
The Use of Interpreters in Medical Education: A Narrative Literature Review
by
 ,
,
Costas S. Constantinou
*, 
Andrew Timothy Ng
,
Chase Beverley Becker
 ,
,
Parmida Enayati Zadeh
and
Alexia Papageorgiou

Department of Basic and Clinical Sciences, Medical School, University of Nicosia, Nicosia 2408, Cyprus
*
Author to whom correspondence should be addressed.
Societies 2021, 11(3), 70; https://0-doi-org.brum.beds.ac.uk/10.3390/soc11030070
Submission received: 27 April 2021
/
Revised: 14 June 2021
/
Accepted: 23 June 2021
/
Published: 1 July 2021
(This article belongs to the Special Issue Cultural Competence in Healthcare and Healthcare Education)
Abstract
:This paper presents the results of a narrative literature review on the use of interpreters in medical education. A careful search strategy was based on keywords and inclusion and exclusion criteria, and used the databases PubMed, Medline Ovid, Google Scholar, Scopus, CINAHL, and EBSCO. The search strategy resulted in 20 articles, which reflected the research aim and were reviewed on the basis of an interpretive approach. They were then critically appraised in accordance with the “critical assessment skills programme” guidelines. Results showed that the use of interpreters in medical education as part of the curriculum is scarce, but students have been trained in how to work with interpreters when interviewing patients to fully develop their skills. The study highlights the importance of integrating the use of interpreters in medical curricula, proposes a framework for achieving this, and suggests pertinent research questions for enriching cultural competence.
1. Introduction
Medical doctors practice medicine in multicultural societies and are expected to exercise cultural competence, such as working with interpreters in order to provide the best quality of care to their patients [1,2,3,4]. There are many definitions of cultural competence, although it generally refers to knowledge regarding social and cultural factors that affect health and illness and to actions necessary for the provision of quality and accessible care [1,2]. The need for cultural competence has been recognized in literature as it may reduce health disparities [2], and doctors can improve their skills and knowledge in this area of practice [5]. Research has shown that cultural competence is associated with increased patient satisfaction and adherence to therapy [1,6] and has helped physicians enhance their cultural sensitivity [7].
Despite these findings, the integration of cultural competence in medical curricula has been underdeveloped [4,8]. Alizadeh and Chavan [1] found 18 models of cultural competence, with many training paradigms for medical practitioners revealing a link between cultural competence and enhanced patient satisfaction and adherence to therapy. However, none of these models were specifically tailored for education purposes. In support of these findings, Sorensen et al. [9] also highlighted the importance of cultural issues and the need to integrate cultural competence in medical curricula.
Cultural competence encompasses several skills: from understanding the social and cultural determinants of health, exploring patients’ beliefs and showing understanding, to working in partnership with patients based on their tailored and individual social and cultural needs. One aspect of cultural competence is to work effectively with people with limited command of the language spoken by health care professionals and to recruit interpreters to assist with this task. This is vital to ensure patients from non-native cultures have equal access to essential information, diagnostic procedures, and treatment regimens [10]. The evidence on the use of interpreters in medical consultations is rich and generally demonstrates that when communication between doctors and patients is augmented, there is a reduction in errors [11] and the cost of medical care in terms of decreased visits in emergency rooms and lower readmission rates [12]. However, Himmelstein, Wright, and Wiederman [13] explained that there is negligible evidence about medical students working with interpreters within the medical curricula. On this note, we think that the following questions are important to consider. First, are medical/health care undergraduate students provided with professional and/or ad hoc interpreter resources when they are at their clinical placements and they encounter patients that do not speak the language of instruction? Second, have the students and interpreters been through a training before they come to work together at the clinical placements? Third, are undergraduate medical/health care students provided with training on how to use interpreters in health care consultations when they graduate? The third question is easier to answer and there is more literature available as it will be shown in this review. However, one might say that if students are taught how to use professional interpreters when interviewing patients, they might be able to use the knowledge and skills when they are provided with interpreters at their clinical placements. This is where the difficulty lies. How many medical schools provide professional and/or ad hoc interpreters when students are sent to their clinical placements in order for the students to fulfill course requirements such as Direct Observations and MiniCex (Mini Consultation Evaluation Exercise)? Are these interpreters trained on how to help students maximize their knowledge and experience and collect evidence for their portfolios? Are the clinical tutors and other clinical staff who supervise the students trained on how to use interpreters to achieve the learning outcomes of the curriculum? What about the patients who are vulnerable when attending these health care settings, especially when they do not speak the health care professionals’ and students’ language? How do they feel to be interviewed by students accompanied by interpreters?
Based on a gap identified by Wright and Wiederman [13] and on the questions above, the research aim of this study focuses on understanding the extent of interpreter utilization in medical education as part of the curriculum and its effects on educational and health outcomes. To address the research aim, this study has conducted a narrative literature review as presented below.
2. Methodology
The methodology used for this narrative review was based on guidelines by Ferrari [14] and the SANRA (Scale for the Assessment of Narrative Review Articles) [15]. These guidelines clarified that narrative reviews should include a clear research aim, ample justification, and a search strategy. The aim of this narrative review is to explore the use of interpreters (ad hoc and professional) in international medical education. Due to the lack of a fixed research hypothesis, as per the guidelines for narrative reviews [14], as per Table 1 our inclusion and exclusion criteria were the following: peer-reviewed articles, theses, dissertations, literature reviews, conference papers, editorials, and books or textbooks that include medical students, published between 2000 and 2020 in the English language.
Based on the criteria above, the following databases were searched: PubMed, Medline Ovid, Google Scholar, Scopus, CINAHL, and EBSCO. We relied on databases which could help us extract papers in social sciences, medical education, and health care, and to which our Institution had access. In order to achieve a focused search and address the aim of the project, we used specific keywords, and these were: interpreters, translators, medical education, medical school, curriculum, medical training, education, medicine, medical students, clinical education, clinical settings, language barriers, facilitators, barriers, confidence, satisfaction, patient perspective, patient outcomes. For facilitating our search and review of the identified articles we organized several questions into four main areas, namely utilization, perspective, impact, and barriers/enablers, as per Table 2 below. We did not treat the questions in Table 1 as research questions but only as guides for our search and for reviewing the articles in order to ensure that the articles selected were the most relevant. These questions were also used as the context for generating codes and constructing overarching themes.
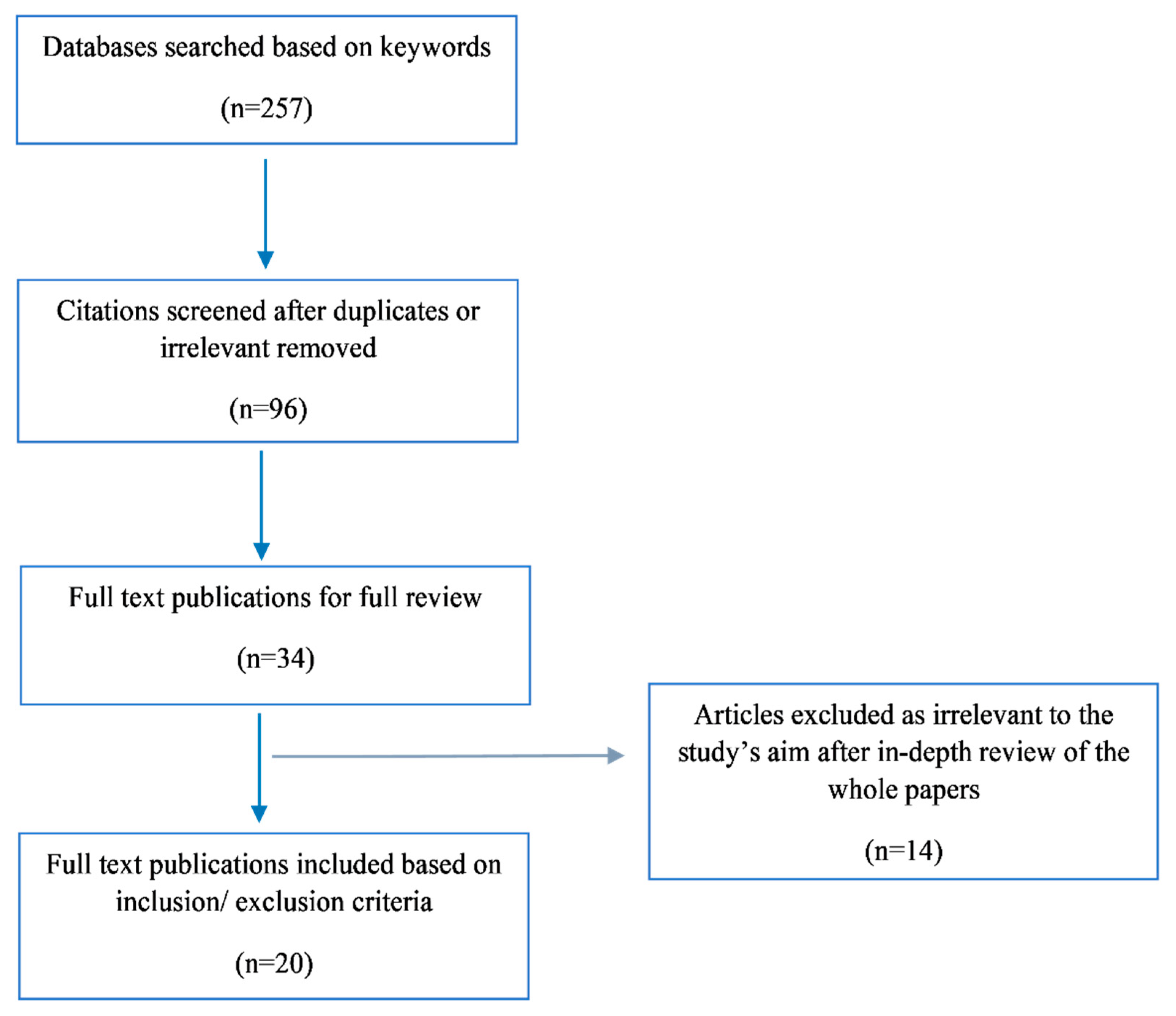
As per Figure 1, the initial search generated 257 articles. The process of excluding duplicates and irrelevant papers resulted in 96 articles. Based on reading the abstracts of these sources in accordance with our inclusion and exclusion criteria, 34 sources were selected for in-depth review. After careful review, 14 articles were excluded because they did not relate to the research aim of this review. These articles largely pertained to clinicians or early career doctors, and challenges faced with language barriers, but they did not discuss interpreting services. The detailed review resulted in the selection of 20 articles as they reflected, directly or indirectly, the research aim of this study.
For the analysis of the articles, we relied on an interpretive approach to effectively understand the use of interpreters in medical education and on Thomas and Harden’s [16] thematic synthesis technique. Thematic synthesis consists of three stages. Firstly, the articles were thoroughly read multiple times to become familiar with the methods and the findings. Secondly, the findings in each article were coded based on the research aim of this study. Thirdly, the codes were grouped together in order to construct overarching themes, ultimately forming a codebook which helped organize and interpret the results. After the construction of the codes and themes, the analysis was drafted and refined by revisiting the articles, initial codes and themes. To ensure the validity of the results, a two-level quality assurance process was instituted, whereby the researchers split into two groups and followed the review procedure (i.e., check codes and themes, revisit the articles, refine the codes and themes) independently.
For the critical appraisal of the articles included, the Critical Assessment Skills Programme (CASP) was used as a guide [17] due to the absence of specific appraisal guidelines for narrative literature reviews [14]. Consequently, the critical appraisal of the articles is presented under results in the form of a narrative and in a table in Appendix A.
3. Results
From the coding of the articles, two overarching themes emerged, largely reflecting the types of articles identified. That is, “use of interpreters during undergraduate medical/health care curricula”, and “developing students’ skills through training in how to use interpreters in health care interviews or consultations”.
3.1. Use of Interpreters during Undergraduate Medical/Health Care Curricula
This section is centrally relevant to the research aim of this study because it focuses on the use of interpreters during undergraduate medical/health care curricula. Interestingly, only five papers discussed the actual use of interpreters in medical or health care education as part of the curriculum [13,18,19,20,21]. More specifically, Itaya et al. 2009 [18] conducted a survey with students and faculty members to understand how the limited English patients (LEP) were managed in dental education and what was the perceived impact on the quality of education. One hundred and twenty-two (122) students and fifty-six (56) faculty members from five out of six dental schools in California—United States of America (USA)—completed the survey and the results revealed that only ad hoc interpreters were used when dental students interacted with LEP patients at their clinical placements. Further, it revealed that the use of interpreters did not meet the required standards by the U.S. Department of Health and Human Services and the Commission on Dental Accreditation (CODA) and that the lack of professional interpreters in dental schools had a negative impact on the quality of dental education. For example, it increased the length of appointments and decreased the students’ ability to provide high-quality care for these patients (e.g., getting patients to accept treatment plans, gaining compliance with home oral health preventive behaviors, completing treatment plans, etc.).
Another study by Simon et al. [19] with a larger sample of participants exploring what dental schools in the USA did to prepare their students to work effectively with interpreters when interacting with LEP patients during their clinical placements—and therefore improve the care of LEP patients—found the same trends. That is, students from 19 out of the 62 dental schools who completed the survey reported that there was insufficient integration of interpreters in their clinical teaching and poor-quality training for this. To elaborate, only 56.3% of the 325 respondents reported that there was some integration of interpreting services in their education. Additionally, 43.7% said that interpreting services were not used and approximately 30% of the students explained that such lack of services compromised the quality of care provided to LEP patients and the achievement of their dental education outcomes. Only 54% of the respondents agreed that they were well prepared to manage LEP patients after graduation.
In addition to dental schools, a more recent study was conducted using medical schools in the USA [13]. Out of the 147 schools that received a survey link, 38 responded with 29 schools reporting their curriculum addressed the use of interpreters. However, only 10 of these 29 schools had used simulated environments for students’ learning or used didactic teaching sessions. The rest of the schools did not have any relevant curriculum. The majority of the schools (22) offered such training during the first two years of education, while seven schools offered the training later: during years three and four. Eighteen (18) of these schools started training their students how to work with interpreters in the last 10 years. However, this study did not explore whether the medical schools provided trained interpreters or ad hoc interpreters to their students when meeting LEP patients at their clinical placements.
The fourth relevant study by Omoruyi et al. [20] developed and evaluated a curriculum to teach medical students how to use telephone interpreter services during their 8-week outpatient pediatric clinical rotation. This is the only study we found to evaluate medical students’ ability to use interpreter skills in actual patient encounters. The researchers used a case-cohort comparison to investigate “behavioral outcomes of the exposed learners to evaluate if the training had an impact on actual patient encounters.” The results of the study suggested that this type of interventions increased medical students’ perceived self-efficacy in using interpreters in actual patient encounters. More specifically, the students who went through the curriculum were more likely to use effectively the skills below than the students who did not receive the curriculum:
- The trainee asked the patient one question at a time.
- The trainee presented information at a pace that was easy to follow for both patient and interpreter—that is, information was given in digestible chunks
- The trainee addressed the patient as “you” and not as “he” or “she.”
- The trainee appropriately closed the encounter: at a minimum, asked the patient if he or she had any questions.
The fifth relevant study by Mazori et al. [21] evaluated a program of working with interpreters at a free clinic. Of the 76 medical students, 40 were allocated to the intervention group and 36 were allocated to the control group. The results of the study were very similar to those of Omoruyi et al. (2018) in that when medical students in the intervention group interviewed a LEP patient in their clinical placements (family medicine clerkship), they were able to improve their communication skills such as:
- Asked patient one question at a time
- Addressed patient directly
- Maintained direct eye contact with patient
- Listened to interpreter without unnecessary interruption
- Asked interpreter questions about incomplete interpretations
- Spoke in short, simple sentences with pauses for interpretation
The findings from these five papers show that the use of interpreters in clinical settings in medical education is scarce—or has not yet been documented—and when interpreting services were used, they were underdeveloped in the sense that a few schools used these services or used them on an ad hoc basis. These papers provided some insights into the use of interpreters in medical education in the USA, but we still do not know the extent of the use of interpreters in medical education globally; what patients think about the services; and how students and interpreters feel about it. Although Omoruyi et al.’s [20] and Mazori et al.’s [21] studies discussed the impact of using interpreters on students’ skills, there is no study included in this review which presents information about long-term educational outcomes, student satisfaction, and the impact of interpreting services in medical education on patients and their health outcomes. Such lack of evidence highlights a huge gap in improving medical education in multicultural environments and the need to empirically explore the impact of interpreting services on educational and health outcomes. Finally, we did not find any studies focusing on students’, patients’, interpreters’, or doctors’ perspectives on interpreting services, and on the facilitators and barriers for utilizing interpreters in medical and health care education. However, despite these gaps, students at some schools have been trained in how to work with interpreters, as discussed below.
3.2. Developing Students’ Skills through Training in How to Use Interpreters in Health Care Interviews or Consultations
Fifteen (15) articles were not centrally located in our research aim because they did not discuss the direct use of interpreters in clinical settings as part of the curriculum. However, they indirectly addressed the training of students in using interpreters. That is, these trainings have largely involved interpreters through scenarios or in simulated environments rather than in actual clinical placements or as part of the existing curriculum like the studies discussed in the previous section. Such trainings indirectly relate to our research aim because it is important to know whether they have helped students, thereby informing decisions about the integration of interpreters in medical education.
The findings of these articles indicated that there has been a variety of training paradigms utilized, especially during the pre-clinical years, such as web-based modules [22,23,24], workshops [25], and evaluation of a longitudinal program [26]. The majority of these paradigms were effective because they helped students develop their skills of using interpreters in their health care interviews/consultations. Specifically, the results demonstrated students had improved their skills in working and collaborating with interpreters [22,23,24,25,26,27], had improved attitudes [23], were more careful while working with people from other cultures, and appreciated patients’ immigration status [23]. In addition, their self-confidence [28,29] and self-efficacy [30,31] were enhanced. Students also became more familiar with the relevant procedures used when working with interpreters and LEP patients [29], enhanced their cultural competence skills [32,33,34,35], and managed to match what they practiced with their curriculum [28].
Moreover, Kalet, Gany, and Senter’s [22] and Kalet et al.’s [23] studies indicated that students greatly appreciated the training paradigms they used and expressed a strong interest in learning to collaborate with interpreters. In addition to the use of professional interpreters, two studies focused on the use of medical students as interpreters [21,34]. The results revealed that these students improved their skills and enhanced their cultural competency, but were challenged when attempting to separate the two roles in educational settings.
All these findings highlight that various training programs have helped students become more fluent in working with interpreters for the benefit of health care praxis and subsequently for patients. Interestingly, these training programs also suggested that occasionally student skills did not improve and that new paradigms should be explored to further develop the curricula. For instance, Lie, Bereknyei, and Vega’s [26] study found that the skills “ask one question at a time”, “listen without interruption”, and “invited questions” deteriorated over time. The authors postulated several reasons for this. They suggested that relying on ad hoc or temporal training paradigms should be avoided because students’ skills may deteriorate if they do not immerse themselves in life-long reflective development [20,26]. In other words, students should engage in repeated utilization of interpreters during their medical studies as part of the curriculum to enhance their fluency. Lie, Bereknyei, and Vega’s study further suggested that without linking this to the formal curriculum, which combined didactic teaching and reflective practices, skills may not be sustainable. Finally, the skill of using interpreters should be taught separately initially for students to master the relevant skills before integrating them with other competencies [26].
4. Critical Appraisal of the Articles Reviewed
The 20 articles reviewed were evaluated based on their relevance to the research aim and scientific vigor. Based on CASP (Critical Assessment Skills Programme) guidelines, all articles had either a clear aim, research question(s), or hypotheses, and their importance ranged from moderate to high (see Appendix A for more detail). This was gauged on how valuable each research paper was in accordance with the following criteria: appropriateness of research design, sampling and data collection, use of validated instruments, discussion of contribution to scholarship, identification of new areas in research, and generalizability or transferability of the findings. The sample sizes in the studies ranged from a few cases (i.e., schools) and a few participants [18] to a few hundred [2,5,25,26,31,35] with varying research methods. Some of the articles employed cross-sectional designs and surveys and used questionnaires to measure perceived effectiveness of training paradigms [5,19,35]. Many articles used pre-post scoring scales or tests [22,23,24,27,30,31], while only very few articles relied on control trials with control or intervention/control groups [20,21,29]. In general, all articles answered their research aim and presented useful results which could inform decisions and open new directions in research.
The review of these articles also revealed some important limitations. In some cases, sample sizes were small [17,33,36], the instruments used were not validated [21,32], or there was no randomization of the population studied [25,30,33]. Additionally, the employment of qualitative methods as a primary research methodology was not seen. The use of qualitative methods could help give an in-depth understanding of the challenges and need for using interpreters. For example, qualitative interviews, focus groups, and observations guided by phenomenological frameworks could provide useful insights and address many research questions regarding students’, patients’, and doctors’ experience with using interpreters in medical education. In a few studies, a focus group was used either for exploratory or expansion purposes [29,35]. Moreover, there is a need to design more randomized control trials in order to better understand the impact of the use of interpreters on educational and health outcomes for students and patients, respectively. The studies were largely from the United States or were about university- or school-specific training paradigms. No comparison between schools and even counties was identified in the literature. In some studies, the testing of students’ skills did not occur in real clinical settings [22,23,24,31]. This raises the issue of the transferability of the results. Although most studies showed improved skills by students, there was no evidence for the sustainability of these skills. Lastly, in general, studies focused on patients from Western countries and were based on the assumption that patients eagerly utilized health care services. This limitation suggests that working with interpreters should be part of the broader canopy of cultural competence whereby both medical students and medical doctors develop skills for working with diverse populations, such as understanding cultural beliefs, daily practices, their perception of evidence-based medicine, and so forth, and involving patients in shared decision making.
5. Discussion
This literature review focused on exploring the use of interpreters with physical presence in medical education and the effects on the quality of medical education and patient care. The findings indicated that the use of interpreters in medical education is scarce or has not yet been documented. Interestingly, medical students have been trained either through their curriculum or on an ad hoc basis on how to work with interpreters effectively based on scenarios or simulated environments; yet the clinical use of interpreters either in pre-clinical or clinical years has been very limited.
The findings regarding the use of interpreters in health care education reflect the existing literature about the usefulness of cultural competence in medical education and health care in general [1,6,7] and also their use in medical consultations [11,12]. Additionally, this study has revealed that training students in how to work with interpreters helps students develop their clinical communication skills and enhance their familiarity in this area which can potentially help them when entering health care settings for their clinical years. This finding is in accordance with what other studies show about the improved skills of doctors when trained in working with interpreters [11,12]. The study’s main contribution to scholarship is that it has shown the significant gaps in the development of medical interpreter use curriculum and the impact of using interpreters in medical education on educational and health outcomes for students and patients respectively. Therefore, the questions which were utilized as a guide for this study’s search strategy, and the review of the selected papers, could be used for research. For example, the following research questions derived from this study can be explored through robust research designs, provided that the use of interpreters in medical education is well integrated:
- What is the effect of the use of interpreters on the quality of medical education?
- What are the levels of confidence and self-efficacy of medical students in using interpreters in medical education (e.g., when they interact and interview LEP patients in their clinical placements)?
- What are the facilitators and barriers for using interpreters in medical education for medical students, their supervisors, and the patients?
- How do patients experience and understand the use of interpreters?
- What are the perspectives of interpreters, health care providers (e.g., clinics, hospitals, health care facilities, etc.), and medical educators?
- How is the use of interpreters in medical education associated with health outcomes?
- What skills do students develop when collaborating with interpreters during their medical education?
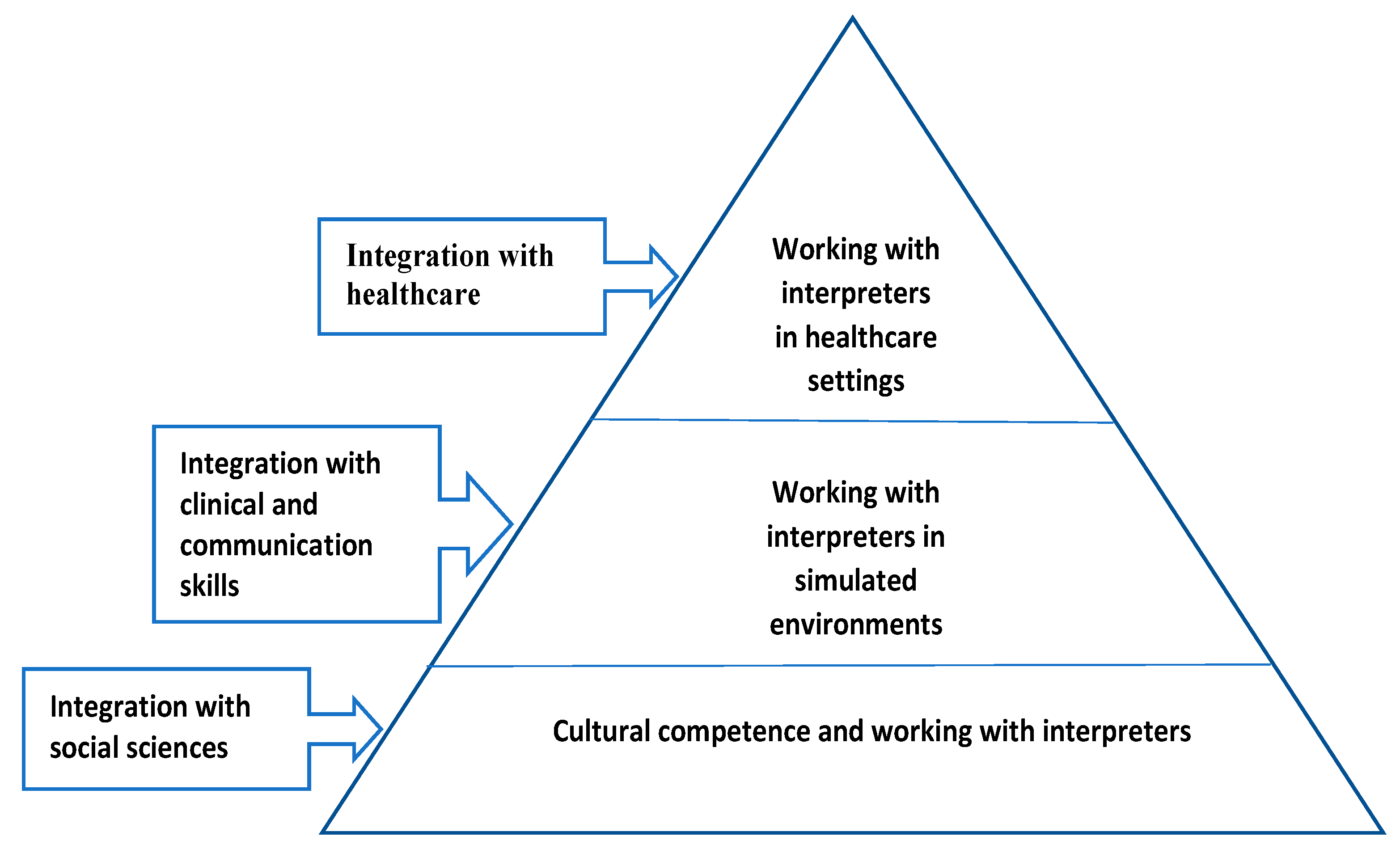
Based on the findings of this study and the identified need to integrate interpreting services in medical education and scientifically explore its impact, we propose a framework for achieving such integration. As per Figure 2, working with interpreters should be under the cultural competence curriculum whereby students acquire knowledge in social and cultural determinants of health and skills in how to work with diverse patients and interpreters. During this stage, training in cultural competence and working with interpreters could be achieved by integration with social sciences and through lectures, interactive cases, and interactive videos. As students move into their medical program and develop their skills, learning how to work with interpreters should be integrated with already-acquired clinical and communication skills. Mastering these skills to work with interpreters could be achieved in simulated environments whereby students learn and practice in small groups utilizing clinical scenarios aided by real simulated patients. Later in their studies, during medical practice or clerkships in hospitals, students could activate the knowledge and skills they gathered from previous years and work effectively with interpreters in health care settings. On this note, this proposed framework suggests that integration of working with interpreters in medical education should be longitudinal and learning should be developed through constructivist and spiral learning approaches.
6. Conclusions
This narrative literature review focused on understanding the scale of utilization of interpreters in medical education and its potential effects on educational and health outcomes. Interestingly, only five papers were identified in that area, two of which were about dental schools and three about medical schools. These five papers showed that the use of interpreters in medical education is scarce and needs to be improved. However, fifteen more articles were reviewed for this study because they indirectly explored the effectiveness of training medical students in how to use interpreters in health care consultations, which showed that students improved their knowledge and skills, although there was no evidence for the sustainability of these skills. This study is an important contribution to the existing scholarship as it highlighted a need to integrate interpreters in medical education within the context of cultural competence curriculum in order to help students to acquire sustainable skills. The study suggested important questions to address research gaps for the future and proposed a framework for achieving successful integration of utilizing interpreters in medical education curricula.
Author Contributions
All authors have contributed substantially to the study and the preparation of the manuscript. C.S.C. has coordinated the study, reviewed and coded the articles, drafted and finalized the manuscript. A.T.N., C.B.B., and P.E.Z. have worked on the design of the study, the search and review of articles, and provided feedback on drafts of the manuscript. A.P. has coordinated the study, provided guidance, reviewed the articles, and provided feedback on drafts of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Review table of selected papers based on CASP criteria. We used the criteria for qualitative studies as they applied to all types of studies included in this review, such as surveys, qualitative, and randomized control trials.
| In-Text Citation | Article | Type of Research and Participants | Aim/ Key Findings | Was There a Clear Aim or Research Question? | Was the Methodology Appropriate? | Was the Research Design Appropriate to Address the Aim? | Was the Recruitment Strategy Appropriate to the Aims of the Research? | Was the Data Collected in a Way That Addressed the Research Issue? | Have Ethical Issues Been Taken into Consideration? | Was the Data Analysis Sufficiently Rigorous? | Is There a Clear Statement of Findings? | How Valuable is the Research? |
| 13 | Himmelstein J., Wright W.S., Wiederman M.W. U.S. medical school curricula on working with medical interpreters and/or patients with limited English proficiency. Adv Med Educ Pract. 2018;9:729–733. | Survey, 38 Schools | Aim: to describe curricula offered by the United States medical schools to teach students to work with medical interpreters and patients with LEP. Key findings: Of the 38 respondents, 29 had curriculum to prepare students to work with medical interpreters and/or patients with LEP and 10 of those had experiences with standardized patients to actually practice. The other 9 schools did not have training part of formal curriculum. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 18 | Itaya LE, Glassman P, Gregorczyk S, Bailit HL. Dental school patients with limited English proficiency: the California experience. J Dent Educ. 2009;73(9):1055–1064. | Survey, 122 students, 56 faculty members from 5 dental schools | Aim: to survey dental schools in California with respect to the number, communication strategies, impact on education and clinic finances, and student and faculty perceptions regarding serving LEP patients in their clinics. Key findings: The results of this survey suggest that dental schools face serious challenges in complying with federal standards for the treatment of LEP patients. Most students believed the current system of using untrained interpreters (e.g., family/friends) was adequate, but they also said it was more difficult to treat LEP patients. | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes |
| 19 | Simon L, Hum L, Nalliah R. Training to Care for Limited English Proficient Patients and Provision of Interpreter Services at U.S. Dental School Clinics. J Dent Educ. 2017;81(2):169–177. | Survey, 325 students | Aim: to survey dental students about their clinical experience with LEP patients, the interpreter resources available at their dental school clinics, and the extent of instruction on these topics. Key findings: The majority of responding students (56.3%) indicated there was some form of interpreter services available on their clinic floor. 43.7% indicated their dental school clinic lacked formal interpreter services, and 35.4% reported that their institution did not take language into account when assigning LEP patients to student clinicians. 37.2% reported that no curricular content pertaining to LEP patients was available. | Yes | Yes | Yes | No | Yes | Can’t tell | Yes | Yes | Yes |
| 20 | Omoruyi EA, Dunkle J, Dendy C, McHugh E, Barratt MS. Cross Talk: Evaluation of a Curriculum to Teach Medical Students How to Use Telephone Interpreter Services. Acad Pediatr. 2018;18(2):214–219. | Web-based training/ pre-post test, 176 students | Aim: to determine if training improves self-reported competency. Key findings: Self-assessment showed that students improved competency in telephone interpretation use. Comparing Average Scores of Audio Files in non-curriculum and curriculum groups, there was higher scores in the curriculum students. | Yes | Yes | Yes | No | No | Can’t tell | Yes | Yes | Yes |
| 21 | Mazori AY, Maron MI, Osterbur ML Badhey, et al. Enhancing Medical Student-Interpreter Collaboration in an Urban Free Clinic. Fam Med. 2019;51(7):593–597. | Randomized control trial, 76 trainees (36 control, 40 intervention) | Aim: to explore the effectiveness of working with interpreters in a clinic. Key findings: The students that had the intervention training scored higher by the interpreters since they were more likely to ask patient 1 question at a time, listen to interpreter without unnecessary interruption, and speak in short/simple sentences with pauses. | Yes | Yes | Yes | Yes | Yes | Can’t tell | Yes | Yes | Yes |
| 22 | Kalet A, Gany F, Senter L. Working with interpreters: an interactive Web-based learning module. Acad Med. 2002;77(9):927. | Web-based training/ pre-post test, 160 students, no control group | Hypothesis: what is the effectiveness of a web-based module aimed at teaching students effective strategies for working with interpreters and diverse patient populations? Students improved by 20% on MCQ post-test and 86% of students were satisfied with learning experience and acquired new knowledge. | Yes | Yes | Yes | No | Yes | Can’t tell | Yes | Yes | Yes |
| 23 | Kalet AL, Mukherjee D, Felix K, et al. Can a web-based curriculum improve students’ knowledge of, and attitudes about, the interpreted medical interview? J Gen Intern Med. 2005;20(10):929–934. | Web-based training/ pre-post test, 640 students, no control group | Aim: to develop and evaluate a web-based curriculum to introduce first-year students to the knowledge and attitudes necessary for working with LEP patients through interpreters. Key findings: Tested knowledge questions improved from 42% to 64% correct pre- to post- test. Pre- and post-module attitude and belief scores were considered statistically significantly improved | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| 24 | Lie D, Bereknyei S, Kalet A, Braddock C 3rd. Learning outcomes of a web module for teaching interpreter interaction skills to pre-clerkship students. Fam Med. 2009;41(4):234–235. | Web-based module, pre-post test, control/intervention groups, 3 medical schools, 304 students | Aim: to evaluate the impact of training in working with LEP patients through interpreters. Key findings: Post-test MCQ test results are improved in those that took part in an online interpreter interaction skills module. However, clinical skills score did not correlate with the magnitude of knowledge gain. | Yes | Yes | Yes | No | Yes | Can’t tell | Yes | Yes | Yes |
| 25 | Fung CC, Lagha RR, Henderson P, Gomez AG. Working with interpreters: how student behavior affects quality of patient interaction when using interpreters. Med Educ Online. 2010;15:10.3402/meo.v15i0.511. | Workshop training, 152 students, OSCE examination, no control group | Aim: to evaluate the effectiveness of a workshop. Key findings: Students did well in managing the interpreted encounter, but had the biggest issue preparing the encounter in that the biggest failed items were arranging the patient and interpreter as they were taught and ensuring confidentiality. | Yes | Yes | Yes | No | No | Can’t tell | Yes | Yes | Yes |
| 26 | Lie DA, Bereknyei S, Vega CP. Longitudinal development of medical students’ communication skills in interpreted encounters. Educ Health (Abingdon). 2010;23(3):466. | One year training, clinical performance assessment and questionnaires, no control group, 192 students | Hypothesis: students will show improvement in objective ratings of communication skills in the interpreted encounter over one year of clinical training. Performance as rated by the patient did not change significantly (after a year of clinical training) for seven items. The ratings by the interpreter improved in two behaviors of setting the stage and introductions. However, performance was worse in some behaviors. | Yes | Yes | Yes | No | No | Can’t tell | Yes | Yes | Yes |
| 27 | Hasbún Avalos O, Pennington K, Osterberg L. Revolutionizing volunteer interpreter services: an evaluation of an innovative medical interpreter education program. J Gen Intern Med. 2013;28(12):1589–1595. | 6 months training, pre-post evaluation, written and oral assessment, 38 students, no control group | Aim: to evaluate the effectiveness of a training program. Key findings: Self-assessed knowledge, skills, and confidence were noted but the value of these changes was unclear. Written testing knowledge of the roles and skills of interpreters needed for proper medical interpretation improved. More students passed oral interpretation exams (a pass was being able to maintain the intended message) after training. This is the highest quality measurement of the program in the paper. | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes |
| 28 | Bansal, A, Swann, J & Smithson, WH 2014, “Using professional interpreters in undergraduate medical consultation skills teaching”, Advances in medical education and practice, vol. 5, pp. 439–450. | Training, Survey, self-reported questionnaires completed by students and GP tutors, 274 students and 8 GP tutors | Aim: to evaluate the effectiveness of training. Key findings: Students’ perceived confidence in consulting increased with interpreter training. GP tutor explained that training helped themselves by filling a gap in their own skills to be used in practice, and the training was helpful and interactive for students | Yes | Yes | No | No | No | No | Can’t tell | Yes | No |
| 29 | Quick KK, Selameab T, Woll A, Mazzei C, Miller JL. Creating and Evaluating Skills-Based Training in Working with Spoken-Language Interpreters for Oral Health Professions Students. J Dent Educ. 2019;83(6):645–653. | Workshop training, pre-post test, 294 students, intervention and control groups, 1 focus group with 11 students | Aim: to evaluate the effectiveness of a training program in terms of trainees’ familiarity and confidence. Both familiarity and confidence in working with LEP patients increased significantly after the training. | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes |
| 30 | McEvoy M, Santos MT, Marzan M, Green EH, Milan FB. Teaching medical students how to use interpreters: a three year experience. Med Educ Online. 2009;14:12. | Training, pre-post test and feedback, 110 students, no control group | Aim: to evaluate the effectiveness of training. Key findings: The study showed that the session was effective in increasing students’ perceived efficacy for using the skills to communicate with a patient with LEP, give instructions to an untrained interpreter, and access a telephone interpreter. | Yes | Yes | Yes | No | No | Can’t tell | No | Yes | Yes |
| 31 | Ikram UZ, Essink-Bot ML, Suurmond J. How we developed an effective e-learning module for medical students on using professional interpreters. Med Teach. 2015;37(5):422–427. | E-learning training module, pre-post test, 281 students, no control group | Aim: to develop an effective e-learning module for medical students on using professional interpreters. Key findings: Professional interpreter use knowledge and self-efficacy increased after completing a teaching e-module. | Yes | Yes | Yes | No | No | Can’t tell | Yes | Yes | Yes |
| 32 | Marion GS, Hildebrandt CA, Davis SW, Marín AJ, Crandall SJ. Working effectively with interpreters: a model curriculum for physician assistant students. Med Teach. 2008;30(6):612–617. | Training, 12-item check list and student feedback, 96 students, no control group, no pre-post test | Aim: to see if physician assistant students could effectively use interpreters to communicate with Spanish-speaking patients after implementation of a cultural competency and medical Spanish curriculum. Key findings: Based on anevaluation of student performance using a 12-item checklist and student feedback on the curriculum, the enhancements were proven successful and feasible | Yes | No | Yes | No | No | Yes | Yes | Yes | No |
| 33 | Jacobs EA, Diamond LC, Stevak L. The importance of teaching clinicians when and how to work with interpreters. Patient Educ Couns. 2010;78(2):149–153. | Training, 72 students, pre-post test, no control group | Aim: to describe the importance of teaching students when and how to overcome language barriers in clinical practice, provide an example of a curriculum for teaching on this topic, and outline the critical issues that must be addressed in this type of teaching. Key findings: Students improved in working with an interpreter, were significantly more likely to endorse that it is easy to work with interpreters, that cultural competency is necessary to provide high quality health care, that the information obtained through interpreters is accurate, and that they will not find it frustrating and more rewarding to care for limited English proficient (LEP) patients. | Yes | Yes | Yes | No | No | Can’t tell | Yes | Yes | Yes |
| 34 | Aitken, G 2019, “Medical Students as Certified Interpreters”, AMA journal of ethics, vol. 21, no. 3, pp. E232–E238. | Descriptive paper | Aim: to look at the interpreter certification program created at a US University to certify medical students as interpreters themselves. Students serving as interpreters gained more experience/exposure, and built cultural competency. On the other hand, they found it hard to separate roles as clinicians vs interpreters. | Yes | Yes | Yes | N/A | N/A | N/A | Yes | Yes | Yes |
| 35 | Mihalic AP, Morrow JB, Long RB & Dobbie AE 2010, “A validated cultural competence curriculum for US pediatric clerkships”, Patient Education & Counseling, vol. 79, no. 1, pp. 77–82. | Survey, self-reported, 149 students, 1 focus group | Aim: to evaluate curriculum in cultural competence. Key findings: improved skills in working with interpreters (90%), improved skills in cross-cultural communication (82%), increased knowledge of racial and ethnic disparities (89%), increased their knowledge of core cultural issues and their impact on health care (91%), and increased their level of awareness and understanding of the culture of medicine (91%). Cultural knowledge test became validated in achieving target reliability of 0.7 for combined pre- and post-tests. Score gain of 17% considered significant | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes |
| 36 | Pelaez AF, Ramirez SI, Valdes Sanchez C, et al. Implementing a medical student interpreter training program as a strategy to developing humanism. BMC Med Educ. 2018;18(1):141. | Training, no control, pre-post surveys, 80 students. | Aim: to address issues by implementing a medical interpretation training program with bilingual medical students with the goal of creating a sustainable language access program and increasing students’ communication skills and empathy, potentially resulting in more humanistic medical professionals. Key findings: After training, 98% felt more confident about interpreting, 87.5% felt more empathy for LEP patients. Program well received by students since 100% recommended training | Yes | Yes | Yes | No | No | Can’t tell | Yes | Yes | Yes |
References
- Alizadeh, S.; Chavan, M. Cultural competence dimensions and outcomes: A systematic review of the literature. Health Soc. Care Community 2016, 24, 117–130. [Google Scholar] [CrossRef] [Green Version]
- Betancourt, J.; Green, A.R.; Carrillo, J.E.; Ananeh-Firempong, O. Defining cultural competence: A practical framework for addressing racial/ethnic disparities in health and health care. Public Health Rep. 2003, 118, 293–302. [Google Scholar] [CrossRef]
- Constantinou, C.S.; Papageorgiou, A.; Andreou, P.; McCrorie, P. How to integrate cultural competence in medical curricula: Learning from a new medical programme. MedEdPublish 2020, 9. [Google Scholar] [CrossRef] [Green Version]
- Constantinou, C.S.; Papageorgiou, A.; Samoutis, G.; McCrorie, P. Acquire, apply, and activate knowledge: A pyramid model for teaching and integrating cultural competence in medical curricula. Patient Educ. Couns. 2018, 101, 1147–1151. [Google Scholar] [CrossRef] [PubMed]
- Borrell-Carrió, F.; Suchman, A.L.; Epstein, R.M. The Biopsychosocial Model 25 Years Later: Principles, Practice, and Scientific Inquiry. Ann. Fam. Med. 2004, 2, 576–582. [Google Scholar] [CrossRef] [Green Version]
- Horvat, L.; Horey, D.; Romios, P.; Kis-Rigo, J. Cultural competence education for health professionals. Cochrane Database Syst. Rev. 2014, CD009405. [Google Scholar] [CrossRef]
- Renzaho, A.M.N.; Romios, P.; Crock, C.; Sonderlund, A.L. The effectiveness of cultural competence programs in ethnic minority patient-centered health care--a systematic review of the literature. Int. J. Qual. Health Care 2013, 25, 261–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hudelson, P.; Dogra, N.; Hendrickx, K.; Verdonk, P.; Essink-Bot, M.-L.; Suurmond, J. The challenges of integrating cultural competence into undergraduate medical curricula across Europe: Experience from the C2ME “Culturally competent in medical education” project. MedEdPublish 2016, 5. [Google Scholar] [CrossRef] [Green Version]
- Sorensen, J.; Jervelund, S.S.; Norredam, M.; Kristiansen, M.; Krasnik, A. Cultural competence in medical education: A questionnaire study of Danish medical teachers’ perceptions of and preparedness to teach cultural competence. Scand. J. Public Health 2017, 45, 153–160. [Google Scholar] [CrossRef] [PubMed]
- White, J.; Plompen, T.; Tao, L.; Micallef, E.; Haines, T. What is needed in culturally competent healthcare systems? A qualitative exploration of culturally diverse patients and professional interpreters in an Australian healthcare setting. BMC Public Health 2019, 19, 1096. [Google Scholar] [CrossRef] [PubMed]
- Flores, G. The Impact of Medical Interpreter Services on the Quality of Health Care: A Systematic Review. Med. Care Res. Rev. 2005, 62, 255–299. [Google Scholar] [CrossRef] [PubMed]
- Brandl, E.J.; Schreiter, S.; Schouler-Ocak, M. Are Trained Medical Interpreters Worth the Cost? A Review of the Current Literature on Cost and Cost-Effectiveness. J. Immigr. Minor. Health 2020, 22, 175–181. [Google Scholar] [CrossRef]
- Himmelstein, J.; Wright, W.S.; Wiederman, M.W. U.S. medical school curricula on working with medical interpreters and/or patients with limited English proficiency. Adv. Med. Educ. Pract. 2018, 9, 729–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrari, R. Writing narrative style literature reviews. Med. Writ. 2015, 24, 230–235. [Google Scholar] [CrossRef]
- Baethge, C.; Goldbeck-Wood, S.; Mertens, S. SANRA—A scale for the quality assessment of narrative review articles. Res. Integr. Peer Rev. 2019, 4, 5. [Google Scholar] [CrossRef] [Green Version]
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med. Res. Methodol. 2008, 8, 45. [Google Scholar] [CrossRef] [Green Version]
- Critical Appraisal Skills Programme. CASP (Systematic Review, Qualitative Studies) Checklist. Available at: CASP CHECKLISTS—CASP—Critical Appraisal Skills Programme (casp-uk.net); CASP: Oxford, UK, 2019. [Google Scholar]
- Itaya, L.E.; Glassman, P.; Gregorczyk, S.; Bailit, H.L. Dental School Patients with Limited English Proficiency: The California Experience. J. Dent. Educ. 2009, 73, 1055–1064. [Google Scholar] [CrossRef]
- Simon, L.; Hum, L.; Nalliah, R. Training to care for limited English proficient patients and provision of interpreter services at US dental school clinics. J. Dent. Educ. 2017, 81, 169–177. [Google Scholar] [CrossRef]
- Omoruyi, E.A.; Dunkle, J.; Dendy, C.; McHugh, E.; Barratt, M.S. Cross Talk: Evaluation of a Curriculum to Teach Medical Students How to Use Telephone Interpreter Services. Acad. Pediatr. 2018, 18, 214–219. [Google Scholar] [CrossRef]
- Mazori, A.; Maron, M.; Osterbur, M.; Santos, D.; Marco, V.; Lin, J.; Cortijo, A.; Nosal, S.; Schoenbaum, E. Enhancing Medical Stu-dent-Interpreter Collaboration in an Urban Free Clinic. Fam. Med. 2019, 51, 593–597. [Google Scholar] [CrossRef] [Green Version]
- Kalet, A.; Gany, F.; Senter, L. Working with interpreters: An interactive Web-based learning module. Acad. Med. 2002, 77, 927. [Google Scholar] [CrossRef]
- Kalet, A.L.; Mukherjee, D.; Felix, K.; Steinberg, S.E.; Nachbar, M.; Lee, A.; Changrani, J.; Gany, F. Can a web-based curriculum improve students’ knowledge of, and attitudes about, the interpreted medical interview? J. Gen. Intern. Med. 2005, 20, 929–934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lie, D.; Bereknyei, S.; Kalet, A.; Braddock, C., 3rd. Learning outcomes of a web module for teaching interpreter interaction skills to pre-clerkship students. Fam. Med. 2009, 41, 234–235. [Google Scholar] [PubMed]
- Fung, C.-C.; Lagha, R.R.; Henderson, P.; Gomez, A.G. Working with interpreters: How student behavior affects quality of patient interaction when using interpreters. Med. Educ. Online 2010, 15, 5151. [Google Scholar] [CrossRef] [Green Version]
- Lie, D.A.; Bereknyei, S.; Vega, C.P. Longitudinal development of medical students’ communication skills in interpreted en-counters. Educ. Health 2010, 23, 466. [Google Scholar]
- Avalos, O.H.; Pennington, K.; Osterberg, L. Revolutionizing Volunteer Interpreter Services: An Evaluation of an Innovative Medical Interpreter Education Program. J. Gen. Intern. Med. 2013, 28, 1589–1595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bansal, A.; Swann, J.; Smithson, W. Using professional interpreters in undergraduate medical consultation skills teaching. Adv. Med. Educ. Pract. 2014, 5, 439–450. [Google Scholar] [CrossRef] [Green Version]
- Quick, K.K.; Selameab, T.; Woll, A.; Mazzei, C.; Miller, J.L. Creating and Evaluating Skills-Based Training in Working with Spoken-Language Interpreters for Oral Health Professions Students. J. Dent. Educ. 2019, 83, 645–653. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, M.; Santos, M.T.; Marzan, M.; Green, E.H.; Milan, F.B. Teaching medical students how to use interpreters: A three year experience. Med. Educ. Online 2009, 14, 4507. [Google Scholar] [CrossRef]
- Ikram, U.Z.; Essink-Bot, M.-L.; Suurmond, J. How we developed an effective e-learning module for medical students on using professional interpreters. Med. Teach. 2014, 37, 422–427. [Google Scholar] [CrossRef]
- Marion, G.S.; Hildebrandt, C.A.; Davis, S.W.; Marín, A.J.; Crandall, S.J. Working effectively with interpreters: A model curriculum for physician assistant students. Med. Teach. 2008, 30, 612–617. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, E.A.; Diamond, L.C.; Stevak, L. The importance of teaching clinicians when and how to work with interpreters. Patient Educ. Couns. 2010, 78, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Aitken, G. Medical Students as Certified Interpreters. AMA J. Ethics 2019, 21, 232–238. [Google Scholar]
- Mihalic, A.P.; Morrow, J.B.; Long, R.B.; Dobbie, A.E. A validated cultural competence curriculum for US pediatric clerkships. Patient Educ. Couns. 2010, 79, 77–82. [Google Scholar] [CrossRef]
- Pelaez, A.F.V.; Ramirez, S.I.; Sanchez, C.V.; Abusharar, S.P.; Romeu, J.C.; Carmichael, C.; Bascoy, S.; Baron, R.; Pichardo-Lowden, A.; Albarracin, N.; et al. Implementing a medical student interpreter training program as a strategy to developing humanism. BMC Med. Educ. 2018, 18, 141. [Google Scholar]
Figure 1.
Flowchart on the literature selection process based on guidelines by Ferrari (2015).

Figure 2.
Longitudinal integration of the use of interpreters in medical education.


{kind=link}
{kind=link}
Table 1.
Inclusion and exclusion criteria.
| Inclusion | Peer-reviewed articles or chapters Theses and dissertations Literature reviews Conference papers Editorials Books or textbooks All of the above, which include or discuss medical students, medical or health care curricula Published in English Period of publication: 2000–2020 |
| Exclusion | Peer review articles, chapters, thesis dissertations, conference papers, editorials, books and textbooks which do not include or discuss medical students, medical or health care curricula Any of the above publications published before 2000 Published in languages other than English |
Table 2.
Organization of search questions.
| Utilization | Are interpreters used in medical education as part of the curriculum? If yes how, where, and when are they used? What is the effect of the use of interpreters on the quality of medical education? How confident are medical students in using interpreters in medical education? |
| Perspectives | What are the patients’ perspectives when they see medical students and interpreters? What are the students’ feelings when being in clinical placements where they do not speak the language of their patients? What are the perspectives of students, interpreters, health care providers (e.g., clinics, hospitals, health care facilities, etc.), and medical educators? |
| Impact | Is there any research done looking at patient outcomes when medical students use interpreters in their clinical placements? What are students learning from the use of interpreters during their medical education? What is the impact of using interpreters in clinical placements/medical education on patients? |
| Barriers/Enablers | What are the facilitators and challenges for using interpreters in medical education for medical students, their supervisors, and the patients? |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Constantinou, C.S.; Ng, A.T.; Becker, C.B.; Zadeh, P.E.; Papageorgiou, A. The Use of Interpreters in Medical Education: A Narrative Literature Review. Societies 2021, 11, 70. https://0-doi-org.brum.beds.ac.uk/10.3390/soc11030070
AMA Style
Constantinou CS, Ng AT, Becker CB, Zadeh PE, Papageorgiou A. The Use of Interpreters in Medical Education: A Narrative Literature Review. Societies. 2021; 11(3):70. https://0-doi-org.brum.beds.ac.uk/10.3390/soc11030070
Chicago/Turabian StyleConstantinou, Costas S., Andrew Timothy Ng, Chase Beverley Becker, Parmida Enayati Zadeh, and Alexia Papageorgiou. 2021. "The Use of Interpreters in Medical Education: A Narrative Literature Review" Societies 11, no. 3: 70. https://0-doi-org.brum.beds.ac.uk/10.3390/soc11030070
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.