
Utility and Usability of Two Forms of Supplemental Vibrotactile Kinesthetic Feedback for Enhancing Movement Accuracy and Efficiency in Goal-Directed Reaching


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Recruitment
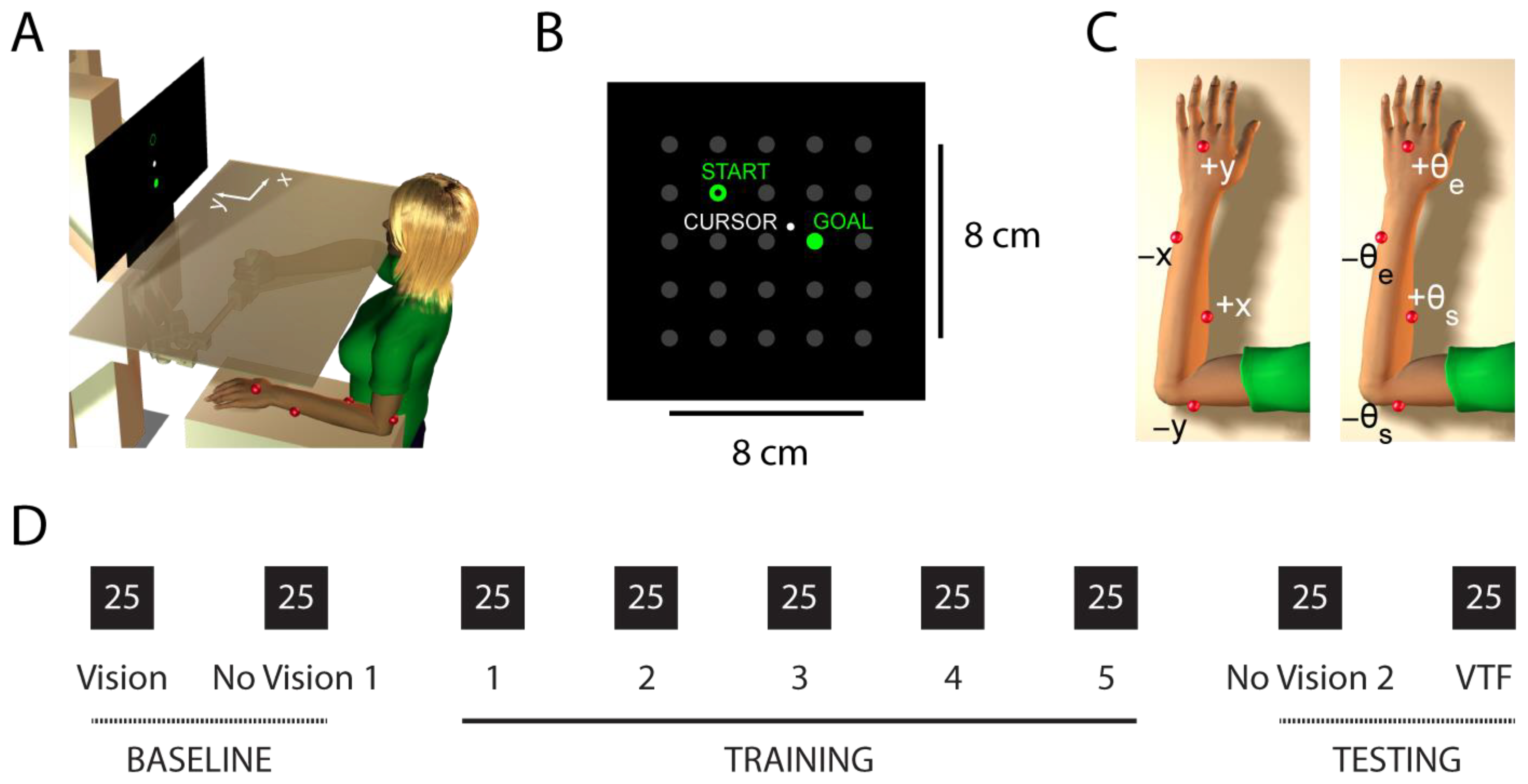
2.2. Experimental Set-Up
2.3. Vibrotactile Feedback Encoding Schemes
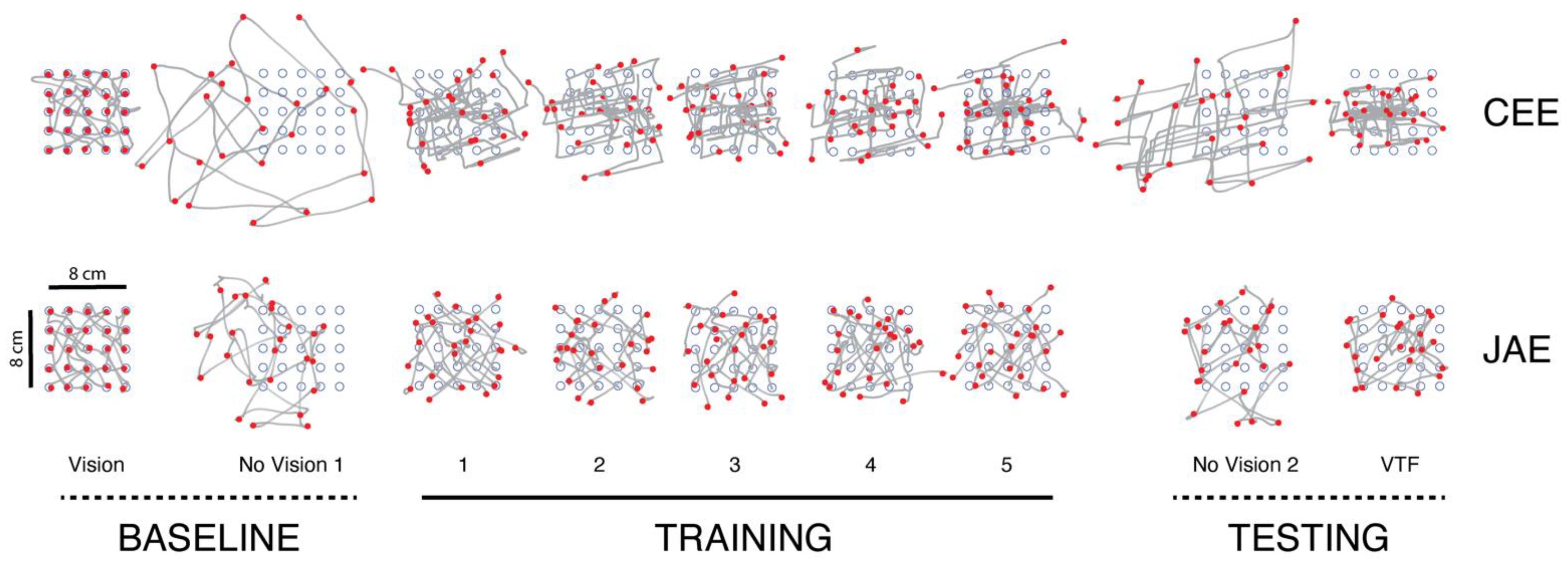
2.4. Testing Procedures
2.5. Analysis of Kinematic Data
2.6. Assessment of Subjective User Experience
2.7. Statistical Hypothesis Testing
3. Results
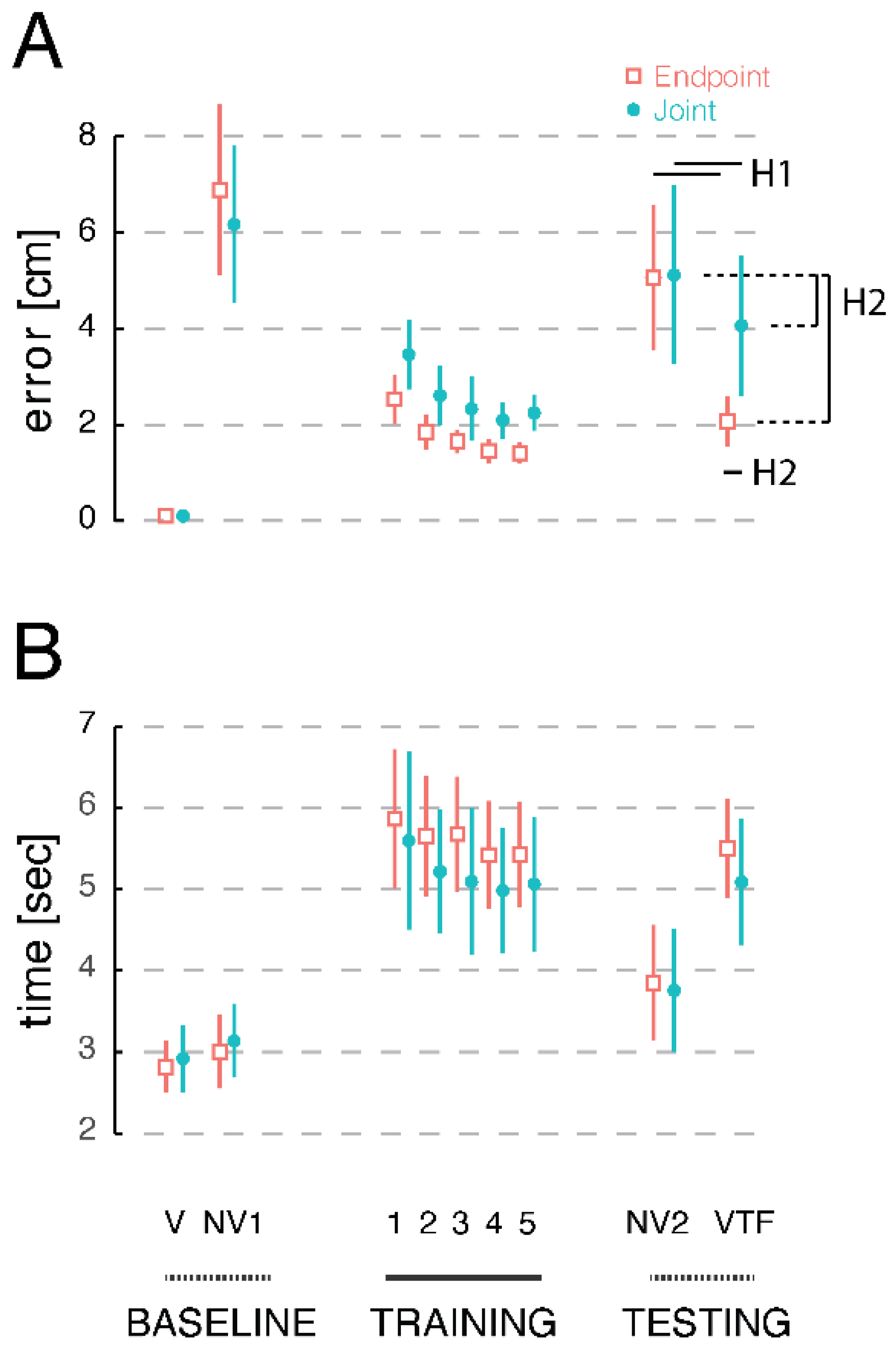
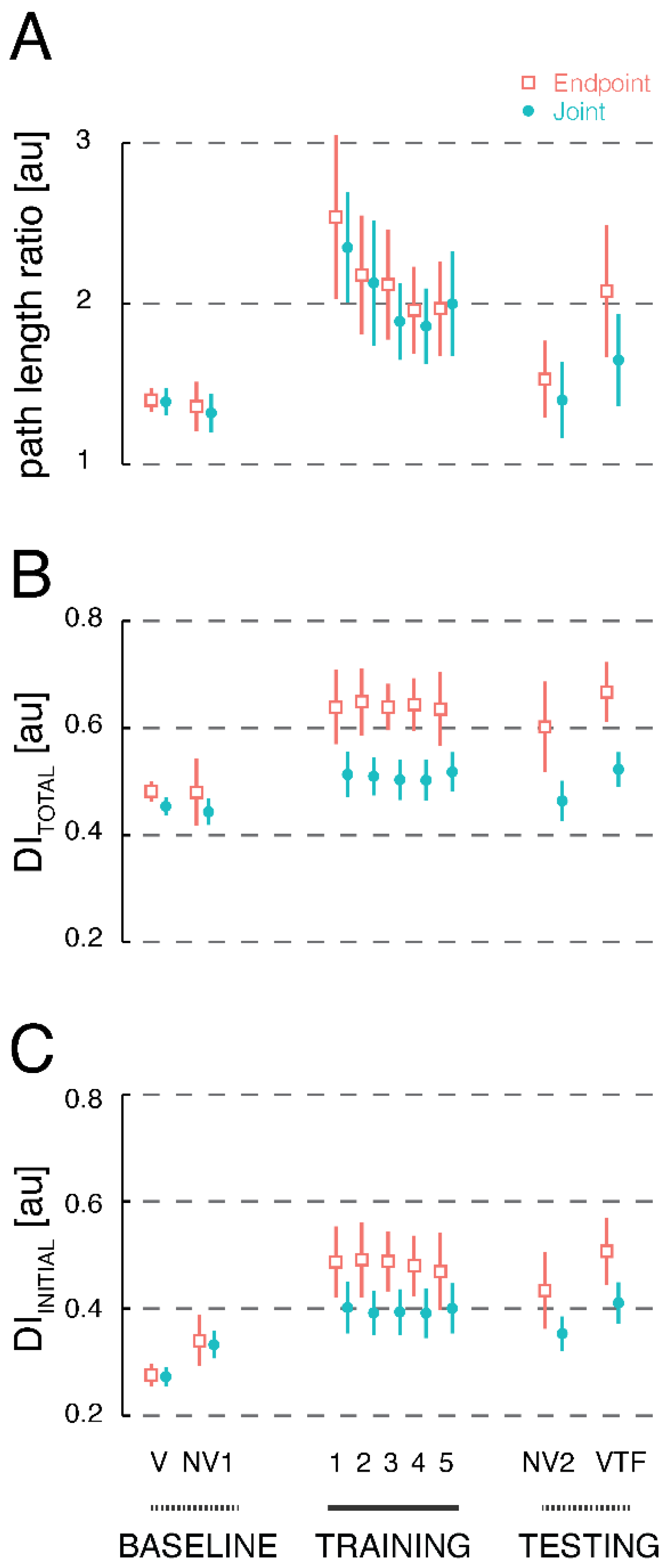
3.1. Effects of Supplemental Vibrotactile Feedback on Primary Measures of Reach Accuracy and Efficiency
3.2. Secondary Analyses of Kinematic Performance during Reaching with Supplemental Vibrotactile Feedback
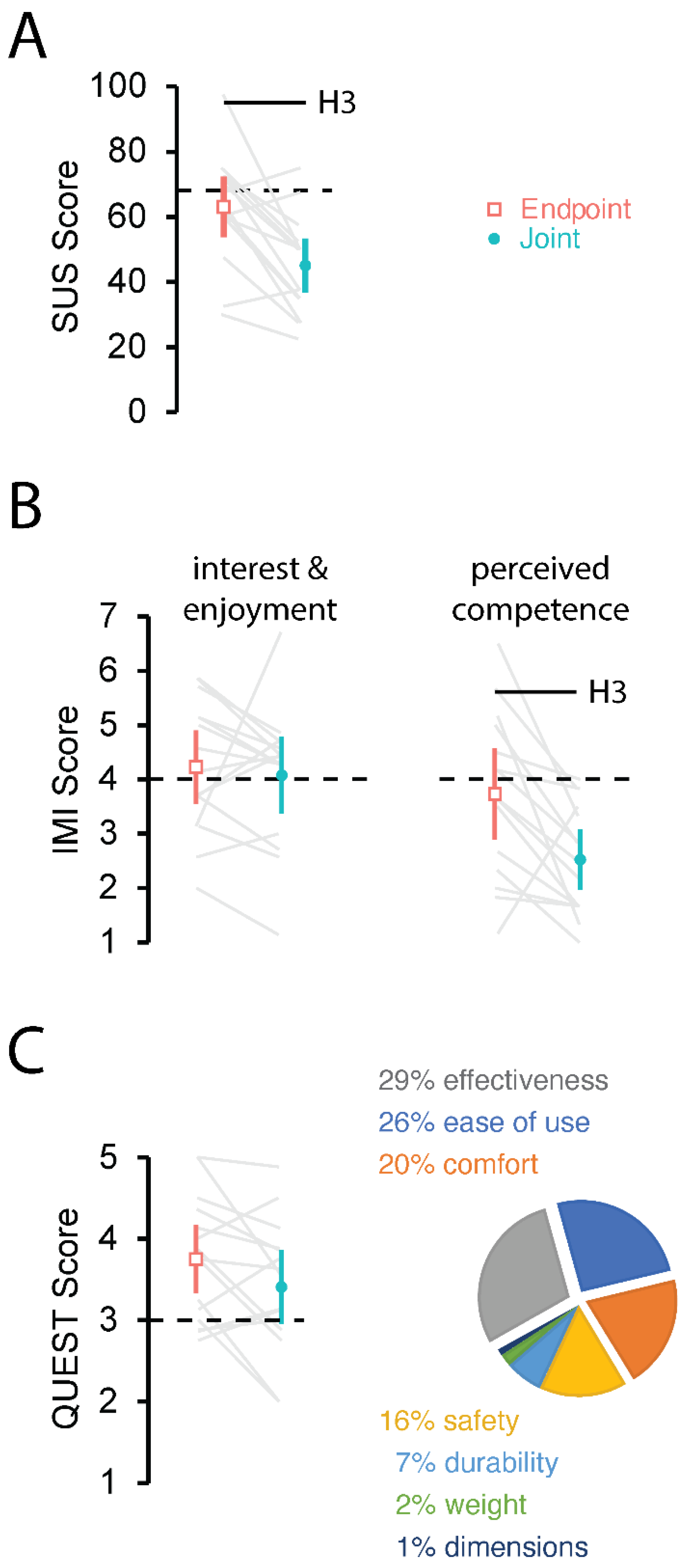
3.3. Subjective User Experience between Cartesian Endpoint Encoding and Joint Angle Encoding
4. Discussion
4.1. Information Encodings for Supplemental Guidance of Movement
4.2. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
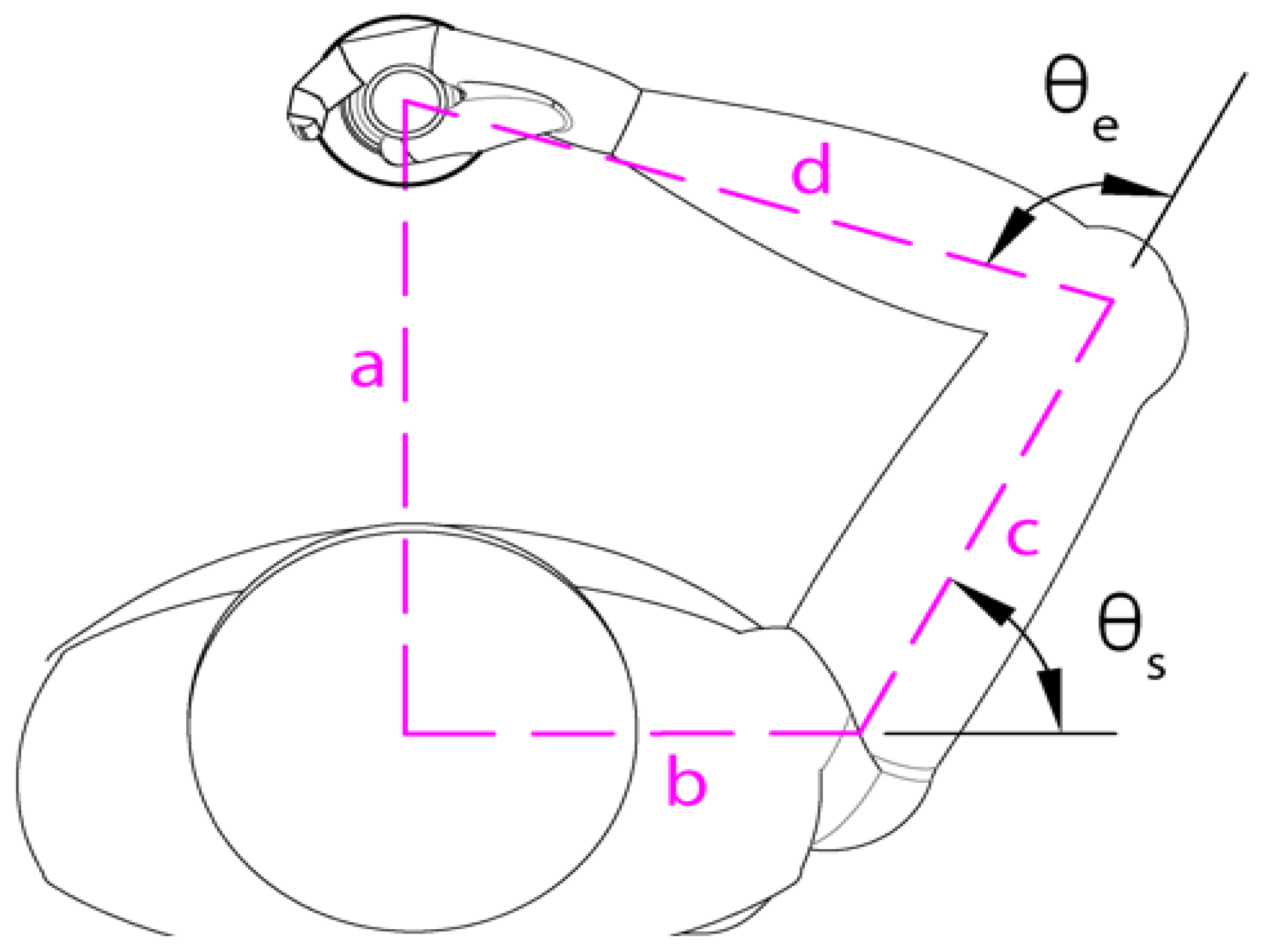
| Subject Number | Sex | Age | YHome to YShoulder (cm) | XHome to XShoulder (cm) | c: Shoulder to Elbow (cm) | d: Elbow to Handle (cm) |
|---|---|---|---|---|---|---|
| 1 | Male | 26 | 23 | 9 | 26 | 32 |
| 2 | Male | 25 | 24 | 8 | 35 | 36 |
| 3 | Female | 24 | 19 | 10 | 30 | 31 |
| 4 | Male | 24 | 28 | 8 | 34 | 36 |
| 5 | Female | 22 | 20 | 9 | 26 | 28 |
| 6 | Male | 27 | 23 | 8 | 30 | 35 |
| 7 | Female | 24 | 24 | 10 | 29 | 29 |
| 8 | Male | 27 | 24 | 8 | 29 | 36 |
| 9 | Female | 25 | 22 | 8 | 26 | 29 |
| 10 | Male | 25 | 19 | 10 | 30 | 31 |
| 11 | Female | 26 | 20 | 7 | 24 | 29 |
| 12 | Female | 27 | 23 | 10 | 27 | 26 |
| 13 | Female | 23 | 24 | 9 | 29 | 32 |
| 14 | Male | 20 | 21 | 17 | 31 | 36 |
| 15 | Female | 23 | 20 | 9 | 27 | 28 |
References
- Sober, S.J.; Sabes, P.N. Multisensory Integration during Motor Planning. J. Neurosci. 2003, 23, 6982–6992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lateiner, J.E.; Sainburg, R.L. Differential Contributions of Vision and Proprioception to Movement Accuracy. Exp. Brain Res. 2003, 151, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Scheidt, R.A.; Conditt, M.A.; Secco, E.L.; Mussa-Ivaldi, F.A. Interaction of Visual and Proprioceptive Feedback during Adaptation of Human Reaching Movements. J. Neurophysiol. 2005, 93, 3200–3213. [Google Scholar] [CrossRef] [PubMed]
- Sarlegna, F.R.; Sainburg, R.L. The Roles of Vision and Proprioception in the Planning of Reaching Movements. Adv. Exp. Med. Biol. 2009, 629, 317–335. [Google Scholar]
- Judkins, T.; Scheidt, R.A. Visuo-Proprioceptive Interactions during Adaptation of the Human Reach. J. Neurophysiol. 2014, 111, 868–887. [Google Scholar] [CrossRef] [Green Version]
- Ghez, C.; Scheidt, R.; Heijink, H. Different Learned Coordinate Frames for Planning Trajectories and Final Positions in Reaching. J. Neurophysiol. 2007, 98, 3614–3626. [Google Scholar] [CrossRef]
- Liu, X.; Scheidt, R.A. Contributions of Online Visual Feedback to the Learning and Generalization of Novel Finger Coordination Patterns. J. Neurophysiol. 2008, 99, 2546–2557. [Google Scholar] [CrossRef] [Green Version]
- Lantagne, D.D.; Mrotek, L.A.; Slick, R.; Beardsley, S.A.; Thomas, D.G.; Scheidt, R.A. Contributions of Implicit and Explicit Memories to Sensorimotor Adaptation of Movement Extent during Goal-Directed Reaching. Exp. Brain Res. 2021, 239, 2445–2459. [Google Scholar] [CrossRef]
- Scheidt, R.A.; Stoeckmann, T. Reach Adaptation and Final Position Control Amid Environmental Uncertainty after Stroke. J. Neurophysiol. 2007, 97, 2824–2836. [Google Scholar] [CrossRef] [Green Version]
- Ballardini, G.; Krueger, A.; Giannoni, P.; Marinelli, L.; Casadio, M.; Scheidt, R.A. Effect of Short-Term Exposure to Supplemental Vibrotactile Kinesthetic Feedback on Goal-Directed Movements after Stroke: A Proof of Concept Case Series. Sensors 2021, 21, 1519. [Google Scholar] [CrossRef]
- Kaczmarek, K.A.; Webster, J.G.; Bach-y-Rita, P.; Tompkins, W.J. Electrotactile and Vibrotactile Displays for Sensory Substitution Systems. IEEE Trans. Biomed. Eng. 1991, 38, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Cuppone, A.V.; Squeri, V.; Semprini, M.; Masia, L.; Konczak, J. Robot-Assisted Proprioceptive Training with Added Vibro-Tactile Feedback Enhances Somatosensory and Motor Performance. PLoS ONE 2016, 11, e0164511. [Google Scholar] [CrossRef] [Green Version]
- Bark, K.; Khanna, P.; Irwin, R.; Kapur, P.; Jax, S.A.; Buxbaum, L.J.; Kuchenbecker, K.J. Lessons in Using Vibrotactile Feedback to Guide Fast Arm Motions. In Proceedings of the 2011 IEEE World Haptics Conference IEEE, Istanbul, Turkey, 21–24 June 2011; pp. 355–360. [Google Scholar]
- Bark, K.; Hyman, E.; Tan, F.; Cha, E.; Jax, S.A.; Buxbaum, L.J.; Kuchenbecker, K.J. Effects of Vibrotactile Feedback on Human Learning of Arm Motions. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 51–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sienko, K.H.; Balkwill, M.D.; Oddsson, L.I.E.; Wall, C. Effects of Multi-Directional Vibrotactile Feedback on Vestibular-Deficient Postural Performance during Continuous Multi-Directional Support Surface Perturbations. J. Vestib. Res. 2008, 18, 273–285. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.-C.; Chen, S.; Sienko, K.H. A Wearable Device for Real-Time Motion Error Detection and Vibrotactile Instructional Cuing. IEEE Trans. Neural Syst. Rehabil. Eng. 2011, 19, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Krueger, A.R.; Giannoni, P.; Shah, V.; Casadio, M.; Scheidt, R.A. Supplemental Vibrotactile Feedback Control of Stabilization and Reaching Actions of the Arm Using Limb State and Position Error Encodings. J. Neuroeng. Rehabil. 2017, 14, 36. [Google Scholar] [CrossRef] [Green Version]
- Risi, N.; Shah, V.; Mrotek, L.A.; Casadio, M.; Scheidt, R.A. Supplemental Vibrotactile Feedback of Real-Time Limb Position Enhances Precision of Goal-Directed Reaching. J. Neurophysiol. 2019, 122, 22–38. [Google Scholar] [CrossRef]
- Shah, V.A.; Thomas, A.; Mrotek, L.A.; Casadio, M.; Scheidt, R.A. Extended Training Improves the Accuracy and Efficiency of Goal-Directed Reaching Guided by Supplemental Kinesthetic Vibrotactile Feedback. Exp. Brain Res. 2023, 241, 479–493. [Google Scholar] [CrossRef]
- Raj, A.K.; Braithwaite, G. The Tactile Situation Awareness System in Rotary Wing Aircraft: Flight Test Results. Curr. Aeromed. Issues Rotary Wing Oper. 1998, 19, 5. [Google Scholar]
- van Erp, J.B.F.; van Veen, H. A Multi-Purpose Tactile Vest for Astronauts in the International Space Station. In Proceedings of the Eurohaptics 2003 Proceedings, Dublin, Ireland, 6–9 July 2003. [Google Scholar]
- van Erp, J.B.F.; van Veen, H.A.H.C.; Jansen, C.; Dobbins, T. Waypoint Navigation with a Vibrotactile Waist Belt. ACM Trans. Appl. Percept. 2005, 2, 106–117. [Google Scholar] [CrossRef]
- Vasudevan, M.K.; Isaac, J.H.R.; Sadanand, V.; Muniyandi, M. Novel Virtual Reality Based Training System for Fine Motor Skills: Towards Developing a Robotic Surgery Training System. Int. J. Med. Robot. Comput. Assist. Surg. 2020, 16, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Spelmezan, D.; Jacobs, M.; Hilgers, A.; Borchers, J. Tactile Motion Instructions for Physical Activities. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Boston, MA, USA, 4–9 April 2009; ACM: New York, NY, USA, 2009; pp. 2243–2252. [Google Scholar]
- Peeters, T.; Vleugels, J.; Garimella, R.; Truijen, S.; Saeys, W.; Verwulgen, S. Vibrotactile Feedback for Correcting Aerodynamic Position of a Cyclist. J. Sports Sci. 2020, 38, 2193–2199. [Google Scholar] [CrossRef]
- Lindeman, R.W.; Yanagida, Y.; Hosaka, K.; Abe, S. The TactaPack: A Wireless Sensor/Actuator Package for Physical Therapy Applications. In Proceedings of the 14th Symposium on Haptic Interfaces for Virtual Environment and Teleoperator Systems, Alexandria, VA, USA, 25–26 March 2006; IEEE: Piscataway, NJ, USA, 2006; pp. 337–341. [Google Scholar]
- Held, J.P.; Klaassen, B.; van Beijnum, B.-J.F.; Luft, A.R.; Veltink, P.H. Usability Evaluation of a VibroTactile Feedback System in Stroke Subjects. Front. Bioeng. Biotechnol. 2017, 4, 98. [Google Scholar] [CrossRef] [Green Version]
- Schoonmaker, R.E.; Cao, C.G.L. Vibrotactile Force Feedback System for Minimally Invasive Surgical Procedures. In Proceedings of the 2006 IEEE International Conference on Systems, Man and Cybernetics, Taipei, Taiwan, 8–11 October 2006; IEEE: Piscataway, NJ, USA, 2006; pp. 2464–2469. [Google Scholar]
- Abiri, A.; Juo, Y.-Y.; Tao, A.; Askari, S.J.; Pensa, J.; Bisley, J.W.; Dutson, E.P.; Grundfest, W.S. Artificial Palpation in Robotic Surgery Using Haptic Feedback. Surg. Endosc. 2019, 33, 1252–1259. [Google Scholar] [CrossRef]
- Kent, B.; Rossa, C. Development of a Tissue Discrimination Electrode Embedded Surgical Needle Using Vibro-Tactile Feedback Derived from Electric Impedance Spectroscopy. Med. Biol. Eng. Comput. 2022, 60, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Ruffaldi, E.; Filippeschi, A.; Frisoli, A.; Sandoval, O.; Avizzano, C.A.; Bergamasco, M. Vibrotactile Perception Assessment for a Rowing Training System. In Proceedings of the World Haptics 2009—Third Joint EuroHaptics Conference and Symposium on Haptic Interfaces for Virtual Environment and Teleoperator Systems, Salt Lake City, UT, USA, 18–20 March 2009; IEEE: Piscataway, NJ, USA, 2009; pp. 350–355. [Google Scholar]
- Lieberman, J.; Breazeal, C. TIKL: Development of a Wearable Vibrotactile Feedback Suit for Improved Human Motor Learning. IEEE Trans. Robot. 2007, 23, 919–926. [Google Scholar] [CrossRef]
- van der Linden, J.; Schoonderwaldt, E.; Bird, J.; Johnson, R. MusicJacket—Combining Motion Capture and Vibrotactile Feedback to Teach Violin Bowing. IEEE Trans. Instrum. Meas. 2011, 60, 104–113. [Google Scholar] [CrossRef]
- Conrad, M.O.; Scheidt, R.A.; Schmit, B.D. Effects of Wrist Tendon Vibration on Arm Tracking in People Poststroke. J. Neurophysiol. 2011, 106, 1480–1488. [Google Scholar] [CrossRef] [Green Version]
- Jones, L.A.; Sarter, N.B. Tactile Displays: Guidance for Their Design and Application. Hum. Factors J. Hum. Factors Ergon. Soc. 2008, 50, 90–111. [Google Scholar] [CrossRef]
- Shull, P.B.; Damian, D.D. Haptic Wearables as Sensory Replacement, Sensory Augmentation and Trainer—A Review. J. Neuroeng. Rehabil. 2015, 12, 59. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; Markopoulos, P.; Yu, B.; Chen, W.; Timmermans, A. Interactive Wearable Systems for Upper Body Rehabilitation: A Systematic Review. J. Neuroeng. Rehabil. 2017, 14, 20. [Google Scholar] [CrossRef] [Green Version]
- Abboud, S.; Hanassy, S.; Levy-Tzedek, S.; Maidenbaum, S.; Amedi, A. EyeMusic: Introducing a “Visual” Colorful Experience for the Blind Using Auditory Sensory Substitution. Restor. Neurol. Neurosci. 2014, 32, 247–257. [Google Scholar] [CrossRef] [Green Version]
- Amedi, A.; Stern, W.M.; Camprodon, J.A.; Bermpohl, F.; Merabet, L.; Rotman, S.; Hemond, C.; Meijer, P.; Pascual-Leone, A. Shape Conveyed by Visual-to-Auditory Sensory Substitution Activates the Lateral Occipital Complex. Nat. Neurosci. 2007, 10, 687–689. [Google Scholar] [CrossRef]
- Dahl, L.; Knowlton, C.; Zaferiou, A. Developing Real-Time Sonification with Optical Motion Capture to Convey Balance-Related Metrics to Dancers. In Proceedings of the 6th International Conference on Movement and Computing, Tempe, AZ, USA, 10–12 October 2019; ACM: New York, NY, USA, 2019; pp. 1–6. [Google Scholar]
- Karatsidis, A.; Richards, R.E.; Konrath, J.M.; van den Noort, J.C.; Schepers, H.M.; Bellusci, G.; Harlaar, J.; Veltink, P.H. Validation of Wearable Visual Feedback for Retraining Foot Progression Angle Using Inertial Sensors and an Augmented Reality Headset. J. Neuroeng. Rehabil. 2018, 15, 78. [Google Scholar] [CrossRef]
- Dosen, S.; Markovic, M.; Strbac, M.; Belic, M.; Kojic, V.; Bijelic, G.; Keller, T.; Farina, D. Multichannel Electrotactile Feedback With Spatial and Mixed Coding for Closed-Loop Control of Grasping Force in Hand Prostheses. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 183–195. [Google Scholar] [CrossRef]
- Ptito, M. Cross-Modal Plasticity Revealed by Electrotactile Stimulation of the Tongue in the Congenitally Blind. Brain 2005, 128, 606–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaczmarek, K.A.; Tyler, M.E.; Bach-Y-Rita, P. Electrotactile Haptic Display on the Fingertips: Preliminary Results. In Proceedings of the 16th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Baltimore, MD, USA, 3–6 November 1994; IEEE: Piscataway, NJ, USA, 1994; pp. 940–941. [Google Scholar]
- Stronks, H.C.; Mitchell, E.B.; Nau, A.C.; Barnes, N. Visual Task Performance in the Blind with the BrainPort V100 Vision Aid. Expert Rev. Med. Devices 2016, 13, 919–931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapur, P.; Premakumar, S.; Jax, S.A.; Buxbaum, L.J.; Dawson, A.M.; Kuchenbecker, K.J. Vibrotactile Feedback System for Intuitive Upper-Limb Rehabilitation. In Proceedings of the World Haptics 2009—Third Joint EuroHaptics Conference and Symposium on Haptic Interfaces for Virtual Environment and Teleoperator Systems, Salt Lake City, UT, USA, 18–20 March 2009; IEEE: Piscataway, NJ, USA, 2009; pp. 621–622. [Google Scholar]
- Tzorakoleftherakis, E.; Bengtson, M.C.; Mussa-Ivaldi, F.A.; Scheidt, R.A.; Murphey, T.D. Tactile Proprioceptive Input in Robotic Rehabilitation after Stroke. In Proceedings of the 2015 IEEE International Conference on Robotics and Automation (ICRA), Seattle, WA, USA, 26–30 May 2015; pp. 6475–6481. [Google Scholar]
- Ferris, T.K.; Sarter, N. Continuously Informing Vibrotactile Displays in Support of Attention Management and Multitasking in Anesthesiology. Hum. Factors J. Hum. Factors Ergon. Soc. 2011, 53, 600–611. [Google Scholar] [CrossRef] [PubMed]
- Kinnaird, C.; Lee, J.; Carender, W.J.; Kabeto, M.; Martin, B.; Sienko, K.H. The Effects of Attractive vs. Repulsive Instructional Cuing on Balance Performance. J. Neuroeng. Rehabil. 2016, 13, 29. [Google Scholar] [CrossRef] [Green Version]
- Elsayed, H.; Weigel, M.; Müller, F.; Schmitz, M.; Marky, K.; Günther, S.; Riemann, J.; Mühlhäuser, M. VibroMap: Understanding the Spacing of Vibrotactile Actuators across the Body. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 2020, 4, 1–16. [Google Scholar] [CrossRef]
- Bao, T.; Su, L.; Kinnaird, C.; Kabeto, M.; Shull, P.B.; Sienko, K.H. Vibrotactile Display Design: Quantifying the Importance of Age and Various Factors on Reaction Times. PLoS ONE 2019, 14, e0219737. [Google Scholar] [CrossRef] [Green Version]
- Shah, V.A.; Casadio, M.; Scheidt, R.A.; Mrotek, L.A. Spatial and Temporal Influences on Discrimination of Vibrotactile Stimuli on the Arm. Exp. Brain Res. 2019, 237, 2075–2086. [Google Scholar] [CrossRef] [Green Version]
- Brooke, J. SUS: A Quick and Dirty Usability Scale. Usability Eval. Ind. 1995, 189, 4–7. [Google Scholar]
- McAuley, E.; Duncan, T.; Tammen, V.V. Psychometric Properties of the Intrinsic Motivation Inventory in a Competitive Sport Setting: A Confirmatory Factor Analysis. Res. Q. Exerc. Sport 1989, 60, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Demers, L.; Weiss-Lambrou, R.; Ska, B. Item Analysis of the Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST). Assist. Technol. 2000, 12, 96–105. [Google Scholar] [CrossRef]
- Demers, L.; Monette, M.; Lapierre, Y.; Arnold, D.L.; Wolfson, C. Reliability, Validity, and Applicability of the Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST 2.0) for Adults with Multiple Sclerosis. Disabil. Rehabil. 2002, 24, 21–30. [Google Scholar] [CrossRef]
- Scheidt, R.A.; Lillis, K.P.; Emerson, S.J. Visual, Motor and Attentional Influences on Proprioceptive Contributions to Perception of Hand Path Rectilinearity during Reaching. Exp. Brain Res. 2010, 204, 239–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitman, P.A.; Adigun, O.O. Anatomy, Skin, Dermatomes. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK535401/ (accessed on 14 March 2023).
- Nolan, M.F. Two-Point Discrimination Assessment in the Upper Limb in Young Adult Men and Women. Phys. Ther. 1982, 62, 965–969. [Google Scholar] [CrossRef] [PubMed]
- Shah, V.A.; Casadio, M.; Scheidt, R.A.; Mrotek, L.A. Vibration Propagation on the Skin of the Arm. Appl. Sci. 2019, 9, 4329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flanagan, J.R.; Rao, A.K. Trajectory Adaptation to a Nonlinear Visuomotor Transformation: Evidence of Motion Planning in Visually Perceived Space. J. Neurophysiol. 1995, 74, 2174–2178. [Google Scholar] [CrossRef]
- Bangor, A.; Kortum, P.; Miller, J. Determining What Individual SUS Scores Mean: Adding an Adjective Rating Scale. J. Usability Stud. 2009, 4, 114–123. [Google Scholar]
- Colombo, R.; Pisano, F.; Mazzone, A.; Delconte, C.; Micera, S.; Carrozza, M.C.; Dario, P.; Minuco, G. Design Strategies to Improve Patient Motivation during Robot-Aided Rehabilitation. J. Neuroeng. Rehabil. 2007, 4, 3. [Google Scholar] [CrossRef] [Green Version]
- Prange, G.B.; Kottink, A.I.R.; Buurke, J.H.; Eckhardt, M.M.E.M.; van Keulen-Rouweler, B.J.; Ribbers, G.M.; Rietman, J.S. The Effect of Arm Support Combined with Rehabilitation Games on Upper-Extremity Function in Subacute Stroke: A Randomized Controlled Trial. Neurorehabil. Neural Repair 2015, 29, 174–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wann, J.P.; Ibrahim, S.F. Does Limb Proprioception Drift? Exp. Brain Res. 1992, 91, 162–166. [Google Scholar] [CrossRef]
- Gault, R.H. Touch as a Substitute for Hearing in the Interpretation and Control of Speech. Arch. Otolaryngol.–Head Neck Surg. 1926, 3, 121–135. [Google Scholar] [CrossRef]
- White, B.W.; Saunders, F.A.; Scadden, L.; Bach-Y-Rita, P.; Collins, C.C. Seeing with the Skin. Percept. Psychophys. 1970, 7, 23–27. [Google Scholar] [CrossRef] [Green Version]
- Bach-Y-Rita, P.; Collins, C.C.; Saunders, F.A.; White, B.; Scadden, L. Vision Substitution by Tactile Image Projection. Nature 1969, 221, 963–964. [Google Scholar] [CrossRef] [PubMed]
- Bach-y-Rita, P.; Kercel, W.S. Sensory Substitution and the Human–Machine Interface. Trends. Cogn. Sci. 2003, 7, 541–546. [Google Scholar] [CrossRef]
- Danilov, Y.; Tyler, M. BrainPort: An Alternative Input to the Brain. J. Integr. Neurosci. 2005, 04, 537–550. [Google Scholar] [CrossRef]
- Lee, B.-C.; Kim, J.; Chen, S.; Sienko, K.H. Cell Phone Based Balance Trainer. J. Neuroeng. Rehabil. 2012, 9, 10. [Google Scholar] [CrossRef] [Green Version]
- Witteveen, H.J.; Rietman, H.S.; Veltink, P.H. Vibrotactile Grasping Force and Hand Aperture Feedback for Myoelectric Forearm Prosthesis Users. Prosthet. Orthot. Int. 2015, 39, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Nesbitt, K. V Designing Multi-Sensory Displays for Abstract Data. Ph.D. Thesis, University of Sydney Australia, Sydney, Australia, 2003. [Google Scholar]
- Tannert, I.; Schulleri, K.H.; Michel, Y.; Villa, S.; Johannsen, L.; Hermsdorfer, J.; Lee, D. Immediate Effects of Vibrotactile Biofeedback Instructions on Human Postural Control. In Proceedings of the 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Guadalajara, Mexico, 1–5 November 2021; IEEE: Piscataway, NJ, USA, 2021; pp. 7426–7432. [Google Scholar]
- Sigrist, R.; Rauter, G.; Riener, R.; Wolf, P. Augmented Visual, Auditory, Haptic, and Multimodal Feedback in Motor Learning: A Review. Psychon. Bull. Rev. 2013, 20, 21–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Priplata, A.; Niemi, J.; Salen, M.; Harry, J.; Lipsitz, L.A.; Collins, J.J. Noise-Enhanced Human Balance Control. Phys. Rev. Lett. 2002, 89, 238101. [Google Scholar] [CrossRef] [PubMed]
- Conrad, M.O.; Gadhoke, B.; Scheidt, R.A.; Schmit, B.D. Effect of Tendon Vibration on Hemiparetic Arm Stability in Unstable Workspaces. PLoS ONE 2015, 10, e0144377. [Google Scholar] [CrossRef] [PubMed]
- Brewster, S.A.; Brown, L.M. Tactons: Structured Tactile Messages for Non-Visual Information Display. In Proceedings of the Australasian User Interface Conference, Dunedin, New Zealand, 18–22 January 2004. [Google Scholar]
- Sklar, A.E.; Sarter, N.B. Good Vibrations: Tactile Feedback in Support of Attention Allocation and Human-Automation Coordination in Event-Driven Domains. Hum. Factors J. Hum. Factors Ergon. Soc. 1999, 41, 543–552. [Google Scholar] [CrossRef]
- Cuppone, A.; Squeri, V.; Semprini, M.; Konczak, J. Robot-Assisted Training to Improve Proprioception Does Benefit from Added Vibro-Tactile Feedback. In Proceedings of the 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 258–261. [Google Scholar]
- Cuppone, A.V.; Semprini, M.; Konczak, J. Consolidation of Human Somatosensory Memory during Motor Learning. Behav. Brain Res. 2018, 347, 184–192. [Google Scholar] [CrossRef]
- Rinderknecht, M.D.; Kim, Y.; Santos-Carreras, L.; Bleuler, H.; Gassert, R. Combined Tendon Vibration and Virtual Reality for Post-Stroke Hand Rehabilitation. In Proceedings of the 2013 World Haptics Conference (WHC), Daejeon, Republic of Korea, 4–17 April 2013; IEEE: Piscataway, NJ, USA, 2013; pp. 277–282. [Google Scholar]
- Tzorakoleftherakis, E.; Murphey, T.D.; Scheidt, R.A. Augmenting Sensorimotor Control Using “Goal-Aware” Vibrotactile Stimulation during Reaching and Manipulation Behaviors. Exp. Brain Res. 2016, 234, 2403–2414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stepp, C.E.; Matsuoka, Y. Relative to Direct Haptic Feedback, Remote Vibrotactile Feedback Improves but Slows Object Manipulation. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010; IEEE: Piscataway, NJ, USA, 2010; pp. 2089–2092. [Google Scholar]
- Kärcher, S.M.; Fenzlaff, S.; Hartmann, D.; Nagel, S.K.; König, P. Sensory Augmentation for the Blind. Front. Hum. Neurosci. 2012, 6, 37. [Google Scholar] [CrossRef] [Green Version]
- Muijzer-Witteveen, H.; Sibum, N.; van Dijsseldonk, R.; Keijsers, N.; van Asseldonk, E. Questionnaire Results of User Experiences with Wearable Exoskeletons and Their Preferences for Sensory Feedback. J. Neuroeng. Rehabil. 2018, 15, 112. [Google Scholar] [CrossRef]
- Goeke, C.M.; Planera, S.; Finger, H.; König, P. Bayesian Alternation during Tactile Augmentation. Front. Behav. Neurosci. 2016, 10, 187. [Google Scholar] [CrossRef] [Green Version]
- Vuori, H. PATIENT SATISFACTION--DOES IT MATTER? Int. J. Qual. Health Care 1991, 3, 183–189. [Google Scholar] [CrossRef]
- Zastowny, T.R.; Roghmann, K.J.; Cafferata, G.L. Patient Satisfaction and the Use of Health Services Explorations in Causality. Med. Care 1989, 27, 705–723. [Google Scholar] [CrossRef] [PubMed]
- Mullan, E.; Markland, D.; Ingledew, D.K. A Graded Conceptualisation of Self-Determination in the Regulation of Exercise Behaviour: Development of a Measure Using Confirmatory Factor Analytic Procedures. Pers. Individ. Dif. 1997, 23, 745–752. [Google Scholar] [CrossRef]
- Vallerand, R.J.; Blssonnette, R. Intrinsic, Extrinsic, and Amotivational Styles as Predictors of Behavior: A Prospective Study. J. Pers. 1992, 60, 599–620. [Google Scholar] [CrossRef]
- Vallerand, R.J. Intrinsic and Extrinsic Motivation in Sport and Physical Activity: A Review and a Look at the Future. In Handbook of Sport Psychology; Wiley: Hoboken, NJ, USA, 2007; pp. 59–83. [Google Scholar]
- Tang, F.; McMahan, R.P.; Allen, T.T. Development of a Low-Cost Tactile Sleeve for Autism Intervention. In Proceedings of the 2014 IEEE International Symposium on Haptic, Audio and Visual Environments and Games (HAVE) Proceedings, Richardson, TX, USA, 10–11 October 2014; IEEE: Piscataway, NJ, USA, 2014; pp. 35–40. [Google Scholar]
- Verrillo, R.T. Age Related Changes in the Sensitivity to Vibration. J. Gerontol. 1980, 35, 185–193. [Google Scholar] [CrossRef]
- Pomplun, E.; Thomas, A.; Corrigan, E.; Shah, V.A.; Mrotek, L.A.; Scheidt, R.A. Vibrotactile Perception for Sensorimotor Augmentation: Perceptual Discrimination of Vibrotactile Stimuli Induced by Low-Cost Eccentric Rotating Mass Motors at Different Body Locations in Young, Middle-Aged, and Older Adults. Front. Rehabil. Sci. 2022, 3, 895036. [Google Scholar] [CrossRef] [PubMed]
- Verrillo, R.T. Vibration Sensation in Humans. Music Percept. 1992, 9, 281–302. [Google Scholar] [CrossRef]
- Carson, R.G.; Kelso, J.A.S. Governing Coordination: Behavioural Principles and Neural Correlates. Exp. Brain Res. 2004, 154, 267–274. [Google Scholar] [CrossRef]
- Huang, J.; Sheffield, B.; Lin, P.; Zeng, F.-G. Electro-Tactile Stimulation Enhances Cochlear Implant Speech Recognition in Noise. Sci. Rep. 2017, 7, 2196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sullivan, J.L.; Dunkelberger, N.; Bradley, J.; Young, J.; Israr, A.; Lau, F.; Klumb, K.; Abnousi, F.; O’Malley, M.K. Multi-Sensory Stimuli Improve Distinguishability of Cutaneous Haptic Cues. IEEE Trans. Haptics 2020, 13, 286–297. [Google Scholar] [CrossRef]






| Interest & Enjoyment | Perceived Competence * | Effort & Importance | Pressure & Tension | Value & Usefulness | |
|---|---|---|---|---|---|
| CEE | 4.2 ± 1.2 | 3.7 ± 1.5 | 5.5 ± 0.9 | 2.6 ± 1.1 | 5.3 ± 1.1 |
| JAE | 4.1 ± 1.3 | 2.5 ± 1.0 | 5.7 ± 0.9 | 3.0 ± 1.2 | 4.6 ± 1.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rayes, R.K.; Mazorow, R.N.; Mrotek, L.A.; Scheidt, R.A. Utility and Usability of Two Forms of Supplemental Vibrotactile Kinesthetic Feedback for Enhancing Movement Accuracy and Efficiency in Goal-Directed Reaching. Sensors 2023, 23, 5455. https://0-doi-org.brum.beds.ac.uk/10.3390/s23125455
Rayes RK, Mazorow RN, Mrotek LA, Scheidt RA. Utility and Usability of Two Forms of Supplemental Vibrotactile Kinesthetic Feedback for Enhancing Movement Accuracy and Efficiency in Goal-Directed Reaching. Sensors. 2023; 23(12):5455. https://0-doi-org.brum.beds.ac.uk/10.3390/s23125455
Chicago/Turabian StyleRayes, Ramsey K., Rachel N. Mazorow, Leigh A. Mrotek, and Robert A. Scheidt. 2023. "Utility and Usability of Two Forms of Supplemental Vibrotactile Kinesthetic Feedback for Enhancing Movement Accuracy and Efficiency in Goal-Directed Reaching" Sensors 23, no. 12: 5455. https://0-doi-org.brum.beds.ac.uk/10.3390/s23125455