
Capacity Strengthening Undertaking—Farm Organized Response of Workers against Risk for Diabetes: (C.S.U.—F.O.R.W.A.R.D. with Cal Poly)—A Concept Approach to Tackling Diabetes in Vulnerable and Underserved Farmworkers in California

 ,
,  ,
,  , and
, and 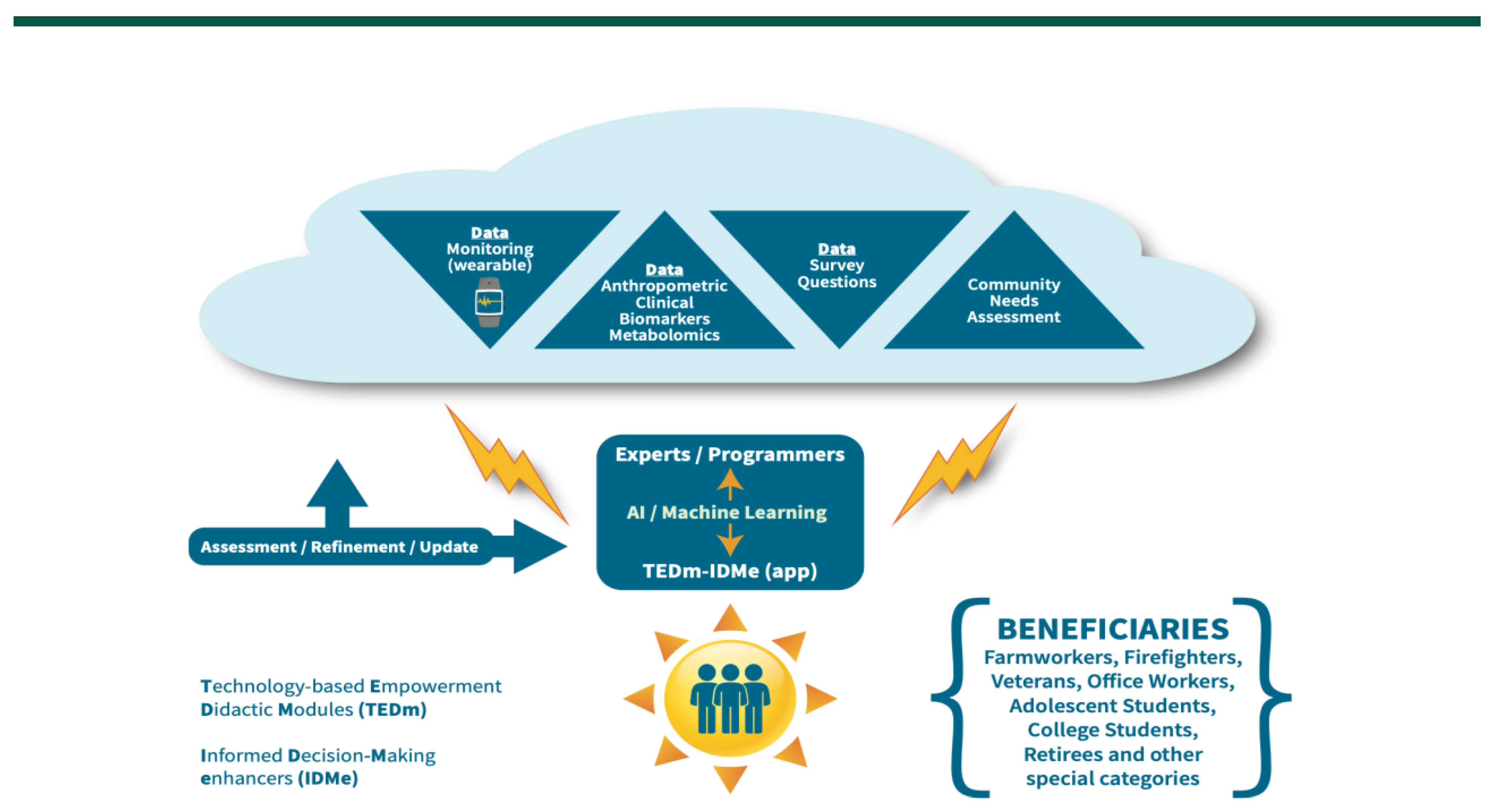{kind=link}
Abstract
:1. Background/Introduction
1.1. Cost of Type 2 Diabetes Mellitus in the US and CA
1.2. Type 2 Diabetes Mellitus among Agriculture Workers
1.3. Feasibility of Education and Technology Use for Disease Risk Attenuation
2. Methodology and Contextual Approach
2.1. The Technology-Based Empowerment Didactic Module (TEDm)
2.2. The Informed Decision-Making Enhancer (IDMe)
2.3. App Development and Infrastructure
- Create artefacts such as design sketches, wireframes, and initial mockups that demonstrate the way the features of the app are presented to the users. As the work proceeds, these initial prototypes are expanded with respect to the addition of features, the revision of the appearance, and the performance from a user’s perspective (e.g., the response time for actions initiated by the user).
- Write code to implement the functionality of the app. In addition to the front end (the part of the app that is visible to the user), there are components performing computational activities behind the scenes. This includes queries to nutritional data bases, collection and storage of user behavior information, generation of recommendations regarding nutrition and behavior modification, and administrative functions such as account management, privacy, and security aspects.
- Develop the infrastructure for the app. The app is to utilize cloud computing and Web services to connect to nutrition data bases, knowledge repositories, data analysis and machine learning tools, and related components. In addition, the collection and management of user data rely on Web infrastructure. A frequently used tool for such purposes is Google’s Firebase mobile development platform specifically intended for fast, efficient, and secure mobile development.
- Features: Desirable aspects of the app, formulated in a language suitable for the intended user population.
- Requirements: More formal specification of the features and functionality of the app, formulated for the use of the software developers.
- Evaluation Criteria: Ideally, these are objective and measurable characteristics of the implemented prototype or system. Within the limits of privacy and technology constraints, we use metrics including time spent with the app, queries made about nutrition, data entry activities. Especially for user interfaces, in-practice user feedback in the form of scales (expressing user satisfaction and similar criteria) or text is commonly used.
- Usability and user experience: Does the current version of the app provide the expected features at that stage? How well can users utilize those features? Are the users satisfied with the way they interact with the app? What problems do users encounter, and what suggestions for improvement do they have.
- Core functionality of the app: Does the app deliver the expected results? Are these results correct and complete (no missing information)?
- Infrastructure: Does the app communicate/interact with respective infrastructure as specified?
2.4. Assumptions
- We assume that farmworkers as indicated by the literature but also common experience, field perception and anecdotal evidence and stakeholder input will have low level of nutrition knowledge and T2DM/CVD knowledge.
- Research has demonstrated that farmworkers would be positive towards using mobile devices to improve their health as it relates to nutrition and T2DM/Hypertension/CVD.
- Our population is typically familiar with smart devices but even the few who are not, are still positively predisposed to learning and are found in a conducive environment which could teach them through their interaction with peers.
2.5. Hypothesis
3. Perspectives and Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lentferink, A.J.; Oldenhuis, H.K.; De Groot, M.; Polstra, L.; Velthuijsen, H.; Van Gemert-Pijnen, J.E. Key Components in eHealth Interventions Combining Self-Tracking and Persuasive eCoaching to Promote a Healthier Lifestyle: A Scoping Review. J. Med Internet Res. 2017, 19, e277. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.L.; Hopkins, C.M.; Brooks, T.L.; Bennett, G.G. Comparing Self-Monitoring Strategies for Weight Loss in a Smartphone App: Randomized Controlled Trial. JMIR mHealth uHealth 2019, 7, e12209. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Classification and Diagnosis of Diabetes. Diabetes Care 2016, 40, S11–S24. [Google Scholar] [CrossRef] [Green Version]
- Ogurtsova, K.; Da Rocha Fernandes, J.D.; Huang, Y.; Linnenkamp, U.; Guariguata, L.; Cho, N.H.; Cavan, D.; Shaw, J.E.; Makaroff, L.E. IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 2017, 128, 40–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association Official Website. Available online: http://www.diabetes.org/diabetes-basics/statistics/?loc=db-slabnav (accessed on 21 August 2019).
- Centers for Disease Control and Prevention. National Diabetes Statistics Report; Centers for Disease Control and Prevention, U.S. Dept of Health and Human Services: Atlanta, GA, USA, 2017; Available online: http://www.diabetes.org/assets/pdfs/basics/cdc-statistics-report-2017.pdf (accessed on 20 August 2022).
- Babey, S.H.; Wolstein, J.; Diamant, A.L.; Goldstein, H. Prediabetes in California: Nearly Half of California Adults on Path to Diabetes; UCLA Center for Health Policy Research and California Center for Public Health Advocacy: Los Angeles, CA, USA, 2016. [Google Scholar]
- Clingerman, E. Type 2 Diabetes Among Migrant and Seasonal Farmworkers. Hisp. Heal. Care Int. 2008, 6, 97–106. [Google Scholar] [CrossRef]
- Nyberg, S.T.; Fransson, E.I.; Heikkilä, K.; Ahola, K.; Alfredsson, L.; Bjorner, J.B.; Borritz, M.; Burr, H.; Dragano, N.; Goldberg, M.; et al. Job Strain as a Risk Factor for Type 2 Diabetes: A Pooled Analysis of 124,808 Men and Women. Diabetes Care 2014, 37, 2268–2275. [Google Scholar] [CrossRef] [Green Version]
- Yu, C.H.Y.; Zinman, B. Type 2 diabetes and impaired glucose tolerance in aboriginal populations: A global perspective. Diabetes Res. Clin. Pract. 2007, 78, 159–170. [Google Scholar] [CrossRef]
- Price, M.; Williamson, D.; McCandless, R.; Mueller, M.; Gregoski, M.; Brunner-Jackson, B.; Treiber, E.; Davidson, L.; Treiber, F.; Afari-Kumah, E.; et al. Hispanic Migrant Farm Workers’ Attitudes Toward Mobile Phone-Based Telehealth for Management of Chronic Health Conditions. J. Med Internet Res. 2013, 15, e76. [Google Scholar] [CrossRef]
- Thompson, R.H.; Snyder, A.; Burt, D.R.; Greiner, D.S.; Luna, M.A. Risk Screening for Cardiovascular Disease and Diabetes in Latino Migrant Farmworkers: A Role for the Community Health Worker. J. Community Heal. 2014, 40, 131–137. [Google Scholar] [CrossRef]
- Ota, C.; DiCarlo, C.E.; Burts, D.C.; Laird, R.; Gioe, C. Training and the needs of adult learners. J. Ext. 2006, 44, 1753–1759. [Google Scholar]
- Knowles, M.S.; Swanson, R.A.; Holton, I.I.I.E.F. The Adult Learner: The Definitive Classic in Adult Education and Human Resource Development, 6th ed.; Elsevier Science and Technology Books: CA, USA, 2006. [Google Scholar]
- Gillis, D.; English, L.M. Extension and health promotion: An adult learning approach. J. Extens. 2001, 39, 1–8. [Google Scholar]
- Svinicki, M.; McKeachie, W.J. McKeachie’s Teaching Tips: Strategies, Research and Theory for College and University Teachers, 14th ed.; Wadsworth, Cengage Learning: Belmont, CA, USA, 2014. [Google Scholar]
- Roka, F.M.; Thissen, C.A.; Monaghan, P.F.; Morera, M.C.; Galindo-Gonzalez, S.; Tovar-Aguilar, J.S. Lessons learned developing an extension-based training program for farm labor supervisors. J. Extens. 2014, 55, v55-4a1. Available online: https://tigerprints.clemson.edu/joejoe/2017august/a1.php (accessed on 19 August 2022).
- Madden, L. Creating a happier, healthier, Hispanic work force. EHS Today 2011, 4, 46. [Google Scholar]
- Unertl, K.M.; Schaefbauer, C.L.; Campbell, T.R.; Senteio, C.; A Siek, K.; Bakken, S.; Veinot, T.C. Integrating community-based participatory research and informatics approaches to improve the engagement and health of underserved populations. J. Am. Med Informatics Assoc. 2015, 23, 60–73. [Google Scholar] [CrossRef]
- Grock, S.; Ku, J.-H.; Kim, J.; Moin, T. A Review of Technology-Assisted Interventions for Diabetes Prevention. Curr. Diabetes Rep. 2017, 17, 1–12. [Google Scholar] [CrossRef]
- Bonoto, B.C.; De Araújo, V.E.; Godói, I.P.; De Lemos, L.L.P.; Godman, B.; Bennie, M.; Diniz, L.M.; Junior, A.A.G. Efficacy of Mobile Apps to Support the Care of Patients With Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. JMIR mHealth uHealth 2017, 5, e4. [Google Scholar] [CrossRef]
- Dunn, C.G.; Turner-McGrievy, G.M.; Wilcox, S.; Hutto, B. Dietary Self-Monitoring Through Calorie Tracking but Not Through a Digital Photography App Is Associated with Significant Weight Loss: The 2SMART Pilot Study—A 6-Month Randomized Trial. J. Acad. Nutr. Diet. 2019, 119, 1525–1532. [Google Scholar] [CrossRef]
- Burke, L.E.; Conroy, M.B.; Sereika, S.M.; Elci, O.U.; Styn, M.A.; Acharya, S.D.; Sevick, M.A.; Ewing, L.J.; Glanz, K. The Effect of Electronic Self-Monitoring on Weight Loss and Dietary Intake: A Randomized Behavioral Weight Loss Trial. Obesity 2011, 19, 338–344. [Google Scholar] [CrossRef]
- Free, C.; Phillips, G.; Galli, L.; Watson, L.; Felix, L.; Edwards, P.; Patel, V.; Haines, A. The Effectiveness of Mobile-Health Technology-Based Health Behaviour Change or Disease Management Interventions for Health Care Consumers: A Systematic Review. PLOS Med. 2013, 10, e1001362. [Google Scholar] [CrossRef] [Green Version]
- Arens, J.H.; Hauth, W.; Weissmann, J. Novel App- and Web-Supported Diabetes Prevention Program to Promote Weight Reduction, Physical Activity, and a Healthier Lifestyle: Observation of the Clinical Application. J. Diabetes Sci. Technol. 2018, 12, 831–838. [Google Scholar] [CrossRef] [Green Version]
- Chew, H.S.J.; Koh, W.L.; Ng, J.S.H.Y.; Tan, K.K. Sustainability of Weight Loss Through Smartphone Apps: Systematic Review and Meta-analysis on Anthropometric, Metabolic, and Dietary Outcomes. J Med Internet Res. 2022, 24, e40141. [Google Scholar] [CrossRef] [PubMed]
- Boucher, J.L. Connectedness: How Technology and Social Networks Are Advancing Diabetes Nutrition Care. Diabetes Spectr. 2019, 32, 69–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerr, D.; King, F.; Klonoff, D.C. Digital Health Interventions for Diabetes: Everything to Gain and Nothing to Lose. Diabetes Spectr. 2019, 32, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Fagherazzi, G.; Ravaud, P. Digital diabetes: Perspectives for diabetes prevention, management and research. Diabetes Metab. 2018, 45, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Asbjørnsen, R.A.; Smedsrød, M.L.; Solberg Nes, L.; Wentzel, J.; Varsi, C.; Hjelmesæth, J.; van Gemert-Pijnen, J.E. Persuasive System Design Principles and Behavior Change Techniques to Stimulate Motivation and Adherence in Electronic Health Interventions to Support Weight Loss Maintenance: Scoping Review. J. Med. Internet Res. 2019, 21, e14265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, Q.; Qu, K.; Luo, Y.; Yin, D.; Ju, Y.; Tang, H. Predicting Diabetes Mellitus With Machine Learning Techniques. Front. Genet. 2018, 9, 515. [Google Scholar] [CrossRef]
- Tsao, H.-Y.; Chan, P.-Y.; Su, E.C.-Y. Predicting diabetic retinopathy and identifying interpretable biomedical features using machine learning algorithms. BMC Bioinform. 2018, 19, 283. [Google Scholar] [CrossRef] [Green Version]
- Farran, B.; Channanath, A.M.; Behbehani, K.; Thanaraj, T.A. Predictive models to assess risk of type 2 diabetes, hypertension and comorbidity: Machine-learning algorithms and validation using national health data from Kuwait—A cohort study. BMJ Open 2013, 3, e002457. [Google Scholar] [CrossRef] [Green Version]
- Swapna, G.; Vinayakumar, R.; Soman, K.P. Diabetes detection using deep learning algorithms. ICT Express 2018, 4, 243–246. [Google Scholar] [CrossRef]
- Vyas, S.; Ranjan, R.; Singh, N.; Mathur, A. Review of Predictive Analysis Techniques for Analysis Diabetes Risk. In Proceedings of the 2019 Amity International Conference on Artificial Intelligence (AICAI), Dubai, United Arab Emirates, 4–6 February 2019; pp. 626–631. [Google Scholar] [CrossRef]
- Meng, X.-H.; Huang, Y.-X.; Rao, D.-P.; Zhang, Q.; Liu, Q. Comparison of three data mining models for predicting diabetes or prediabetes by risk factors. Kaohsiung J. Med Sci. 2013, 29, 93–99. [Google Scholar] [CrossRef] [Green Version]
- Alam, T.M.; Iqbal, M.A.; Ali, Y.; Wahab, A.; Ijaz, S.; Baig, T.I.; Hussain, A.; Malik, M.A.; Raza, M.M.; Ibrar, S.; et al. A model for early prediction of diabetes. Informatics Med. Unlocked 2019, 16, 100204. [Google Scholar] [CrossRef]
- Wu, H.; Yang, S.; Huang, Z.; He, J.; Wang, X. Type 2 diabetes mellitus prediction model based on data mining. Inform. Med. Unlocked 2018, 10, 100–107. [Google Scholar] [CrossRef]
- Kavakiotis, I.; Tsave, O.; Salifoglou, A.; Maglaveras, N.; Vlahavas, I.; Chouvarda, I. Machine Learning and Data Mining Methods in Diabetes Research. Comput. Struct. Biotechnol. J. 2017, 15, 104–116. [Google Scholar] [CrossRef]
- Li, S. Machine Learning for Diabetes. Towards Data Science. Available online: https://towardsdatascience.com/machine-learning-for-diabetes-562dd7df4d42 (accessed on 11 September 2019).
- Sennaar, K. Machine Learning for Managing Diabetes: 5 Current Use Cases. Emerj. Available online: https://emerj.com/ai-sector-overviews/machine-learning-managing-diabetes-5-current-use-cases/ (accessed on 11 September 2019).
- Cahn, A.; Shoshan, A.; Sagiv, T.; Yesharim, R.; Raz, I.; Goshen, R. Use of a Machine Learning Algorithm Improves Prediction of Progression to Diabetes. Diabetes 2018, 67, 1286-p. [Google Scholar] [CrossRef]
- Dankwa-Mullan, I.; Rivo, M.; Sepulveda, M.; Park, Y.; Snowdon, J.; Rhee, K. Transforming Diabetes Care Through Artificial Intelligence: The Future Is Here. Popul. Heal. Manag. 2019, 22, 229–242. [Google Scholar] [CrossRef] [Green Version]
- Contreras, I.; Vehi, J. Artificial Intelligence for Diabetes Management and Decision Support: Literature Review. J. Med Internet Res. 2018, 20, e10775. [Google Scholar] [CrossRef]
- Kent, J. Artificial Intelligence Mobile Coach Can Aid Diabetes Care. HealthITAnalytics. Available online: https://healthitanalytics.com/news/artificial-intelligence-mobile-coach-can-aid-diabetes-care (accessed on 11 September 2019).
- Dietsche, E. Israeli startup Sweetch leverages AI for diabetes prevention. MedCity News. December 2018. Available online: https://medcitynews.com/2018/12/israeli-startup-sweetch/ (accessed on 11 September 2019).
- Stircu, S. How artificial intelligence will shape the future of diabetes. Medtech Views. November 2017. Available online: http://www.medtechviews.eu/article/how-artificial-intelligence-will-shape-future-diabetes (accessed on 11 September 2019).
- Hartson, R.; Pyla, P.S. The UX Book: Process and Guidelines for Ensuring a Quality User Experience; Elsevier: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Garrett, J.J. The Elements of User Experience: User-Centered Design for the Web and Beyond; Pearson Education: London, UK, 2010. [Google Scholar]
- Nielsen, J.; Budiu, R. Mobile Usability, 1st ed.; New Riders: Berkeley, CA, USA, 2012. [Google Scholar]
- Nayebi, F.; Desharnais, J.-M.; Abran, A.; Nayebi, F.; Desharnais, J.; Abran, A. The state of the art of mobile application usability evaluation. In Proceedings of the 2012 25th IEEE Canadian Conference on Electrical and Computer Engineering (CCECE), Montreal, QC, Canada, 29 April–2 May 2012; pp. 1–4. [Google Scholar] [CrossRef]
- Moumane, K.; Idri, A.; Abran, A. Usability evaluation of mobile applications using ISO 9241 and ISO 25062 standards. SpringerPlus 2016, 5, 548. [Google Scholar] [CrossRef] [Green Version]
- Sikalidis, A.K. From Food for Survival to Food for Personalized Optimal Health: A Historical Perspective of How Food and Nutrition Gave Rise to Nutrigenomics. J. Am. Coll. Nutr. 2018, 38, 84–95. [Google Scholar] [CrossRef]
- Marcum, J.A. Nutrigenetics/Nutrigenomics, Personalized Nutrition, and Precision Healthcare. Curr. Nutr. Rep. 2020, 9, 338–345. [Google Scholar] [CrossRef]
- Mullins, V.A.; Bresette, W.; Johnstone, L.; Hallmark, B.; Chilton, F.H. Genomics in Personalized Nutrition: Can You “Eat for Your Genes”? Nutrients 2020, 12, 3118. [Google Scholar] [CrossRef]
- Ahluwalia, M.K. Nutrigenetics and nutrigenomics—A personalized approach to nutrition. Adv Genet. 2021, 108, 277–340. [Google Scholar] [CrossRef]
- Samieri, C.; Yassine, H.N.; van Lent, D.M.; Lefèvre-Arbogast, S.; van de Rest, O.; Bowman, G.L.; Scarmeas, N. Personalized nutrition for dementia prevention. Alzheimer’s Dement. 2021, 18, 1424–1437. [Google Scholar] [CrossRef]
- Kristo, A.; Sikalidis, A.; Uzun, A. Traditional Societal Practices Can Avert Poor Dietary Habits and Reduce Obesity Risk in Preschool Children of Mothers with Low Socioeconomic Status and Unemployment. Behav. Sci. 2021, 11, 42. [Google Scholar] [CrossRef] [PubMed]
- Kristo, A.S.; Çinar, N.; Kucuknil, S.L.; Sikalidis, A.K. Technological Devices and Their Effect on Preschool Children’s Eating Habits in Communities of Mixed Socioeconomic Status in Istanbul; a Pilot Cross-Sectional Study. Behav. Sci. 2021, 11, 157. [Google Scholar] [CrossRef] [PubMed]
- Sikalidis, A.; Kelleher, A.; Kristo, A. Mediterranean Diet. Encyclopedia 2021, 1, 371–387. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sikalidis, A.K.; Kristo, A.S.; Reaves, S.K.; Kurfess, F.J.; DeLay, A.M.; Vasilaky, K.; Donegan, L. Capacity Strengthening Undertaking—Farm Organized Response of Workers against Risk for Diabetes: (C.S.U.—F.O.R.W.A.R.D. with Cal Poly)—A Concept Approach to Tackling Diabetes in Vulnerable and Underserved Farmworkers in California. Sensors 2022, 22, 8299. https://0-doi-org.brum.beds.ac.uk/10.3390/s22218299
Sikalidis AK, Kristo AS, Reaves SK, Kurfess FJ, DeLay AM, Vasilaky K, Donegan L. Capacity Strengthening Undertaking—Farm Organized Response of Workers against Risk for Diabetes: (C.S.U.—F.O.R.W.A.R.D. with Cal Poly)—A Concept Approach to Tackling Diabetes in Vulnerable and Underserved Farmworkers in California. Sensors. 2022; 22(21):8299. https://0-doi-org.brum.beds.ac.uk/10.3390/s22218299
Chicago/Turabian StyleSikalidis, Angelos K., Aleksandra S. Kristo, Scott K. Reaves, Franz J. Kurfess, Ann M. DeLay, Kathryn Vasilaky, and Lorraine Donegan. 2022. "Capacity Strengthening Undertaking—Farm Organized Response of Workers against Risk for Diabetes: (C.S.U.—F.O.R.W.A.R.D. with Cal Poly)—A Concept Approach to Tackling Diabetes in Vulnerable and Underserved Farmworkers in California" Sensors 22, no. 21: 8299. https://0-doi-org.brum.beds.ac.uk/10.3390/s22218299