
Detecting Minor Symptoms of Parkinson’s Disease in the Wild Using Bi-LSTM with Attention Mechanism

 , ,
, ,
Abstract
:1. Introduction
2. Literature Review: Deep Learning for Parkinson’s Disease Identification Based on Upper Limb Motion Data
2.1. Artificial Neural Networks
2.2. Convolutional Neural Networks
2.3. Long Short-Term Memory
2.4. Hybrid Deep Learning Architectures
2.5. Limitations in Previous Studies, Addressed in the Present Study
3. Methodology
3.1. Dataset Description
3.2. Data Preprocessing
3.3. Windowing and Feature Extraction
3.4. Implementation of Bidirectional LSTM with Attention
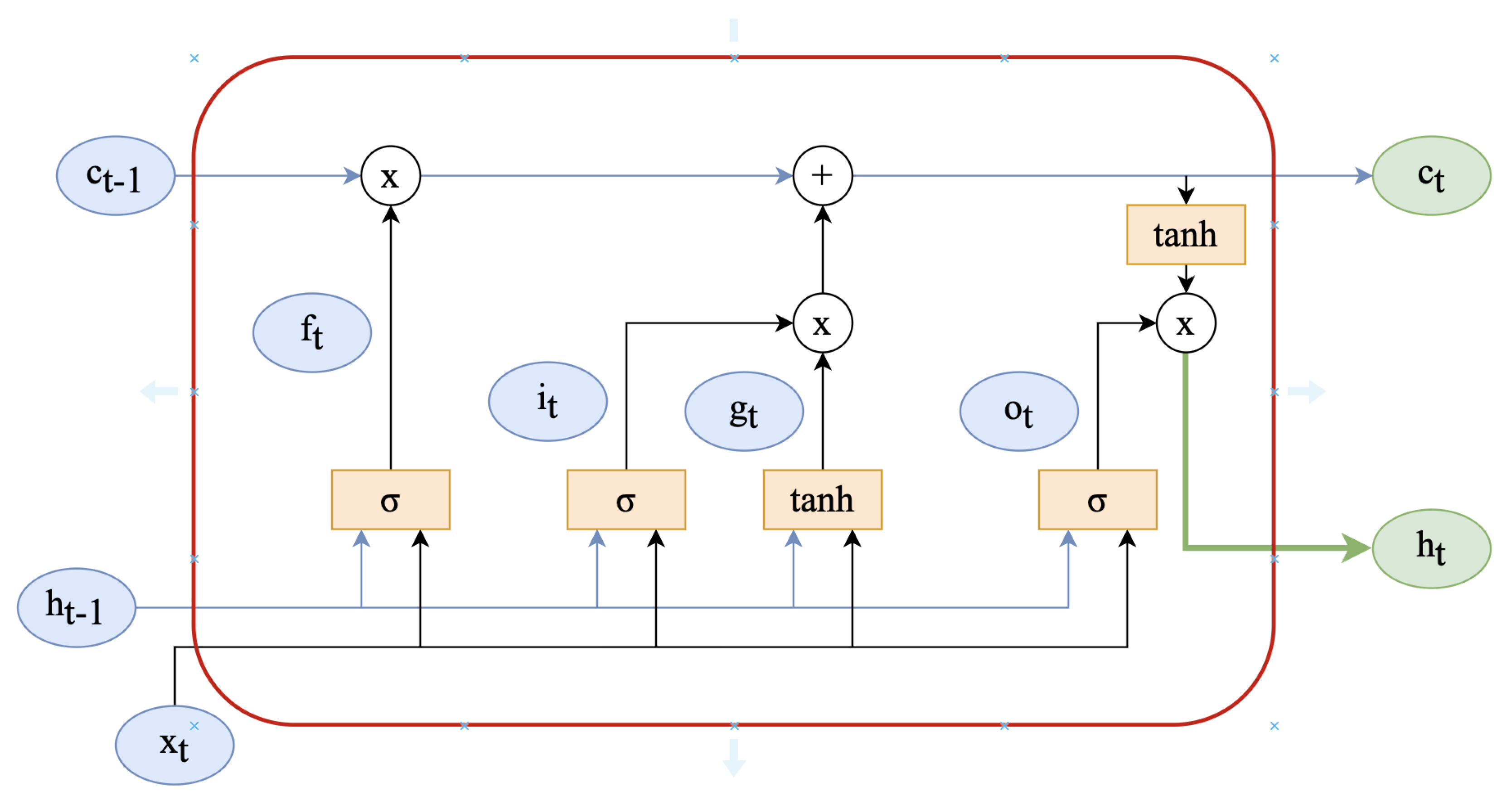
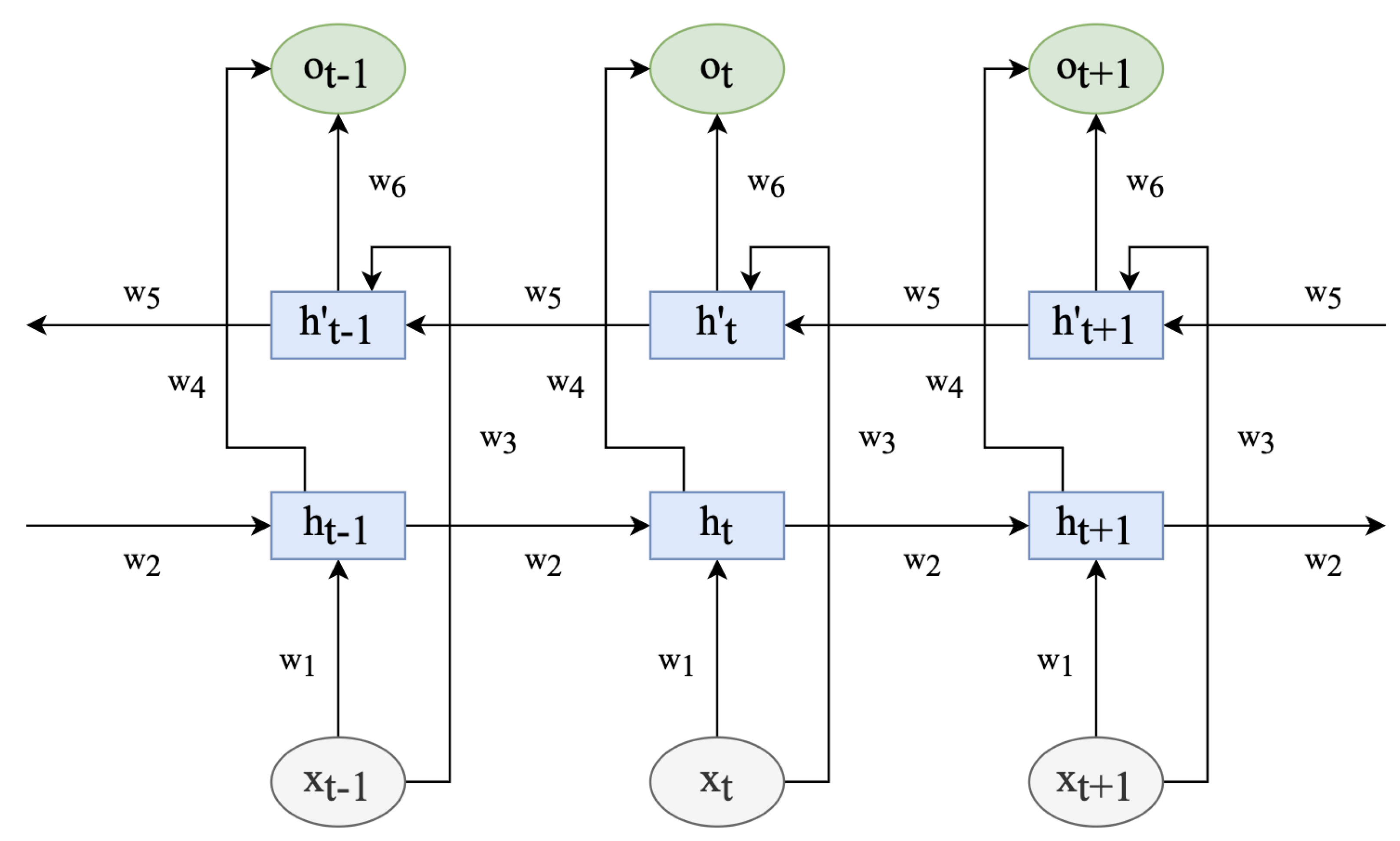
3.4.1. Bidirectional LSTM Layer
3.4.2. Attention Layer
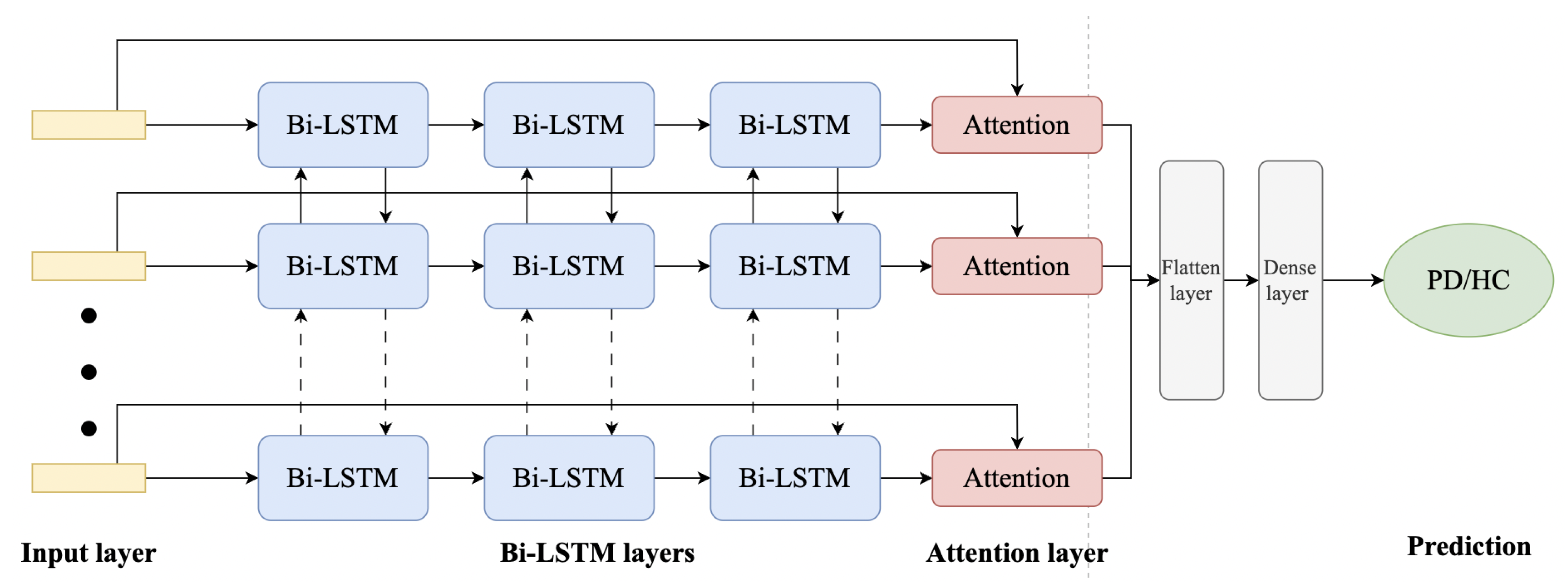
3.4.3. Network Architecture
3.4.4. Experimental Setup and Implementation
4. Results
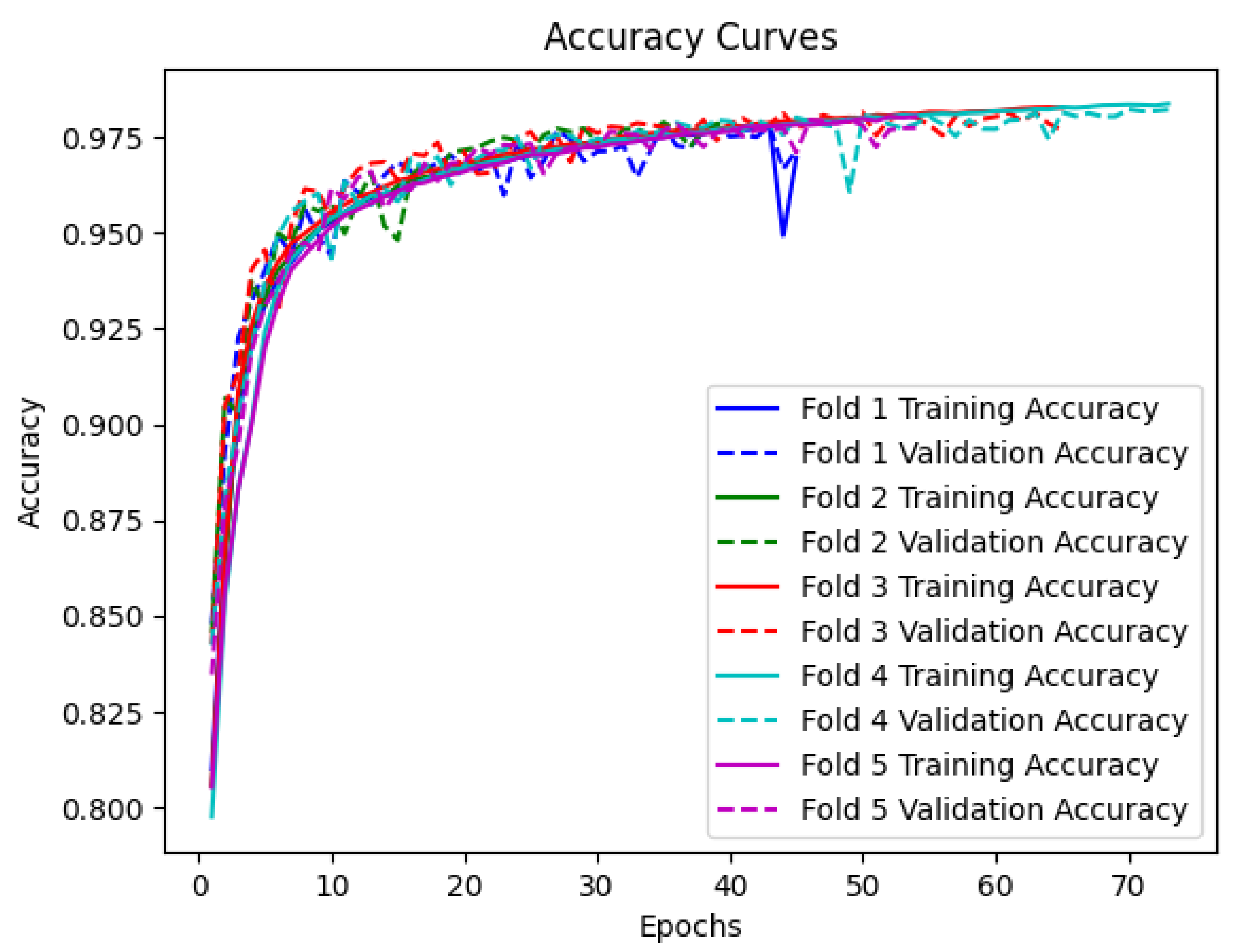
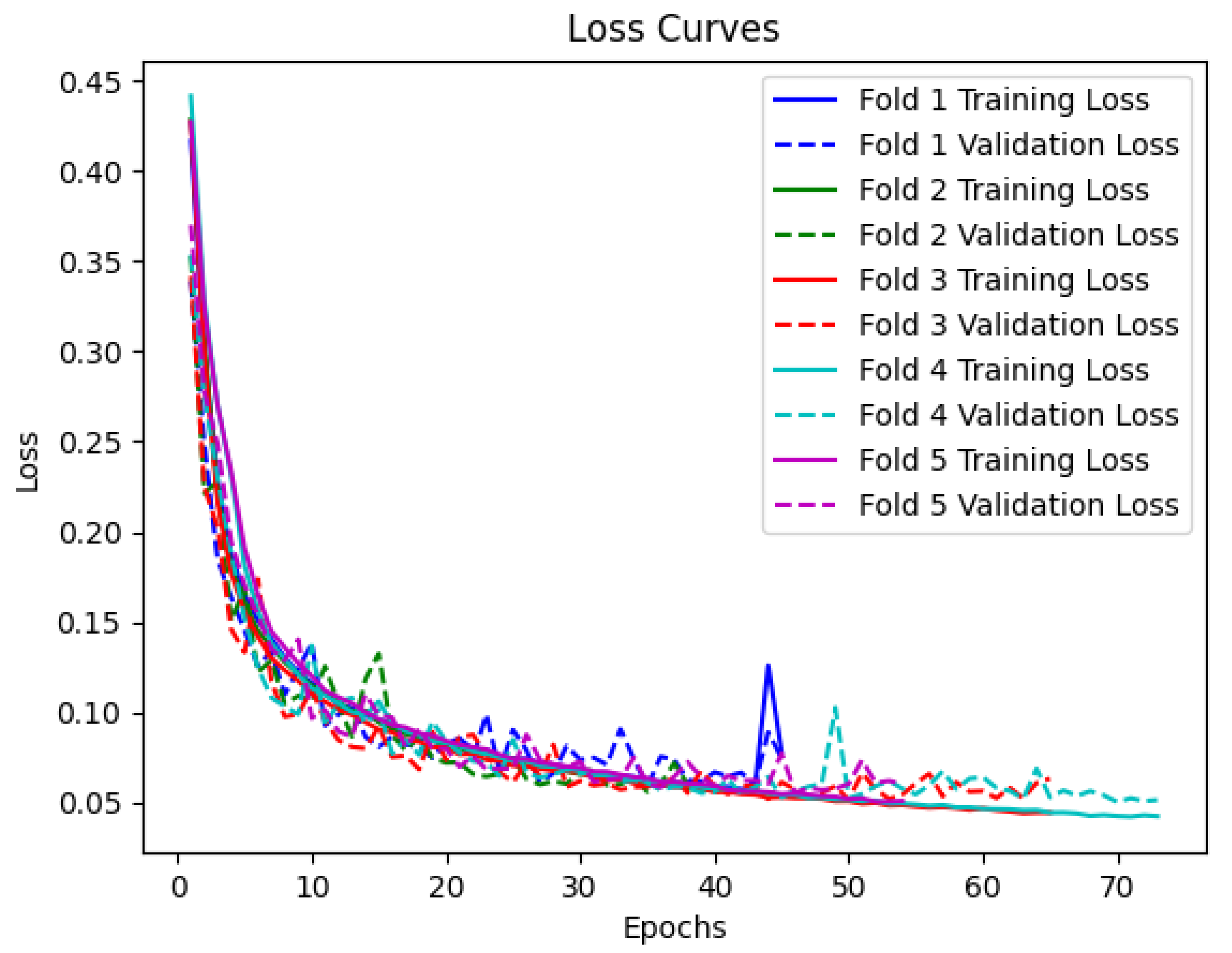
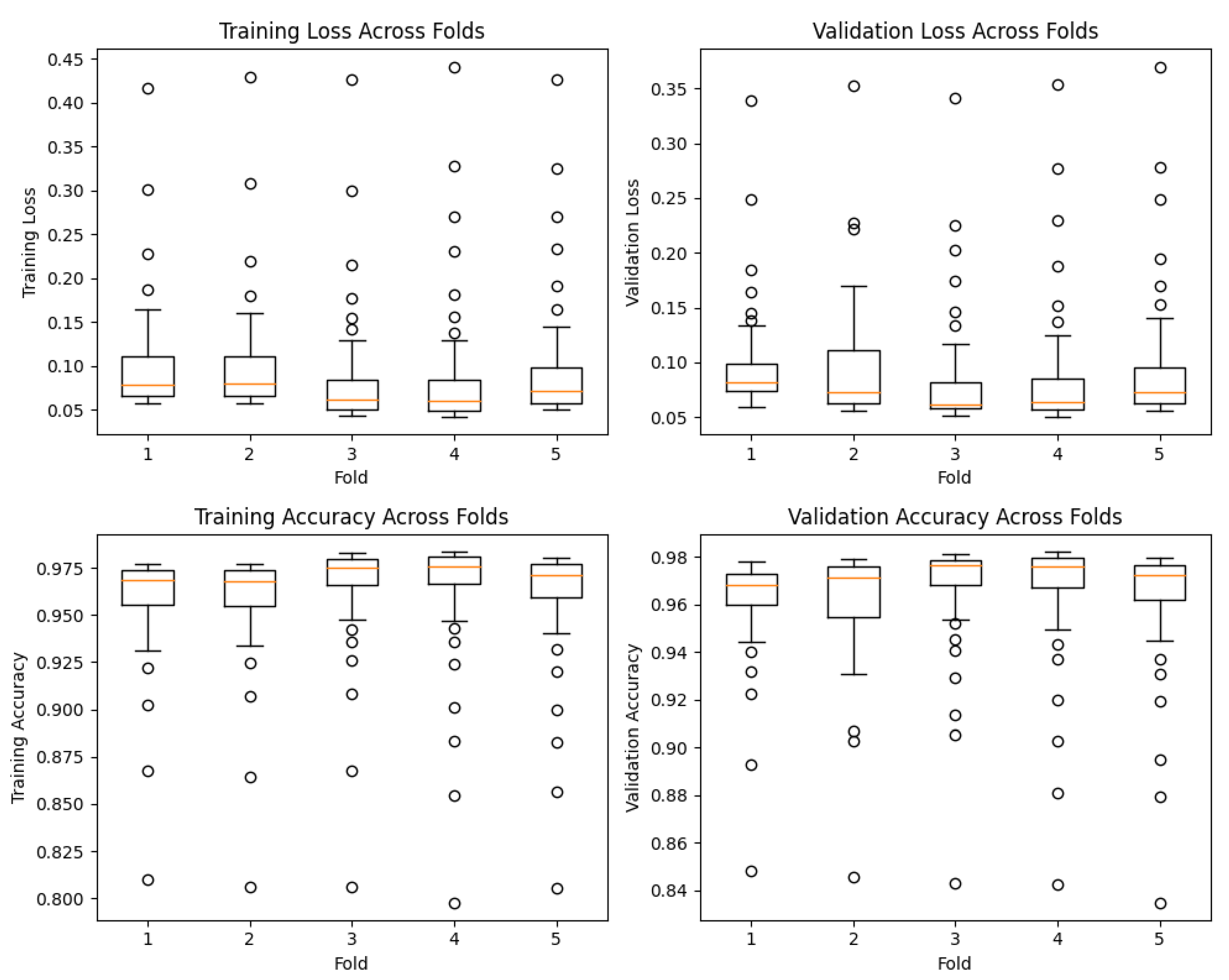
4.1. Training and Validation
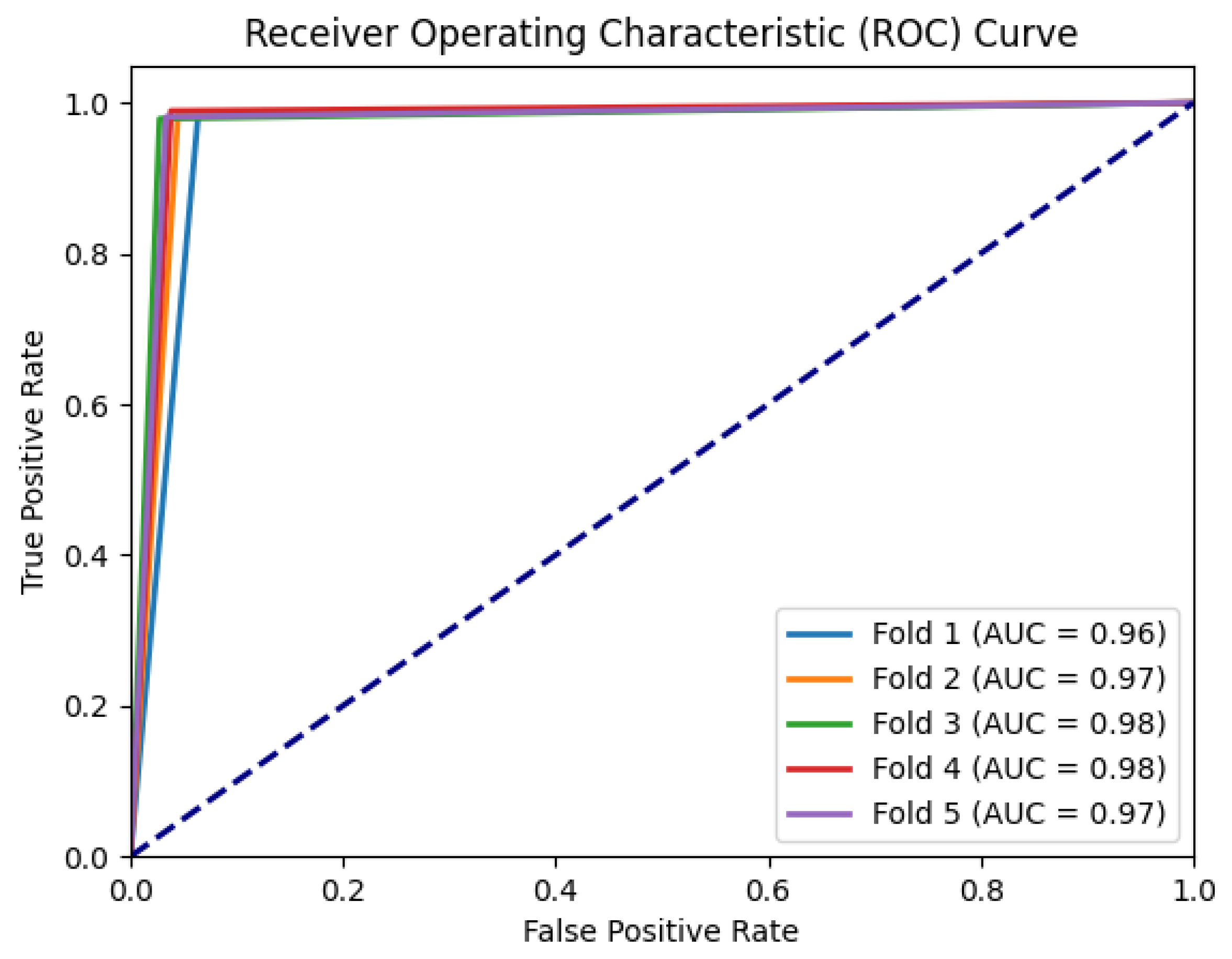
4.2. Performance Evaluation on the Test Set
4.3. An Additional Experiment with a Subset of the Dataset
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PD | Parkinson’s disease |
| HC | Healthy control |
| ML | Machine learning |
| DL | Deep learning |
| AI | Artificial intelligence |
| Bi-LSTM | Bidirectional long short-term memory |
| CNN | Convolutional neural network |
| DNN | Deep neural network |
| RNN | Recurrent neural network |
| ANN | Artificial neural network |
| IQR | Interquartile range |
| AUC | Area under the curve |
| ROC | Receiving operating characteristic |
References
- Parkinson Disease; World Health Organization: Geneva, Switzerland, 2023; Available online: https://www.who.int/news-room/fact-sheets/detail/parkinson-disease (accessed on 9 August 2023).
- Rossi, A.; Berger, K.; Chen, H.; Leslie, D.; Mailman, R.B.; Huang, X. Projection of the prevalence of Parkinson’s disease in the coming decades: Revisited. Mov. Disord. Off. J. Mov. Disord. Soc. 2018, 33, 156–159. [Google Scholar] [CrossRef] [PubMed]
- Lubomski, M.; Davis, R.L.; Sue, C.M. Health-related quality of life for parkinson’s disease patients and their caregivers. J. Mov. Disord. 2021, 14, 42–52. [Google Scholar] [CrossRef] [PubMed]
- Duncan, G.W.; Khoo, T.K.; Yarnall, A.J.; O’Brien, J.T.; Coleman, S.Y.; Brooks, D.J.; Barker, R.A.; Burn, D.J. Health-related quality of life in early Parkinson’s disease: The impact of nonmotor symptoms. Mov. Disord. Off. J. Mov. Disord. Soc. 2014, 29, 195–202. [Google Scholar] [CrossRef]
- Dorsey, E.R.; Elbaz, A.; Nichols, E.; Abbasi, N.; Abd-Allah, F.; Abdelalim, A.; Adsuar, J.C.; Ansha, M.G.; Brayne, C.; Choi, J.Y.J.; et al. Global, regional, and national burden of Parkinson’s disease, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 939–953. [Google Scholar] [CrossRef]
- Titova, N.; Chaudhuri, K.R. Personalized medicine and nonmotor symptoms in parkinson’s disease. Int. Rev. Neurobiol. 2017, 134, 1257–1281. [Google Scholar] [CrossRef]
- Armstrong, M.J.; Okun, M.S. Diagnosis and treatment of parkinson disease: A review. JAMA 2020, 323, 548–560. [Google Scholar] [CrossRef]
- Ntetsika, T.; Papathoma, P.E.; Markaki, I. Novel targeted therapies for Parkinson’s disease. Mol. Med. 2021, 27, 17. [Google Scholar] [CrossRef]
- Ye, H.; Robak, L.A.; Yu, M.; Cykowski, M.; Shulman, J.M. Genetics and pathogenesis of parkinson’s syndrome. Annu. Rev. Pathol. 2023, 18, 95–121. [Google Scholar] [CrossRef]
- Emamzadeh, F.N.; Surguchov, A. Parkinson’s disease: Biomarkers, treatment, and risk factors. Front. Neurosci. 2018, 12, 612. [Google Scholar] [CrossRef]
- Straccia, G.; Colucci, F.; Eleopra, R.; Cilia, R. Precision medicine in parkinson’s disease: From genetic risk signals to personalized therapy. Brain Sci. 2022, 12, 1308. [Google Scholar] [CrossRef]
- Noyce, A.J.; Lees, A.J.; Schrag, A.E. The prediagnostic phase of Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2016, 87, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Bloem, B.R.; Okun, M.S.; Klein, C. Parkinson’s disease. Lancet 2021, 397, 2284–2303. [Google Scholar] [CrossRef]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS clinical diagnostic criteria for Parkinson’s disease: MDS-PD Clinical Diagnostic Criteria. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef]
- Sauerbier, A.; Jenner, P.; Todorova, A.; Chaudhuri, K.R. Non motor subtypes and Parkinson’s disease. Park. Relat. Disord. 2016, 22 (Suppl. S1), S41–S46. [Google Scholar] [CrossRef] [PubMed]
- Tolosa, E.; Garrido, A.; Scholz, S.W.; Poewe, W. Challenges in the diagnosis of Parkinson’s disease. Lancet Neurol. 2021, 20, 385–397. [Google Scholar] [CrossRef]
- Pasquini, J.; Ceravolo, R.; Qamhawi, Z.; Lee, J.Y.; Deuschl, G.; Brooks, D.J.; Bonuccelli, U.; Pavese, N. Progression of tremor in early stages of Parkinson’s disease: A clinical and neuroimaging study. Brain J. Neurol. 2018, 141, 811–821. [Google Scholar] [CrossRef]
- Dirkx, M.F.; Zach, H.; Bloem, B.R.; Hallett, M.; Helmich, R.C. The nature of postural tremor in Parkinson disease. Neurology 2018, 90, e1095–e1103. [Google Scholar] [CrossRef]
- de Lau, L.M.L.; Koudstaal, P.J.; Hofman, A.; Breteler, M.M.B. Subjective complaints precede Parkinson disease: The rotterdam study. Arch. Neurol. 2006, 63, 362–365. [Google Scholar] [CrossRef] [PubMed]
- Marras, C.; Schüle, B.; Munhoz, R.P.; Rogaeva, E.; Langston, J.W.; Kasten, M.; Meaney, C.; Klein, C.; Wadia, P.M.; Lim, S.Y.; et al. Phenotype in parkinsonian and nonparkinsonian LRRK2 G2019S mutation carriers. Neurology 2011, 77, 325–333. [Google Scholar] [CrossRef]
- Skaramagkas, V.; Pentari, A.; Kefalopoulou, Z.; Tsiknakis, M. Multi-modal deep learning diagnosis of parkinson’s disease—A systematic review. IEEE Trans. Neural Syst. Rehabil. Eng. 2023, 31, 2399–2423. [Google Scholar] [CrossRef]
- Yang, Y.; Yuan, Y.; Zhang, G.; Wang, H.; Chen, Y.C.; Liu, Y.; Tarolli, C.G.; Crepeau, D.; Bukartyk, J.; Junna, M.R.; et al. Artificial intelligence-enabled detection and assessment of Parkinson’s disease using nocturnal breathing signals. Nat. Med. 2022, 28, 2207–2215. [Google Scholar] [CrossRef] [PubMed]
- Tsakanikas, V.; Ntanis, A.; Rigas, G.; Androutsos, C.; Boucharas, D.; Tachos, N.; Skaramagkas, V.; Chatzaki, C.; Kefalopoulou, Z.; Tsiknakis, M.; et al. Evaluating gait impairment in parkinson’s disease from instrumented insole and imu sensor data. Sensors 2023, 23, 3902. [Google Scholar] [CrossRef] [PubMed]
- Chatzaki, C.; Skaramagkas, V.; Tachos, N.; Christodoulakis, G.; Maniadi, E.; Kefalopoulou, Z.; Fotiadis, D.I.; Tsiknakis, M. The Smart-Insole Dataset: Gait Analysis Using Wearable Sensors with a Focus on Elderly and Parkinson’s Patients. Sensors 2021, 21, 2821. [Google Scholar] [CrossRef] [PubMed]
- Skaramagkas, V.; Andrikopoulos, G.; Kefalopoulou, Z.; Polychronopoulos, P. Towards differential diagnosis of essential and parkinson’s tremor via machine learning. In Proceedings of the 2020 28th Mediterranean Conference on Control and Automation, MED 2020, Saint-Raphaël, France, 16–19 June 2020; pp. 782–787. [Google Scholar] [CrossRef]
- Goschenhofer,, J.; Pfister, F.M.; Yuksel, K.A.; Bischl, B.; Fietzek, U.; Thomas, J. Wearable-based Parkinson’s Disease Severity Monitoring using Deep Learning. In Lecture Notes in Computer Science; Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics; Springer: Berlin/Heidelberg, Germany, 2019; pp. 400–415. [Google Scholar]
- Kefalopoulou, Z.; Chatzaki, C.; Skaramagkas, V.; Chroni, E.; Tachos, N.; Fotiadis, D.; Tsiknakis, M. Pressure Sensor Insole Gait Assessment for Parkinson’s Disease patients: A pilot study. In Movement Disorders; Wiley: Hoboken, NJ, USA, 2022; Volume 37, p. S193. [Google Scholar]
- Chatzaki, C.; Skaramagkas, V.; Kefalopoulou, Z.; Tachos, N.; Kostikis, N.; Kanellos, F.; Triantafyllou, E.; Chroni, E.; Fotiadis, D.I.; Tsiknakis, M. Can Gait Features Help in Differentiating Parkinson’s Disease Medication States and Severity Levels? A Machine Learning Approach. Sensors 2022, 22, 9937. [Google Scholar] [CrossRef]
- Skaramagkas, V.; Andrikopoulos, G.; Kefalopoulou, Z.; Polychronopoulos, P. A Study on the Essential and Parkinson’s Arm Tremor Classification. Signals 2021, 2, 201–224. [Google Scholar] [CrossRef]
- Lu, M.; Zhao, Q.; Poston, K.L.; Sullivan, E.V.; Pfefferbaum, A.; Shahid, M.; Katz, M.; Kouhsari, L.M.; Schulman, K.; Milstein, A.; et al. Quantifying Parkinson’s disease motor severity under uncertainty using MDS-UPDRS videos. Med. Image Anal. 2021, 73, 102179. [Google Scholar] [CrossRef]
- Tsakanikas, V.D.; Dimopoulos, D.G.; Tachos, N.S.; Chatzaki, C.; Skaramagkas, V.; Christodoulakis, G.; Tsiknakis, M.; Fotiadis, D.I. Gait and balance patterns related to Free-Walking and TUG tests in Parkinson’s Disease based on plantar pressure data. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Virtual, 1–5 November 2021; pp. 236–239. [Google Scholar] [CrossRef]
- Rajkomar, A.; Dean, J.; Kohane, I. Machine learning in medicine. N. Engl. J. Med. 2019, 380, 1347–1358. [Google Scholar] [CrossRef]
- Fraiwan, L.; Khnouf, R.; Mashagbeh, A.R. Parkinson’s disease hand tremor detection system for mobile application. J. Med. Eng. Technol. 2016, 40, 127–134. [Google Scholar] [CrossRef]
- Castrillón, R.; Acien, A.; Orozco-Arroyave, J.R.; Morales, A.; Vargas-Bonilla, J.F.; Vera-Rodríguez, R.; Fierrez, J.; Ortega-Garcia, J.; Villegas, A. Characterization of the Handwriting Skills as a Biomarker for Parkinson’s Disease. In Proceedings of the 2019 14th IEEE International Conference on Automatic Face & Gesture Recognition (FG 2019), Lille, France, 14–18 May 2019; pp. 1–5. [Google Scholar]
- Bazgir, O.; Frounchi, J.; Habibi, S.A.H.; Palma, L.; Pierleoni, P. A neural network system for diagnosis and assessment of tremor in Parkinson disease patients. In Proceedings of the 2015 22nd Iranian Conference on Biomedical Engineering, ICBME, Tehran, Iran, 25–27 November 2015; pp. 1–5. [Google Scholar] [CrossRef]
- Wu, H.; Zhang, Y.; Wu, X.; Yang, F. Assessment of Upper Limb Tremors in Patients with Parkinson’s Disease Based on Displacement and Acceleration Information. In Proceedings of the 5th International Conference on Automation, Control and Robotics Engineering, CACRE 2020, Dalian, China, 19–20 September 2020; pp. 177–182. [Google Scholar] [CrossRef]
- Lekadir, K.; Osuala, R.; Gallin, C.; Lazrak, N.; Kushibar, K.; Tsakou, G.; Aussó, S.; Alberich, L.C.; Marias, K.; Tsiknakis, M.; et al. Future-ai: Guiding principles and consensus recommendations for trustworthy artificial intelligence in medical imaging. arXiv 2021, arXiv:2109.09658. [Google Scholar] [CrossRef]
- Xing, X.; Luo, N.; Li, S.; Zhou, L.; Song, C.; Liu, J. Identification and Classification of Parkinsonian and Essential Tremors for Diagnosis Using Machine Learning Algorithms. Front. Neurosci. 2022, 16, 701632. [Google Scholar] [CrossRef]
- Tong, L.; He, J.; Peng, L. CNN-Based PD Hand Tremor Detection Using Inertial Sensors. IEEE Sens. Lett. 2021, 5, 7002504. [Google Scholar] [CrossRef]
- Sun, M.; Watson, A.; Blackwell, G.; Jung, W.; Wang, S.; Koltermann, K.; Helm, N.; Zhou, G.; Cloud, L.; Pretzer-Aboff, I. TremorSense: Tremor Detection for Parkinson’s Disease Using Convolutional Neural Network. In Proceedings of the 2021 IEEE/ACM Conference on Connected Health: Applications, Systems and Engineering Technologies, CHASE 2021, Washington, DC, USA, 16–17 December 2021; pp. 1–10. [Google Scholar] [CrossRef]
- Folador, J.P.; Santos, M.C.S.; Luiz, L.M.D.; de Souza, L.A.P.S.; Vieira, M.F.; Pereira, A.A.; de Oliveira Andrade, A. On the use of histograms of oriented gradients for tremor detection from sinusoidal and spiral handwritten drawings of people with Parkinson’s disease. Med. Biol. Eng. Comput. 2021, 59, 195–214. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.B.; Lee, W.W.; Kim, A.; Lee, H.J.; Park, H.Y.; Jeon, H.S.; Kim, S.K.; Jeon, B.; Park, K.S. Wrist sensor-based tremor severity quantification in Parkinson’s disease using convolutional neural network. Comput. Biol. Med. 2018, 95, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Kaushik, S.; Choudhury, A.; Sheron, P.K.; Dasgupta, N.; Natarajan, S.; Pickett, L.A.; Dutt, V. AI in healthcare: Time-series forecasting using statistical, neural, and ensemble architectures. Front. Big Data 2020, 3, 4. [Google Scholar] [CrossRef] [PubMed]
- Absar, N.; Uddin, N.; Khandaker, M.U.; Ullah, H. The efficacy of deep learning based LSTM model in forecasting the outbreak of contagious diseases. Infect. Dis. Model. 2021, 7, 170–183. [Google Scholar] [CrossRef]
- Thummikarat, H.; Chongstitvatana, P. An implementation of machine learning for parkinson’s disease diagnosis. In Proceedings of the ECTI-CON 2021—2021 18th International Conference on Electrical Engineering/Electronics, Computer, Telecommunications and Information Technology: Smart Electrical System and Technology, Virtual, 19–22 May 2021; pp. 258–261. [Google Scholar] [CrossRef]
- A V, A.S.; Lones, M.A.; Smith, S.L.; Vallejo, M. Evaluation of Recurrent Neural Network Models for Parkinson’s Disease Classification Using Drawing Data. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Virtual, 1–5 November 2021; pp. 1702–1706. [Google Scholar] [CrossRef]
- Hssayeni, M.D.; Jimenez-Shahed, J.; Burack, M.A.; Ghoraani, B. Wearable Sensors for Estimation of Parkinsonian Tremor Severity during Free Body Movements. Sensors 2019, 19, 4215. [Google Scholar] [CrossRef] [PubMed]
- Hathaliya, J.J.; Modi, H.; Gupta, R.; Tanwar, S. Deep learning and Blockchain-based Essential and Parkinson Tremor Classification Scheme. In Proceedings of the IEEE INFOCOM 2022—IEEE Conference on Computer Communications Workshops (INFOCOM WKSHPS), Virtual, 2–5 May 2022; pp. 1–6. [Google Scholar] [CrossRef]
- Shahtalebi, S.; Atashzar, S.F.; Patel, R.V.; Jog, M.S.; Mohammadi, A. A deep explainable artificial intelligent framework for neurological disorders discrimination. Sci. Rep. 2021, 11, 9630. [Google Scholar] [CrossRef]
- Taleb, C.; Likforman-Sulem, L.; Mokbel, C.; Khachab, M. Detection of Parkinson’s disease from handwriting using deep learning: A comparative study. Evol. Intell. 2020, 1–12. [Google Scholar] [CrossRef]
- Taleb, C.; Khachab, M.; Mokbel, C.; Likforman-Sulem, L. Feature selection for an improved Parkinson’s disease identification based on handwriting. In Proceedings of the 1st IEEE International Workshop on Arabic Script Analysis and Recognition, ASAR 2017, Nancy, France, 3–5 April 2017; pp. 52–56. [Google Scholar] [CrossRef]
- Papadopoulos, A.; Kyritsis, K.; Klingelhoefer, L.; Bostanjopoulou, S.; Chaudhuri, K.R.; Delopoulos, A. Detecting parkinsonian tremor from imu data collected in-the-wild using deep multiple-instance learning. IEEE J. Biomed. Health Inform. 2020, 24, 2559–2569. [Google Scholar] [CrossRef]
- Chan, P.Y.; Ripin, Z.M.; Halim, S.A.; Arifin, W.N.; Yahya, A.S.; Eow, G.B.; Tan, K.; Hor, J.Y.; Wong, C.K. Motion characteristics of subclinical tremors in Parkinson’s disease and normal subjects. Sci. Rep. 2022, 12, 4021. [Google Scholar] [CrossRef]
- Oppenheim, A.; Schafer, R. Discrete-Time Signal Processing: Pearson New International Edition, 3rd ed.; Pearson Education Limited: Harlow, UK, 2013. [Google Scholar]
- Yamansavaşçılar, B.; Güvensan, M.A. Activity recognition on smartphones: Efficient sampling rates and window sizes. In Proceedings of the 2016 IEEE International Conference on Pervasive Computing and Communication Workshops (PerCom Workshops), Sydney, Australia, 14–18 March 2016; pp. 1–6. [Google Scholar] [CrossRef]
- Djordjevic, I. Chapter 3—Quantum circuits and quantum information processing fundamentals. In Quantum Information Processing and Quantum Error Correction; Djordjevic, I., Ed.; Academic Press: Oxford, UK, 2012; pp. 91–117. [Google Scholar] [CrossRef]
- Akandeh, A.; Salem, F.M. Slim lstm networks: Lstm_6 and lstm_c6. In Proceedings of the 2019 IEEE 62nd International Midwest Symposium on Circuits and Systems (MWSCAS), Dallas, TX, USA, 4–7 August 2019; pp. 630–633. [Google Scholar] [CrossRef]
- Siami-Namini, S.; Tavakoli, N.; Namin, A.S. The performance of lstm and bilstm in forecasting time series. In Proceedings of the 2019 IEEE International Conference on Big Data (Big Data), Los Angeles, CA, USA, 9–12 December 2019; pp. 3285–3292. [Google Scholar] [CrossRef]
- Graves, A.; Fernández, S.; Schmidhuber, J. Bidirectional lstm networks for improved phoneme classification and recognition. In Proceedings of the Artificial Neural Networks: Formal Models and Their Applications—ICANN, Warsaw, Poland, 11–15 September 2005; Lecture Notes in Computer Science. Duch, W., Kacprzyk, J., Oja, E., Zadrożny, S., Eds.; Springer: Berlin/Heidelberg, Germany, 2005; pp. 799–804. [Google Scholar] [CrossRef]
- Afendras, G.; Markatou, M. Optimality of training/test size and resampling effectiveness in cross-validation. J. Stat. Plan. Inference 2019, 199, 286–301. [Google Scholar] [CrossRef]
- Papadopoulos, A.; Iakovakis, D.; Klingelhoefer, L.; Bostantjopoulou, S.; Chaudhuri, K.R.; Kyritsis, K.; Hadjidimitriou, S.; Charisis, V.; Hadjileontiadis, L.J.; Delopoulos, A. Unobtrusive detection of Parkinson’s disease from multi-modal and in-the-wild sensor data using deep learning techniques. Sci. Rep. 2020, 10, 21370. [Google Scholar] [CrossRef] [PubMed]
- Habets, J.G.V.; Herff, C.; Kubben, P.L.; Kuijf, M.L.; Temel, Y.; Evers, L.J.W.; Bloem, B.R.; Starr, P.A.; Gilron, R.; Little, S. Rapid dynamic naturalistic monitoring of bradykinesia in parkinson’s disease using a wrist-worn accelerometer. Sensors 2021, 21, 7876. [Google Scholar] [CrossRef]
- Mahadevan, N.; Demanuele, C.; Zhang, H.; Volfson, D.; Ho, B.; Erb, M.K.; Patel, S. Development of digital biomarkers for resting tremor and bradykinesia using a wrist-worn wearable device. npj Digit. Med. 2020, 3, 5. [Google Scholar] [CrossRef] [PubMed]
- Bhidayasiri, R. Differential diagnosis of common tremor syndromes. Postgrad. Med. J. 2005, 81, 756–762. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | Description | Formula |
|---|---|---|
| Maximum | The maximum value in the signal (per axis). | |
| Minimum | The minimum value in the signal (per axis). | |
| Mean | The average value of the signal (per axis). | |
| Standard deviation (std) | A measure of the dispersion or spread of the signal values around the mean (per axis). | |
| Kurtosis | A measure of the peakedness or flatness of the signal’s distribution (per axis). | |
| Zero Crossing Rate | The rate at which the signal changes its sign. | |
| Skewness | A measure of the asymmetry of the signal’s distribution (per axis). | |
| Correlation | The correlation coefficients between different signal components or dimensions (for xy, xz, yz axes). | |
| Maximum PSD | The maximum power spectral density value in the signal. | |
| Average PSD | The average power spectral density value in the signal. | |
| Standard Deviation of PSD | A measure of the variation or spread of the power spectral density values. | |
| Spectral Centroid | The center of mass of the power spectral density distribution, representing the average frequency content of the signal. | |
| Spectral Rolloff | The frequency below which a specified percentage of the total power of the signal is contained. | |
| Spectral Flatness | A measure of the tonality or noisiness of the signal. | |
| Spectral Skewness | A measure of the asymmetry of the power spectral density distribution around its centroid. | |
| Spectral Kurtosis | A measure of the peakedness or flatness of the power spectral density distribution around its centroid. | |
| Entropy | A measure of the randomness or unpredictability of the signal, calculated using Shannon’s entropy formula [56]. | |
| Total Energy | The total energy or power in the signal, calculated as the sum of the squared values. | |
| Signal Magnitude Area | The sum of the absolute values of the signal. |
| Layer | Neurons | Output Shape | Parameters | Activation |
|---|---|---|---|---|
| Input layer | 33 | (-, 33, 1) | 0 | - |
| Bi-LSTM layer 1 | 32 | (-, 33, 64) | 8704 | - |
| Dropout 1 | - | (-, 33, 64) | 0 | - |
| Bi-LSTM layer 2 | 64 | (-, 33, 128) | 66,048 | - |
| Dropout 2 | - | (-, 33, 128) | 0 | - |
| Bi-LSTM layer 3 | 128 | (-, 33, 256) | 263,168 | - |
| Attention layer | - | (-, 33, 256) | 0 | - |
| Dropout 3 | - | (-, 33, 256) | 0 | - |
| Flatten layer | - | (-, 8448) | 0 | - |
| Dense layer | 1 | (-, 1) | 8449 | Sigmoid |
| Model | Experiment | Accuracy | Precision | Recall | Specificity | F1-Score |
|---|---|---|---|---|---|---|
| LSTM [45] | Typing | 0.73 | ||||
| Two-Stacked LSTM [46] | Writing | 0.91 | - | 1.00 | 0.65 | 0.94 |
| CNN-BiLSTM [50] | Writing | 0.98 | - | 0.95 | 1.00 | |
| DNN [33] | Hand poses | 0.95 | - | - | - | - |
| BiLSTM + attention (proposed model) | Talking on the phone | 0.98 | 0.99 | 0.98 | 0.96 | 0.98 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skaramagkas, V.; Boura, I.; Spanaki, C.; Michou, E.; Karamanis, G.; Kefalopoulou, Z.; Tsiknakis, M. Detecting Minor Symptoms of Parkinson’s Disease in the Wild Using Bi-LSTM with Attention Mechanism. Sensors 2023, 23, 7850. https://0-doi-org.brum.beds.ac.uk/10.3390/s23187850
Skaramagkas V, Boura I, Spanaki C, Michou E, Karamanis G, Kefalopoulou Z, Tsiknakis M. Detecting Minor Symptoms of Parkinson’s Disease in the Wild Using Bi-LSTM with Attention Mechanism. Sensors. 2023; 23(18):7850. https://0-doi-org.brum.beds.ac.uk/10.3390/s23187850
Chicago/Turabian StyleSkaramagkas, Vasileios, Iro Boura, Cleanthi Spanaki, Emilia Michou, Georgios Karamanis, Zinovia Kefalopoulou, and Manolis Tsiknakis. 2023. "Detecting Minor Symptoms of Parkinson’s Disease in the Wild Using Bi-LSTM with Attention Mechanism" Sensors 23, no. 18: 7850. https://0-doi-org.brum.beds.ac.uk/10.3390/s23187850