Analysis of the Impact of China’s Hierarchical Medical System and Online Appointment Diagnosis System on the Sustainable Development of Public Health: A Case Study of Shanghai


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Patient Selection Model
2.1. Basic Hypotheses of the Model
2.1.1. Hypothesis about Ideal Cities [39,40,41]
- (1)
- The distribution of residents in cities is evenly distributed.
- (2)
- The time required for residents to move from one place to another in an urban area is completely proportional to the linear distance between the two places.
- (3)
- The prevalence rate of residents in different areas is the same.
2.1.2. Hypothesis about the Medical Systems [42,43,44]
- (1)
- The medical institutions of the same level have the same service capacity—cure rate, cure time, hospitalization speed, service radius, etc.
- (2)
- All areas of the city are covered by the services of at least one grassroots medical institution or one superior medical institution.
- (3)
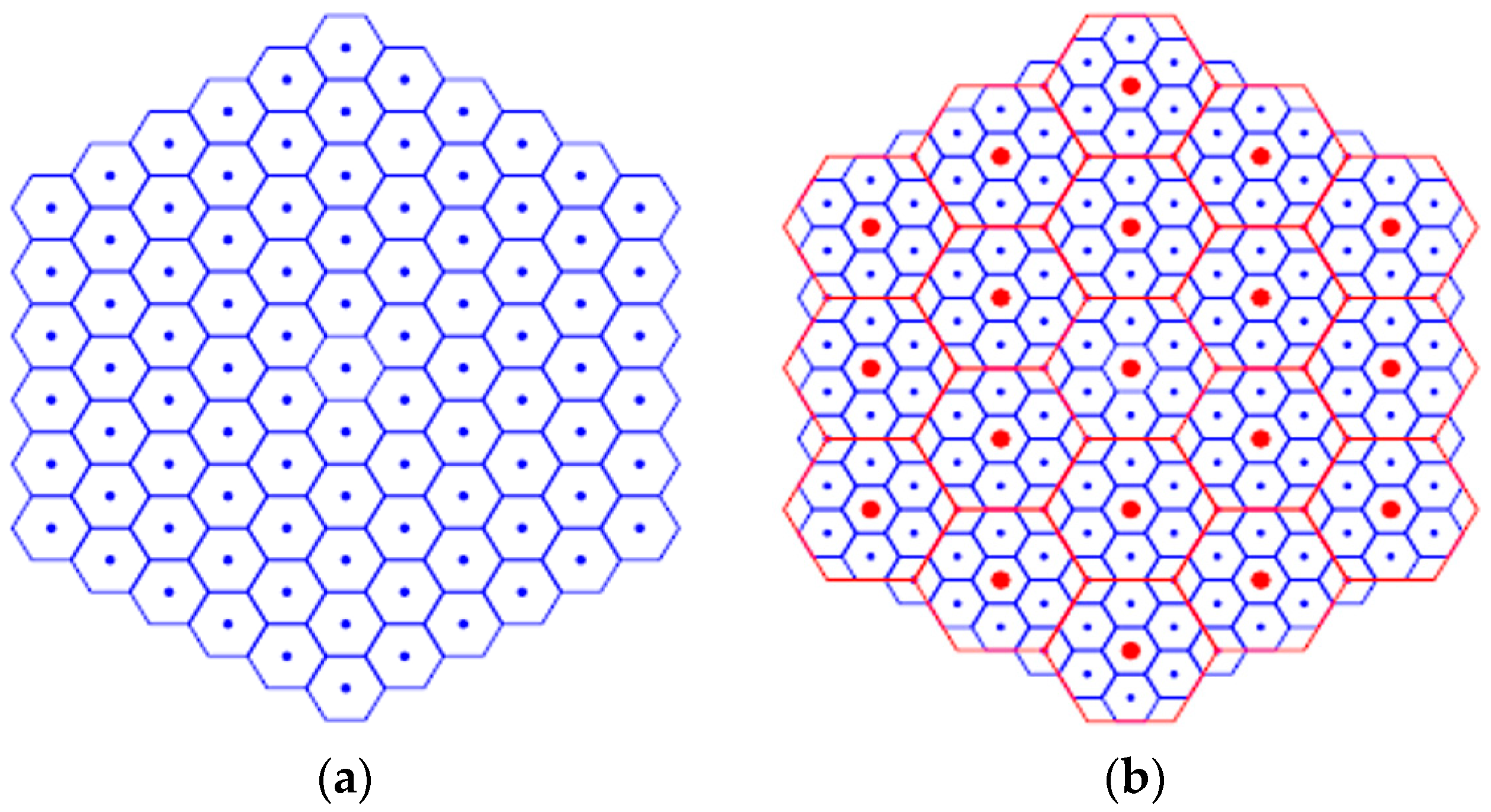
- The location of the superior medical institution can be nested into the location of the subordinate medical institution and the ratio of the two is 1:8.
2.1.3. Hypothesis about the Rules of Patients’ Medical Service-Seeking Choice [47,48,49]
- (1)
- After the patient becomes ill, according to his (her) own region, the choice of whether or not to seek medical treatment in the nearest region should be made in line with the medical treatment experience among other residents in the region.
- (2)
- After selecting the medical treatment location, the patient can choose whether to make an online appointment or not.
- (3)
- The patient cannot know the healing capability of the subordinate medical institutions for his (her) own disease but can feel whether he (she) is cured.
- (4)
- The patient suffers from a mild but urgent disease, that is, the condition will not change in a short time, but the patient hopes to be cured immediately after the disease.
2.1.4. Hypothesis about the Treatment Rules of Medical Institutions [50,51,52]
- (1)
- The cure rate of the subordinate medical institutions was P and , and there was no misdiagnosis rate.
- (2)
- If the referral is supported by the medical institution, and the referral patient has certain priority.
2.2. Analysis of the Patients’ Medical Service-Seeking Behaviors
2.2.1. The Medical Treatment System Does Not Support Referral or Online Appointment
2.2.2. The Medical Treatment System Does Not Support Referral but Supports Online Appointments
2.2.3. The Medical Treatment System Supports Referral but Does Not Support Online Appointments
2.2.4. The Medical Treatment System Supports Referral and Online Appointment
2.3. Basic Conclusions of the Model
- (1)
- Because of the planned use of the existing medical resources, online appointments greatly increases the time utility of patients and play a decisive role in alleviating the high cost of patients’ medical time. At the same time, when medical institutions begin to use online appointments, patients will use them to increase their own time utility (with some guidance).
- (2)
- Only when the subordinate medical institutions have a certain cure rate for most diseases can the hierarchical medical treatment continuously improve the patients’ acceptance. However, because hierarchical medical treatment can make more medical resources be used, the ultimate time utility of hierarchical medical treatment is higher than that of online appointments alone.
- (3)
- Both online appointments and hierarchical medical treatment can reduce the time cost and increase the time utility of patients, but there is a certain competitive relationship between them from a certain perspective. Therefore, we need to further analyze the relationship between them through cellular automata model and policy simulation.
3. Simulations and Discussions
3.1. Basic Assumptions
- (1)
- Generation rules for patients. Select an appropriate number of patients per unit time , and use the average distribution to simulate the fluctuation of the population. After selecting the number of patients in a specific unit time according to the random number, the patient’s location information is assigned randomly . Next, read the probability of medical treatment strategy of patients in the cell through the location information. Then, through the probability of medical strategy, determine a specific patient after the onset of the medical strategy.
- (2)
- Movement rules for patients. Because the condition of the patient in this paper is not enough for emergency treatment, when the time evolves to the normal operating hours of the medical institution, the patient can go to the medical institution according to his (her) own treatment strategy. In this process, the time required for the patient to move is the required distance S divided by the urban traffic speed , and then the value is rounded up or down plus one so that the data type of the time is always an integer.
- (3)
- Medical treatment rules. In the process of normal operation of the medical institution, it sorts the patients according to the preset medical system. Then according to the order, the patient with higher priority are diagnosed and treated according to his (her) own diagnosis and treatment speed. Here we assume that a time step in a subordinate medical institution can diagnose patients, and a time step in a superior medical institution can diagnose patients. After the patients are treated, a fixed time is added as the treatment duration. When a patient is treated in a subordinate medical institution, it is necessary to randomly determine whether the patient needs to be transferred through the treatment rate preset by the subordinate medical institution. A patient who needs to be referred goes to a superior medical institution through the previous movement rule. When the medical institution is about to close, we agree that the medical institution will guarantee the treatment of a very small number of patients who are still in the hospital by extending the clinic or transferring them to the emergency department. By doing this, we can prevent these patients going home and then returning to the medical institution for treatment the next day, resulting in a lower time utility, thus misleading the results.
- (4)
- The evolution rule of medical treatment strategy for the patient in the cell. The healing patient needs to compare the time cost of his (her) own medical treatment process with the time cost of all patients in the social treatment process to judge the quality of his(her) own strategy. The evolutionary s intensity of the patient’s medical strategy in the cell can be obtained by multiplying the time cost of the patient’s strategy with the strategy modification factor.
3.2. Benchmark Data
3.3. Simulation Results
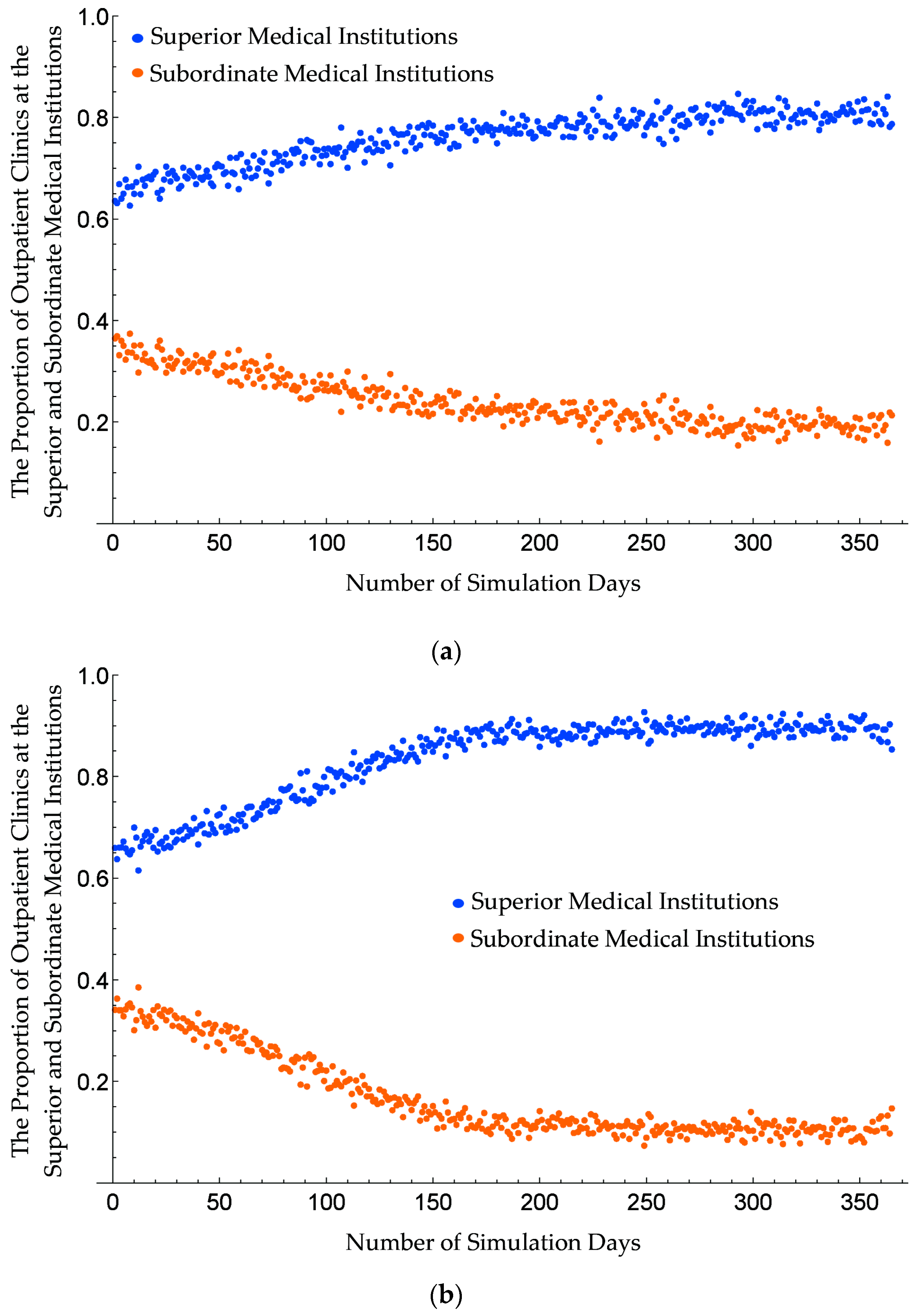
- The comparison between Figure 4a and Figure 5a shows that under the medical treatment system that does not support referral or online appointments, patients tend to go directly to the superior medical institution, resulting in a decrease in the outpatient proportion of the subordinate medical institution. However, when the length of medical treatment is equal to the duration of compulsory treatment divided by the cure rate of the subordinate medical institution, the time effectiveness of patients going to the two-level medical institutions begins to be the same, and the rating rate does not change much at this time.
- The comparison between Figure 4b and Figure 5b shows that under the system of supporting online appointments but not supporting referral, the implementation of an appointment system can effectively reduce the waiting time of residents, thus reducing the time cost of residents. However, due to the reduction of the waiting time of residents, the advantage of the former short waiting time of subordinate medical institutions will no longer appear, which leads to the lowest limit of the rating rate allowed by the procedure.
- The comparison between Figure 4c and Figure 5c shows that under the medical treatment system that support referral but does not support online appointments, due to the existence of referral mechanism, the proportion of outpatient clinics in the subordinate medical institution has been greatly increased, thus releasing the medical capability of the subordinate medical institution and reducing the time for patients to seek medical treatment to a certain extent. However, due to the absence of an appointment mechanism, a large amount of waiting time makes it difficult for the length of medical treatment of patient to continue to decline.
3.4. Results Analysis
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- National Health Commission of the People’s Republic of China. Statistical Bulletin on the Development of China’s Health Care Industry in 2018; National Health Commission of the People’s Republic of China: Beijing, China, 2019. Available online: http://www.nhc.gov.cn/guihuaxxs/s10748/201905/9b8d52727cf346049de8acce25ffcbd0.shtml (accessed on 24 October 2019).
- The State Council of People’s Republic of China. Deepen the Reform of China’s Medical and Health System; The State Council of People’s Republic of China: Beijing, China, 2009. Available online: http://www.gov.cn/ztzl/ygzt/ (accessed on 24 October 2019).
- Cinaroglu, S.; Baser, O. The relationship between medical innovation and health expenditure before and after health reform. Heal. Policy Technol. 2018, 7, 379–387. [Google Scholar] [CrossRef]
- Liang, J.; Zheng, X.; Chen, Z.; Dai, S.; Xu, J.; Ye, H.; Zhang, Z.; Ge, F.; Lei, J. The experience and challenges of healthcare-reform-driven medical consortia and Regional Health Information Technologies in China: A longitudinal study. Int. J. Med. Inform. 2019, 131, 103954. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zhang, Y. Discussing the Relationship between Developing Health Service Industry and Health System Reform. Chin. Heal. Econ. 2014, 33, 5–7. [Google Scholar]
- Office of the State Council of People’s Republic of China. Guidance on Promoting the Construction of Hierarchical Medical System; Office of the State Council of People’s Republic of China: Beijing, China, 2015. Available online: http://www.gov.cn/xinwen/2015-09/11/content_2929789.htm?mType=Group (accessed on 24 October 2019).
- Fang, P.; Han, Q.; Xie, Q.; Xiao, F.U.; Xia, L.I.; Tiantian, H.U. Urban secondary hospitals and the hierarchical medical system: Development strategy study. Chin. J. Hosp. Adm. 2016, 32, 500–502. [Google Scholar]
- Zeng, J.; Shi, L.; Zou, X.; Chen, W.; Ling, L. Rural-to-urban migrants’ experiences with primary care under different types of medical institutions in Guangzhou, China. PLoS ONE 2015, 10, e0140922. [Google Scholar] [CrossRef]
- Zhan, Q.; Wang, Y.L.; Chen, X. Evaluation of antibacterial use in outpatients of township and community primary medical institutions in a district of Sichuan Province, China. J. Glob. Antimicrob. Resist. 2019, 19, 201–206. [Google Scholar] [CrossRef]
- Chen, Z.; Barros, C.P.; Hou, X. Has the medical reform improved the cost efficiency of Chinese hospitals? Soc. Sci. J. 2016, 53, 510–520. [Google Scholar] [CrossRef]
- Lu, C.; Zhang, Z.; Lan, X. Impact of China’s referral reform on the equity and spatial accessibility of healthcare resources: A case study of Beijing. Soc. Sci. Med. 2019, 235, 112386. [Google Scholar] [CrossRef]
- Liu, X.; Jian, X. Calling a stage-based treatment model for chronic liver diseases in China mainland. Ann. Hepatol. 2019, 09, 007. [Google Scholar] [CrossRef]
- Leng, W.; Yang, J.; Fan, X.; Sun, Y.; Xu, H.; Gao, X.; Wang, Y.; Li, W.; Xu, Y.; Han, Y.; et al. Contemporary invasive management and in-hospital outcomes of patients with non–ST-segment elevation myocardial infarction in China: Findings from China Acute Myocardial Infarction (CAMI) Registry. Am. Heart J. 2019, 215, 1–11. [Google Scholar] [CrossRef]
- Li, L.; Fu, H. China’s health care system reform: Progress and prospects. Int. J. Health Plan. Manag. 2017, 32, 240–253. [Google Scholar] [CrossRef] [PubMed]
- Yip, W.; Fu, H.; Chen, A.T.; Zhai, T.; Jian, W.; Xu, R.; Pan, J.; Hu, M.; Zhou, Z.; Chen, Q.; et al. 10 years of health-care reform in China: Progress and gaps in Universal Health Coverage. Lancet 2019, 394, 1192–1204. [Google Scholar] [CrossRef]
- Wu, H.; Lu, N. Online written consultation, telephone consultation and offline appointment: An examination of the channel effect in online health communities. Int. J. Med. Inform. 2017, 107, 107–119. [Google Scholar] [CrossRef] [PubMed]
- Hao, H.; Zhang, K.; Wang, W.; Gao, G. A tale of two countries: International comparison of online doctor reviews between China and the United States. Int. J. Med. Inform. 2017, 99, 37–44. [Google Scholar] [CrossRef]
- Xiao, Q.; Luo, L.; Zhao, S.; Ran, X.; Feng, Y. Online appointment scheduling for a nuclear medicine department in a Chinese hospital. Comput. Math. Methods Med. 2018, 2018, 5148215. [Google Scholar] [CrossRef]
- Ministry of Health of People’s Republic of China. Progress in the Appointment of Medical Services in Public Hospitals in China; Ministry of Health of People’s Republic of China: Beijing, China, 2011. Available online: http://www.gov.cn/gzdt/2011-07/12/content_1905090.htm (accessed on 24 October 2019).
- Hu, Y.; Pratt, C.B. Grounding civic engagement in strategic communication for China’s public-health programs: Air-quality campaigns as a case study. Public Relat. Rev. 2017, 43, 461–467. [Google Scholar] [CrossRef]
- Yang, W.; Yuan, G.; Han, J. Is China’s air pollution control policy effective? Evidence from Yangtze River Delta cities. J. Clean. Prod. 2019, 220, 110–133. [Google Scholar] [CrossRef]
- Yuan, G.; Yang, W. Study on optimization of economic dispatching of electric power system based on Hybrid Intelligent Algorithms (PSO and AFSA). Energy 2019, 183, 926–935. [Google Scholar] [CrossRef]
- Lu, Z.; Chen, H.; Hao, Y.; Wang, J.; Song, X.; Mok, T.M. The dynamic relationship between environmental pollution, economic development and public health: Evidence from China. J. Clean. Prod. 2017, 166, 134–147. [Google Scholar] [CrossRef]
- Yang, W.; Li, L. Analysis of Total Factor Efficiency of Water Resource and Energy in China: A Study Based on DEA-SBM Model. Sustainability 2017, 9, 1316. [Google Scholar] [CrossRef]
- Li, L.; Yang, W. Total Factor Efficiency Study on China’s Industrial Coal Input and Wastewater Control with Dual Target Variables. Sustainability 2018, 10, 2121. [Google Scholar] [CrossRef]
- Bian, S.; Guo, Q.; Wang, X. Construction of senior service system in the context of a healthy China. Glob. Heal. J. 2018, 2, 28–34. [Google Scholar] [CrossRef]
- Yang, W.; Li, L. Efficiency evaluation of industrial waste gas control in China: A study based on data envelopment analysis (DEA) model. J. Clean. Prod. 2018, 179, 1–11. [Google Scholar] [CrossRef]
- Weissman, G.E. Hierarchical Condition Categories for Pulmonary Diseases: Population Health Management and Policy Opportunities. Chest 2019, 155, 868–873. [Google Scholar] [CrossRef]
- Qiu, S.; Alizadeh, A.; Dooley, L.M.; Zhang, R. The effects of authentic leadership on trust in leaders, organizational citizenship behavior, and service quality in the Chinese hospitality industry. J. Hosp. Tour. Manag. 2019, 40, 77–87. [Google Scholar] [CrossRef]
- Gao, H.; Yang, W.; Yang, Y.; Yuan, G. Analysis of the Air Quality and the Effect of Governance Policies in China’s Pearl River Delta, 2015–2018. Atmosphere 2019, 10, 412. [Google Scholar] [CrossRef]
- Şahin, T.; Ocak, S.; Top, M. Analytic hierarchy process for hospital site selection. Heal. Policy Technol. 2019, 8, 42–50. [Google Scholar] [CrossRef]
- Yuan, G.; Yang, W. Evaluating China’s Air Pollution Control Policy with Extended AQI Indicator System: Example of the Beijing-Tianjin-Hebei Region. Sustainability 2019, 11, 939. [Google Scholar] [CrossRef]
- Wang, Y.; Sun, L.; Hou, J. Hierarchical Medical System Based on Big Data and Mobile Internet: A New Strategic Choice in Health Care. JMIR Med. Inf. 2017, 5, e22. [Google Scholar] [CrossRef]
- Pan, X.; Song, J.; Zhang, B. Patient admission control in a hierarchical healthcare system. IFAC-Pap. OnLine 2017, 50, 4636–4641. [Google Scholar] [CrossRef]
- Ren, P.; Xu, Z.; Liao, H.; Zeng, X. A thermodynamic method of intuitionistic fuzzy MCDM to assist the hierarchical medical system in China. Inf. Sci. 2017, 420, 490–504. [Google Scholar] [CrossRef]
- Zheng, Y.; He, Y.; Xu, Z.; Pedrycz, W. Assessment for hierarchical medical policy proposals using hesitant fuzzy linguistic analytic network process. Knowl. Based Syst. 2018, 161, 254–267. [Google Scholar] [CrossRef]
- Sun, X.; Sun, T.; Jin, Y.; Wang, Y.P. Spatial Organization of Hierarchical Medical Services within the City Proper of Tianjin, China: Towards Efficient Medical Alliances. Sustainability 2019, 11, 229. [Google Scholar] [CrossRef] [Green Version]
- Runtu, T.M.; Novieastari, E.; Handayani, H. How does organizational culture influence care coordination in hospitals? A systematic review. Enferm. Clín. 2019, 29, 785–802. [Google Scholar] [CrossRef]
- Tang, L. An ideal city model belonging to China. China Econ. Rep. 2013, 9, 70–74. [Google Scholar]
- Jia, P.; Qin, F. Realistic Urban Planning. Beijing Plan. Rev. 2015, 6, 58–61. [Google Scholar]
- Torrisi, V.; Ignaccolo, M.; Inturri, G. Estimating travel time reliability in urban areas through a dynamic simulation model. Transp. Res. Procedia 2017, 27, 857–864. [Google Scholar] [CrossRef]
- Liu, M.; Zhang, X. Analysis on the Regional Differences and Their Causes about Total Factor Productivity Growth of China’s Health Care System. Shanghai J. Econ. 2013, 3, 68–80. [Google Scholar]
- Zhang, J.; Tan, W.; Qi, Y. Model of “Internet + Healthcare” System Based on System Dynamics. J. Shenyang Univ. Technol. 2019, 12, 137–144. [Google Scholar]
- Zheng, D.; Gong, J.; Zhang, C. Efficiency of medical service systems in the rural areas of Mainland China: A comparative study from 2013 to 2017. Public Health 2019, 171, 139–147. [Google Scholar] [CrossRef]
- Yang, W.X.; Li, L.G. Energy Efficiency, Ownership Structure, and Sustainable Development: Evidence from China. Sustainability 2017, 9, 912. [Google Scholar] [CrossRef] [Green Version]
- Yu, J.; Zhou, K.; Yang, S. Land use efficiency and influencing factors of urban agglomerations in China. Land Use Policy 2019, 88, 104143. [Google Scholar] [CrossRef]
- Cheng, B.; Li, X.; Lu, Y.; Tan, Y. Agent-based Modeling and Simulation Research into Residents Healthcare Choice. Syst. Eng. 2009, 27, 96–101. [Google Scholar]
- Jiang, Y.; Yang, J. Route of Achieving Hierarchical Medical System by Optimizing the Elements of Affecting the Choice of Medical Service. Chin. Hosp. 2015, 19, 15–17. [Google Scholar]
- Yang, Z. Turn allocation within the medical-service-seeking party in Chinese accompanied medical consultations. J. Pragmat. 2019, 143, 135–155. [Google Scholar] [CrossRef]
- Shi, M. Vertical Regional Medical Cluster in China: Progress and Challenges. Chin. J. Heal. Policy 2013, 6, 28–32. [Google Scholar]
- Li, J.; Zhen, T.; Zhao, F.; Gu, J.; Dou, W.; Ma, X.; Han, Z.; Wen, N. Research on the Problems of Primary Medical Care System Based on Medical Consortium—Taking Shandong Province as an Example. Soft Sci. Heal. 2014, 28, 747–751. [Google Scholar]
- Peiris, D.; Sun, L.; Patel, A.; Tian, M.; Essue, B.; Jan, S.; Zhang, P. Systematic medical assessment, referral and treatment for diabetes care in China using lay family health promoters: Protocol for the SMARTDiabetes cluster randomised controlled trial. Implement. Sci. 2016, 11, 116. [Google Scholar] [CrossRef] [Green Version]
- Akdur, G. The use of biological cellular automaton models in medical, health and biological studies. Procedia Soc. Behav. Sci. 2011, 28, 825–831. [Google Scholar] [CrossRef] [Green Version]
- Chen, D.D.; Lin, Y.C.; Wu, F. A design framework for optimizing forming processing parameters based on matrix cellular automaton and neural network-based model predictive control methods. Appl. Math. Model. 2019, 76, 918–937. [Google Scholar] [CrossRef]
- Sitko, M.; Chao, Q.; Wang, J.; Perzynski, K.; Muszka, K.; Madej, L. A parallel version of the cellular automata static recrystallization model dedicated for high performance computing platforms–Development and verification. Comput. Mater. Sci. 2020, 172, 109283. [Google Scholar] [CrossRef]
- Shanghai Municipal Health Commission. Shanghai Health and Wellness Statistics, 2018; Shanghai Municipal Health Commission: Shanghai, China, 2019. Available online: http://wsjkw.sh.gov.cn/tjsj2/20190507/63877.html (accessed on 24 October 2019).
- Shanghai Municipal Bureau of Statistics. Shanghai Statistical Yearbook 2018; China Statistics Press: Beijing, China, 2019. [Google Scholar]
- Li, J.; Luo, L.; Wu, X.; Liao, C.; Liao, H.; Shen, W. Prioritizing the elective surgery patient admission in a Chinese public tertiary hospital using the hesitant fuzzy linguistic ORESTE method. Appl. Soft Comput. 2019, 78, 407–419. [Google Scholar] [CrossRef]
- Wu, X.; Wu, X.; Gao, Y.; Wang, L.; Jin, J.; Li, Y.; Cheng, S.; Wen, X.; Wang, A.; Li, Q.; et al. Research-training needs of clinical nurses: A nationwide study among tertiary hospitals in China. Int. J. Nurs. Sci. 2019, 6, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Lok, K.I.; Zhang, L.; Hu, A.; Ungvari, G.S.; Bressington, D.T.; Cheung, T.; An, F.R.; Xiang, Y.T. Prevalence of verbal and physical workplace violence against nurses in psychiatric hospitals in China. Arch. Psychiatr. Nurs. 2019, 33, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Ning, X. Implement the Palliative Care in Medical Practice of a Tertiary Comprehensive Hospital in China. Chin. Med. Sci. J. 2018, 33, 210–215. [Google Scholar]
- Huang, W.T.; Chen, P.S.; Liu, J.J.; Chen, Y.R.; Chen, Y.H. Dynamic configuration scheduling problem for stochastic medical resources. J. Biomed. Inform. 2018, 80, 96–105. [Google Scholar] [CrossRef]
- Yin, C.; He, Q.; Liu, Y.; Chen, W.; Gao, Y. Inequality of public health and its role in spatial accessibility to medical facilities in China. Appl. Geogr. 2018, 92, 50–62. [Google Scholar] [CrossRef]
- Liu, J.; Zhu, B.; Zhang, N.; He, R.; Mao, Y. Are medical graduates’ initial intentions consistent with whether they ultimately opt for rural practice after graduation? A cross-sectional survey in western China. Lancet 2018, 392, S18. [Google Scholar] [CrossRef]
- Yang, W.; Li, L. Efficiency Evaluation and Policy Analysis of Industrial Wastewater Control in China. Energies 2017, 10, 1201. [Google Scholar] [CrossRef]
- Yang, M. Demand for social health insurance: Evidence from the Chinese New Rural Cooperative Medical Scheme. China Econ. Rev. 2018, 52, 126–135. [Google Scholar] [CrossRef]
- Lai, I.K.W.; Tam, S.K.T.; Chan, M.F.S. Knowledge cloud system for network collaboration: A case study in medical service industry in China. Expert Syst. Appl. 2012, 39, 12205–12212. [Google Scholar] [CrossRef]
- Liu, L.; Liu, L.; Fu, X.; Huang, Q.; Zhang, X.; Zhang, Y. A cloud-based framework for large-scale traditional Chinese medical record retrieval. J. Biomed. Inform. 2018, 77, 21–33. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Yang, W. Does Whistleblowing Work for Air Pollution Control in China? A Study Based on Three-party Evolutionary Game Model under Incomplete Information. Sustainability 2019, 11, 324. [Google Scholar] [CrossRef] [Green Version]
- Qi, X.; Wan, Y.; Huang, J. Traditional Chinese medicine treatment of solid-pseudopapillary tumor of the pancreas: A case report. Adv. Integr. Med. 2019, 6, S56–S57. [Google Scholar] [CrossRef]
- Zang, R.; Shi, J.; Lerut, T.E.; Wang, L.; Liu, C.; Brunelli, A.; Petersen, R.H.; Ng, C.S.H.; Lim, E.; Gao, S. Ten-Year Trends of Clinicopathologic Features and Surgical Treatment of Lung Cancer in China. Ann. Thorac. Surg. 2019, 08, 017. [Google Scholar] [CrossRef]













© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shen, X.; Yang, W.; Sun, S. Analysis of the Impact of China’s Hierarchical Medical System and Online Appointment Diagnosis System on the Sustainable Development of Public Health: A Case Study of Shanghai. Sustainability 2019, 11, 6564. https://0-doi-org.brum.beds.ac.uk/10.3390/su11236564
Shen X, Yang W, Sun S. Analysis of the Impact of China’s Hierarchical Medical System and Online Appointment Diagnosis System on the Sustainable Development of Public Health: A Case Study of Shanghai. Sustainability. 2019; 11(23):6564. https://0-doi-org.brum.beds.ac.uk/10.3390/su11236564
Chicago/Turabian StyleShen, Xiaojuan, Weixin Yang, and Shaorong Sun. 2019. "Analysis of the Impact of China’s Hierarchical Medical System and Online Appointment Diagnosis System on the Sustainable Development of Public Health: A Case Study of Shanghai" Sustainability 11, no. 23: 6564. https://0-doi-org.brum.beds.ac.uk/10.3390/su11236564