Electroacupuncture with Usual Care for Patients with Non-Acute Pain after Back Surgery: Cost-Effectiveness Analysis Alongside a Randomized Controlled Trial


Abstract
:1. Introduction
2. Materials and Methods
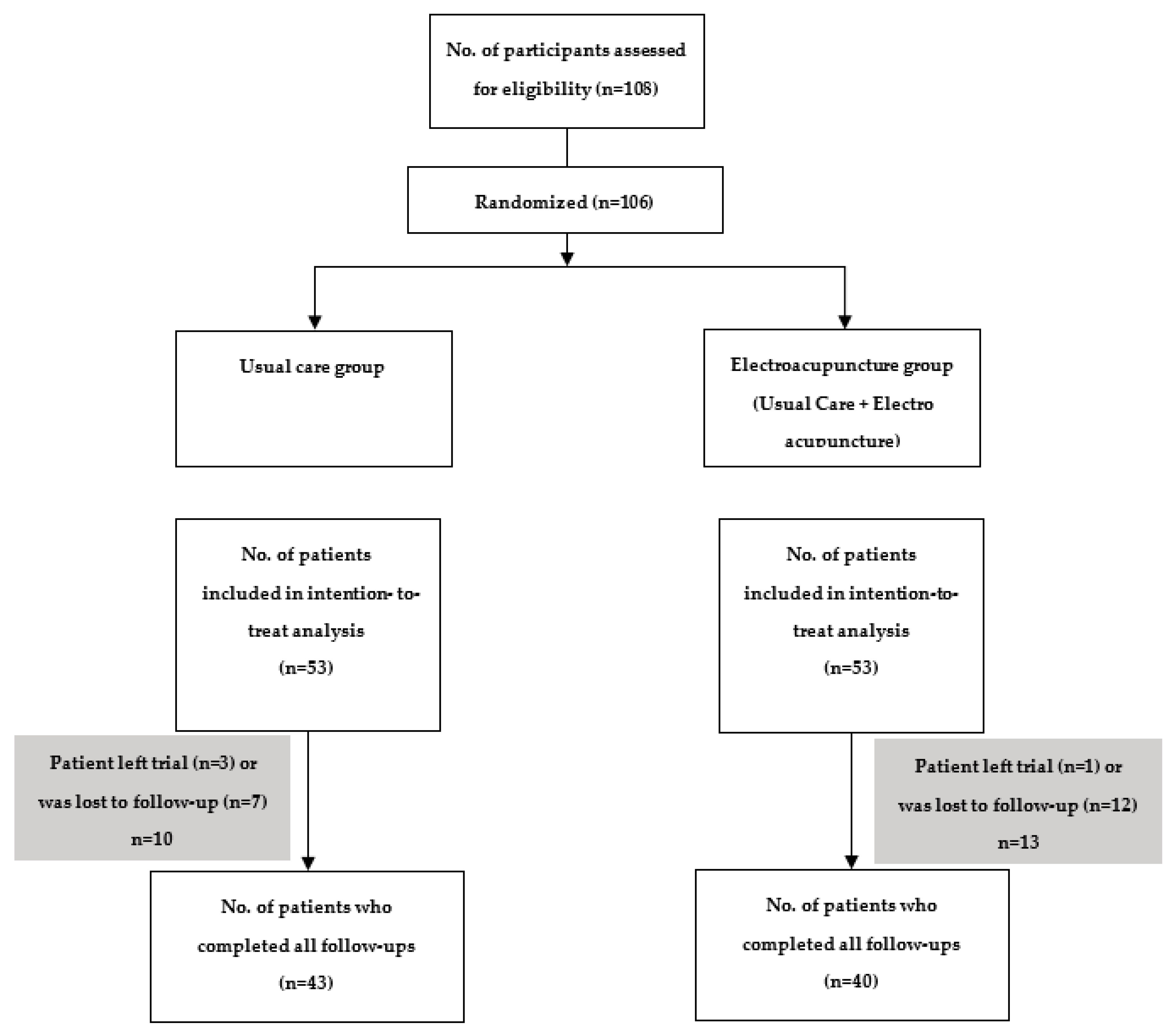
2.1. Randomization Design and Participants
2.2. Ethics
2.3. Interventions
2.3.1. Usual Care
2.3.2. Electroacupuncture Collaboration
2.3.3. Permitted and Prohibited Concomitant Treatments
2.4. Utility Measure and Valuation
2.5. Resource Use and Cost Measures
2.6. Missing Data Analysis
2.7. Cost-Utility Analyses
2.8. Sensitivity Analysis
3. Results
3.1. Costs
3.2. Utilities
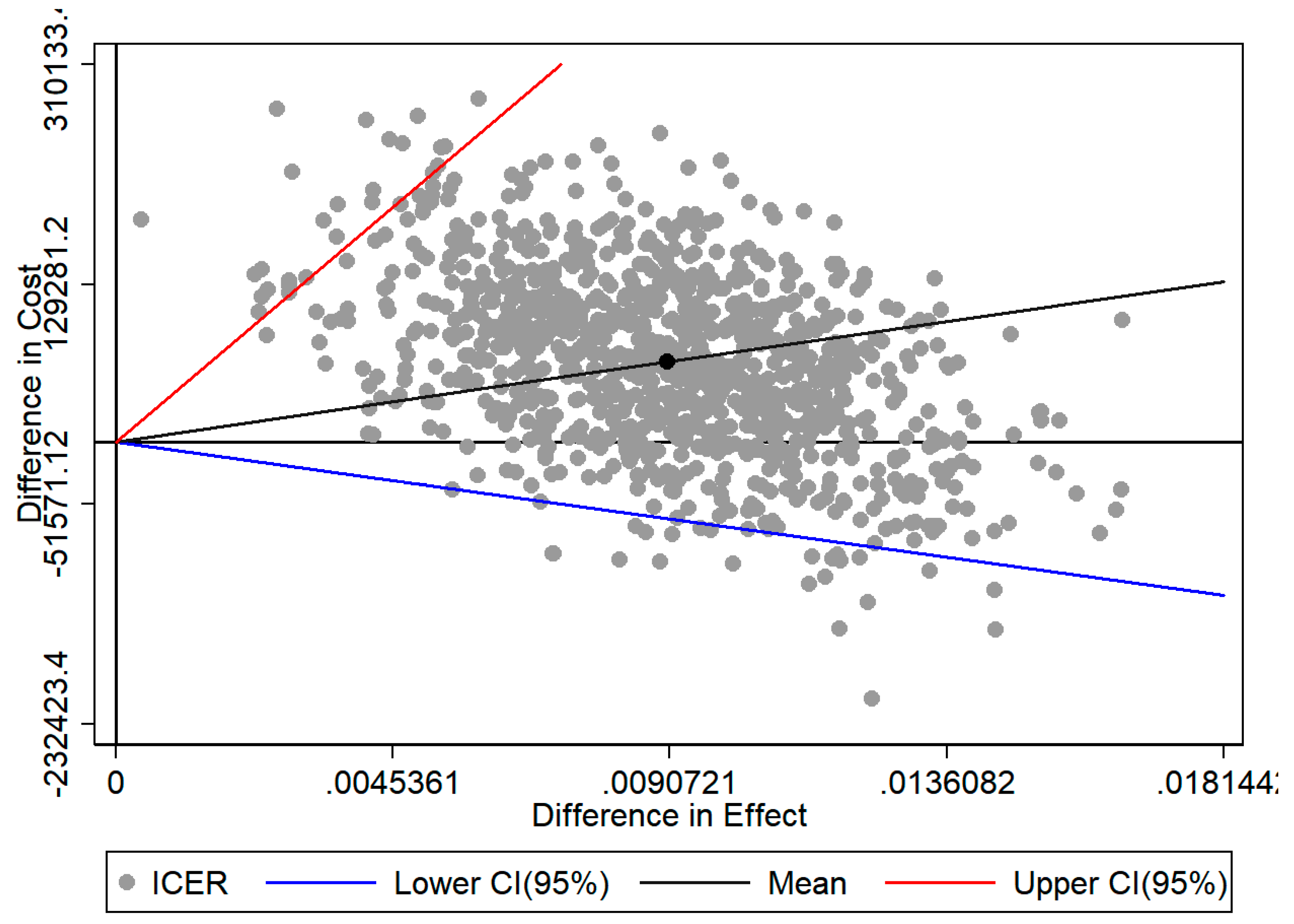
3.3. Incremental Cost-Effectiveness Ratio (ICER)
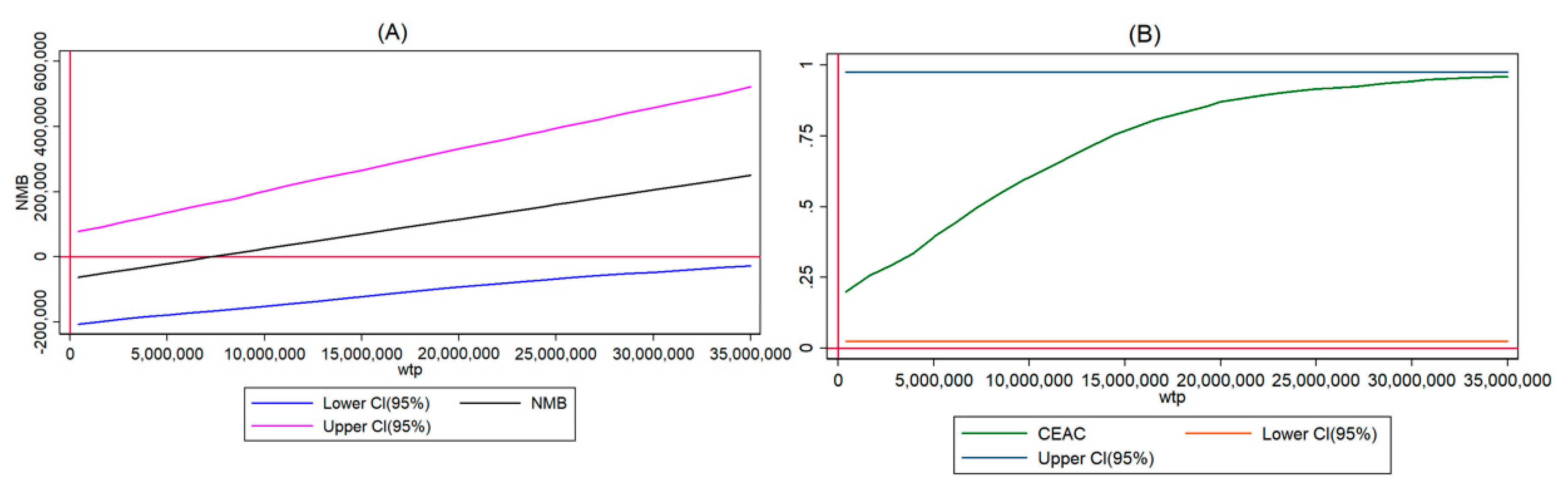
3.4. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ogura, S.; Jakovljevic, M. Health Financing Constrained by Population Aging-An Opportunity to Learn from Japanese Experience/Finansiranje Zdravstvene Zaštite U Uslovima Starenja Popualcije-Prilika Da Učimo Na Japanskom Iskustvu. J. Exp. Clin. Res. 2014, 15, 175–181. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Moon, Y. A Study of the Financial Projection of Health Expenditures of The Aged of National Health Insurance - Focused on the Healthy Ageing of EU -. J. Crit. Soc. Policy 2018, 58, 53–93. [Google Scholar]
- Health Insurance Review & Assessment Service. Available online: https://www.hira.or.kr/rd/insuadtcrtr/bbsView.do?pgmid=HIRAA030069000400&brdScnBltNo=4&brdBltNo=51540&isPopupYn=Y#none (accessed on 1 May 2020).
- Andersson, G.B. Epidemiological features of chronic low-back pain. Lancet 1999, 354, 581–585. [Google Scholar] [CrossRef]
- Hoy, D.; March, L.; Woolf, A.; Blyth, F.; Brooks, P.; Smith, E.; Vos, T.; Barendregt, J.; Blore, J.; Murray, C. The global burden of neck pain: Estimates from the global burden of disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1309–1315. [Google Scholar] [CrossRef]
- Oliveira, C.B.; Maher, C.G.; Pinto, R.Z.; Traeger, A.C.; Lin, C.-W.C.; Chenot, J.-F.; van Tulder, M.; Koes, B.W. Clinical practice guidelines for the management of non-specific low back pain in primary care: An updated overview. Eur. Spine J. 2018, 27, 2791–2803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cummins, J.; Lurie, J.D.; Tosteson, T.; Hanscom, B.; Abdu, W.A.; Birkmeyer, N.J.; Herkowitz, H.; Weinstein, J. Descriptive epidemiology and prior healthcare utilization of patients in the spine patient outcomes research trial’s (sport) three observational cohorts: Disc herniation, spinal stenosis and degenerative spondylolisthesis. Spine 2006, 31, 806. [Google Scholar] [CrossRef]
- Korea Institute of Oriental medicine. Lumbar Herniated Intervertebral Disc Korean Medicine Clinical Practice Guideline; Elsevier Korea: Seoul, Korea, 2015. [Google Scholar]
- Sin, S.; Kim, M.; Kim, C.; Jung, C. A study on medicinal Service Use of spinal Surgery Patients; Health Insurance Review & Assessment Service Seoul: Seoul, Korea, 2015; p. 124. [Google Scholar]
- Kim, C.H.; Chung, C.K.; Park, C.S.; Choi, B.; Kim, M.J.; Park, B.J. Reoperation rate after surgery for lumbar herniated intervertebral disc disease: Nationwide cohort study. Spine 2013, 38, 581–590. [Google Scholar] [CrossRef]
- Kim, C.H.; Chung, C.K.; Park, C.S.; Choi, B.; Hahn, S.; Kim, M.J.; Lee, K.S.; Park, B.J. Reoperation rate after surgery for lumbar spinal stenosis without spondylolisthesis: A nationwide cohort study. Spine J. 2013, 13, 1230–1237. [Google Scholar] [CrossRef]
- Ostelo, R.W.; Costa, L.O.P.; Maher, C.G.; de Vet, H.C.; van Tulder, M.W. Rehabilitation after lumbar disc surgery. Cochrane Database Syst. Rev. 2008, 14, CD003007. [Google Scholar]
- Ostelo, R.W.; De Vet, H.C.; Vlaeyen, J.W.; Kerckhoffs, M.R.; Berfelo, W.M.; Wolters, P.M.; Van den Brandt, P.A. Behavioral graded activity following first-time lumbar disc surgery: 1-year results of a randomized clinical trial. Spine 2003, 28, 1757–1765. [Google Scholar] [CrossRef]
- Taylor, R.S.; Taylor, R.J. The economic impact of failed back surgery syndrome. Br. J. Pain 2012, 6, 174–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skolasky, R.L.; Wegener, S.T.; Maggard, A.M.; Riley III, L.H. The impact of reduction of pain after lumbar spine surgery: The relationship between changes in pain and physical function and disability. Spine 2014, 39, 1426–1432. [Google Scholar] [CrossRef] [PubMed]
- Hutchison, R.W.; Chon, E.H.; Tucker Jr, W.F.; Gilder, R.; Moss, J.; Daniel, P. A comparison of a fentanyl, morphine, and hydromorphone patient-controlled intravenous delivery for acute postoperative analgesia: A multicenter study of opioid-induced adverse reactions. Hosp. Pharmacy 2006, 41, 659–663. [Google Scholar] [CrossRef]
- Ricardo Buenaventura, M.; Rajive Adlaka, M.; Nalini Sehgal, M. Opioid complications and side effects. Pain Physician 2008, 11, S105–S120. [Google Scholar]
- Ballantyne, J.C.; LaForge, S.K.J.P. Opioid dependence and addiction during opioid treatment of chronic pain. Pain 2007, 129, 235–255. [Google Scholar] [CrossRef]
- Wheway, J.; Agbabiaka, T.B.; Ernst, E. Patient safety incidents from acupuncture treatments: A review of reports to the National Patient Safety Agency. Int. J. Risk Saf. Med. 2012, 24, 163–169. [Google Scholar] [CrossRef]
- Lin, C.-W.C.; Haas, M.; Maher, C.G.; Machado, L.A.; van Tulder, M.W. Cost-effectiveness of guideline-endorsed treatments for low back pain: A systematic review. Eur. Spine J. 2011, 20, 1024–1038. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.-H.; Choi, T.-Y.; Lee, M.S.; Lee, H.; Shin, B.-C.; Lee, H. Acupuncture for acute low back pain: A systematic review. Clin. J. Pain 2013, 29, 172–185. [Google Scholar] [CrossRef]
- Casimiro, L.; Barnsley, L.; Brosseau, L.; Milne, S.; Welch, V.; Tugwell, P.; Wells, G.A. Acupuncture and electroacupuncture for the treatment of rheumatoid arthritis. Cochrane Database Syst. Rev. 2005, 19, CD003788. [Google Scholar] [CrossRef]
- Huang, H.; Zheng, S.; Feng, J. Thin’s abdominal acupuncture for treatment of failed back surgery syndrome in 20 cases of clinical observation. Guid. J. Trad. Chin. Med. Pharm. 2012, 18, 63–65. [Google Scholar]
- Heo, I.; Hwang, M.-S.; Hwang, E.-H.; Cho, J.-H.; Ha, I.-H.; Shin, K.-M.; Lee, J.-H.; Kim, N.-K.; Son, D.-W.; Shin, B.-C. Electroacupuncture as a complement to usual care for patients with non-acute low back pain after back surgery: A pilot randomised controlled trial. BMJ Open 2018, 8, e018464. [Google Scholar] [CrossRef] [PubMed]
- Glick, H.A.; Doshi, J.A.; Sonnad, S.S.; Polsky, D. Economic Evaluation in Clinical Trials; OUP Oxford: Oxford, UK, 2014. [Google Scholar]
- Annemans, L.; Van Buyten, J.P.; Smith, T.; Al-Kaisy, A. Cost effectiveness of a novel 10 kHz high-frequency spinal cord stimulation system in patients with failed back surgery syndrome (FBSS). J. Long-Term Eff. Med Implant 2014, 24, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Roulaud, M.; Durand-Zaleski, I.; Ingrand, P.; Serrie, A.; Diallo, B.; Peruzzi, P.; Hieu, P.D.; Voirin, J.; Raoul, S.; Page, P.; et al. Multicolumn spinal cord stimulation for significant low back pain in failed back surgery syndrome: Design of a national, multicentre, randomized, controlled health economics trial (ESTIMET Study). Neuro-Chir. 2015, 61, S109–S116. [Google Scholar] [CrossRef]
- Zucco, F.; Ciampichini, R.; Lavano, A.; Costantini, A.; De Rose, M.; Poli, P.; Fortini, G.; Demartini, L.; De Simone, E.; Menardo, V.; et al. Cost-Effectiveness and Cost-Utility Analysis of Spinal Cord Stimulation in Patients With Failed Back Surgery Syndrome: Results From the PRECISE Study. Neuromodulation J. Int. Neuromodulation Soc. 2015, 18, 266–276. [Google Scholar] [CrossRef] [Green Version]
- Farber, S.H.; Han, J.L.; Elsamadicy, A.A.; Hussaini, Q.; Yang, S.; Pagadala, P.; Parente, B.; Xie, J.; Lad, S.P. Long-term Cost Utility of Spinal Cord Stimulation in Patients with Failed Back Surgery Syndrome. Pain Physician 2017, 20, E797–E805. [Google Scholar]
- Kim, N.; Yang, B.; Lee, T.; Kwon, S. An economic analysis of usual care and acupuncture collaborative treatment on chronic low back pain: A Markov model decision analysis. BMC Complement. Altern. Med. 2010, 10, 74. [Google Scholar] [CrossRef] [Green Version]
- Shin, B.-C.; Cho, J.-H.; Ha, I.-H.; Heo, I.; Lee, J.-H.; Kim, K.-W.; Kim, M.-R.; Jung, S.-Y.; Kwon, O.; Kim, N.-K. A multi-center, randomized controlled clinical trial, cost-effectiveness and qualitative research of electroacupuncture with usual care for patients with non-acute pain after back surgery: Study protocol for a randomized controlled trial. Trials 2018, 19, 65. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.-K.; Nam, H.-S.; Chuang, L.-H.; Kim, K.-Y.; Yang, H.-K.; Kwon, I.-S.; Kind, P.; Kweon, S.-S.; Kim, Y.-T. South Korean time trade-off values for EQ-5D health states: Modeling with observed values for 101 health states. Value Health 2009, 12, 1187–1193. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health and Welfare. Designating 65 Hospitals as the Pilot Project Participating Hospitals and Clinics for Chuna of Korean Medicine. Available online: http://www.mohw.go.kr/react/al/sal0301vw.jsp?PAR_MENU_ID=04&MENU_ID=0403&page=1&CONT_SEQ=338360 (accessed on 1 May 2020).
- Richardson, G.; Manca, A.J.H.E. Calculation of quality adjusted life years in the published literature: A review of methodology and transparency. Health Econ. 2004, 13, 1203–1210. [Google Scholar] [CrossRef]
- Shin, H. Current Issues and Tasks in Health Policy. Health Welf. Policy Forum 2020, 1, 9–22. [Google Scholar]
- Thomson, S.; Foubister, T.; Mossialos, E. Financing Health Care in the European Union: Challenges and Policy Responses; World Health Organization. Regional Office for Europe: Copenhagen, Denmark, 2009. [Google Scholar]
- Zhang, R.; Lao, L.; Ren, K.; Berman, B.M. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology 2014, 120, 482–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ratcliffe, J.; Thomas, K.J.; MacPherson, H.; Brazier, J. A randomised controlled trial of acupuncture care for persistent low back pain: Cost effectiveness analysis. BMJ (Clin. Res. Ed.) 2006, 333, 626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witt, C.M.; Jena, S.; Selim, D.; Brinkhaus, B.; Reinhold, T.; Wruck, K.; Liecker, B.; Linde, K.; Wegscheider, K.; Willich, S.N. Pragmatic randomized trial evaluating the clinical and economic effectiveness of acupuncture for chronic low back pain. Am. J. Epidemiol. 2006, 164, 487–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andronis, L.; Kinghorn, P.; Qiao, S.; Whitehurst, D.G.; Durrell, S.; McLeod, H.J. Cost-effectiveness of non-invasive and non-pharmacological interventions for low back pain: A systematic literature review. Appl. Health Econ. Health Policy 2017, 15, 173–201. [Google Scholar] [CrossRef] [PubMed]
- Willich, S.N.; Reinhold, T.; Selim, D.; Jena, S.; Brinkhaus, B.; Witt, C.M.J.P. Cost-effectiveness of acupuncture treatment in patients with chronic neck pain. Pain 2006, 125, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Taylor, P.; Pezzullo, L.; Grant, S.J.; Bensoussan, A.J.P.P. Cost-effectiveness of Acupuncture for Chronic Nonspecific Low Back Pain. Pain Pract. 2014, 14, 599–606. [Google Scholar] [CrossRef]
- Toroski, M.; Nikfar, S.; Mojahedian, M.M.; Ayati, M.H. Comparison of the Cost-utility Analysis of Electroacupuncture and Nonsteroidal Antiinflammatory Drugs in the Treatment of Chronic Low Back Pain. J. Acupunct. Meridian Stud. 2018, 11, 62–66. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Usual Care (N = 53) | Electroacupuncture (N = 53) | p-Value | |||
|---|---|---|---|---|---|---|
| Mean, SD or N, Percent | Mean, SD or N, Percent | |||||
| Sex | Male (N, %) | 26 | 49.06 | 27 | 50.94 | 0.846 |
| Female (N, %) | 27 | 50.94 | 26 | 49.06 | ||
| Age | 46.08 | 14.56 | 45.91 | 13.09 | 0.950 | |
| Income (KRW) | Less than 10 million | 8 | 15.09 | 6 | 11.32 | 0.445 |
| 10–50 million | 25 | 47.17 | 23 | 43.40 | ||
| 50–100 million | 19 | 35.85 | 19 | 35.85 | ||
| More than 100 million | 1 | 1.89 | 5 | 9.43 | ||
| BMI | 23.9 | 3.89 | 23.9 | 3.06 | 0.996 | |
| OP hospital | Clinic | 22 | 41.51 | 16 | 30.19 | 0.340 |
| Hospital | 23 | 43.40 | 24 | 45.28 | ||
| General hospital | 8 | 15.09 | 13 | 24.53 | ||
| Carer | None | 5 | 9.43 | 5 | 9.43 | 0.631 |
| Family | 37 | 69.81 | 41 | 77.36 | ||
| Family and carer | 4 | 7.55 | 1 | 1.89 | ||
| Carer | 7 | 13.21 | 6 | 11.32 | ||
| Admission day | 20.43 | 19.71 | 34.35 | 68.08 | 0.156 | |
| Operation cost | 4,403,529 | 3,183,233.00 | 7,941,085 | 21,800,000.00 | 0.253 | |
| Direct medical cost | 1,725,472 | 1,965,332.00 | 3,798,113 | 5,806,710.00 | 0.016 | |
| Care time | 319.7 | 526.10 | 262 | 333.90 | 0.502 | |
| Week work time | 48.51 | 23.83 | 50.06 | 24.62 | 0.747 | |
| Absenteeism (day) | 32.26 | 86.25 | 27.55 | 71.10 | 0.774 | |
| Presenteeism (percent) | 6.151 | 2.38 | 6.039 | 2.58 | 0.819 | |
| EQ-5D (baseline) | 0.72 | 0.13 | 0.74 | 0.15 | 0.296 | |
| EQ-VAS | 62.15 | 11.31 | 60.58 | 14.26 | 0.532 | |
| Variables | Follow-Up Time | Usual Care (n = 43) | Electroacupuncture (n = 40) | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| EQ-5D | Baseline | 0.741 | 0.11 | 0.755 | 0.155 |
| 4 weeks | 0.771 | 0.105 | 0.797 | 0.095 | |
| 8 weeks | 0.782 | 0.108 | 0.810 | 0.097 | |
| 12 weeks | 0.791 | 0.105 | 0.820 | 0.117 | |
| 24 weeks | 0.804 | 0.101 | 0.803 | 0.15 | |
| Direct medical costs (KRW) | 1–4 weeks | 119,355 | 24,013 | 230,085 | 50,409 |
| 5–8 weeks | 2474 | 8552 | 11,320 | 69,990 | |
| 9–12 weeks | 1228 | 6937 | 6285 | 34,834 | |
| 13–24 weeks | 37,660 | 162,502 | 83,875 | 351,700 | |
| Direct non-medical costs (KRW) | 1–4 weeks | 143,365 | 63,631 | 130,000 | 6236 |
| 5–8 weeks | 125,780 | 56,194 | 116,210 | 6230 | |
| 9–12 weeks | 125,909 | 56,212 | 116,796 | 8160 | |
| 13–24 weeks | 126,637 | 56,265 | 117,868 | 9596 | |
| Productivity costs (KRW) | 1–4 weeks | 610,361 | 130,076 | 600,011 | 142,028 |
| 5–8 weeks | 330,598 | 191,156 | 338,616 | 215,182 | |
| 9–12 weeks | 313,959 | 173,367 | 313,205 | 225,202 | |
| 13–24 weeks | 1,106,316 | 742,713 | 1,021,153 | 693,301 | |
| Resources | Usual Care (n = 43) | Electroacupuncture (n = 40) | Mean Difference | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | 95% CI | |
| QALYs (6 months) | 0.361 | 0.041 | 0.370 | 0.047 | 0.009 | (−0.010, 0.028) |
| Direct medical costs | 160,718 | 159,735 | 331,565 | 374,476 | 170,847 | (46,645, 295,049) |
| Direct non-medical costs | 521,691 | 231,482 | 480,873 | 26,190 | −40,818 | (−114,105, 32,468) |
| Productivity costs | 2,361,235 | 1,044,315 | 2,272,985 | 1,142,409 | −88249.4 | (−565,821, 389,322) |
| Total costs (LSP) | 682,409 | 274,958 | 812,438 | 382,578 | 130,029 | (−14,718, 274,776) |
| Total costs (SP) | 3,043,643 | 1,098,816 | 3,085,423 | 1,338,813 | 41,780 | (−491,576, 575,136) |
| Analyses | Perspectives | Treatments | Cost | Delta Cost | QALYs | Delta QALYs | ICER |
|---|---|---|---|---|---|---|---|
| ITT | SP | UC (N = 53) | 3,052,480 | 0.35836 | |||
| EA (N = 53) | 3,117,082.6 | 64,602.56 | 0.367526 | 0.009 | 7,048,602.88 | ||
| LSP | UC (N = 53) | 683,687 | 0.358677 | ||||
| EA (N = 53) | 827,131 | 143,444 | 0.366774 | 0.008 | 17,716,572.4 | ||
| PP | SP | UC (N = 43) | 3,043,643 | 0.361 | |||
| EA (N = 40) | 3,085,423 | 41,780 | 0.37 | 0.009 | 4,674,999.16 | ||
| LSP | UC (N = 43) | 682,409 | 0.361 | ||||
| EA (N = 40) | 812,438 | 130,029 | 0.37 | 0.009 | 14,549,698.4 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, N.; Shin, K.-M.; Seo, E.-S.; Park, M.; Lee, H.-Y. Electroacupuncture with Usual Care for Patients with Non-Acute Pain after Back Surgery: Cost-Effectiveness Analysis Alongside a Randomized Controlled Trial. Sustainability 2020, 12, 5033. https://0-doi-org.brum.beds.ac.uk/10.3390/su12125033
Kim N, Shin K-M, Seo E-S, Park M, Lee H-Y. Electroacupuncture with Usual Care for Patients with Non-Acute Pain after Back Surgery: Cost-Effectiveness Analysis Alongside a Randomized Controlled Trial. Sustainability. 2020; 12(12):5033. https://0-doi-org.brum.beds.ac.uk/10.3390/su12125033
Chicago/Turabian StyleKim, NamKwen, Kyung-Min Shin, Eun-Sung Seo, Minjung Park, and Hye-Yoon Lee. 2020. "Electroacupuncture with Usual Care for Patients with Non-Acute Pain after Back Surgery: Cost-Effectiveness Analysis Alongside a Randomized Controlled Trial" Sustainability 12, no. 12: 5033. https://0-doi-org.brum.beds.ac.uk/10.3390/su12125033