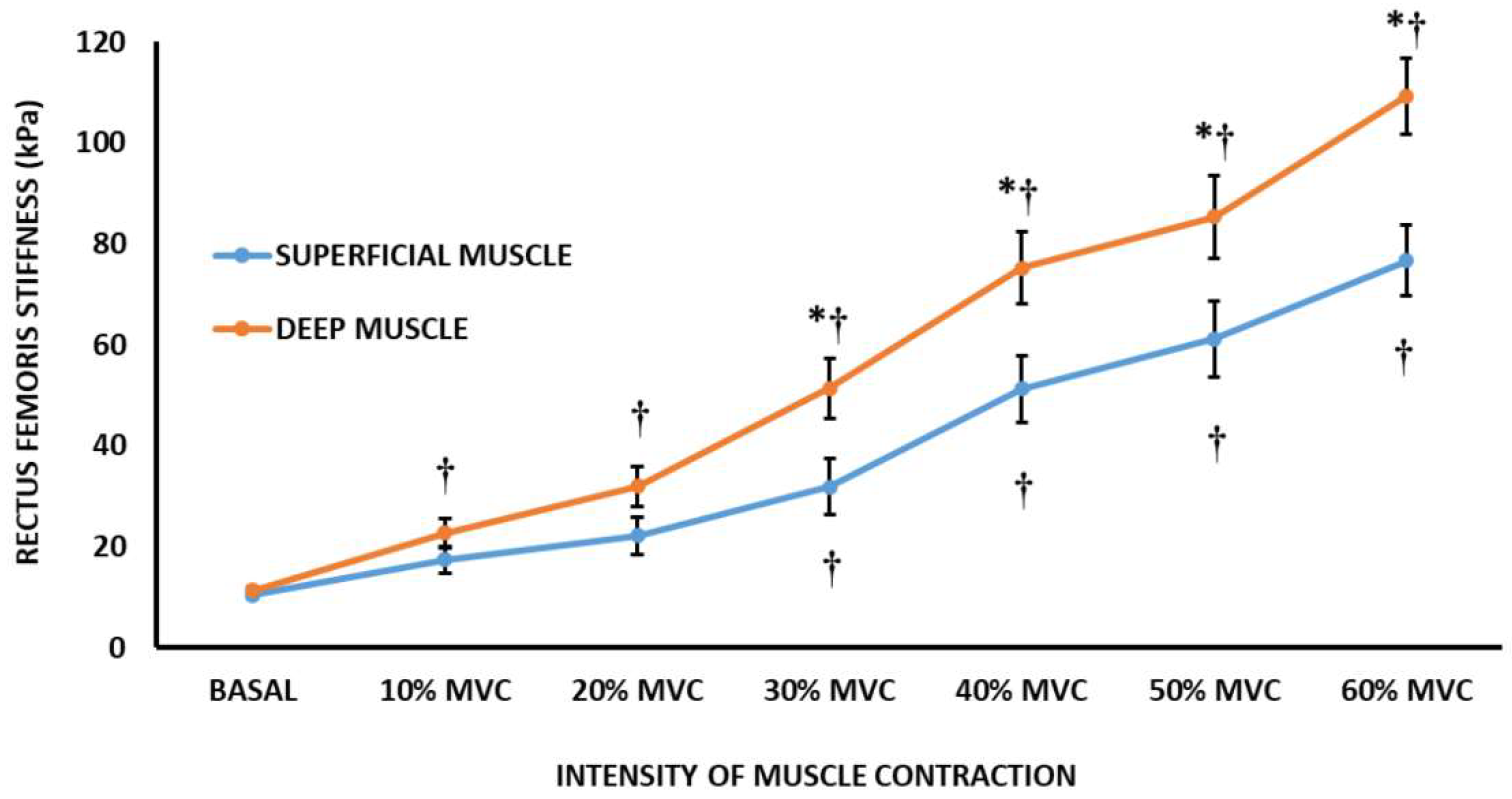
 Differences to basal condition. ﹡ Differences between superficial muscle region and deep muscle region; p < 0.05.
Differences to basal condition. ﹡ Differences between superficial muscle region and deep muscle region; p < 0.05.
Differences to basal condition. ﹡ Differences between superficial muscle region and deep muscle region; p < 0.05.
Differences to basal condition. ﹡ Differences between superficial muscle region and deep muscle region; p < 0.05.

{kind=link}
{kind=link}
| Title 1 | Young Modulus (kPa) | Speed of Sound (m/s) | Success Percentage (%) |
|---|---|---|---|
| Rectus femoris superficial region | |||
| Basal condition | 10.47 ± 2.74 | 1.91 ± 0.30 | 100 |
| 10% MVC | 17.41 ± 8.40 | 2.50 ± 0.76 | 100 |
| 20% MVC | 22.17 ± 10.83 | 2.78 ± 0.78 | 100 |
| 30% MVC | 31.83 ± 17.05 | 3.27 ± 1.04 | 100 |
| 40% MVC | 51.25 ± 28.90 | 4.11 ± 1.18 | 95 |
| 50% MVC | 61.16 ± 37.03 | 4.59 ± 1.35 | 95 |
| 60% MVC | 76.67 ± 36.07 | 5.09 ± 1.22 | 85 |
| Rectus femoris deep region | |||
| Basal condition | 11.33 ± 4.60 | 1.93 ± 0.34 | 100 |
| 10% MVC | 22.70 ± 18.43 | 2.65 ± 0.95 | 100 |
| 20% MVC | 31.94 ± 26.37 | 3.11 ± 1.13 | 100 |
| 30% MVC | 51.46 ± 38.17 * | 3.95 ± 1.42 * | 100 |
| 40% MVC | 75.21 ± 42.27 * | 4.83 ± 1.38 * | 95 |
| 50% MVC | 85.34 ± 45.05 * | 5.17 ± 1.39 | 95 |
| 60% MVC | 109.29 ± 40.04 * | 5.84 ± 1.25 * | 85 |
| Patellar tendon | |||
| Basal condition | 82.37 ± 27.97 | 5.41 ± 1.56 | 100 |
| 10% MVC | 186.24 ± 36.87 | 6.28 ± 1.83 | 70 |
| 20% MVC | - | - | 40 |
| 30% MVC | - | - | 30 |
| 40% MVC | - | - | 30 |
| 50% MVC | - | - | 10 |
| 60% MVC | - | - | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bravo-Sánchez, A.; Abián, P.; Lucenteforte, G.; Jiménez, F.; Abián-Vicén, J. The Applicability of Shear Wave Elastography to Assess Myotendinous Stiffness of Lower Limbs during an Incremental Isometric Strength Test. Sensors 2022, 22, 8033. https://0-doi-org.brum.beds.ac.uk/10.3390/s22208033
Bravo-Sánchez A, Abián P, Lucenteforte G, Jiménez F, Abián-Vicén J. The Applicability of Shear Wave Elastography to Assess Myotendinous Stiffness of Lower Limbs during an Incremental Isometric Strength Test. Sensors. 2022; 22(20):8033. https://0-doi-org.brum.beds.ac.uk/10.3390/s22208033
Chicago/Turabian StyleBravo-Sánchez, Alfredo, Pablo Abián, Giacomo Lucenteforte, Fernando Jiménez, and Javier Abián-Vicén. 2022. "The Applicability of Shear Wave Elastography to Assess Myotendinous Stiffness of Lower Limbs during an Incremental Isometric Strength Test" Sensors 22, no. 20: 8033. https://0-doi-org.brum.beds.ac.uk/10.3390/s22208033