Recent Approaches for Solid Dose Vaccine Delivery
by
 ,
,
Nishat Jahan
1,* ,
,
Sabrina Rahman Archie
2,
Abdullah Al Shoyaib
2,
Nadia Kabir
1 and
Karmen Cheung
3 1
Department of Pharmacy, University of Asia Pacific, Dhaka 1205, Bangladesh
2
Department of Pharmaceutical Technology, University of Dhaka, Dhaka 1000, Bangladesh
3
Department of Chemical Engineering, Loughborough University, Loughborough LE11 3TU, UK
*
Author to whom correspondence should be addressed.
Sci. Pharm. 2019, 87(4), 27; https://0-doi-org.brum.beds.ac.uk/10.3390/scipharm87040027
Submission received: 10 August 2019
/
Revised: 12 September 2019
/
Accepted: 18 September 2019
/
Published: 14 October 2019
(This article belongs to the Special Issue New Insights into Drug Delivery and Absorption)
Abstract
:Recent studies on vaccine delivery systems are exploring the possibility of replacing liquid vaccines with solid dose vaccines due to the many advantages that solid dose vaccines can offer. These include the prospect of a needle-free vaccine delivery system leading to better patient compliance, cold chain storage, less-trained vaccinators and fewer chances for needle stick injury hazards. Some studies also indicate that vaccines in a solid dosage form can result in a higher level of immunogenicity compared to the liquid form, thus providing a dose-sparing effect. This review outlines the different approaches in solid vaccine delivery using various routes of administration including, oral, pulmonary, intranasal, buccal, sublingual, and transdermal routes. The various techniques and their current advancements will provide a knowledge base for future work to be carried out in this arena.
1. Introduction
In 1798 Edward Jenner first demonstrated the idea of vaccination [1], and ever since then, it has become an essential entity of human health protection. Vaccination has provided people respite from various life-threatening diseases, like small pox and tetanus, that used to kill millions of people before the discovery of vaccine. New vaccines are still being investigated for many diseases that are yet unbeatable by today’s medical advancement. There is also a growing demand for a safer, more compatible and cost-effective vaccine delivery system, as vaccine production, preservation and immunisation programmes are extremely expensive. Most vaccines are still being administered parenterally through injection either via intramuscular or subcutaneous routes, which have been proven to initiate effective systemic immunisation [2]. However, recent studies on vaccines suggest that vaccines administered in solid dosage forms have a potential advantage over liquid dosage forms, as they provide a higher level of immunogenicity, thus leading to a dose-sparing effect [3]. Solid dosage forms also have many other advantages over liquid dosage forms in terms of avoiding the need for cold chain storage, less training for vaccinators and a lower cost [4,5]. If these solid dosage forms can be made needle-free this will also minimise the chance of disease transmission from needle-stick injury and increase patient compliance, as it would be pain-free. This review will summarise the current approaches undertaken by several research organisations to successfully develop a solid-dose vaccine delivery system and its potential to exhibit a dose-sparing effect. Additionally, it will explore the various solid vaccine dosage forms that have been designed for the different delivery routes (oral, transdermal, pulmonary, nasal, buccal and sublingual) and compare their limitations and benefits. The benefits, juxtaposed with the drawbacks, will provide researchers and scientists a clear overview for their forthcoming work on vaccine delivery.
1.1. Rationale for Solid Dosage Form of Vaccine
According to the World Health Organization (WHO), the term ‘vaccine’ refers to a biological preparation that improves immunity to a particular disease. It is typically made up of weakened or killed forms of the disease-causing microbe, its toxins or one of its surface proteins, that, when introduced in the body at sufficient amount will elicit immunogenicity, preparing the body for any future invasion by the same organism. Vaccines can be prophylactic (prevent infectious disease; e.g., tetanus or influenza vaccines) or therapeutic (cancer vaccines) [6].
Although vaccines are widely delivered in liquid form using needles, this form of vaccine delivery faces some limitations, like needle-stick injuries, poor patient compliance, cold chain storage and a lack of T-cell mediated immunity and mucosal protection [7]. A solid vaccine delivery system, on the other hand, comes with some inherent advantages, including, no needle-stick injuries, less extensive purification requirement, better patient compliance and improved shelf-life [8]. Additionally, vaccines are thought to show more immunogenicity when delivered in solid form, due to dose-sparing [3]. Due to these advantages, many companies are steering their research towards solid dose vaccine delivery. Vaccine solid dosage forms include the forms of vaccines that are prepared, stored and delivered in the solid state, which can occur either as amorphous powders or as crystals of various morphologic structures, fabricated into different dosage forms, such as various types of tablets, capsules, granules, sachets, reconstitutable powders, powders, dry-powder inhalers, chewables, injectors, microneedles, films and others [9,10]. For example, Vivotif for typhoid [11] and Flumist for influenza [12]. On the other hand, the vaccines which are found in the forms of solutions, suspensions or emulsions, can be termed liquid dose vaccines. For example, Rotarix Vaccine for Rota virus [13].
1.2. Dose-Sparing and Cost-Effectiveness
When the same dose of antigen or a lower dose gives a higher antibody titre, it provides a dose-sparing effect, which, in turn, can make vaccines more cost-effective [14]. Several solid vaccine formulations have been shown to produce dose-sparing effects; for instance, influenza vaccine dry-powder for inhalation has been shown to a produce higher IgG titre compared to the intramuscular liquid influenza vaccine in mice at a same dose of 5 µg surface glycoprotein haemagglutinin (HA). The dry powder might have resulted in increased local viscosity due to dissolution of the powders, leading to reduced mucociliary clearance and higher antigen uptake [15]. This enhanced immunity could also be due to activation of both systemic and mucosal humoral immunity by the inhaled solid vaccine powder [16]. Formation of more doses from the same batch of vaccine is particularly important when vaccine demand increases, such as during a pandemic influenza outbreak [14]. Unforseen events can also cause an increase in demand, such as the loss due to contamination of half of the U.S. supply of influenza vaccine, creating a critical shortage and incomplete vaccine coverage [17]. Various emergency measures were considered to either increase the supply of vaccines by reducing the intramuscular doses or importing doses from manufacturers that do not supply the United States [17]. There is a also a tenency for pharmaceutical companies to invest in a frequently used drug rather than preventive treatments like vaccines due to low profit opportunities from drugs for preventive treatments [18].
1.3. Cold-Chain
The equipment, materials and processes required to ensure the storage of vaccines within the temperature range of (usually) 2 to 8 °C from the time of manufacture until they are administered to subjects, are referred to as ‘cold chain.’ Most vaccines need to be maintained at this temperature to maintain their potency. Vaccines, such as the oral polio vaccine, and the measles, mumps and rubella (MMR) varicella and yellow fever vaccines are heat sensitive, whereas diphtheria and tetanus toxoids, pertussis vaccine and hepatitis B vaccine are sensitive to freezing [19]. Frozen vaccines need to be stored in a freezer between −50 °C and −15 °C [20]. However, maintaining cold storage facilities, cold transportation and cold boxes makes vaccine programs expensive, and hinder the easy and proper distribution of vaccines, especially for the small cities and villages of developing countries. Solid dosage form vaccines, like microneedle patches, have the potential of eliminating the need for cold chain vaccines [14]. Although the currently available lyophilised forms of vaccines that need to be reconstituted before injection are required to be refrigerated, they have relatively better stability than the liquid dosage form; however, it still complicates the vaccine administration process because of the additional reconstitution steps, making the process more time-consuming. Additionally, a vial consisting of water (diluent) needs to be provided for reconstitution, which further adds cost to the overall procedure [14]. Moreover, vaccine tableting circumvents the need for the expensive sterile fill and finishing method that would normally be required by injected vaccines [21].
1.4. Safety
The traditional way of administering vaccines can be associated with a risk of spread of infectious diseases between patients and healthcare providers due to needle-stick injuries, especially in developing countries, or during a bioterrorism emergency or a natural pandemic. Improper use of needles and syringes include use without sterilisation between patients and improper disposal of needles and syringes which may otherwise put the whole community at risk of needle-stick injuries (sharp hazard) [19].
1.5. Compliance
Needles and syringes also result in poor compliance with vaccine schedules due to parental concerns about the number of vaccine administrations, and needle-phobia [19]. The discomfort needles cause can give rise to incomplete vaccination coverage [22]. Although combination vaccines can be used, the immunogenicity is sometimes compromised. Combination vaccines administered mucosally have shown to be effective without compromising immunogenicity of vaccines [19].
1.6. The Training of Vaccinators
Needle-free delivery systems will make it easier for mass vaccination programs to be carried out, as less healthcare training will be required. This will also increase the speed of vaccine delivery [19].
1.7. Rapid Distribution
Solid vaccine dosage forms, for instance as tablets, or releasable solid coatings with microneedle technology [3], will ease the method of distribution. For instance, during the influenza pandemic in 2009, the supply of vaccines was limited, and in Los Angeles County, California, 247 people per hour were in the queue for immunisation, and the rate of immunisation was about 239 people per hour at each distribution point. This indicates that in a city of 9 million people, it would take 60 days to complete the immunisation campaign [21]. However, if vaccine tablets were available (which is undergoing research now), the entire city could have been immunised in one day. And since people would not need to wait in line, it would evade the exposure of individuals to the growing outbreak [21].
2. Types of Solid Dose Vaccine Delivery System
2.1. Mucosal Routes
Currently, most vaccines are administered by means of injection, which includes mainly subcutaneous and intramuscular route. Although this provides sufficient systemic immunity, it fails to induce adequate mucosal immunity, whereas vaccines administered through mucosal routes (oral, intranasal, pulmonary, buccal and sublingual) have been found to be effective for induction of both systemic and local immunity [23]. Mucosal vaccines are able to provide both prophylactic and therapeutic responses against different diseases, and cancer [24]. Additionally, mucosal immunity provides the first line of protection for infections that initiate at the mucosal surface [25]. Mucosal routes mostly have special microfold (M) cells that are present in the epithelium covering the follicles of mucosal tissues. These M cells are responsible for the antigen transport to mucosa associated lymphoid tissues (MALT). The Peyer’s patch in the gastrointestinal route, the nasopharynx associated lymphoid tissues (NALT) in the nasal route and the bronchus-associated lymphoid tissue (BALT), are important for the induction of mucosal immunity following vaccination. Moreover, the mucosal route has the added advantage of making vaccine delivery simpler and safer than parenteral routes, which is particularly important for mass immunisation. However, rapid removal of the vaccine’s antigens by body fluids and enzymes is one of the biggest challenges mucosal immunity has to combat [23].
2.1.1. The Oral Route
Pain free delivery, safety and absence of risk of contamination via blood have always made the oral route the most preferred choice of delivery for most drugs, but the biggest challenge has been to protect the orally administered product from acidic and proteolytic degradation in the gastrointestinal tract. This can cause in a decline of the biological activity or cause adverse immunogenicity [26]. Several efforts have been made to overcome these challenges and explore the oral route for solid dose vaccine delivery.
The vaccines that are currently available through oral route are rotavirus, typhoid, cholera and some poliovirus vaccines. These usually require multiple preparatory steps that increase the chances of mistakes, thus affecting vaccine potency. Additionally, some vaccines are available in glass vials that need to be reconstituted with diluents using needles and syringes prior to administration. Antacid buffer is also sometimes provided in vials to neutralise the effect of the low pH of stomach acid, thus augmenting the problem of the cold chain [27]. An oral solid dose vaccine in the form of a tablet would undoubtedly be a very convenient option and investigations in this area are encouraged. Currently live attenuated typhoid vaccine, marketed as Vivotif, is available on the market as orally administered, enteric-coated capsules that can be swallowed without the need for additional buffering [27]. They contain an attenuated strain of the bacteria Salmonella typhi, Ty21a. The manufacturing of the vaccine involves several steps. First, the vaccine is mixed with sucrose (stabilizer), ascorbic acid and amino acids, and lyophilised. Next the lyophilised preparation is mixed with lactose and magnesium stearate and packed into gelatine capsules which are then enteric-coated to protect the vaccine from stomach acid. The capsules are finally packaged in blisters for distribution [11].
Some studies have demonstrated that when vaccine tablets were administered directly to the intestines, in the form of a suspension, the vaccines were able to elicit sufficient immunogenicity. For instance, in one study by Talavera et al., oral uncoated tablets containing inactivated cholera vaccine (Vibrio cholera strain C7258) were found to elicit immunogenicity in an adult rabbit intraduodenal inoculation model [28]. Excipients for the tablets were selected so that they are compatible with the active compound and the evaluation was performed using ELISA (enzyme-linked immune sorbent assay). Then inoculum from suspensions of tablets and the active compound were administered to the animals in the duodenum luminal space after performing a laparotomy. Antibacterial serum antibodies and vibriocidal titre measurements showed that there were no significant differences between the immunogenicity of the active compound and tablet formulation, thus demonstrating that LPS’s (lipopolysaccharide) antigenic activity remained unaffected in the final tablet formulation even after undergoing the technological process. In general, administration of whole cell inactivated vaccine may not require buffering from gastric acidity. This has been corroborated by a study carried out on a vaccine developed in Vietnam, which illustrates similar results of immunogenicity with or without protection from gastric acid. The study thus concludes that tablet formulation can be a useful pharmaceutical dosage form for producing whole cell inactivated vaccine against the deadly disease cholera, particularly prevalent in the underdeveloped regions. It further recommends preclinical and stability studies, and also, a study to evaluate the necessity of the enteric-coating for the vaccine tablet [28]. Subsequent studies were also conducted to compare the immunogenicity of oral uncoated and enteric-coated tablets containing inactivated cholera vaccines in an attempt to improve the immune response by shielding the vaccine from gastric acidity. However, no significant differences were found in terms of immunogenicity between the two types of tablets. The underlying reason can also be attributed to the fact that intraduodenal inoculation model in rabbits used did not allow proper evaluation of acid resistances for the two types of tablet formulations in vivo. Clinical studies might help to examine this further, and explain the situation; nonetheless, enteric coated tablets could be a possible pharmaceutical product for cholera vaccine [29].
A similar study was carried out by Lopez et al. where the immunogenicity effect induced on Sprague–Dawley rats by enteric coated and uncoated oral tablets of an inactivated cholera vaccine and any toxicity produced were compared. Tablets were dispersed in 2 mL drinking water for each dose and were administered to the rat orally using cannula. No significant difference in immunogenicity was found between the responses to either coated or uncoated tablets, and the tablets also did not show any toxicity to the rats [30].
However, a major drawback for oral tablets is the difficulty of swallowing, especially for children, although this can be overcome by microencapsulation with enteric polymers [29]. In addition to that, several studies have shown the effect of vitamin A deficiency and microbiota on the immune response to vaccination [31,32]. It has been found that vitamin-A deficiency disrupts the retinoic acid dependent upregulation of mucosal integrins and the trafficking of antigen specific T lymphocytes to the gastrointestinal tract, thus hampers the vaccine-mediated gastrointestinal immunity [33].
To overcome the problems of swallowing in children and elderly subjects, fast dissolving tablets (FDT) that readily dissolve in the mouth can be a plausible choice for vaccine administration. Moreover, it can also circumvent the risk of choking in patients, thus improving patient compliance. One such FDT tablet formulation has been proposed by Lal et al., where freeze-drying technique was used to produce oral tablet directly in compact blister sheet using the trivalent live attenuated vaccine (ACE527) for prevention of diarrhoea evoked by enterotoxigenic Escherichia coli as the model vaccine. Ten different formulations were prepared and examined for their structural integrity, dissolution time, moisture content and glass transition temperature. Bacterial viabilities were also assessed by CFU (colony-forming units) assays. The optimised formulation consisted of cryoprotectants (sucrose and trehalose), buffers and stabilizers (phosphate and glutamate salts), and binders (Natrosol®, polyvinylpyrrolidone and mannitol). Bacterial viability-loss during freeze drying was less than 0.3log10 (50% recovery), and during storage (at 2–8 °C for at least 12 months) was less than 0.4log10 (40% recovery). However, a higher process loss was observed when stored at higher temperature, like 25 °C or 37 °C, probably due to the low glass transition temperature that was insufficient for maintaining the amorphous glassy state. Further work is required to enhance the thermostability of the vaccines, which is crucial for avoiding the cold chain. Other than freeze-drying, most processes for producing FDT, like direct compression or mass extrusion, involve high compression and the use of shear force, which may prove to be harsh for vulnerable biological material [27]. A proprietary FDT formulation, Zydis® for olanzapine, an antipsychotic drug, has been produced by Catalent Pharma Solutions using their patented freeze-drying technology [34], but none is still available for vaccines [17]. Besides, to overcome the vitamin-A deficiency it is recommended to give vitamin-A supplements during the vaccination process, though the actual dose needs to be determined in human studies [35].
In a recent phase I clinical trial funded by Vaxart Inc., an oral recombinant adenovirus (rAd5) based vaccine for influenza A H1N1 was administered in the form of tablets to establish its safety and immunogenicity in humans. The non-replicating adenovirus vector’s elicit expression of haemagglutinin, a double-stranded RNA adjuvant and immunogenicity, were measured using haemagglutination-inhibition titres and microneutralisation titres. Individuals with pre-existing immunity to this influenza strain were excluded from the study. Tablets were enteric-coated and were prepared by mixing the purified vector with excipients, freeze-dried and followed by tableting with microcrystalline cellulose and starch. The results showed that the oral vaccine was able to elicit antibody responses to influenza in more than 90% of participants. The tablets demonstrated stability at room temperature for more than 270 days, which makes this approach feasible and encouraging [21]. It seems to be a promising technology for oral vaccine delivery in solid dosage form; however, there has not been any mention of a dose-sparing effect in this technology.
2.1.2. Pulmonary Route
The respiratory tract is the portal of entry for many pathogens and is thus equipped with well-established immunity. The lung provides a large surface area for interaction with antigens. The mucosal layer of the lung contains dendritic cells; and the lung parenchyma is lined with many epithelial cells, and antigen-presenting cells, like dendritic cells and alveolar macrophages [36]. The pulmonary delivery of vaccines can induce both systemic and local immunity. Local immunity is induced by secreted IgA, the production of which is evoked by bronchoalveolar lymphoid tissue. Besides liquid aerosols, vaccines can be administered through the pulmonary route as dry-powder aerosols as well, and these can be presented in live attenuated, inactivated, subunit, toxoid or adjuvanted forms [36]. For instance, the dry-powder of a subunit influenza vaccine was produced by spray-freeze drying (SFD) using the oligosaccharide inulin as the stabilizer. It showed that the pulmonary administration of dry-powder formulation in BALB/c mice led to higher serum IgG titres than the droplets of an aqueous solution of the subunit vaccine, the immunogenicity result of which was comparable to the intramuscular vaccination. All the vaccines were presented without adjuvants. The aerodynamic particle size of the dry-powder aerosols was 5.3 µm, and that of the droplets was 25 µm. The higher titre values can be attributed to the smaller particle size of the dry-powder aerosols, which resulted in deeper penetration of the particles into the lung [16]. However, another study using a dry-powder measles vaccine on macaques suggests the contrary. The results of the study showed that the immune response generated in animals by dry-powder aerosol was lower compared to the intramuscular injection of the vaccine. It was concluded that an improvement in either the formulation or the delivery method could give better results [37]. On the other hand, some other studies with a dry-powder measles vaccine did show some promising results. For instance, Kisich et al. used a stable and high potency dry-powder measles vaccine with a particle size distribution that was appropriate for inhalation. It was manufactured by CO2-assisted nebulization with a Bubble Dryer® (CAN-BD), processed from a bulk, liquid, Edmonston–Zagreb, live attenuated measles virus vaccine supplied by the Serum Institute of India. PuffHaler®, a novel dry-powder inhaler (Figure 1), was used, and the vaccine was administered into cotton rats. The deposition of vaccine in their lungs and successive viral replication was monitored by measles-specific RT-PCR. The immunity in response to dry-powder inhalation was similar to that by injection [38].
One particular study has reported three elementary steps for the preparation of dry-powder blends for administration through inhalation. First, the mass median diameter of the particles needs to be reduced to 1 to 5 µm. The size reduction can be achieved by different procedures, like spray drying, precipitation from supercritical fluids, and jet milling or micronisation. After this, the micronised particles need to be blended with an excipient, usually lactose. These carrier particles facilitate the distribution of the small particles and allow correct filling into the inhaler storage system in a reproducible fashion. The final step is to fill the blend into the storage systems [39]. Dura Pharmaceuticals developed a powder formulation of a measles vaccine for aerosol delivery, where they used jet milling for size reduction to generate particles (1–5 µm) suitable for pulmonary delivery. They were able to show that size reduction by jet milling did not cause any significant physical changes and the potency of live attenuated measles vaccine was preserved [40]. They also developed a unique breath actuated inhaler Spiros® that uses electromechanical energy to aerosolise and deliver a constant dose at different flow rates. It has a powder storage platform where it can store moisture or photo-sensitive compounds and eliminates the need for powder reconstitution. Additionally, it is environmentally safe, since, being breath-actuated, it does not require the need for propellants [39].
2.1.3. Intranasal Route
The nasal route is one of the suitable routes for vaccine administration, among other mucosal routes [41]. It has been found that, vaccination through this route elicits both systemic and mucosal immunity in human and animal models [42,43,44,45]. Intranasal vaccination is beneficial to children and elderly patients, because of its patient compliance. It is needle free and self administration is possible. Moreover, this route is non-invasive and only needs a small antigenic dose. The induction of mucosal and systemic immune responses makes this route different from the parenteral route, as the parenteral route only induces systemic immunity [46]. In contrast, rapid clearance, inefficient uptake of drugs and the lack of a human compatible adjuvant are some drawbacks of intranasal route [41]. Figure 2 demonstrates the basic feature of the intranasal administration of solid dose vaccine.
In rodents, nasal-associated lymphoid tissue (NALT) is the prime inductive site for mucosal immunity in the nasopharyngeal tract [48,49,50]. In human, Waldeyer’s ring, the lymphoid tissues or tonsils, is considered as the equivalent to NALT [51]. Mucosal surface protection depends on the secretory immunoglobulin-A (sIgA) and other innate defence mechanisms to protect it from pathogens [52]. Research with varying animals indicates the human immunology. Though human immunity mechanisms and biological combinations differ from animal models, appropriate in vitro studies have to be conducted before performing human trials of the intranasal vaccines [41]. Therefore, phenotypic and physiological features of NALT can be simulated to the appropriate in vitro models for the development of an intranasal vaccine [53]. Some strategies for the intranasal delivery of solid vaccine have been mentioned below:
Live attenuated vaccines: The first trivalent vaccine by intranasal route for seasonal influenza is FluMist, manufactured by MedImmune [54,55]. FluMist is advantageous over injectable trivalent vaccines for seasonal influenza because of a longer period of protection, better cross-protection, increased efficacy, and both mucosal and systemic immunity can be achieved. However, few drawbacks have been found in case of FluMist, as it causes adverse side effects, which become a safety concern, for allergy and asthma patients. Furthermore, irregular side effects like Bell’s palsy has also been noted [54].
Mucoadhesion enhancement: As most of the antigens tend to be removed easily by mucociliary clearance due to their little or no affinity towards nasal epithelium cells, mucoadhesives are co-administered with the antigens to increase the absorption rate, as well as residence time. Different polymers, for instance, polylactide-co-glycolide (PLGA), carbopol, chitosan and alginate have been used as mucoadhesives for intranasal vaccine delivery [56], as shown in Table 1. Sodium alginate and carbopol are hydrophilic polymers, and therefore, these polymers can form hydrogen bonds and be absorbed to the mucus. As a result, these hydrophilic polymers increase nasal residence time [57,58].
Particulate delivery system: Liposomes, virosomes and ISCOMs (immune-stimulating complexes) are particulates that act as vaccines which are administered through the nasal drug delivery system [67,68,69]. Liposomes are mainly made up of various ratios of cholesterol and lipids, which enclose an aqueous core. This structure allows the incorporation of wide-ranging of antigens [68,70]. The composition of virosomes includes extracted glycoproteins, which come from virus particles and mimic viral compounds. It has been found that various antigens, such as DNA [71], influenza [72,73] and HIV proteins [74] can be incorporated through the nasal route by virosomes efficiently. ISCOMS are composed of saponins, lipids and an antigen, where saponin is used as an adjuvant. Hydrophobic bonding is present among the components which enables them to be held together. Cholesterol and saponins are the main constituents of ISCOMs [75]. A particulate delivery system confers a depot effect and prevents antigen degradation. Further research needs to be conducted on the physical and chemical properties of the particulates to develop nasal drug delivery system.
Lipopeptides can be derived from both bacterial and synthetic derivatives, which act as immunostimulants. Effectiveness, non-toxicity, high purity and yield are some advantages of the lipopeptide-based delivery system. Moreover, this system nullifies the requirement of adjuvants, generates cellular as well as antibody responses, and induces both mucosal and systemic immune responses [76]. Recently, bioengineered antigen coated spherical polyhydroxyalkanoate (PHA) beads have been found to be a potential substitute to subunit vaccines, because of their unique design space, as well as their physicochemical and immunological properties, which lead to the development of safe particulate vaccine delivery [77].
Mucosal Adjuvants: Mucosal adjuvants can be used as delivery vehicles, as well as immunostimulatory molecules [78]. Usually, peptide and protein antigens need adjuvants, as these antigens show poor immunogenicity. However, it is a challenge to achieve a potent effect from adjuvants without causing toxicity. As mucosal surfaces get exposed to wide range of foreign particles, the mucosal system has to be very specific to antigens, which can in turn prevent unwanted responses and activation of immune system. Therefore, novel approaches and more research needs to be conducted for developing appropriate and potent mucosal adjuvants [41]. During selection of the device for a solid vaccine, some factors need to be considered; for instance, administration volume, spray performance and protection during transportation and storage [46].
Solid vaccines can be delivered through unit dose and the bidose nasal powder delivery system. Unitdose nasal powder delivery system is an active technology delivering a single dose of nasal powder vaccine. The maximum filling volume is 140 mm3 or 20–50 mg. The filling technology is conventional, in other words, like capsule filling. In case of the unitdose nasal powder delivery system, coordination of actuation with inhalation is not needed. The bidose nasal powder delivery system is a passive technology. Because of its special blister lamination or foil, it provides optimum protection to a solid powder vaccine. In case of this system, the maximum filling volume of the device is 190 mm3 or 50–100 mg, followed by automated filling and assembling technology [46].
Importantly, relative humidity plays a crucial role for maintaining the stability of dry-powder vaccines by affecting inter-particulate forces [79,80]. It is recommended to store the dry-powder inhaler under 40%–45% relative humidity [81]. Since most of the developing countries have higher relative humidity, it is crucial to take this factor into consideration during the formulation and packaging of the dry-powder vaccine formulation [82].
2.1.4. The Buccal and Sublingual Routes
Compared to the other mucosal routes that have been discussed above, the buccal and sublingual routes have received little attention as potential routes of vaccine delivery (Figure 3). When vaccines are targeted towards the mucosa of the ventral surface of the tongue and the floor of the mouth under the tongue, it is referred to as sublingual delivery. On the other hand, buccal delivery refers to delivery via buccal mucosa, which is mainly the one found in the inner side of cheeks, the gums, and the upper and lower inner lips [23]. Compared to gastrointestinal mucosal routes, buccal and sublingual vaccine delivery do not have the problem of the vaccine material being degraded by harsh gastric environments (gastric fluids and gastric enzymes), although some enzymes are present in the mouth. Since studies have failed to detect any special cells like M cells in the buccal and sublingual routes, it is assumed that the efficiency of these routes probably depends on the permeability of the membranes. The permeability, in turn, varies with the thickness and the degree of keratinisation of these membranes. The thickness of the human buccal mucosa is estimated to be around 500–800 μm and that of the sublingual mucosa is about 100–200 μm. Hence sublingual region is more permeable than buccal region. The sublingual route thus provides rapid uptake of macromolecules, making it an attractive choice for vaccine delivery. Nonetheless, the buccal route is also an attractive route of delivery due to the high number of Langerhans cells (LCs) present in the buccal region. The distribution of immune cells, especially the abundance of oral LCs, makes the oral mucosa a preferred option for vaccine delivery. Buccal and sublingual immunisation can evoke both mucosal and systemic immunity against pathogens, even at distant sites, like the respiratory and reproductive tracts. However, the main challenge in this route is to overcome the ‘salivary washout’ effect which might dilute the antigen and cause swallowing of the dosage [23].
Studies have been carried out for the evaluation of vaccine containing tablets using the sublingual route. In one study, model protein ovalbumin (OVA) was administered in combination with the adjuvant cholera toxin (CT) in mice via the sublingual route and it was reported that sublingual mucosa is an effective site for the induction of both systemic and wider mucosal immune responses. The immunisation results were found to be comparable to those of intranasal immunisation and superior to those of oral immunisation in terms of the magnitude and anatomic dissemination of the induced immune responses [83]. A subsequent study was carried out to investigate the effect of different rates of the release of the same antigen from tablet formulation on immune responses after sublingual immunisation. Fast release and extended release (ER) tablets were prepared to compare the respective immune responses. ER tablets are usually based on gelling hydrophilic polymers, called hydrophilic matrix tablets. The polymers form a gel layer around the tablet when they come into contact with water. The release rate will be regulated by the overall swelling and erosion [84]. The ER tablets for model antigen ovalbumin in this study were made of two-layer tablets, comprising of a mucoadhesive layer (composed of carbopol) and a controlled release layer. Since the tablets could not stick to the floor of the mouth in mice, they were applied on the ventral side of the tongue, resulting in the release of the antigen in the sublingual region. The tablets contained 250 μg of ovalbumin, directly followed by a 1 μg/mL CT solution as an adjuvant. It was found that immunisations by fast releasing tablets had higher immune responses than extended release formulations and were comparable to the reference solution (ovalbumin and CT of the same doses). ER tablets were thought to provoke a higher immune response due to the longer exposure to the immune system. But the result of the investigation was to the contrary. One of the explanations could be the continuous release of the antigen resulted in a lower dose being presented to the immune system that was insufficient to provoke a strong immune response. The amount of salivation and chewing movements can also affect the dissolution of the tablets. Thus, it was concluded that a fast-release sublingual tablet can be a possible vaccine delivery system, but the immunisation potential of ER tablets needs to be investigated further [2]. The study also evaluated the stabilizing potential of different excipients during freeze-drying of a model vaccine, killed whole-cell Vibrio cholera, that causes enteric infections. Sucrose was found to maintain the immunogenicity of the bacteria and proved to be useful for producing a complete immunogenic formulation of the commercially available oral cholera vaccine DukoralTM [10].
A recent research effort has been conducted to design wafer formulation using several excipient combinations for the delivery of wafers containing HPV vaccine via sublingual vaccination. One of the fast-disintegrating formulations for producing wafers was found to possess a diameter of 4 mm that had a dissolution time of less than 25 seconds (in 3 mL at 37 °C). The formulation was comprised of approximately 65% (w/w) myo-inositol (the placebo HPV powder) and 35% microcrystalline cellulose (MCC) [85].
2.2. Transdermal Route
2.2.1. Microneedle Delivery System
This type of delivery system is a promising way of delivery of vaccines. It mainly possesses short needles (less than 1 mm; can vary between 25–1000 μm in length) formed into arrays to penetrate the stratum corneum and access the epidermis or dermis.
Results from different studies show that breaching the epidermal layer with microneedles causes less microbial penetration compared to hypodermic needles [86]. Preliminary clinical studies in humans have shown that no pain and minimal sensation from microneedles arrays are felt, most likely because, although the microneedles are long enough to pierce through stratum corneum (10 to 15 μm deep), they are short enough to avoid the nerves located in deeper tissues [19].
There are four different, main types of microneedle: solid microneedles, that are used to pre-treat the skin before administration of the active ingredients; drug-coated solid microneedles, that function by drug dissolution in the skin; hollow microneedles—these are used for injections; and dissolving microneedles, that are produced from a polymer which contains the active ingredient in its matrix, and can serve as controlled or rapid release systems [86], as illustrated in Figure 4.
The tough barrier of stratum corneum limits access to drugs that are hydrophobic, low molecular weight and potent. Microneedles have been found to successfully deliver a variety of large and hydrophilic compounds into the skin, such as proteins and DNA. In vivo delivery has been carried out for peptides (insulin and desmopressin), plasmid DNA, oligonucleotides, hepatitis B, anthrax and Japanese encephalitis vaccines [88].
Several companies, such as Biovalv Technologies, Inc. (Westborough, MA), are working on developing this method of vaccine delivery and attaining FDA approval for the products. In a study, the Macroflux® microprojection array system (ALZA Corp., Mountain View, CA) was used to evaluate the ability of microneedles to deliver vaccines. The skin of hairless guinea pigs was penetrated by 330 μm long microneedles (coated with dry film of ovalbumin antigen), with 190 microprojections per cm2 administered on a 1 or 2 cm2 patch [19].
A multitude of studies have been carried out on solid microneedles in an attempt to deliver vaccines in solid dosage form. Some of the investigations regarding coating and dissolving microneedles in the last 10 years have been summarised in Table 2 and Table 3. Figure 5 and Figure 6 show the scanning electron microscopy images of a coated and dissolving microneedle patch to provide a clear understanding of the microneedle fabrication.
2.2.2. Jet Injectors and Solid Dose Injectors
Different approaches have been made to deliver vaccines in a needle-free delivery system. Jet injectors were designed to deliver liquid vaccine through a nozzle using high pressure, in which case the high-speed narrow stream penetrates into the skin. It can be targeted for intradermal, subcutaneous or intramuscular tissue depending on the fluid stream. Powder jet injectors for vaccines have also been under development (PowderJect Pharmaceuticals PLC, Oxford, UK). They deliver vaccines to the epidermis [19]. Although jet injectors have been proven to show higher antibody titres and avoid cold chain, the pain and severity of local reactions and bleeding were found to be similar to needle and syringes. The PowderJect technology (currently owned by Pfizer) fires powders into the skin that contain antigen. It has shown promising results for the delivery of DNA vaccines that were coated onto gold carrier particles. But the system has the problems of controlled delivery and specific penetration depth in different skin types and locations on the body. Additionally, the use of compressed gas and explosives make this device complicated, expensive, and potentially dangerous [14].
Former Glide Pharma has designed another solid dose injector which contains an actuator and a cassette that contains the drug with the vaccine in the form of a needle that has a pointed end. When the pre-set spring force is achieved, the actuator triggers and automatically delivers the drug. The pushing action is important as it delivers the drug in a controlled way at the depth of skin every time, regardless of the skin type and location. However, in Powderject technology, it was difficult to set a particular velocity that would work accurately and reliably for all patients. The actuator can be designed as disposable or reusable units when multiple doses are required. The cassettes can be removed from the actuator and the actuator resets for reuse. One of the other advantages of Glide Pharma’s solid dose injector over Powderject is that it can be self-administered, whereas the latter requires trained healthcare professionals for its implementation [112,113].
Nemaura Pharma has also developed a prototype solid dose injector for delivering vaccines transdermally. The basic mechanism is the insertion of a super sharp stainless-steel needle to breach the tough outer barrier of skin, the stratum corneum, which is followed by the delivery of a solid dose vaccine formulation wrapped around the needle, as shown in Figure 7. The result of the in vivo proof of concept study that they carried out in mice using DTaP vaccine, demonstrates that this technology does have potential for developing a low cost, self-administered, solid dose vaccine delivery system [3].
2.2.3. Epidermal Powder Immunisation (EPI)
Epidermal powder immunisation or EPI delivers solid powder vaccines to the epidermis with the help of needle free powder-delivery technology. As the epidermis contains a lot of Langerhans cells (LC) but lacks blood vessels and sensory nerve endings, it becomes an important target site for needle free drug delivery [114]. It has been found from pre-clinical studies, that the production of different types of cytokines, like TNF-α and IL-12, was increased by EPI with the help of epidermal LCs and keratinocytes, which in turn increased the immune response in mice [115,116]. Epidermal powder immunisation is advantageous over parenteral needle injection in many ways, such as the improved immune response; decreased antigen dose requirement; enhanced safety, as it avoids injury by needle injection and the risk of blood borne diseases transmission; painlessness; the elimination of needle phobia; and high temperature storage stability, eliminating the requirement for an intact cold chain [114].
The EPI delivery system is similar to a particle mediated DNA vaccine delivery system, for which ND devices, Helios™, gene gun, PowderJect XRR and AccellR are used [117,118]. In case of epidermal delivery system, powder formulation is delivered to the epidermis by the motive force of a small volume (5 mL or less) of compressed helium gas. PowderJect ND device consists of a disposable and single use helium gas canister which eliminates the chance of patient to patient contamination [119,120]. Probable degradation in the performance of this device with excessive use can also be overcome [114]. Figure 8 shows a schematic diagram of a PowderJect ND5.2, a prototype single-use delivery device for epidermal powder immunisation.
Various particle characteristics need to be considered during powder formulation for epidermal powder immunisation (EPI), such as particle size, particle shape, density, powder flow properties, particle integrity, and physical and chemical stability. Gold micro-particles and sugar excipient formulations are two different types of powder formulation used in epidermal powder immunisation technology [114].
Epidermal powder immunisation is applied in disease control because of its potency and effectiveness. Serum antibodies are important as prophylactics for immunisation against infections caused by different extracellular bacteria and viruses, and these antibodies can be increased by EPI. Besides that, EPI can also have potential immunological activity against chronic infections, caused by intracellular bacteria and viruses. It has also been found that, adjuvants that are used in EPI cause low systemic bioavailability, which in turn decreases the risk of systemic toxicity [114]. EPI has great significance in cancer immunotherapy as well. Epidermal powder immunisation eliminates the necessity for ex vivo cultures of dendritic cells (DC), unlike DC-based cancer immunotherapy. A gold formulation of EPI is used in cancer immunotherapy, which results in DC activation and the loading effect. Furthermore, it has been found that EPI is compatible with tumour cell lysates’ delivery, immunostimulatory agents, pure antigens and adjuvants [114].
Different studies on animal models have demonstrated that, epidermal powder immunisation technology may play a great role in effective allergy immunotherapy using an antigen and suitable adjuvant, by promoting strong Th1 responses. As EPI can elicit mucosal responses, it can be said that EPI can both cause an effect systemically and in the skin [114]. An influenza vaccine has been developed for use in EPI. However, more preclinical and clinical studies need to be conducted for appropriate product development for EPI. Additionally, these administration tools (injectors, cartridges, etc), as shown in Figure 9, can add cost to vaccinating, which may not be tenable in low-resource settings.
3. Discussion
Immunisation with a vaccine not only protect vaccinated individual but also protects the surrounding community indirectly by generating herd immunity [124]. Despite multiple successful campaigns for vaccination, death caused by infections remains the second leading cause of death worldwide, and this statistic is even worse in the low income countries [125]. It is indicated that about 20% of these deaths can be prevented with proper vaccination of currently available vaccines, indicating the need for substantial improvements in vaccine distribution, administration and vaccine technology in order to make vaccination more easily accessible [126]. One of the ways of combating these burdens could be the use of solid vaccines, as this can reduce the costs of vaccination, and increase vaccine efficiency by inducing mucosal, as well as systemic immunity.
Table 4 provides a summary of the different routes of administration for solid dose vaccine delivery, their current status and associated challenges. Solid dose vaccines are increasing in popularity due to circumvention of the cold chain, needle-free technologies and lower costs of handling and storage, as mentioned earlier. Many solid dose vaccine forms are designed not to be in direct contact with the bloodstream, which further increases their safety, as that will keep potent (often toxic) adjuvants and preservatives away from the general circulation. Solid dosage forms might actually curtail the need for preservatives due to their high thermostabilities [4,5,109]. If the dose-sparing effect can be achieved by harnessing the immunological power of skin immunisation, the need for adjuvants will be further minimized improving the safety of the vaccine to a great extent [107]. Solid dose vaccines, apart from ensuring the stability of the therapeutic agents and preventing the necessity of cold chain storage and sharp waste, have another advantageous factor. Patient compliance can be increased, as both the prime dose and booster shots can be combined in a single dose using solid dosage forms [127].
The oral route is always one of the most desired; however, swallowing and palatability pose a difficulty for the administration of vaccines to children [123]. Additionally, vaccines that are given orally or deposited directly on the mucosal surfaces face some challenges. For instances, mucosal secretion can dilute the vaccine’s dose; mucosal gel can capture the solid particles and mucosal proteases and nucleases can attack them; and sometimes, epithelial barriers can impede the penetration of the vaccine [128]. However, formulation techniques and delivery strategies have been developed and tested to address these challenges and these have been reviewed elsewhere [129]. The buccal and sublingual routes seem to be promising ways of delivery of mucosal vaccines, but further work needs to be carried to explore those avenues. Another important consideration for solid vaccine formulation development is the drying process which may damage the stability and potency of the vaccine. For instance, lyophilization can lead to protein instability due to irreversible changes in protein structure during the freeze-drying process [130]. However, these challenges can be addressed by introducing adjuvants into the protein formulation, like stabilizers, or by the modified spray-dried method [131,132,133].
Coated and dissolving microneedle technologies have made considerable advancements, with the aim of replacing hypodermic needles, and numerous works have been carried out in this area in the recent past, as summarised in Table 2 and Table 3. However, skin inflammation is a major concern for skin delivery, although studies have been carried out to minimise this response. For instance, in one study, the administration of rabies DNA vaccine in dogs using dissolving microneedle patches was reported to be well tolerated in the skin, with mild erythema, minimal wheal formation and a complete resolution of skin reactions within 7 days, without generating any systemic adverse effects [109]. In another study, it was reported that the BCG (Bacille Calmette–Guerin) vaccine powder-laden and dissolvable microneedle arrays displayed similar vaccination efficacy compared to the intradermal (ID) route without incurring significant skin inflammation, whereas the ID vaccination of BCG is known to cause severe inflammation for weeks at the site of inoculation [111].
Most likely, solid dose vaccine research is suffering because it is expensive to produce and companies might not have invested, as they see these innovations to be mostly profitable to the developing countries from which they will make less commercial success. With the growing need for more commercially viable products in this field more investment is suggested for solid dose vaccine research, to be able to overcome the short comings of traditional routes of delivery.
Author Contributions
N.J. conceived the idea and wrote the major sections of the manuscript; S.R.A. wrote Section 2.1.2, Section 2.1.3 and Section 2.2.3; A.A.S. was involved in evidence collection and review of the manuscript; N.K. wrote Section 2.2.1; and K.C. reviewed and edited the entire manuscript, and gave critical insights.
Funding
Thanks to Institute of Energy, Environment, Research and Development (IEERD), University of Asia Pacific for supporting publication of this article.
Conflicts of Interest
The authors declare that there is no conflict of interest.
References
- Riedel, S. Edward Jenner and the history of smallpox and vaccination. Proceeding 2005, 18, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Borde, A.; Ekman, A.; Holmgren, J.; Larsson, A. Effect of protein release rates from tablet formulations on the immune response after sublingual immunization. Eur. J. Pharm. Sci. 2012, 47, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Broadhead, J.; Cheung, K. Vaccine Delivery Using the Nemaura Solid Dose Injector. ONdrugDelivery Mag. 2016, 65, 18–22. [Google Scholar]
- Liao, J.-F.; Lee, J.-C.; Lin, C.-K.; Wei, K.-C.; Chen, P.-Y.; Yang, H.-W. Self-Assembly DNA Polyplex Vaccine inside Dissolving Microneedles for High-Potency Intradermal Vaccination. Theranostics 2017, 7, 2593–2605. [Google Scholar] [CrossRef] [PubMed]
- Kolluru, C.; Gomaa, Y.; Prausnitz, M.R. Development of a thermostable microneedle patch for polio vaccination. Drug Deliv. Transl. Res. 2019, 9, 192–203. [Google Scholar] [CrossRef] [PubMed]
- Vaccines. Available online: http://www.who.int/topics/vaccines/en/ (accessed on 26 July 2016).
- Wang, J.; Thorson, L.; Stokes, R.W.; Santosuosso, M.; Huygen, K.; Zganiacz, A.; Hitt, M.; Xing, Z. Single Mucosal, but Not Parenteral, Immunization with Recombinant Adenoviral-Based Vaccine Provides Potent Protection from Pulmonary Tuberculosis. J. Immunol. 2004, 173, 6357–6365. [Google Scholar] [CrossRef] [PubMed]
- Lycke, N. Recent progress in mucosal vaccine development: Potential and limitations. Nat. Rev. Immunol. 2012, 12, 592–605. [Google Scholar] [CrossRef]
- Allen, L.V.; Popovich, N.G.; Ansel, H.C. Ansel’s Pharmaceutical Dosage Forms and Drug Delivery Systems, 9th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2011; pp. 184–185. [Google Scholar]
- Borde, A. Design of Solid Dosage Forms for Mucosal Vaccination Investigations on the Influence of Excipients on Product Performance. Ph.D. Thesis, Chalmers University of Technology, Gothenburg, Sweden, 2012. [Google Scholar]
- Vivotif. Available online: http://www.fda.gov/BiologicsBloodVaccines/Vaccines/ApprovedProducts/ucm094070.htm (accessed on 9 August 2016).
- FluMist® Quadrivalent (Influenza Vaccine Live, Intranasal). Available online: https://www.flumistquadrivalent.com/ (accessed on 6 September 2019).
- Rotarix (Rotavirus Vaccine, Live, Oral Suspension): Side Effects, Interactions, Warning, Dosage &Amp; Uses. Available online: https://www.rxlist.com/rotarix-drug.htm (accessed on 6 September 2019).
- Potter, C.; Nabahi, S. Solid Pharmaceutical and Vaccine Dose 2013. U.S. Patent 14/095,101, 3 December 2013. [Google Scholar]
- Saluja, V.; Amorij, J.-P.; Kapteyn, J.C.; de Boer, A.H.; Frijlink, H.W.; Hinrichs, W.L.J. A comparison between spray drying and spray freeze drying to produce an influenza subunit vaccine powder for inhalation. J. Control. Release 2010, 144, 127–133. [Google Scholar] [CrossRef]
- Amorij, J.-P.; Saluja, V.; Petersen, A.H.; Hinrichs, W.L.J.; Huckriede, A.; Frijlink, H.W. Pulmonary delivery of an inulin-stabilized influenza subunit vaccine prepared by spray-freeze drying induces systemic, mucosal humoral as well as cell-mediated immune responses in BALB/c mice. Vaccine 2007, 25, 8707–8717. [Google Scholar] [CrossRef]
- Kenney, R.T.; Frech, S.A.; Muenz, L.R.; Villar, C.P.; Glenn, G.M. Dose Sparing with Intradermal Injection of Influenza Vaccine. N. Engl. J. Med. 2004, 351, 2295–2301. [Google Scholar] [CrossRef]
- Kremer, M.; Snyder, C.M. Preventives Versus Treatments. Q. J. Econ. 2015, 130, 1167–1239. [Google Scholar] [CrossRef]
- Giudice, E.L.; Campbell, J.D. Needle-free vaccine delivery. Adv. Drug Deliv. Rev. 2006, 58, 68–89. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Epidemiology and Prevention of Vaccine-Preventable Diseases; Hamborsky, J., Kroger, A., Wolfe, S., Eds.; Public Health Foundation: Washington, DC, USA, 2015; pp. 63–78.
- Liebowitz, D.; Lindbloom, J.D.; Brandl, J.R.; Garg, S.J.; Tucker, S.N. High titre neutralising antibodies to influenza after oral tablet immunisation: A phase 1, randomised, placebo-controlled trial. Lancet Infect. Dis. 2015, 15, 1041–1048. [Google Scholar] [CrossRef]
- Bal, S.M.; Ding, Z.; Van Riet, E.; Jiskoot, W.; Bouwstra, J.A. Advances in transcutaneous vaccine delivery: Do all ways lead to Rome? J. Control. Release 2010, 148, 266–282. [Google Scholar] [CrossRef]
- Kraan, H.; Vrieling, H.; Czerkinsky, C.; Jiskoot, W.; Kersten, G.; Amorij, J.P. Buccal and sublingual vaccine delivery. J. Control. Release 2014, 190, 580–592. [Google Scholar] [CrossRef] [Green Version]
- Sheikh, Z.; Jahan, N.; Karim, R. Mucosal delivery of vaccines: A review. Int. J. Pharm. Technol. 2017, 9, 6498–6520. [Google Scholar]
- Huang, J.; Garmise, R.J.; Crowder, T.M.; Mar, K.; Hwang, C.R.; Hickey, A.J.; Mikszta, J.A.; Sullivan, V.J. A novel dry powder influenza vaccine and intranasal delivery technology: Induction of systemic and mucosal immune responses in rats. Vaccine 2004, 23, 794–801. [Google Scholar] [CrossRef]
- Wang, S.; Liu, H.; Zhang, X.; Qian, F. Intranasal and oral vaccination with protein-based antigens: Advantages, challenges and formulation strategies. Protein Cell 2015, 6, 480–503. [Google Scholar] [CrossRef]
- Lal, M.; Priddy, S.; Bourgeois, L.; Walker, R.; Pebley, W.; Brown, J.; Desai, J.; Darsley, M.J.; Kristensen, D.; Chen, D. Development of a fast-dissolving tablet formulation of a live attenuated enterotoxigenic E. coli vaccine candidate. Vaccine 2013, 31, 4759–4764. [Google Scholar] [CrossRef]
- Talavera, A.; Año, G.; Pino, Y.; Castaño, J.; Uribarri, E.; Riverón, L.; Gil, S.; Fernández, S.; Cedré, B.; Valmaseda, T.; et al. Formulation in tablets of a cholera whole cells inactivated vaccine candidate. Vaccine 2006, 24, 3381–3387. [Google Scholar] [CrossRef]
- Fernández, S.; Año, G.; Castaño, J.; Pino, Y.; Uribarri, E.; Riverón, L.A.; Cedré, B.; Valmaseda, T.; Falero, G.; Pérez, J.L.; et al. Evaluation of enteric-coated tablets as a whole cell inactivated vaccine candidate against Vibrio cholerae. Travel Med. Infect. Dis. 2013, 11, 103–109. [Google Scholar] [CrossRef] [PubMed]
- López, Y.; Infante, J.F.; Sifontes, S.; Díaz, D.; Pérez, V.; No, G.; Hernández, T.; Fernández, S.; Castã No, J.L.; Cedré, B.; et al. Pharmacology and toxicology of an oral tablet whole cells inactivated cholera vaccine in Sprague Dawley rats. Vaccine 2011, 29, 3596–3599. [Google Scholar] [CrossRef] [PubMed]
- Ciabattini, A.; Olivieri, R.; Lazzeri, E.; Medaglini, D. Role of the Microbiota in the Modulation of Vaccine Immune Responses. Front. Microbiol. 2019, 10, 1305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lynn, M.A.; Tumes, D.J.; Choo, J.M.; Sribnaia, A.; Blake, S.J.; Leong, L.E.X.; Young, G.P.; Marshall, H.S.; Wesselingh, S.L.; Rogers, G.B.; et al. Early-Life Antibiotic-Driven Dysbiosis Leads to Dysregulated Vaccine Immune Responses in Mice. Cell Host Microbe 2018, 23, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, D.R.; De Calisto, J.; Simmons, N.L.; Cruz, A.N.; Villablanca, E.J.; Mora, J.R.; Barouch, D.H. Vitamin A Deficiency Impairs Vaccine-Elicited Gastrointestinal Immunity. J. Immunol. 2011, 187, 1877–1883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montgomery, W.; Treuer, T.; Karagianis, J.; Ascher-Svanum, H.; Harrison, G. Orally disintegrating olanzapine review: Effectiveness, patient preference, adherence, and other properties. Patient Prefer. Adherence 2012, 6, 109–125. [Google Scholar] [CrossRef] [PubMed]
- Surman, S.L.; Penkert, R.R.; Jones, B.G.; Sealy, R.E.; Hurwitz, J.L. Vitamin Supplementation at the Time of Immunization with a Cold-Adapted Influenza Virus Vaccine Corrects Poor Mucosal Antibody Responses in Mice Deficient for Vitamins A and D. Clin. Vaccine Immunol. 2016, 23, 219–227. [Google Scholar] [CrossRef] [Green Version]
- Tonnis, W.F.; Kersten, G.F.; Frijlink, H.W.; Hinrichs, W.L.J.; de Boer, A.H.; Amorij, J.-P. Pulmonary vaccine delivery: A realistic approach? J. Aerosol Med. Pulm. Drug Deliv. 2012, 25, 249–260. [Google Scholar] [CrossRef]
- de Swart, R.L.; LiCalsi, C.; Quirk, A.V.; van Amerongen, G.; Nodelman, V.; Alcock, R.; Yüksel, S.; Ward, G.H.; Hardy, J.G.; Vos, H.; et al. Measles vaccination of macaques by dry powder inhalation. Vaccine 2007, 25, 1183–1190. [Google Scholar] [CrossRef]
- Kisich, K.O.; Higgins, M.P.; Park, I.; Cape, S.P.; Lindsay, L.; Bennett, D.J.; Winston, S.; Searles, J.; Sievers, R.E. Dry powder measles vaccine: Particle deposition, virus replication, and immune response in cotton rats following inhalation. Vaccine 2011, 29, 905–912. [Google Scholar] [CrossRef]
- Licalsi, C.; Christensen, T.; Bennett, J.V.; Phillips, E.; Witham, C. Dry powder inhalation as a potential delivery method for vaccines. Vaccine 1999, 17, 1796–1803. [Google Scholar] [CrossRef]
- Licalsi, C.; Maniaci, M.J.; Christensen, T.; Phillips, E.; Ward, G.H.; Witham, C. A powder formulation of measles vaccine for aerosol delivery. Vaccine 2001, 19, 2629–2636. [Google Scholar] [CrossRef]
- Zaman, M.; Chandrudu, S.; Toth, I. Strategies for intranasal delivery of vaccines. Drug Deliv. Transl. Res. 2013, 3, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Muszkat, M.; Friedman, G.; Schein, M.H.; Naveh, P.; Greenbaum, E.; Schlesinger, M.; Zakay-Rones, Z.; Yehuda, A.B. Local SIgA response following administration of a novel intranasal inactivated influenza virus vaccine in community residing elderly. Vaccine 2000, 18, 1696–1699. [Google Scholar] [CrossRef]
- Hashigucci, K.; Ogawa, H.; Ishidate, T.; Yamashita, R.; Kamiya, H.; Watanabe, K.; Hattori, N.; Sato, T.; Suzuki, Y.; Nagamine, T.; et al. Antibody responses in volunteers induced by nasal influenza vaccine combined with Escherichia coli heat-labile enterotoxin B subunit containing a trace amount of the holotoxin. Vaccine 1996, 14, 113–119. [Google Scholar] [CrossRef]
- Moldoveanu, Z.; Clements, M.L.; Prince, S.J.; Murphy, B.R.; Mestecky, J. Human immune responses to influenza virus vaccines administered by systemic or mucosal routes. Vaccine 1995, 13, 1006–1012. [Google Scholar] [CrossRef]
- Smith, D.J.; Bot, S.; Dellamary, L.; Bot, A. Evaluation of novel aerosol formulations designed for mucosal vaccination against influenza virus. Vaccine 2003, 21, 2805–2812. [Google Scholar] [CrossRef]
- Birkhoff, M.; Leitz, M.; Marx, D. Advantages of Intranasal Vaccination and Considerations on Device Selection. Indian J. Pharm. Sci. 2009, 71, 729. [Google Scholar]
- Bahamondez-Canas, T.F.; Cui, Z. Intranasal immunization with dry powder vaccines. Eur. J. Pharm. Biopharm. 2018, 122, 167–175. [Google Scholar] [CrossRef]
- Zuercher, A.W.; Coffin, S.E.; Thurnheer, M.C.; Fundova, P.; Cebra, J.J. Nasal-associated lymphoid tissue is a mucosal inductive site for virus-specific humoral and cellular immune responses. J. Immunol. 2002, 168, 1796–1803. [Google Scholar] [CrossRef]
- Hiroi, T.; Iwatani, K.; Iijima, H.; Kodama, S.; Yanagita, M.; Kiyono, H. Nasal immune system: distinctive Th0 and Th1/Th2 type environments in murine nasal-associated lymphoid tissues and nasal passage, respectively. Eur. J. Immunol. 1998, 28, 3346–3353. [Google Scholar] [CrossRef]
- Wu, H.Y.; Nguyen, H.H.; Russell, M.W. Nasal lymphoid tissue (NALT) as a mucosal immune inductive site. Scand. J. Immunol. 1997, 46, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Cesta, M.F. Normal Structure, Function, and Histology of Mucosa-Associated Lymphoid Tissue. Toxicol. Pathol. 2006, 34, 599–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whaley, K.J.; Zeitlin, L. Preventing transmission: Plant-derived microbicides and mucosal vaccines for reproductive health. Vaccine 2005, 23, 1819–1822. [Google Scholar] [CrossRef] [PubMed]
- Corr, S.C.; Gahan, C.C.G.M.; Hill, C. M-cells: Origin, morphology and role in mucosal immunity and microbial pathogenesis. FEMS Immunol. Med. Microbiol. 2008, 52, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Belshe, R.B.; Mendelman, P.M.; Treanor, J.; King, J.; Gruber, W.C.; Piedra, P.; Bernstein, D.I.; Hayden, F.G.; Kotloff, K.; Zangwill, K.; et al. The Efficacy of Live Attenuated, Cold-Adapted, Trivalent, Intranasal Influenzavirus Vaccine in Children. N. Engl. J. Med. 1998, 338, 1405–1412. [Google Scholar] [CrossRef] [PubMed]
- Izurieta, H.S.; Haber, P.; Wise, R.P.; Iskander, J.; Pratt, D.; Mink, C.; Chang, S.; Braun, M.M.; Ball, R. Adverse Events Reported Following Live, Cold-Adapted, Intranasal Influenza Vaccine. JAMA 2005, 294, 2720. [Google Scholar] [CrossRef]
- Garg, N.K.; Mangal, S.; Khambete, H.; Sharma, P.K.; Tyagi, R.K. Mucosal delivery of vaccines: role of mucoadhesive/biodegradable polymers. Recent Pat. Drug Deliv. Formul. 2010, 4, 114–128. [Google Scholar] [CrossRef]
- Yang, J.; Zhao, J.; Fang, Y. Calorimetric studies of the interaction between sodium alginate and sodium dodecyl sulfate in dilute solutions at different pH values. Carbohydr. Res. 2008, 343, 719–725. [Google Scholar] [CrossRef]
- Sahoo, S.; Chakraborti, C.K.; Mishra, S.C. Qualitative analysis of controlled release ciprofloxacin/carbopol 934 mucoadhesive suspension. J. Adv. Pharm. Technol. Res. 2011, 2, 195–204. [Google Scholar] [CrossRef]
- Singh, M.; O’Hagan, D. The preparation and characterization of polymeric antigen delivery systems for oral administration. Adv. Drug Deliv. Rev. 1998, 34, 285–304. [Google Scholar] [CrossRef]
- Makhlof, A.; Fujimoto, S.; Tozuka, Y.; Takeuchi, H. In vitro and in vivo evaluation of WGA–carbopol modified liposomes as carriers for oral peptide delivery. Eur. J. Pharm. Biopharm. 2011, 77, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Witschi, C.; Mrsny, R.J. In vitro evaluation of microparticles and polymer gels for use as nasal platforms for protein delivery. Pharm. Res. 1999, 16, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Wen, Z.-S.; Xu, Y.-L.; Zou, X.-T.; Xu, Z.-R. Chitosan Nanoparticles Act as an Adjuvant to Promote both Th1 and Th2 Immune Responses Induced by Ovalbumin in Mice. Mar. Drugs 2011, 9, 1038–1055. [Google Scholar] [CrossRef] [PubMed]
- Rauw, F.; Gardin, Y.; Palya, V.; Anbari, S.; Gonze, M.; Lemaire, S.; van den Berg, T.; Lambrecht, B. The positive adjuvant effect of chitosan on antigen-specific cell-mediated immunity after chickens vaccination with live Newcastle disease vaccine. Vet. Immunol. Immunopathol. 2010, 134, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Verheul, R.J.; Hagenaars, N.; van Es, T.; van Gaal, E.V.B.; de Jong, P.H.J.L.F.; Bruijns, S.; Mastrobattista, E.; Slütter, B.; Que, I.; Heldens, J.G.M.; et al. A step-by-step approach to study the influence of N-acetylation on the adjuvanticity of N,N,N-trimethyl chitosan (TMC) in an intranasal nanoparticulate influenza virus vaccine. Eur. J. Pharm. Sci. 2012, 45, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Shen, Y.; Jiang, Z.; Wang, Y.; Chu, Y.; Xiong, S. Intranasal delivery of chitosan–DNA vaccine generates mucosal SIgA and anti-CVB3 protection. Vaccine 2004, 22, 3603–3612. [Google Scholar] [CrossRef]
- Aspden, T.J.; Mason, J.D.T.; Jones, N.S.; Lowe, J.; Skaugrud, O.; Illum, L. Chitosan as a Nasal Delivery System: The Effect of Chitosan Solutions on in Vitro and in Vivo Mucociliary Transport Rates in Human Turbinates and Volunteers. J. Pharm. Sci. 1997, 86, 509–513. [Google Scholar] [CrossRef]
- Almeida, A.; Souto, E. Solid lipid nanoparticles as a drug delivery system for peptides and proteins. Adv. Drug Deliv. Rev. 2007, 59, 478–490. [Google Scholar] [CrossRef]
- Jabbal-Gill, I. Nasal vaccine innovation. J. Drug Target. 2010, 18, 771–786. [Google Scholar] [CrossRef]
- Sharma, S.; Mukkur, T.K.S.; Benson, H.A.E.; Chen, Y. Pharmaceutical Aspects of Intranasal Delivery of Vaccines Using Particulate Systems. J. Pharm. Sci. 2009, 98, 812–843. [Google Scholar] [CrossRef] [PubMed]
- Henriksen-Lacey, M.; Korsholm, K.S.; Andersen, P.; Perrie, Y.; Christensen, D. Liposomal vaccine delivery systems. Expert Opin. Drug Deliv. 2011, 8, 505–519. [Google Scholar] [CrossRef] [PubMed]
- Cusi, M.G.; Terrosi, C.; Savellini, G.G.; Di Genova, G.; Zurbriggen, R.; Correale, P. Efficient delivery of DNA to dendritic cells mediated by influenza virosomes. Vaccine 2004, 22, 735–739. [Google Scholar] [CrossRef] [PubMed]
- Glück, U.; Gebbers, J.O.; Glück, R. Phase 1 evaluation of intranasal virosomal influenza vaccine with and without Escherichia coli heat-labile toxin in adult volunteers. J. Virol. 1999, 73, 7780–7786. [Google Scholar]
- Glück, R.; Mischler, R.; Durrer, P.; Fürer, E.; Lang, A.B.; Herzog, C.; Cryz, S.J. Safety and Immunogenicity of Intranasally Administered Inactivated Trivalent Virosome-Formulated Influenza Vaccine Containing Escherichia coli Heat-Labile Toxin as a Mucosal Adjuvant. J. Infect. Dis. 2000, 181, 1129–1132. [Google Scholar] [CrossRef]
- Bomsel, M.; Tudor, D.; Drillet, A.-S.; Alfsen, A.; Ganor, Y.; Roger, M.-G.; Mouz, N.; Amacker, M.; Chalifour, A.; Diomede, L.; et al. Immunization with HIV-1 gp41 Subunit Virosomes Induces Mucosal Antibodies Protecting Nonhuman Primates against Vaginal SHIV Challenges. Immunity 2011, 34, 269–280. [Google Scholar] [CrossRef] [Green Version]
- Pearse, M.J.; Drane, D. ISCOMATRIX® adjuvant for antigen delivery. Adv. Drug Deliv. Rev. 2005, 57, 465–474. [Google Scholar] [CrossRef]
- Bessler, W.G.; Baier, W.; vd Esche, U.; Hoffmann, P.; Heinevetter, L.; Wiesmüller, K.H.; Jung, G. Bacterial lipopeptides constitute efficient novel immunogens and adjuvants in parenteral and oral immunization. Behring Inst. Mitt. 1997, 390–399. [Google Scholar]
- Gonzalez-Miro, M.; Chen, S.; Gonzaga, Z.J.; Evert, B.; Wibowo, D.; Rehm, B.H.A. Polyester as Antigen Carrier toward Particulate Vaccines. Biomacromolecules 2019, 20, 3213–3232. [Google Scholar] [CrossRef]
- Zeng, L. Mucosal adjuvants: Opportunities and challenges. Hum. Vaccin. Immunother. 2016, 12, 2456–2458. [Google Scholar] [CrossRef] [Green Version]
- Price, R.; Young, P.M.; Edge, S.; Staniforth, J.N. The influence of relative humidity on particulate interactions in carrier-based dry powder inhaler formulations. Int. J. Pharm. 2002, 246, 47–59. [Google Scholar] [CrossRef]
- Coelho, M.C.; Harnby, N. The effect of humidity on the form of water retention in a powder. Powder Technol. 1978, 20, 197–200. [Google Scholar] [CrossRef]
- USP 32 General Notices and Requirements: Applying to Standards, Tests, Assays, and Other Specifications of the United States Pharmacopeia. Available online: https://www.uspnf.com/sites/default/files/usp_pdf/EN/USPNF/generalNoticesandRequirementsFinal.pdf (accessed on 13 July 2019).
- Tiozzo Fasiolo, L.; Manniello, M.D.; Tratta, E.; Buttini, F.; Rossi, A.; Sonvico, F.; Bortolotti, F.; Russo, P.; Colombo, G. Opportunity and challenges of nasal powders: Drug formulation and delivery. Eur. J. Pharm. Sci. 2018, 113, 2–17. [Google Scholar] [CrossRef]
- Çuburu, N.; Kweon, M.-N.; Song, J.-H.; Hervouet, C.; Luci, C.; Sun, J.-B.; Hofman, P.; Holmgren, J.; Anjuère, F.; Czerkinsky, C. Sublingual immunization induces broad-based systemic and mucosal immune responses in mice. Vaccine 2007, 25, 8598–8610. [Google Scholar] [CrossRef] [PubMed]
- Tajarobi, F.; Abrahmsén-Alami, S.; Hansen, M.; Larsson, A. The Impact of Dose and Solubility of Additives on the Release from HPMC Matrix Tablets—Identifying Critical Conditions. Pharm. Res. 2009, 26, 1496–1503. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.J. Formulation of HPV Dry Powder Wafers for Sublingual Vaccination, 2012. Bachelor’s Thesis, University of Colorado Boulder, Boulder, CO, USA, 2012. Available online: https://scholar.colorado.edu/cgi/viewcontent.cgi?referer=https://www.google.com/&httpsredir=1&article=1473&context=honr_theses (accessed on 13 July 2019).
- Indermun, S.; Luttge, R.; Choonara, Y.E.; Kumar, P.; Du Toit, L.C.; Modi, G.; Pillay, V. Current advances in the fabrication of microneedles for transdermal delivery. J. Control. Release 2014, 185, 130–138. [Google Scholar] [CrossRef]
- Kim, Y.-C.; Park, J.-H.; Prausnitz, M.R. Microneedles for drug and vaccine delivery. Adv. Drug Deliv. Rev. 2012, 64, 1547–1568. [Google Scholar] [CrossRef] [Green Version]
- Gill, H.S.; Prausnitz, M.R. Coated microneedles for transdermal delivery. J. Control. Release 2007, 117, 227–237. [Google Scholar] [CrossRef] [Green Version]
- Vrdoljak, A.; McGrath, M.G.; Carey, J.B.; Draper, S.J.; Hill, A.V.S.; O’Mahony, C.; Crean, A.M.; Moore, A.C. Coated microneedle arrays for transcutaneous delivery of live virus vaccines. J. Control. Release 2012, 159, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Hiraishi, Y.; Nandakumar, S.; Choi, S.-O.; Lee, J.W.; Kim, Y.-C.; Posey, J.E.; Sable, S.B.; Prausnitz, M.R. Bacillus Calmette-Guérin vaccination using a microneedle patch. Vaccine 2011, 29, 2626–2636. [Google Scholar] [CrossRef]
- Prow, T.W.; Chen, X.; Prow, N.A.; Fernando, G.J.P.; Tan, C.S.E.; Raphael, A.P.; Chang, D.; Ruutu, M.P.; Jenkins, D.W.K.; Pyke, A.; et al. Nanopatch-Targeted Skin Vaccination against West Nile Virus and Chikungunya Virus in Mice. Small 2010, 6, 1776–1784. [Google Scholar] [CrossRef] [PubMed]
- Perez Cuevas, M.B.; Kodani, M.; Choi, Y.; Joyce, J.; O’Connor, S.M.; Kamili, S.; Prausnitz, M.R. Hepatitis B vaccination using a dissolvable microneedle patch is immunogenic in mice and rhesus macaques. Bioeng. Transl. Med. 2018, 3, 186–196. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-C.; Lee, S.-H.; Choi, W.-H.; Choi, H.-J.; Goo, T.-W.; Lee, J.-H.; Quan, F.-S. Microneedle delivery of trivalent influenza vaccine to the skin induces long-term cross-protection. J. Drug Target. 2016, 24, 943–951. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.-H.; Noh, J.-Y.; Kim, K.-H.; Park, J.-K.; Lee, J.-H.; Jeong, S.D.; Jung, D.-Y.; Song, C.-S.; Kim, Y.-C. Effect of zymosan and poly (I:C) adjuvants on responses to microneedle immunization coated with whole inactivated influenza vaccine. J. Control. Release 2017, 265, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Edens, C.; Collins, M.L.; Goodson, J.L.; Rota, P.A.; Prausnitz, M.R. A microneedle patch containing measles vaccine is immunogenic in non-human primates. Vaccine 2015, 33, 4712–4718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Vlasova, A.; Velasquez, D.E.; Saif, L.J.; Kandasamy, S.; Kochba, E.; Levin, Y.; Jiang, B. Skin Vaccination against Rotavirus Using Microneedles: Proof of Concept in Gnotobiotic Piglets. PLoS ONE 2016, 11, e0166038. [Google Scholar] [CrossRef]
- Yang, H.-W.; Ye, L.; Guo, X.D.; Yang, C.; Compans, R.W.; Prausnitz, M.R. Ebola Vaccination Using a DNA Vaccine Coated on PLGA-PLL/γPGA Nanoparticles Administered Using a Microneedle Patch. Adv. Healthc. Mater. 2017, 6, 1600750. [Google Scholar] [CrossRef]
- Schipper, P.; van der Maaden, K.; Groeneveld, V.; Ruigrok, M.; Romeijn, S.; Uleman, S.; Oomens, C.; Kersten, G.; Jiskoot, W.; Bouwstra, J. Diphtheria toxoid and N-trimethyl chitosan layer-by-layer coated pH-sensitive microneedles induce potent immune responses upon dermal vaccination in mice. J. Control. Release 2017, 262, 28–36. [Google Scholar] [CrossRef]
- Moreno, E.; Schwartz, J.; Calvo, A.; Blanco, L.; Larrea, E.; Irache, J.M.; Sanmartín, C.; Coulman, S.A.; Soto, M.; Birchall, J.C.; et al. Skin vaccination using microneedles coated with a plasmid DNA cocktail encoding nucleosomal histones of Leishmania spp. Int. J. Pharm. 2017, 533, 236–244. [Google Scholar] [CrossRef]
- Duong, H.T.T.; Kim, N.W.; Thambi, T.; Giang Phan, V.H.; Lee, M.S.; Yin, Y.; Jeong, J.H.; Lee, D.S. Microneedle arrays coated with charge reversal pH-sensitive copolymers improve antigen presenting cells-homing DNA vaccine delivery and immune responses. J. Control. Release 2018, 269, 225–234. [Google Scholar] [CrossRef]
- Seok, H.; Noh, J.Y.; Lee, D.Y.; Kim, S.J.; Song, C.S.; Kim, Y.C. Effective humoral immune response from a H1N1 DNA vaccine delivered to the skin by microneedles coated with PLGA-based cationic nanoparticles. J. Control. Release 2017, 265, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Tu, J.; Du, G.; Reza Nejadnik, M.; Mönkäre, J.; van der Maaden, K.; Bomans, P.H.H.; Sommerdijk, N.A.J.M.; Slütter, B.; Jiskoot, W.; Bouwstra, J.A.; et al. Mesoporous Silica Nanoparticle-Coated Microneedle Arrays for Intradermal Antigen Delivery. Pharm. Res. 2017, 34, 1693–1706. [Google Scholar] [CrossRef] [PubMed]
- Turvey, M.E.; Uppu, D.S.S.M.; Mohamed Sharif, A.R.; Bidet, K.; Alonso, S.; Ooi, E.E.; Hammond, P.T. Microneedle-based intradermal delivery of stabilized dengue virus. Bioeng. Transl. Med. 2019, 4, e10127. [Google Scholar] [CrossRef] [PubMed]
- Bachy, V.; Hervouet, C.; Becker, P.D.; Chorro, L.; Carlin, L.M.; Herath, S.; Papagatsias, T.; Barbaroux, J.-B.; Oh, S.-J.; Benlahrech, A.; et al. Langerin negative dendritic cells promote potent CD8+ T-cell priming by skin delivery of live adenovirus vaccine microneedle arrays. Proc. Natl. Acad. Sci. USA 2013, 110, 3041–3046. [Google Scholar] [CrossRef]
- Matsuo, K.; Hirobe, S.; Yokota, Y.; Ayabe, Y.; Seto, M.; Quan, Y.-S.; Kamiyama, F.; Tougan, T.; Horii, T.; Mukai, Y.; et al. Corrigendum to “Transcutaneous immunization using a dissolving microneedle array protects against tetanus, diphtheria, malaria, and influenza” [J. Control. Release 160 (2012) 495–501]. J. Control. Release 2014, 184, 18–19. [Google Scholar] [CrossRef]
- Zaric, M.; Becker, P.D.; Hervouet, C.; Kalcheva, P.; Ibarzo Yus, B.; Cocita, C.; O’Neill, L.A.; Kwon, S.-Y.; Klavinskis, L.S. Long-lived tissue resident HIV-1 specific memory CD8+ T cells are generated by skin immunization with live virus vectored microneedle arrays. J. Control. Release 2017, 268, 166–175. [Google Scholar] [CrossRef] [Green Version]
- Esser, E.S.; Romanyuk, A.; Vassilieva, E.V.; Jacob, J.; Prausnitz, M.R.; Compans, R.W.; Skountzou, I. Tetanus vaccination with a dissolving microneedle patch confers protective immune responses in pregnancy. J. Control. Release 2016, 236, 47–56. [Google Scholar] [CrossRef]
- Chu, L.Y.; Ye, L.; Dong, K.; Compans, R.W.; Yang, C.; Prausnitz, M.R. Enhanced Stability of Inactivated Influenza Vaccine Encapsulated in Dissolving Microneedle Patches. Pharm. Res. 2016, 33, 868–878. [Google Scholar] [CrossRef]
- Arya, J.M.; Dewitt, K.; Scott-Garrard, M.; Chiang, Y.-W.; Prausnitz, M.R. Rabies vaccination in dogs using a dissolving microneedle patch. J. Control. Release 2016, 239, 19–26. [Google Scholar] [CrossRef]
- Mistilis, M.J.; Joyce, J.C.; Esser, E.S.; Skountzou, I.; Compans, R.W.; Bommarius, A.S.; Prausnitz, M.R. Long-term stability of influenza vaccine in a dissolving microneedle patch. Drug Deliv. Transl. Res. 2017, 7, 195–205. [Google Scholar] [CrossRef]
- Chen, F.; Yan, Q.; Yu, Y.; Wu, M.X. BCG vaccine powder-laden and dissolvable microneedle arrays for lesion-free vaccination. J. Control. Release 2017, 255, 36–44. [Google Scholar] [CrossRef]
- Transdermal Patches, Microneedles & Needle-Free Injection: Manufacturing Lines Roll as Concepts Become Products. ONdrugDelivery Mag. 2013, 40, 4–7.
- Schiffelers, R. Drug Delivery—Select Biosciences Inaugural Summit. 2–4 September 2009, London, UK. IDrugs 2009, 12, 679–682. [Google Scholar] [PubMed]
- Chen, D.; Maa, Y.-F.; Haynes, J.R. Needle-free epidermal powder immunization. Expert Rev. Vaccines 2002, 1, 265–276. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Burger, M.; Chu, Q.; Endres, R.; Zuleger, C.; Dean, H.; Payne, L.G. Epidermal powder immunization: Cellular and molecular mechanisms for enhancing vaccine immunogenicity. Virus Res. 2004, 103, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Osorio, J.E.; Zuleger, C.L.; Burger, M.; Chu, Q.; Payne, L.G.; Chen, D. Immune responses to hepatitis B surface antigen following epidermal powder immunization. Immunol. Cell Biol. 2003, 81, 52–58. [Google Scholar] [CrossRef]
- Johnston, S.A.; Tang, D.C. Gene gun transfection of animal cells and genetic immunization. Methods Cell Biol. 1994, 43, 353–365. [Google Scholar]
- Barry, M.A.; Johnston, S.A. Biological features of genetic immunization. Vaccine 1997, 15, 788–791. [Google Scholar] [CrossRef]
- Chen, D.; Endres, R.L.; Erickson, C.A.; Weis, K.F.; McGregor, M.W.; Kawaoka, Y.; Payne, L.G. Epidermal immunization by a needle-free powder delivery technology: Immunogenicity of influenza vaccine and protection in mice. Nat. Med. 2000, 6, 1187–1190. [Google Scholar] [CrossRef]
- Burkoth, T.; Bellhouse, B.; Sarphie, D. Transdermal and Transmucosal Powdered Drug Delivery—PubMed Labs. Crit. Rev. Ther. Drug Carr. Syst. 1999, 16, 331–384. [Google Scholar] [CrossRef]
- Amorij, J.-P.; Hinrichs, W.L.; Frijlink, H.W.; Wilschut, J.C.; Huckriede, A. Needle-free influenza vaccination. Lancet. Infect. Dis. 2010, 10, 699–711. [Google Scholar] [CrossRef]
- Kim, Y.-C. Skin Vaccination Methods: Gene Gun, Jet Injector, Tattoo Vaccine, and Microneedle. In Percutaneous Penetration Enhancers Physical Methods in Penetration Enhancement; Springer: Berlin, Germany, 2017; pp. 485–499. [Google Scholar]
- Cheung, K.; Das, D.B. Microneedles for drug delivery: Trends and Progress. Drug Deliv. 2014, 23, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Doherty, M.; Buchy, P.; Standaert, B.; Giaquinto, C.; Prado- Cohrs, D. Vaccine impact: Benefits for human health. Vaccine 2016, 34, 6707–6714. [Google Scholar] [CrossRef] [PubMed]
- WHO The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 5 September 2019).
- Irvine, D.J.; Swartz, M.A.; Szeto, G.L. Engineering synthetic vaccines using cues from natural immunity. Nat. Mater. 2013, 12, 978–990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saroja, C.; Lakshmi, P.; Bhaskaran, S. Recent trends in vaccine delivery systems: A review. Int. J. Pharm. Investig. 2011, 1, 64–74. [Google Scholar] [Green Version]
- Neutra, M.R.; Kozlowski, P.A. Mucosal vaccines: The promise and the challenge. Nat. Rev. Immunol. 2006, 6, 148–158. [Google Scholar] [CrossRef]
- Ryan, E.J.; Daly, L.M.; Mills, K.H. Immunomodulators and delivery systems for vaccination by mucosal routes. Trends Biotechnol. 2001, 19, 293–304. [Google Scholar] [CrossRef]
- Arakawa, T.; Prestrelski, S.J.; Kenney, W.C.; Carpenter, J.F. Factors affecting short-term and long-term stabilities of proteins. Adv. Drug Deliv. Rev. 2001, 46, 307–326. [Google Scholar] [CrossRef]
- Ohtake, S.; Martin, R.A.; Yee, L.; Chen, D.; Kristensen, D.D.; Lechuga-Ballesteros, D.; Truong-Le, V. Heat-stable measles vaccine produced by spray drying. Vaccine 2010, 28, 1275–1284. [Google Scholar] [CrossRef]
- Rathore, N.; Rajan, R.S. Current Perspectives on Stability of Protein Drug Products during Formulation, Fill and Finish Operations. Biotechnol. Prog. 2008, 24, 504–514. [Google Scholar] [CrossRef]
- Amorij, J.-P.; Huckriede, A.; Wilschut, J.; Frijlink, H.W.; Hinrichs, W.L.J. Development of Stable Influenza Vaccine Powder Formulations: Challenges and Possibilities. Pharm. Res. 2008, 25, 1256–1273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Design and use of the PuffHaler dry-powder inhaler [38].
Figure 1.
Design and use of the PuffHaler dry-powder inhaler [38].

Figure 2.
Intranasal administration of a solid dose vaccine [47].
Figure 2.
Intranasal administration of a solid dose vaccine [47].

Figure 3.
Graphical representation of buccal and sublingual vaccine delivery routes [23].
Figure 3.
Graphical representation of buccal and sublingual vaccine delivery routes [23].

Figure 4.
Methods of drug delivery to the skin using microneedles (MN). Microneedles are first applied to the skin (A) and then used for drug delivery (B) [87].
Figure 4.
Methods of drug delivery to the skin using microneedles (MN). Microneedles are first applied to the skin (A) and then used for drug delivery (B) [87].

Figure 5.
Scanning electron microscopy imaging of DT/TMC (Diphtheria toxoid/N-trimethyl chitosan) coated microneedle arrays [98].
Figure 5.
Scanning electron microscopy imaging of DT/TMC (Diphtheria toxoid/N-trimethyl chitosan) coated microneedle arrays [98].

Figure 6.
Scanning electron microscopy image of dissolving microneedles (MNs) containing DNA Polyplex Vaccine [4].
Figure 6.
Scanning electron microscopy image of dissolving microneedles (MNs) containing DNA Polyplex Vaccine [4].

Figure 7.
Delivery using the Nemaura solid dose delivery system (Modified from Fig. 2 of Reference [3] with permission from Nemaura Pharma Ltd, Loughborough, UK).
Figure 7.
Delivery using the Nemaura solid dose delivery system (Modified from Fig. 2 of Reference [3] with permission from Nemaura Pharma Ltd, Loughborough, UK).

Figure 8.
PowderJect ND5.2, a prototype single-use delivery device for epidermal powder immunisation [121].
Figure 8.
PowderJect ND5.2, a prototype single-use delivery device for epidermal powder immunisation [121].

Figure 9.
A schematic diagram showing the different types of skin vaccination methods [122].
Figure 9.
A schematic diagram showing the different types of skin vaccination methods [122].


{kind=link}
{kind=link}
{kind=link}
{kind=link}
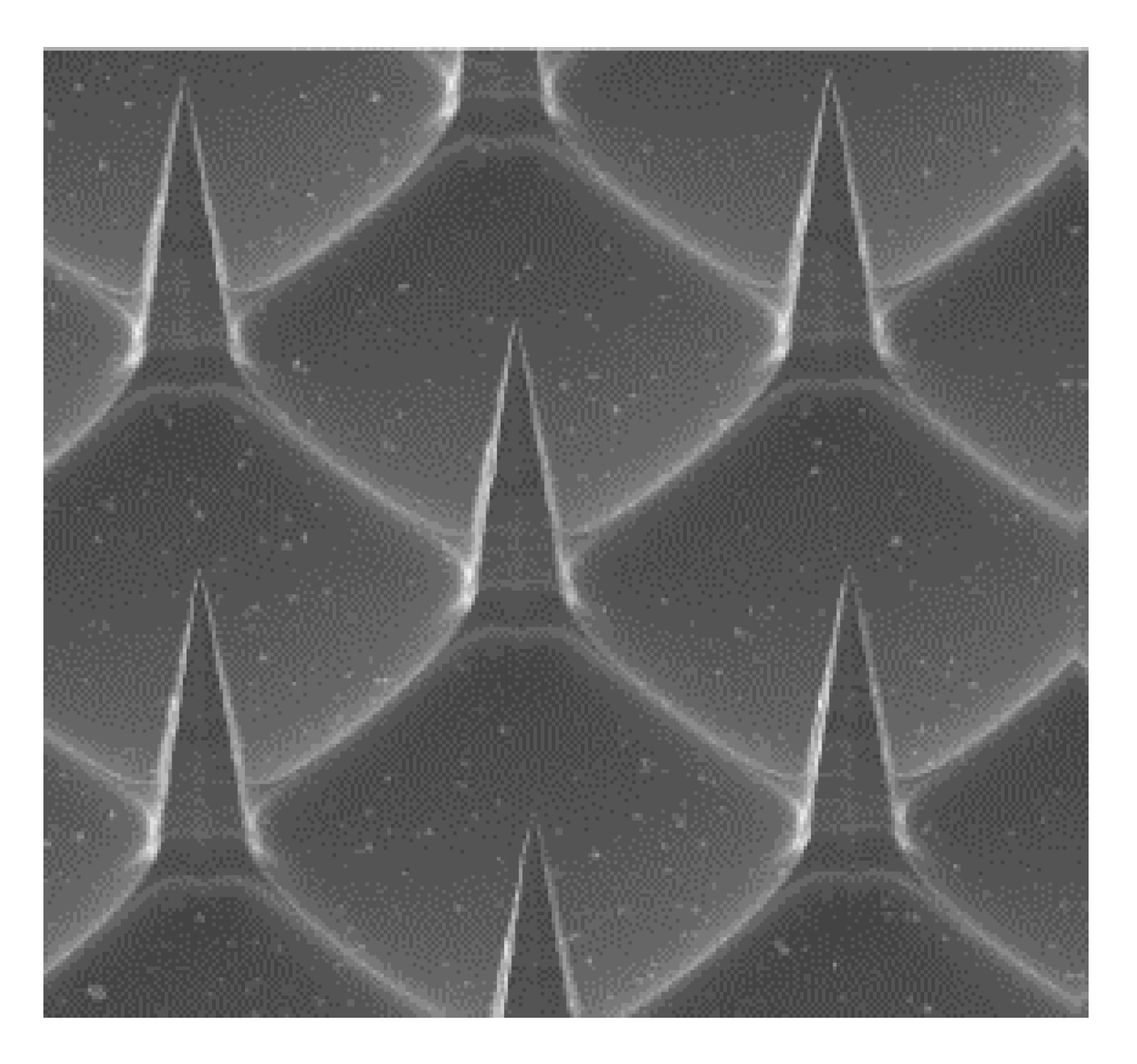{kind=link}
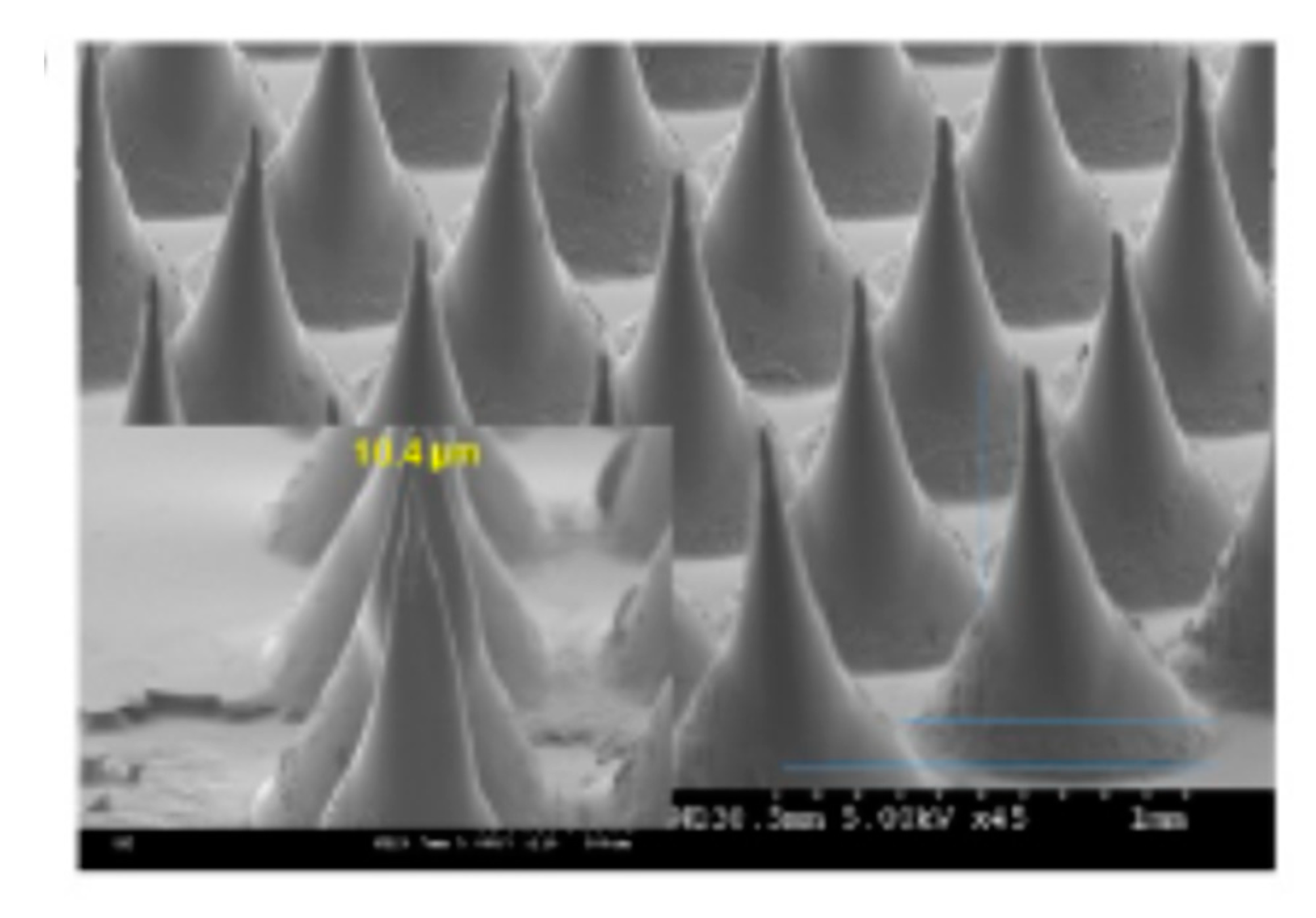{kind=link}
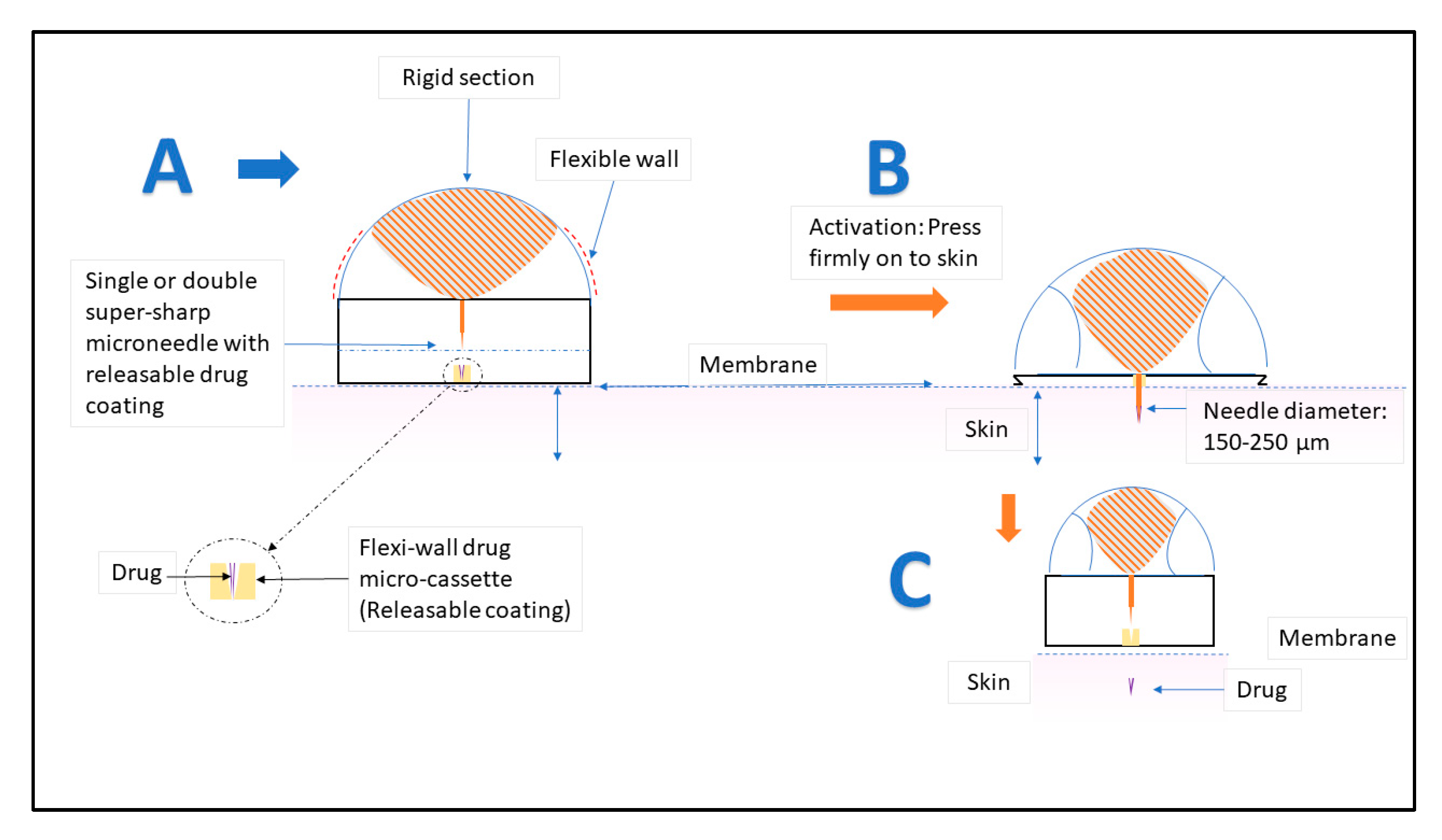{kind=link}
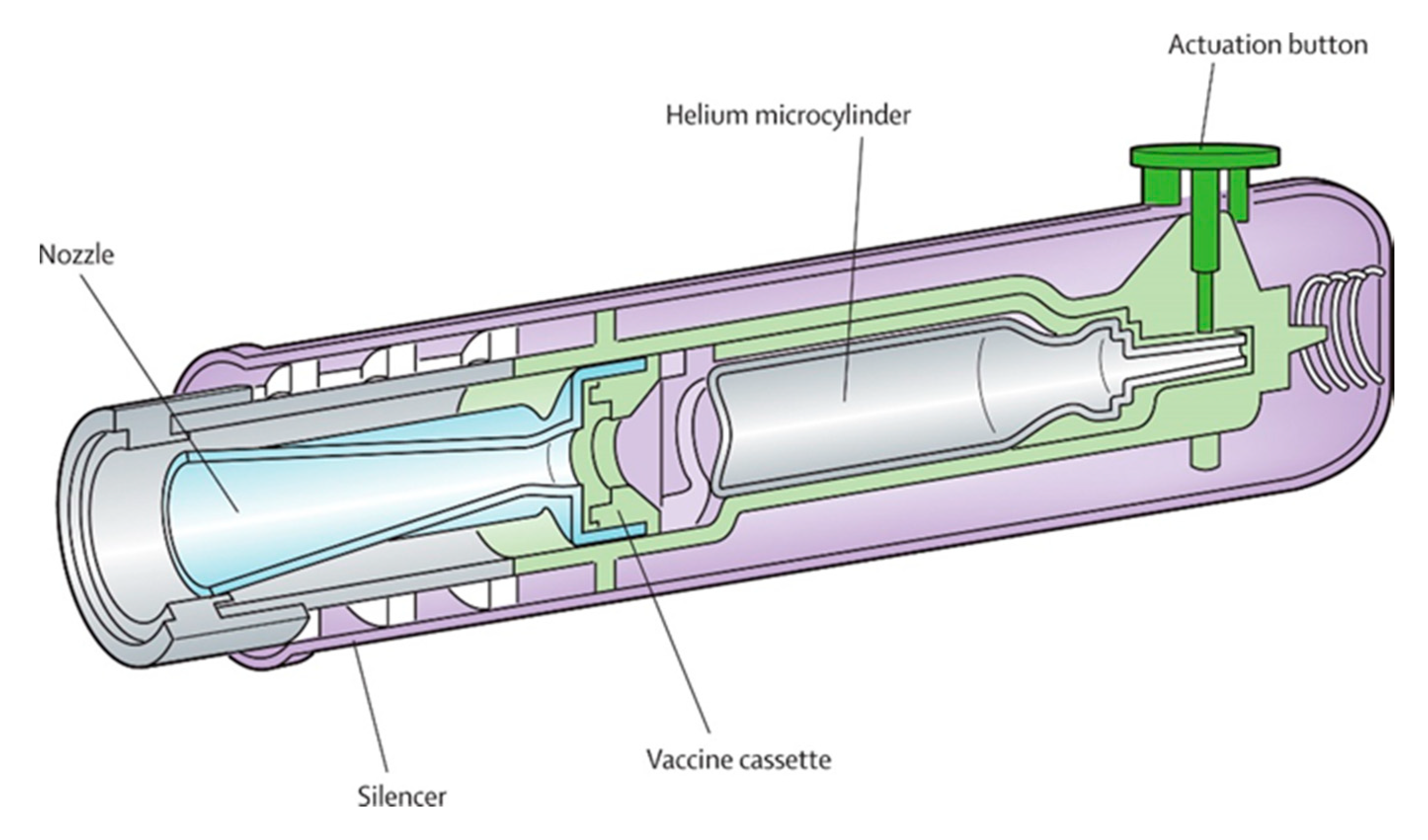{kind=link}
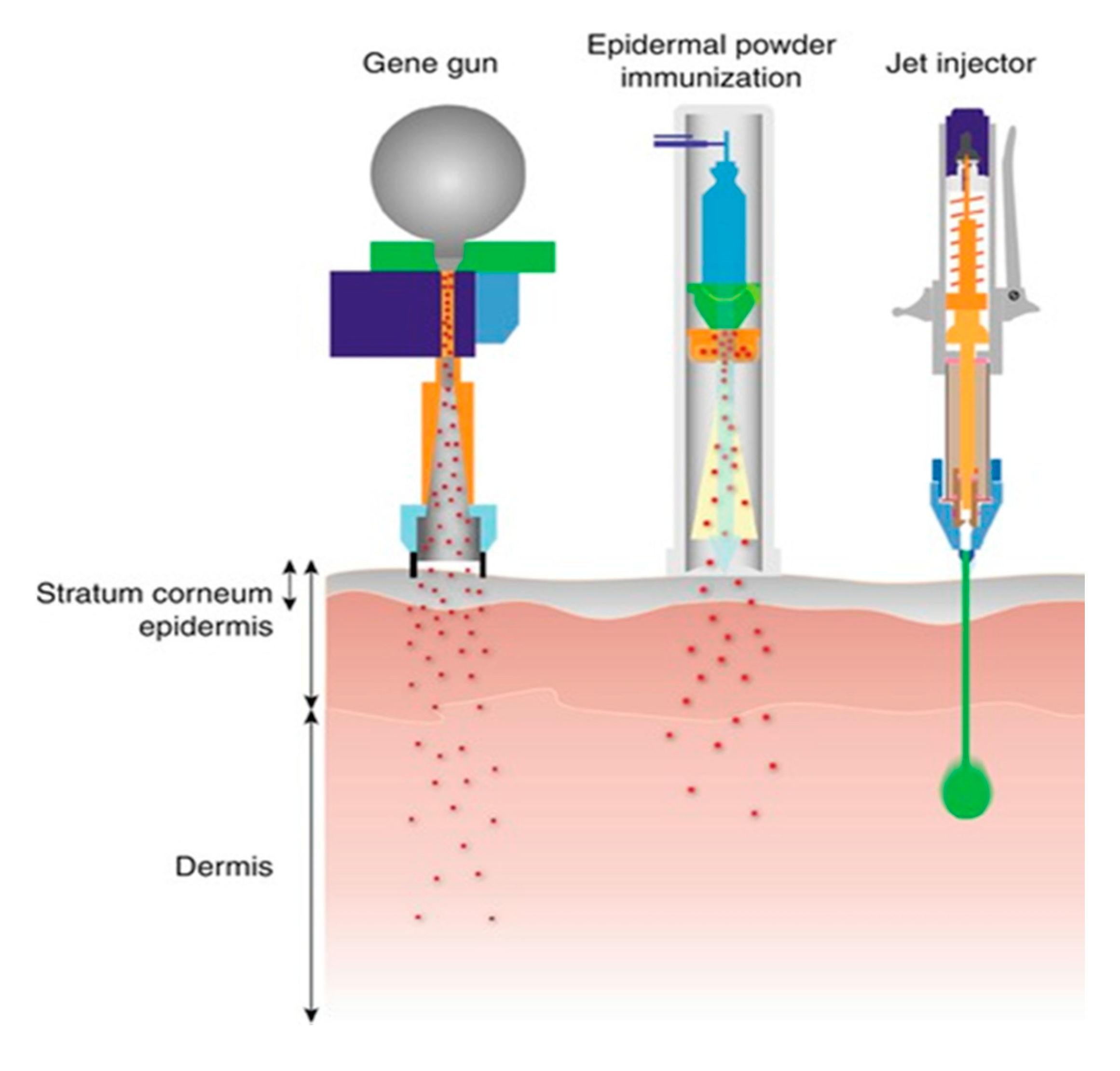{kind=link}
Table 1.
Comparative studies among different polymers used for mucoadhesives intranasal solid vaccine delivery.
Table 1.
Comparative studies among different polymers used for mucoadhesives intranasal solid vaccine delivery.
| Name of the Polymer | Property | Advantages |
|---|---|---|
| Sodium Alginate |
|
|
| Carbopol |
|
|
| Chitosan |
Table 2.
A summary of studies on the delivery of vaccines using coated microneedles.
| Disease Name | Type of Vaccine | Experimental Species | Advantages | Refs. |
|---|---|---|---|---|
| Adenovirus Infection | Live adenovirus virus | Mice |
| [89] |
| Tuberculosis | Bacillus Calmette-Guérin (BCG) | Guinea pigs |
| [90] |
| Chikungunya | Inactivated whole chikungunya virus | Mice |
| [91] |
| Hepatitis B | Adjuvant-free hepatitis B vaccine antigen | Mice |
| [92] |
| Hepatitis C | Hepatitis C virus NS3/4A protein | Mice |
| [92] |
| Influenza | Trivalent influenza vaccine containing inactivated A/PR/8/34 (H1N1), A/Hong Kong/68 (H3N2), and B/Lee/40 | Mice |
| [93] |
| Zymosan and poly (I:C) adjuvants coated with whole inactivated influenza vaccine |
| [94] | ||
| Measles | Measles vaccine | Rhesus macaques |
| [95] |
| Rota virus | Inactivated rotavirus vaccine | Piglets |
| [96] |
| West Nile virus | DNA-delivered attenuated West Nile virus vaccine | Mice |
| [91] |
| Ebola | DNA coated on PLGA-PLL/γPGA nanoparticles Polylactic-co-glycolic acid—poly-l-lysine/poly-γ-glutamic acid | Mice |
| [97] |
| Diphtheria | Diphtheria toxoid and N-trimethyl chitosan layer-by-layer | Mice |
| [98] |
| Leishmaniasis | Plasmid DNA cocktail encoding the Leishmania infantum nucleosomal histones H2A, H2B, H3 and H4 | Mice |
| [99] |
| Prophylactic vaccines | DNA polyplex vaccine | Mice |
| [100] |
| H1N1 DNA vaccine | Coated with a polyplex containing poly lactic-co-glycolic acid/polyethyleneimine (PLGA/PEI) nanoparticles | Mice |
| [101] |
| Antigen delivery | Lipid bilayer-coated; Mesoporous silica nanoparticles (LB-MSN-OVA) with antigen ovalbumin | Mice |
| [102] |
| Dengue | Dengue virus- stabilized microneedles arrays using saccharide-based formulations | Mice |
| [103] |
Table 3.
A summary of studies on the delivery of vaccines using dissolving microneedles.
| Disease Name | Type of Vaccine with Polymer Composition | Experimental Species | Advantages | Refs. |
|---|---|---|---|---|
| Adenovirus Infection | Live recombinant human adenovirus type 5 (rAdHu5) with silicone template | Mice |
| [104] |
| Diphtheria | Diptheria toxoid (DT) with Sodium hyaluronate | Mice |
| [105] |
| HIV | Recombinant human adenovirus type 5 vector (AdHu5) encoding HIV-1 gag with sodium carboxymethylcellulose (Na-CMC) | Mice |
| [106] |
| Malaria | SE36 recombinant molecule (malaria vaccine) with Sodium hyaluronate | Mice |
| [105] |
| Poliovirus | Inactivated polio vaccine (IPV) with maltodextrin and D-sorbitol | N/A |
| [5] |
| Tetanus | Unadjuvanted tetanus toxoid with polyvinyl alcohol (PVA), sucrose and CMC | Pregnant mice |
| [107] |
| Influenza | Inactivated Influenza Vaccine loaded with polydimethylsiloxane (PDMS) | Mice |
| [108] |
| DNA polyplex vaccine | Branched polyethylenimine (bPEI) pre-coated with polydimethylsiloxane (PDMS) | Mice |
| [4] |
| Rabies | Rabies DNA vaccine molded with Polydimethylsiloxane (PDMS) | Dogs |
| [109] |
| Influenza | Trivalent subunit influenza vaccine formulated with combinations of trehalose/sucrose, sucrose/arginine, and arginine/heptagluconate | Mice |
| [110] |
| Tuberculosis | Live attenuated Bacille Calmette–Guerin (BCG) bacillusis vaccine powder-laden with biocompatible and dissolvable hyaluronic acid | Mice |
| [111] |
| Hepatitis B | Adjuvant-free HBsAg vaccine with trehalose and carboxy methyl cellulose | Mice and rhesus macaques |
| [92] |
Table 4.
Summary of the different routes of administration for solid dose vaccine delivery and the associated challenges.
Table 4.
Summary of the different routes of administration for solid dose vaccine delivery and the associated challenges.
| Route of Administration | Type of Vaccine | Current Status | Challenges | Ref. |
|---|---|---|---|---|
| Oral | Vivotif- enteric coated capsules-vaccine for typhoid | Market available |
| [27] |
| Enteric coated and uncoated oral tablets of inactivated cholera vaccine | Preclinical study | [30] | ||
| Vaxart Inc. an oral recombinant adenovirus (rAd5) based vaccine to influenza A H1N1 | Phase I | [21] | ||
| Pulmonary Route | Influenza vaccine by spray-freeze drying (SFD) using the oligosaccharide inulin as stabilizer | Preclinical study |
| [16] |
| Powder formulation of measles vaccine by Dura Pharmaceuticals | Preclinical study | [40] | ||
| Intranasal Route | FluMist, manufactured by Astra-Zeneca | Market product |
| [54,55,56] |
| Buccal and Sublingual Route | Ovalbumin (OVA) in combination with the adjuvant cholera toxin (CT) | Preclinical |
| [41] |
| Two layered ER tablet containing ovalbumin, comprising of a mucoadhesive layer and a controlled release layer | Preclinical study | [42] | ||
| Wafer formulation containing HPV vaccine | Preclinical study | [44] | ||
| Epidermal Powder Immunisation (EPI) | Hepatitis B (DNA) and influenza (protein) | Phase I |
| [114] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Jahan, N.; Archie, S.R.; Shoyaib, A.A.; Kabir, N.; Cheung, K. Recent Approaches for Solid Dose Vaccine Delivery. Sci. Pharm. 2019, 87, 27. https://0-doi-org.brum.beds.ac.uk/10.3390/scipharm87040027
AMA Style
Jahan N, Archie SR, Shoyaib AA, Kabir N, Cheung K. Recent Approaches for Solid Dose Vaccine Delivery. Scientia Pharmaceutica. 2019; 87(4):27. https://0-doi-org.brum.beds.ac.uk/10.3390/scipharm87040027
Chicago/Turabian StyleJahan, Nishat, Sabrina Rahman Archie, Abdullah Al Shoyaib, Nadia Kabir, and Karmen Cheung. 2019. "Recent Approaches for Solid Dose Vaccine Delivery" Scientia Pharmaceutica 87, no. 4: 27. https://0-doi-org.brum.beds.ac.uk/10.3390/scipharm87040027